
Abstract
Background:
Although many instruments aiming to measure attitudes toward people with borderline personality disorder (BPD) exist, most demonstrate limited evidence of construct validity.
Aims:
To evaluate the psychometric properties of the Prejudice toward People with Borderline Personality Disorder (PPBPD) scale in a sample of healthcare providers (HCPs) and expand the nomological network of prejudice toward people with BPD.
Method:
A survey containing the PPBPD scale and related measures was completed by 593 HCPs who provided services for people with BPD.
Results:
Confirmatory factor analysis supported the four-factor structure, comprising fear/avoidance, malevolence, authoritarianism, and unpredictability. Differential associations were found between the four PPBPD factors and correlates, such as knowledge of BPD, belief in treatment effectiveness and patient recovery, prior contact with patients who have BPD, and empathy.
Conclusions:
The results provided evidence for the validity and psychometric properties of the PPBPD in a sample of HCPs and support its utility in measuring attitudes toward people with BPD. The expansion of the PPBPD’s nomological network improves understanding of how this prejudice may be maintained, and reduced, in healthcare settings. This research will contribute to efforts in developing and implementing interventions to support HCPs and reduce prejudice toward people living with BPD.
Keywords
Introduction
Despite continued publications on the issue, healthcare provider (HCP) stigma toward people with borderline personality disorder (BPD) remains pervasive (Ring & Lawn, 2019). People living with BPD face reduced willingness to help, therapeutic pessimism, blame, and treatment denial when seeking care (Lam et al., 2016; Markham & Trower, 2003; Sulzer, 2015). Understanding the underlying negative attitudes, or prejudice, that lead to discriminatory behaviors (Corrigan & Kosyluk, 2014) is a vital step in reducing stigma. Various instruments have been utilized to measure attitudes toward people with BPD, many of which require validation (Baker & Beazley, 2022). For example, the Attitude to Personality Disorder Questionnaire (APDQ; Bowers & Allan, 2006) was used to assess the effect of a DBT training program on attitudes, finding a significant improvement in some attitudes toward patients with BPD (Tan et al., 2023). In another study, the Borderline Patients – Cognitive Attitudes and Treatment (BPD-CAT) and Emotional Attitudes (BPD-EA) inventories (Bodner et al., 2011) were used to evaluate an education program aiming to improve attitudes toward people with BPD and found that the intervention improved BPD-EA Negative Attitudes subscale scores, but worsened scores on the BPD-CAT Antagonistic Judgments subscale (Dickens et al., 2019). The use of different operationalizations of attitudes within these studies, however, prevents the integration of their results to inform future intervention development.
Across the existing scales there is no clear and consistent conceptualization of attitudes toward people with BPD. As such, scales often omit important aspects of attitudes, for instance the APDQ (Bowers & Allan, 2006) which focuses solely on the affective aspect of attitudes and omits the cognitive and behavioral intention aspects. Often, scale items do not target people with BPD, instead targeting other entities such as the individual or their knowledge (e.g. Shanks et al., 2011). The attitude dimensions being assessed also vary across measures, such as perceived dangerousness (e.g. Link et al., 1987) or empathy (e.g. McAllister et al., 2002), with no agreement on the content or structure of the dimensions underlying prejudice toward people with BPD. Further, there is limited evidence that the factor structures of each scale are replicable. For example, the factor structures of the BPD-CAT and BPD-EA (Bodner et al., 2011) have not been replicated.
To address similar limitations in measures of attitudes toward people with mental health conditions, the Prejudice toward People with Mental Illness (PPMI; Kenny et al., 2018) scale was developed based on thematic analysis of existing conceptualizations and measures. Subsequent analysis identified and supported four latent factors of Fear/Avoidance (desire for social distance and belief of dangerousness), Malevolence (lack of sympathy), Authoritarianism (limiting choice and autonomy), and Unpredictability (belief that people with mental health conditions behave in completely unforeseeable ways). This four-factor structure has been supported across different groups and languages (e.g. Alharthi et al., 2021; Bizumic et al., 2022; Sander et al., 2022), as well as when assessing prejudice toward people with specific mental health conditions like schizophrenia, depression, dissociative identity disorder, and BPD (Bizumic & Gunningham, 2022; Reisinger & Gleaves, 2023; Sheppard et al., 2023).
The four factors are bipolar and contain an equal number of items that measure both prejudicial (e.g. ‘People with [borderline personality disorder] do not deserve our sympathy’) and supportive attitudes (e.g. ‘People who have [borderline personality disorder] should be free to make their own decisions’). This allows the causes and outcomes of supportive, as well as prejudicial, attitudes to be assessed and provides more meaningful outcomes for interventions aiming to improve attitudes. Consequently, a version of the PPMI scale that was adapted to focus on people with BPD, called the Prejudice toward People with BPD (PPBPD) scale (Sheppard et al., 2023), could be valuable in assessing, improving understanding of, and addressing the high levels of prejudice toward people with BPD reported in HCPs.
The current study
The first aim of this study was to evaluate the psychometric properties of the PPBPD scale in a sample of HCPs. The scale has worked well in medical, clinical psychology, and undergraduate psychology students, as well as a general population sample (Sheppard et al., 2023). HCPs, however, typically have closer interactions with people who have BPD and greater knowledge of the condition than people in the general population. As such, it is possible that prejudice operates differently within this population. Assessing whether the scale works in a HCP sample would provide valuable information regarding the structure of prejudice toward people with BPD and the utility of the PPBPD scale. In this endeavor, we expected that the four-factor structure comprising fear/avoidance, malevolence, authoritarianism, and unpredictability, would be replicated in a sample of HCPs (Hypothesis 1).
