
Abstract
Background:
People living with borderline personality disorder (BPD) face high levels of prejudice and discrimination from both the community and medical professionals, but no measure of prejudice toward people living with BPD exists.
Aims:
The current study aimed to adapt an existing Prejudice toward People with Mental Illness (PPMI) scale and investigate the structure and nomological network of prejudice toward people with BPD.
Methods:
The original 28-item PPMI scale was adapted to create the Prejudice toward People with Borderline Personality Disorder (PPBPD) scale. The scale and related measures were completed by three samples: 217 medical or clinical psychology students, 303 psychology undergraduate students, and 314 adults from the general population.
Results:
The original four-factor structure of the PPMI was supported in the PPBPD scale. Reported prejudice toward people with BPD was more negative than prejudice toward people with mental illness in general. The association of the PPBPD scale with antecedents and consequences was assessed, including social dominance orientation, right-wing authoritarianism, ethnocentrism, personality traits, empathy, prior contact, and feelings toward other stigmatized groups and mental illnesses.
Conclusions:
This study provided evidence for the validity and psychometric properties of the PPBPD scale across three samples and investigated anticipated relationships with theoretically related antecedents and consequences. This research will help improve understanding of the expressions underlying prejudice toward people with BPD.
The public interest in the 2022 Depp V. Heard trial brought attention to borderline personality disorder (BPD), a previously uncommonly recognized disorder (Furnham et al., 2015). People living with BPD report some of the highest levels of public, healthcare provider, and self-stigma of all diagnosis groups (Sheehan et al., 2016). Consequently, as public knowledge of BPD grows, it is vital that effective stigma reduction efforts are made.
Stigma toward people with mental illness and its negative impact on wellbeing, help-seeking, relationships, employment, healthcare costs, mental health outcomes, and the broader community are well documented (Corker et al., 2016; Osumili et al., 2016; Sharac et al., 2010; Webber et al., 2014; Wright et al., 2015). Nevertheless, limited success of stigma reducing interventions suggests a need for an expansion of knowledge of stigma toward people with mental illness, and its components (Corrigan et al., 2014; Griffiths et al., 2014; Stuart, 2016).
Stigma toward people with mental illness is expressed via stereotypes, prejudice, and discrimination (Corrigan & Kosyluk, 2014). Stereotypes are the knowledge component of stigma, which when endorsed becomes prejudice, the attitudinal component, which in turn tends to lead to discrimination, the behavioral component. A reduction in prejudice that drives discrimination will likely have the greatest success in reducing stigma (Kenny et al., 2018). Therefore, greater understanding of the antecedents, consequences, and structure of prejudice is necessary. Further, discrepancies in attitudes found toward people with different kinds of mental illness (Bizumic & Gunningham, 2022; Catthoor et al., 2015; Reavley & Jorm, 2011) indicates understanding and reducing prejudice requires a disorder-specific approach.
Research suggests people with personality disorders receive less public sympathy than people with any other mental illness (Furnham et al., 2015). Nonetheless, despite BPD being one of the most researched mental illnesses (Bonnington & Rose, 2014), no general population measure for assessing prejudice toward people with BPD exists. Most BPD stigma research has instead relied on adapting existing scales of stigma toward mental illness or personality disorders that omit important components of prejudice and/or are designed for use in healthcare provider populations only.
The Prejudice toward People with Mental Illness (PPMI) scale was developed to address the psychometric limitations of existing measures of attitudes toward people with mental illness in general and to facilitate the integration of prejudice and stigma research (Kenny et al., 2018). Thematic and statistical analysis of the PPMI scale identified four underlying bipolar factors, (i) Fear/Avoidance (interaction difficulty and desire for social distance), (ii) Malevolence (unsympathetic attitudes and belief of inferiority), (iii) Authoritarianism (desire to control and force treatment), and (iv) Unpredictability (believing people with mental illnesses behave unpredictably). The bipolar nature of these factors allows for a more nuanced investigation of the attitudes held toward people with mental illness, as people may express prejudicial attitudes in one area (e.g. express the desire for social distance), but supportive attitudes in other areas (e.g. believing society should provide appropriate access to treatment). The PPMI scale was positioned within a nomological network outlining anticipated relationships with external variables, further supporting construct validity, and has been successfully validated across multiple samples and cultures (Alharthi et al., 2021; Kenny & Bizumic, 2016; Sander et al., 2022; Scarf et al., 2020).