The second aim was to test and expand the nomological network of the PPBPD model. Previously, empathy (specifically empathic concern and perspective-taking), frequency and quality of contact with people who have BPD, and knowledge of BPD have been linked to reduced prejudice toward people with BPD (Sheppard et al., 2023). Given that education in BPD care and treatment options have led to improved attitudes and hope for patient recovery (Tan et al., 2023; Usher et al., 2024), it is likely that knowledge of treatment options and belief in treatment effectiveness will also be associated with lower prejudice. Furthermore, HCP’s belief in BPD recovery was identified as an important theme in positive therapeutic relationships by people living with BPD (Romeu-Labayen et al., 2020), indicating that it may relate to more positive attitudes toward people with BPD in a HCP sample. Additionally, given that research suggests self-compassion can buffer against compassion-fatigue and burnout, and has positive associations with empathy, particularly perspective-taking (Duarte et al., 2016; Fuochi et al., 2018; Savieto et al., 2019), we expected that it would also be associated with lower prejudice. Subsequently, we hypothesized that prejudice toward people with BPD would negatively relate to empathy, frequency and quality of contact, knowledge of BPD and treatment options, belief that treatment is effective, belief in patient recovery, and self-compassion (Hypothesis 2).
Although increased contact is thought to reduce prejudice, negative attitudes and stigma have been linked to stressful interactions with patients who have BPD (Commons Treloar, 2009). Following this, distress tolerance, the ability to tolerate and accept distress without being overwhelmed or making it worse, has been identified as an important skill when providing services to patients with BPD (McMain et al., 2015) and may be linked to reduced prejudice. Additionally, given that people living with BPD have been perceived as more in control of their condition and behavior than people with other mental health conditions (Elliott & Ragsdale, 2024; Sulzer, 2015), the perception of controllability (either control of a cause or of a behavior; Markham & Trower, 2003) and responsibility for behavior may play a significant role in higher prejudice (Corrigan et al., 2003; Cryer et al., 2020). Finally, the perceived un-treatability and ‘difficulty’ of patients with BPD were identified as key themes related to stigma toward people with BPD (Ring & Lawn, 2019) and would be expected to relate to higher prejudice. Thus, we hypothesized that prejudice toward people with BPD would positively relate to increased contact with patients experiencing a mental health crisis, distress intolerance, the belief that a person can control whether they develop BPD, belief in greater control over and responsibility for behavior than people with other mental health conditions, and the perception that providing care for patients with BPD is more difficult than for patients who do not have BPD (Hypothesis 3).
Method
Ethical considerations
This study was approved by the Australian National University Human Ethics Committee (Protocol: 2019/753). Participants gave informed written consent prior to commencing the survey and could opt to remove their data from the analysis upon survey completion without penalty.
Participants
Participants were recruited via the online survey platform Prolific Academia in March 2024. Participants on Prolific have been reported to provide higher quality data than participants from other online platforms or student samples (Douglas et al., 2023). People living in Australia, New Zealand, Ireland, or the United Kingdom were sought as similarities in access to publicly funded baseline healthcare, as well as private healthcare options, and an emphasis on primary and secondary care teams (Dixit & Sambasivan, 2018; OECD, 2019; OECD/European Observatory on Health Systems and Policies, 2021; Tikkanen et al., 2020) make these nations’ healthcare systems somewhat comparable. Participants who worked in a broad range of healthcare professions were sought in order to test how the PPBPD scale performed across a sample that varied in expertise and knowledge. Of the 599 participants who completed the survey, five were removed due to choosing to have their data removed from the analysis, and one for completing the survey too quickly (less than 1/3 of the median completion time).
The final sample included 593 participants. The mean age was 37.4 (SD = 11.2) and the majority of respondents reported being female (56.2%), from the United Kingdom (82.8%), and working in a community health setting (35.8%). Table 1 presents the participant demographic and profession information.
Participant demographics.
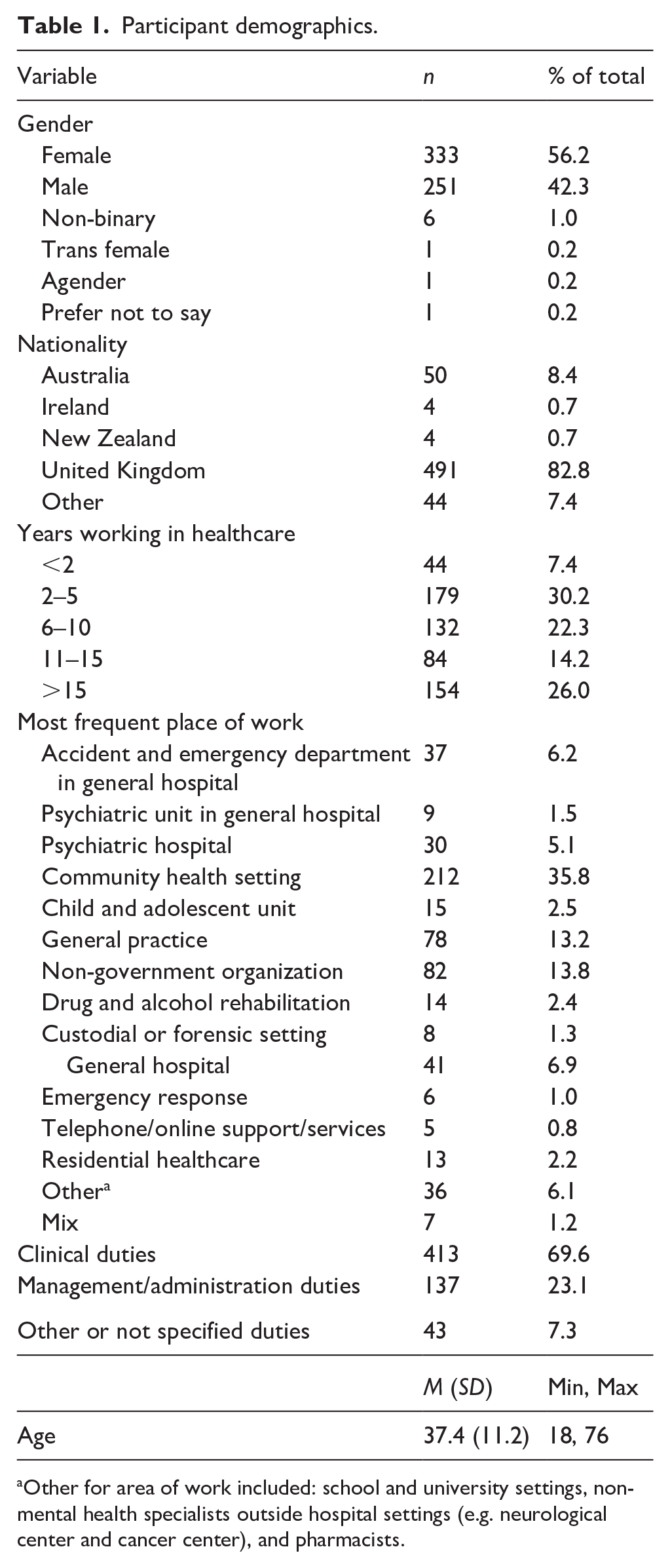
Other for area of work included: school and university settings, non-mental health specialists outside hospital settings (e.g. neurological center and cancer center), and pharmacists.
Procedure and materials
Participants completed two online surveys. Participants who indicated that they worked in healthcare were selected for a brief, paid (£0.15) screening survey to determine if they had knowledge of BPD and provide services to people who have BPD (see Supplemental Material 1). Eligible participants were then invited to participate in the paid main survey (£3). The surveys consisted of measures of demographic and profession-related variables, knowledge of and contact with people who have BPD, prejudice toward people with BPD, and hypothesized correlates. The measures were presented in this order, with the presentation order of the correlates being randomized. The presentation order of items within each scale was also randomized. Unless otherwise stated, the individual item scores of single item measures were used in the analysis and scale scores were calculated by taking the average of the item scores. All reported coefficient alphas, McDonald’s Coefficient Omega, and Spearman-Brown coefficients were obtained from the current study.
Prejudice toward people with BPD
Prejudice was measured using the 28-item PPBPD scale (Sheppard et al., 2023; α = .91; ω = .91). The 8-item Fear/Avoidance (α = .87; ω = .88), 8-item Malevolence (α = .77; ω = .77), 6-item Authoritarianism (α = .79; ω = .79), and 6-item Unpredictability (α = .79; ω = .79) subscales are scored on a 9-point Likert scale, ranging from 1 (very strongly disagree) to 9 (very strongly agree). Higher scores were indicative of more prejudicial attitudes. The scale can be found in Supplemental Material 2.
Experience with and knowledge of BPD
Ten questions from Cleary et al.’s (2002) staff experience, knowledge and attitudes survey were used to assess experience with and knowledge of BPD. Three single-item questions asked respondents to indicate their profession, work duties, and years in healthcare (see Table 1). A 3-item scale and a 5-item scale were used to assess respondent’s self-reported knowledge and confidence in identifying, assessing, managing, and referring patients with BPD, respectively. Both scales ranged from 1 (not at all) to 4 (very). A 7-item measure was used to assess knowledge of BPD. Respondents were asked to indicate if they agreed, disagreed, or did not know the answer to six statements related to BPD and select the incorrect statement for the seventh item. Each correct response was given one point, which were totaled to provide a scale score ranging from 0 to 7. Finally, two single-item questions were used to assess the respondent’s perceived difficulty of providing services to patients with BPD (ranging from 1 = easy, to 5 = very difficult) and whether they find working with clients who have BPD to be more difficult than other patients (1 = more difficult, 0 = ‘the same’ or ‘less difficult’).
Recognition of treatment options
Participants were also asked to indicate if they ‘have knowledge of’, ‘have little knowledge of’, ‘recognize but don’t know about it’, or were ‘not aware of’ seven types of treatment for BPD (see Supplemental Material 3). Responses were given a score of 0 to 4, respectively, and item scores were summed to provide an overall recognition of treatment score. The treatments included in this question were informed by recent reviews of treatment for BPD (Choi-Kain et al., 2017; Levy et al., 2018).
Belief in treatment effectiveness and patient recovery
A single item ‘Borderline personality disorder can be effectively treated’, 1 (strongly disagree) to 5 (strongly agree), was used to assess the belief that BPD is a treatable condition. An additional 4-items assessed HCPs belief in their patients’ potential for recovery (α = .86; e.g. ‘I believe that they are able to recover’) on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). Higher scores were indicative of greater belief that treatment is effective and belief in their patients’ ability to recover.
Perception of and reasons for difficulty treating patients with BPD
An 11-item bespoke scale was designed to investigate why participants may perceive treating patients with BPD as difficult (e.g. ‘I don’t have sufficient training for treating BPD’). The items were based on Ring and Lawn’s (2019) literature review of mental healthcare professionals’ perceptions of treating patients with BPD. Participants indicated agreement with each item on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Individual item scores were used in the analysis.