More recently, the PPMI scale has been successfully adapted to focus on prejudice toward people with depression and with schizophrenia (Bizumic & Gunningham, 2022), in both mental health professionals and the general population (Bizumic et al., 2022), suggesting the utility of the scale to assess both specific and general mental illness prejudice. Given this, the current study aimed to adapt the PPMI scale to produce a reliable measure for prejudice toward people with BPD that can be used across populations and to develop a nomological network of antecedents and observable outcomes to aid understanding of this prejudice. We expected the four-factor structure of Fear/Avoidance, Malevolence, Authoritarianism, and Unpredictability would replicate in prejudice toward people with BPD (Hypothesis 1).
As discussed above, research suggests people living with BPD face higher levels of stigma and prejudice than other diagnosis groups. Subsequently, we expected prejudice toward people with BPD would be more negative than prejudice toward people with mental illness in general (Hypothesis 2).
Ideological beliefs such as social dominance orientation (SDO; Sidanius & Pratto, 1999), right-wing authoritarianism (RWA; Bizumic & Duckitt, 2018), and ethnocentrism (Bizumic et al., 2009) were found to positively relate to prejudice, whereas the Big-Five’s agreeableness and openness to experience (McCrae & Costa, 2008), empathic concern and perspective-taking (Davis, 1980), and past contact with people with mental illness have related negatively (Bizumic & Gunningham, 2022; Kenny et al., 2018). Additionally, generalized prejudice and discriminatory behaviors were found to be consequences of prejudice toward people with mental illness. To provide construct validity for the Prejudice toward People with BPD (PPBPD) scale, the construct’s position within the aforementioned variables was investigated. Thus, we expected prejudice toward people with BPD would relate positively to SDO, RWA, ethnocentrism, and discriminatory behavior (Hypothesis 3). Finally, we expected prejudice toward people with BPD to relate negatively to empathy, prior contact with people with BPD, knowledge about BPD, agreeableness, openness to experience, and positivity toward stigmatized groups and other mental illnesses (Hypothesis 4).
Method
Participants
This study was approved by the Australian National University. Human Research Ethics Committee and participants provided informed written consent.
Sample 1
Sample 1 consisted of 217 Australian and New Zealand clinical psychology students, medical students, and undergraduate psychology students whose mean age was 26.8 years (SD = 8.13). Most participants were female (82%), Australian citizens (79%), White (69%), reported an average socio-economic status (SES; 38%), and selected English as their primary language (90%).
Sample 2
Sample 2 consisted of 303 Australian undergraduate psychology students who participated as part of their course requirements. Participant mean age was 21.6 years (SD = 2.57) and most were female (59%), Australian citizens (57%), White (50%), reported an average SES (45%), and selected English as their primary language (65%).
Sample 3
Sample 3 consisted of 314 people from the general population. Participant mean age was 29.75 years (SD = 10.57). In this sample 51% were female, 31% had completed college/university, and 45% spoke English as their first language. Participants primarily reported UK (16%) or Australian (16%) citizenship, with the remaining participants having other citizenship (68%).
Further information about demographics is in Supplemental Material 1.
Procedure
Participants completed either an online or paper and pen survey. All samples were provided with information about BPD to ensure some knowledge of BPD prior to completing the survey (Supplemental Material 2). Participants in sample 1 completed a knowledge of BPD measure and viewed a description of BPD after demographic questions at the beginning of the survey. Participants in sample 2 viewed segments of an award-winning documentary about people living with BPD called ‘Borderline’ (Ratner, 2016) prior to commencing the survey. Participants in sample 3 were provided with a vignette of a person living with BPD.