Controllability and responsibility
A single item was used to assess the respondent’s belief in whether a person can control if they develop BPD (Cryer et al., 2020). Two additional single item measures were adapted based on Corrigan’s (2000) Controllability, Affect, and Behavioral Response model to assess belief of whether a person with BPD is more in control of, or responsible for, their behaviors than people with other severe mental disorders. Participants indicated agreement with each item on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Contact
Frequency, situation, and quality of prior contact were measured via a single item asking how often the respondent interacts with someone who has BPD ranging from never to every work day (Bizumic & Gunningham, 2022), a 5-item measure of the regularity of contact situations (e.g. ‘As a regular ongoing patient/client’; almost never to almost always), and a feeling thermometer rating on average how positive interactions were (−50 = very negative experience, +50 = very positive experience). Individual item scores were used in the analyses.
Self-compassion, empathy, and distress intolerance
Self-compassion was measured with the 12-item Self-Compassion Scale – Short Form (α = .89; Raes et al., 2011), and six 2-item subscales: Common Humanity (the Spearman–Brown coefficient, ρ = .70), Self-kindness (ρ = .69), Mindfulness (ρ = .72), Isolation (ρ = .73), Self-judgment (ρ = .74), and Over Identification (ρ = .79). Empathy and distress intolerance were measured with the 7-item Empathic Concern (α = .81) and Perspective-Taking (α = .80) subscales of the Interpersonal Reactivity Index (Davis, 1980), and the 10-item Distress Intolerance scale (α = .92; McHugh & Otto, 2012). These scales were each measured on a 5-point Likert scale. Higher scores were indicative of greater self-compassion, empathic concern for others, perspective-taking, and distress intolerance, respectively.
Data analysis
Confirmatory factor analysis was performed using R Statistical Software (v4.2.2; R Core Team, 2022) and lavaan R package (Rosseel, 2012) to investigate the hypothesized four-factor structure of the PPBPD scale. An additional negative ‘method factor’, on which all negatively-keyed items were loaded, was included to account for method effects due to acquiescence bias or failing to attend to negative wording of items (Schmitt & Stults, 1986). The following fit indices and cut-off points were used to assess the model fit: CFI ⩾ 0.90, RMSEA ⩽ 0.06, and SRMR ⩽ 0.08 (Tabachnick & Fidell, 2013).
All remaining analyses were conducted using jamovi (v2.3.18; The jamovi project, 2024). Mean differences in attitudes across professional groups were explored using independent samples t-tests. Associations between study variables were explored using zero-order and semipartial correlations.
Results
On average, participants reported low-to-medium levels of prejudice across the total scale (M = 3.8, SD = 0.9), and the Fear/avoidance (M = 3.7, SD = 1.3), Malevolence (M = 2.9, SD = 1.0), and Authoritarianism (M = 3.3, SD = 1.2) subscales. The average score for the Unpredictability subscale was above the mid-point of the scale (M = 5.8, SD = 1.1). The mean and standard deviations for the correlates can be found in Supplemental Material 4.
Scale structure
When compared to a unidimensional model and three-factor model (see Supplemental Material 2), the four-factor model demonstrated the best fit, χ2(326) = 974.68, p < .001, CFI = 0.90, RMSEA = 0.058, SRMR = 0.052. The four factors were significantly correlated (see Figure 1) and the 28 items loaded onto their hypothesized factors.
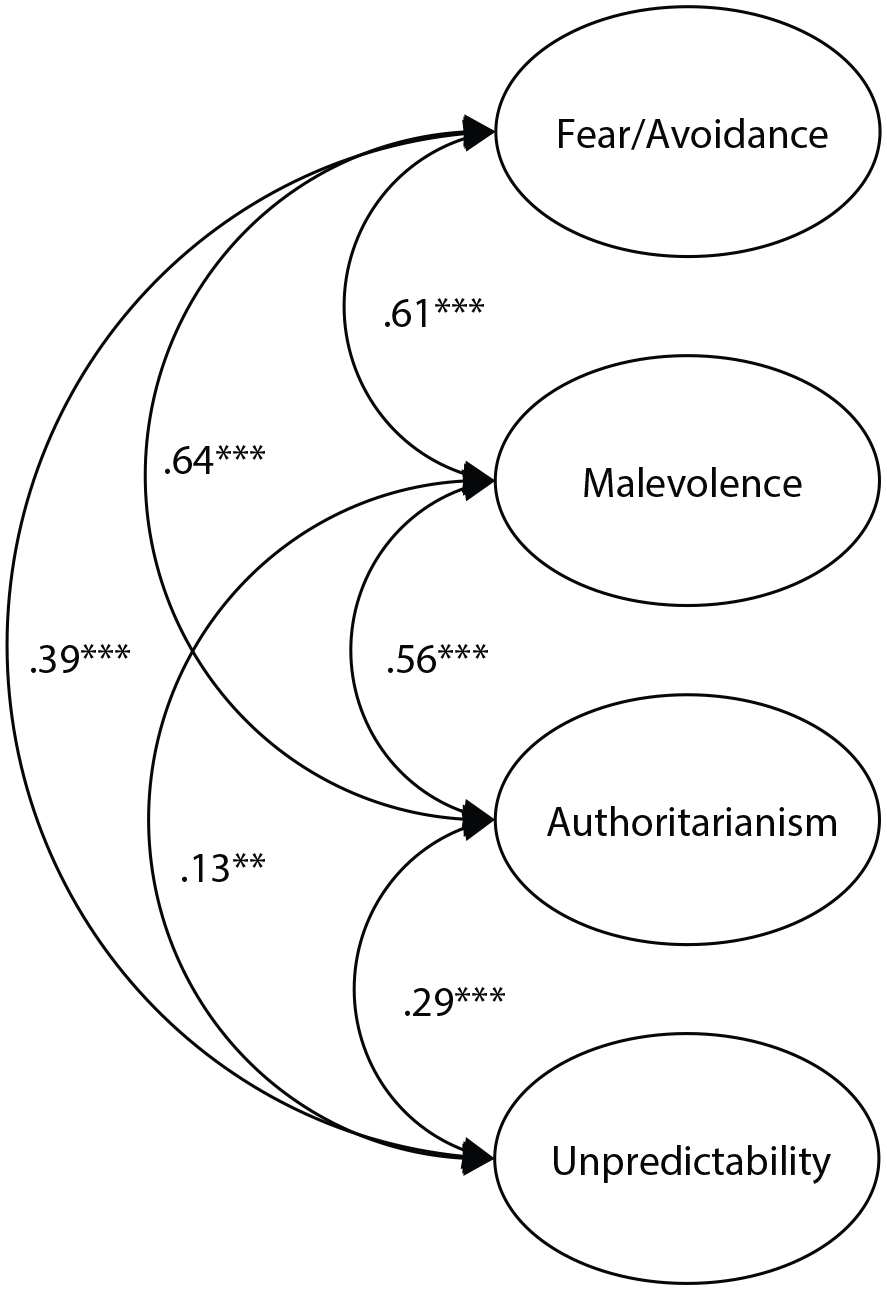
Intercorrelations between the factors in the four-factor model of prejudice toward people with borderline personality disorder.
Profession-related differences in attitudes
Mean PPBPD scores for participants working in accident and emergency departments (A&E) were significantly higher than participants working in other healthcare contexts, t(591) = 3.57, p < .001 (see Supplemental Material 5). The difference in mean scores was also found in the fear/avoidance, t(591) = 3.29, p < .01, malevolence, t(591) = 3.04, p < .01, and unpredictability subscales, t(591) = 2.54, p < .05. Significantly higher scale scores than other contexts were also found in participants who worked in general practice for total, t(591) = 2.30, p < .05, fear/avoidance, t(591) = 3.02, p < .01, and unpredictability prejudice, t(591) = 3.12, p < .01. Respondents who indicated their work duties were mostly clinical reported significantly higher fear/avoidance scores than respondents with non-clinical duties, t(591) = 1.59, p < .05. Furthermore, significantly lower scores were found in participants who frequently worked across a mix of contexts for total PPBPD, t(591) = −2.35, p < .05, as well as for fear/avoidance, t(591) = −2.20, p < .05.
Correlation analysis
Correlation analysis was used to examine the associations between the PPBPD scale and theorized correlates. Knowledge of BPD and treatment options, belief that treatment is effective, belief in patient recovery, frequency and quality of contact, empathy, and self-compassion all had negative associations with the PPBPD’s four dimensions (see Table 2). Analysis of semi-partial correlations examined the unique relationships between the four dimensions and the antecedents and correlates. When controlling for the effect of the other three dimensions, fear/avoidance had the strongest associations with positive prior contact and belief in patient recovery. Malevolence had the strongest associations with recognition/knowledge of treatment options and empathic concern. Unpredictability had a weak negative relationship with positive prior contact, and authoritarianism had a weak negative relationship with perspective-taking.
Zero-order (r) and semipartial (sr) correlations of the PPBPD scale and subscales with correlates (where relationships were expected to be negative).
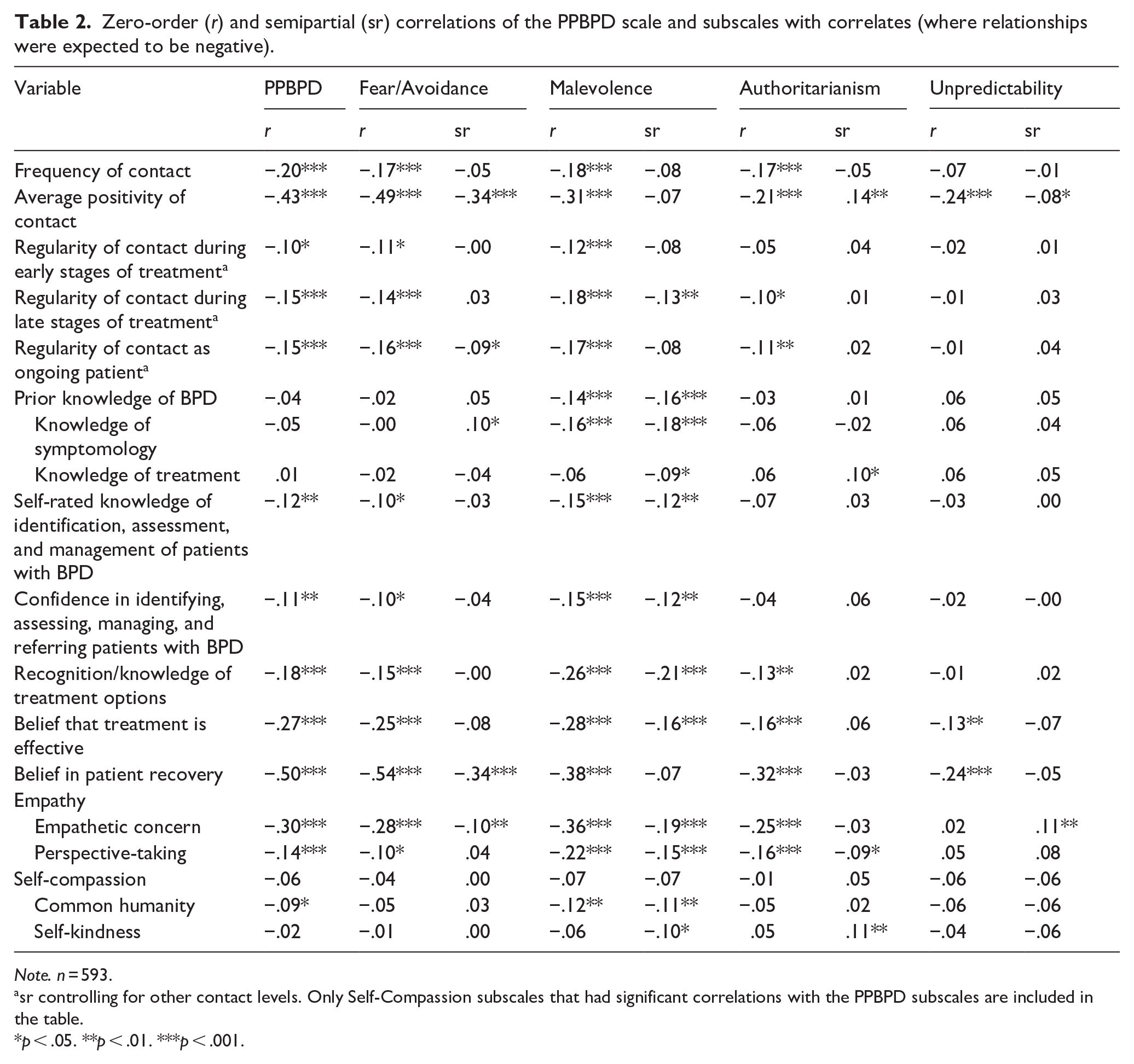
Note. n = 593.
sr controlling for other contact levels. Only Self-Compassion subscales that had significant correlations with the PPBPD subscales are included in the table.
p < .05. **p < .01. ***p < .001.
Perceiving BPD patients as being more difficult to provide services for, increased contact with patients experiencing a mental health crisis, perceived controllability of developing BPD, and belief in behavior control and responsibility, but not distress intolerance, had positive associations with the total PPBPD scale and the four dimensions (see Table 3). Semi-partial correlations show differential associations for each of the four dimensions. Fear/avoidance was most strongly associated with the perception that patients with BPD are more difficult to provide services for. Malevolence was most strongly associated with the belief that people with BPD have more control over and responsibility for their behaviors than those with other severe disorders, and the perception that patients with BPD are untreatable. Authoritarianism only related to the perceived controllability of developing BPD. Unpredictability was associated with patients being perceived as more difficult, specifically the belief that patients with BPD are an increased risk of harm or are too complex.
Zero-order (r) and Semipartial (sr) correlations of the PPBPD scale and subscales with correlates (where relationships were expected to be positive).
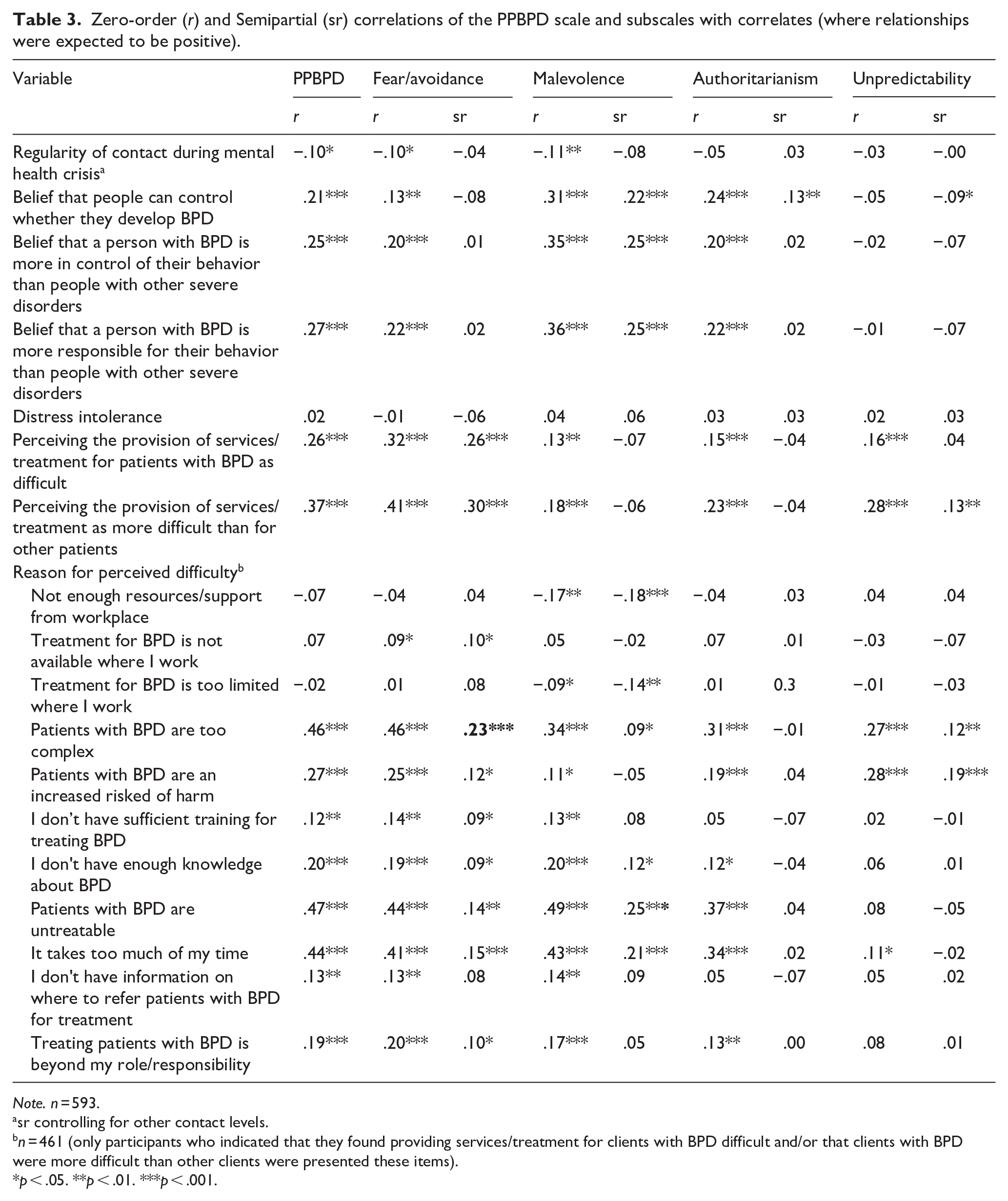
Note. n = 593.
sr controlling for other contact levels.
n = 461 (only participants who indicated that they found providing services/treatment for clients with BPD difficult and/or that clients with BPD were more difficult than other clients were presented these items).
p < .05. **p < .01. ***p < .001.
Perceived difficulty and reasons
The perception of and reasons for difficulty providing services to patients with BPD were examined (see Supplemental Material 6). Most participants (70.0%) reported providing services to patients with BPD as difficult, with half (50.6%) reporting it as more difficult than for other patients. The most common reasons related to limited training, knowledge, resources, and treatment options, with not having enough resources/support from the workplace being endorsed by 79.7%. Additionally, 64.2% of participants reported that an increased risk of harm contributed to service/treatment provision difficulty.
Discussion
The current study aimed to investigate the psychometric properties of the PPBPD scale in a sample of HCPs and expand upon the nomological network. In support of Hypothesis 1, the four-factor structure was supported within a HCP sample, indicating that HCP attitudes toward people with BPD comprise the four dimensions of fear/avoidance, malevolence, authoritarianism, and unpredictability. This provides support for the structural validity of the PPBPD scale and indicates that prejudice toward people with BPD has the same four-factor structure in a HCP sample as it does in student and general population samples (Sheppard et al., 2023).
Hypotheses 2 and 3 were partially supported, as most of the predicted correlations between the PPBPD scales and external variables were found, supporting the construct validity of the PPBPD scale and expanding the nomological network. The correlations between fear/avoidance and prior positive contact, malevolence and empathic concern, authoritarianism and perspective-taking, and unpredictability and prior positive contact replicate those found in a prior study (Sheppard et al., 2023). The predicted, novel correlations between the PPBPD scale and the external variables demonstrate concordance with the literature. For example, prior research suggests that perceptions of controllability (either control of development or behavior) relate to blame toward people with mental health conditions (Haslam & Kvaale, 2015) and greater support for segregation and forced treatment (Corrigan et al., 2003), which are reflected in the positive associations found between perceptions of controllability and the Malevolence and Authoritarianism subscales, respectively.
Although an attention to emotional arousal and reactivity in both client and therapist has been recommended for cultivating positive therapeutic relationships with patients who have BPD (for a review, see: McMain et al., 2015), a possible relationship between negative attitudes and skills like distress tolerance had not been empirically tested. The non-significant correlation found in this study indicates that distress intolerance does not relate directly to prejudice toward people with BPD. It is possible that, although distress tolerance is considered important for therapists, its influence may not have as great an impact on the attitudes and patient relationships of the various HCP groups included in this sample. Conversely, distress tolerance may have indirect impacts on attitudes, through factors such as contact quality and improved service provision, which were not examined in this study.
The sample included a variety of HCPs who were expected to have a range of expertise and knowledge related to BPD. This was intended to reflect the broad range of HCPs a person with BPD may come into contact with, as people with BPD experience stigma in both primary and secondary care settings (for a review, see: Ring & Lawn, 2019; Wu et al., 2022). Hence, it was important to test the PPBPD scale within a wide range of HCPs who provide services for patients with BPD, and whose variations in knowledge and exposure would be expected to lead to different responses on the scale. Validation of the PPBPD scale within such a sample provides evidence that the PPBPD model is relevant to HCPs across expertise levels and that the PPBPD scale is useful for research investigating attitudes in different HCP groups.
The differential associations between the four dimensions and the external variables demonstrate the utility of assessing prejudice toward people with BPD using the PPBPD scale. Improving understanding of the specific antecedents and consequences of each dimension provides vital information for developing research-based interventions aiming to improve attitudes. As shown in this study, a group (or person) can demonstrate low prejudice on one or more dimensions, and high prejudice on others. Identifying dimensions of interest to a specific group can promote the implementation of targeted, successful stigma reducing interventions that may also save time and resources.
This study supports that the PPBPD model and scale are useful in understanding the complexities of prejudice in HCP populations. Given that intervention success can vary for different aspects of stigma (Modgill et al., 2014), deeper understanding of the type of attitudes a population hold provides more information for how the prejudice may be tackled. For example, previous research investigating the success of education interventions in reducing the four dimensions of prejudice toward people with mental health conditions have found no significant reductions in malevolence prejudice (Kenny & Bizumic, 2016; Richards et al., 2023). Nonetheless, the associations with treatment knowledge and belief in treatability indicate that education focused on treatment could be more successful in reducing malevolence attitudes. Indeed, training sessions on specific forms of BPD treatment/management have been found to improve HCP attitudes toward patients with BPD (Tan et al., 2023; Usher et al., 2024). Further, the significantly higher fear/avoidance and unpredictability prejudice found in participants working in general practice may indicate the benefit of exposure and contact focused interventions for people working in this context (Sheppard et al., 2023). Kohrt et al. (2020) found that training sessions that included contact with and in-person recovery stories from both people with BPD and HCPs were successful in increasing willingness to interact with patients who have mental health conditions from 54% to 81%. Following the relationships found in this study, it is possible that instilling hope for their patients’ prognosis and the HCP’s role in recovery could be beneficial in increasing willingness to engage with patients who have BPD.
Limitations and suggestions for future research
Correlations, particularly those of external variables with authoritarianism and unpredictability, were small to moderate. Prejudice is highly complex and influenced by many factors, and the current study could only include a limited number of variables. Future research may look to identify other relevant variables and investigate causative relationships, both to further validate the PPBPD and improve knowledge of the causes and consequences of these attitudes. Burnout, stress, and exposure to intense emotional pain and trauma, often collectively called ‘compassion fatigue’ (Lisle et al., 2020), for example, may have particular importance for the attitudes HCPs hold toward people with BPD.
The wide variety of HCPs within the sample supports the use of the PPBPD scale across various HCP groups; however, the sample consisted primarily of community healthcare workers. Considering that treatment and support for people with BPD often involves community healthcare workers (e.g. Care Program Approach; National Institute for Health and Care Excellence, 2009), this study supports that the PPBPD scale can be utilized with HCPs who are integral to the treatment outcomes of people with BPD. Nevertheless, we cannot be sure that this sample is representative of the broader population of HCPs who provide services for people with BPD. Moreover, the study did not have sufficient power to investigate the associations between prejudice and external correlates within different professional contexts. Following this, future research may look to investigate prejudice toward people with BPD in specific healthcare populations. Previous research has indicated that some professions may hold more negative attitudes than others (Lam et al., 2016; Ring & Lawn, 2019). Indeed, this study indicated that people working in A&E settings may hold more prejudicial attitudes. Determining why these contextual differences may occur, for example, different levels of burnout, compassion-fatigue, or education/resource access, is vital in understanding how to support HCPs and improve attitudes toward people with BPD.
Summary and conclusions
The PPBPD model and associated scale were supported in a sample of HCPs, providing an empirically tested measure for attitudes toward people with BPD that can be used both within and outside healthcare populations. This supports its utility in improving understanding of prejudice toward people with BPD in healthcare settings. It is hoped that these findings will encourage further research into prejudice toward people living with BPD and the development of successful, research-based interventions.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251345028 – Supplemental material for The Prejudice toward People with Borderline Personality Disorder Scale in a healthcare provider sample
Supplemental material, sj-docx-1-isp-10.1177_00207640251345028 for The Prejudice toward People with Borderline Personality Disorder Scale in a healthcare provider sample by Hannah Sheppard, Boris Bizumic, Elizabeth Huxley and Alison L. Calear in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We are grateful to Amelia Norbury, Chun Kit Hui, and Nicholas Wai for their comments on a prior version of the manuscript. We are also thankful to Mental Health Australia for funding this study through the 2020 Grace Groom Memorial Scholarship.
Author contributions
Hannah Sheppard led the conception and design of the study. She completed the data acquisition and analysis. Hannah also led the interpretation of the data, drafted the manuscript, and submitted the manuscript. Boris Bizumic supervised and contributed to the conception and design of the study. He contributed to the interpretation of the data, critically reviewed and edited all draft versions of the manuscript, and provided final approval of the version to be published. Elizabeth Huxley contributed to the conception and design of the study, including the development of the measures designed for this study. She contributed to the interpretation of the data, critically reviewed and edited draft versions of the manuscript, and provided final approval of the version to be published. Alison Calear contributed to the conception and design of the study, including the selection of measures included in the survey and the development of the measures designed for this study. She critically reviewed and edited draft versions of the manuscript, and provided final approval of the version to be published.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hannah Sheppard received funding for this study from Mental Health Australia via the 2020 Grace Groom Memorial Scholarship. Alison Calear is supported by NHMRC Fellowship (1173146). The sponsors had no involvement in the study design; collection, analysis and interpretation of the data; the writing of the article; or, decision to submit it for publication.
Ethical consideration
This study was reviewed and approved by the Australian National University Human Research Ethics Committee (Protocol: 2019/753), and the procedures followed were in accordance with the Helsinki Declaration as revised in 2013.
Consent to participate
The participants provided their written, informed consent to participate in this study.
Consent for publication
Prior to consenting to participate, participants were informed that data from the project may be included in student theses, published in journal articles and books, and presented at professional conferences, and that no individual participant would be identifiable in any of these formats. Upon completion of the survey, participants could opt to have their data removed from the study. The data of any participant who requested this was deleted and was not included in the analyses.
Data availability
Following the study’s approved ethics protocol, the averaged data are available from the author, H. Sheppard, upon a reasonable request.
Research material availability
The PPBPD scale is freely available for research use and is included in the supplemental material for this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.