Participants completed demographics first, then the PPMI (sample 1 only) and PPBPD, then the measures of proposed antecedents and consequences (which were presented in a random order).
Sample 3 was collected as part of another research project and only the data collected for the PPBPD scale was used in this study.
Materials
Unless stated otherwise, all measures used a 9-point Likert-type scale, ranging from 1 (very strongly disagree) to 9 (very strongly agree) and the scale scores were the average of the item scores.
Prejudice toward people with borderline personality disorder
The 28-item PPBPD scale was created by replacing the term ‘mental illness’ in the PPMI with the term ‘borderline personality disorder’ (see Supplemental Material 3). The PPBPD scale was included in all three samples and had satisfactory reliability for the scale (sample 1 α = .91; sample 2 α = .90; and sample 3 α = .89), and its subscales: Fear/Avoidance (eight items; α = .85, .89, and .86; e.g. ‘I am not scared of people with borderline personality disorder’, reverse-scored), Malevolence (eight items; α = .77, .78, and .75; e.g. ‘People with borderline personality disorder do not deserve our sympathy’), Authoritarianism (six items; α = .80, .81, and .82; e.g. ‘People who have borderline personality disorder should be forced to have treatment’), and Unpredictability (six items; α = .88, .80, and .79; e.g. ‘People with borderline personality disorder often do unexpected things’). Higher scores indicate higher prejudice levels.
Prejudice toward people with mental illness
The 28-item PPMI scale (Kenny et al., 2018) was included for sample 1 only (α = .92), with balanced subscales measuring the factors of Fear/Avoidance (α = .88), Malevolence (α = .79), Authoritarianism (α = .81), and Unpredictability (α = .87).
Contact
A 10-item Level of Contact Report (Holmes et al., 1999) was adapted to create two scales to measure past contact with people with mental illness (sample 1 only) and BPD. Participants responded true or false to statements such as ‘I have a friend who has borderline personality disorder’ and were given a rank score of 1 to 10 based on their most intimate situation experienced, with 10 being the most intimate.
Quality of contact
Two feeling thermometers measured quality of contact with people with mental illness (sample 1 only) and BPD. Participants who indicated they had had contact with people with BPD rated their experience on a 101-point sliding scale −50 (very negative experience) to +50 (very positive experience).
Empathy
The 7-item Empathic Concern (sample 1 α = .78; sample 2 α = .82; e.g. ‘I would describe myself as a pretty soft-hearted person’) and the 7-item Perspective-Taking (α = .77; e.g. ‘I try to look at everybody’s side of a disagreement before I make a decision’; sample 1 only) subscales of the Interpersonal Reactivity Index (Davis, 1980) were used to measure empathy. Respondents indicated the accuracy of each statement on a Likert scale from 1 (very inaccurate) to 5 (very accurate).
Big-five personality traits
The 4-item Agreeableness (sample 1 α = .83; sample 2 α = .79; e.g. ‘I feel others’ emotions’) and Openness to Experience/Intellect (α = .75 and .69; e.g. ‘I have a vivid imagination’) subscales of the MINI-IPIP (Donnellan et al., 2006) were included to measure these Big-Five traits. Respondents indicated the accuracy of each statement on a Likert scale from 1 (very inaccurate) to 5 (very accurate).
Discriminatory behavior
A 6-item discriminatory behavior measure (α = .65; Kenny et al., 2018) assessed past behaviors toward people with mental illness in sample 1. Participants indicated the number of times, ranging from never to three or more times, they had engaged in the listed behaviors. This was replaced with an adapted 2-item behavioral intentions scenarios measure (Kenny et al., 2018) for sample 2, in which participants indicated which of four behaviors they would engage in in hypothetical scenarios (e.g. when a fellow student states that people with BPD should not be allowed to have children: ranging from 1 ‘I would voice my disagreement with the student’ to 4 ‘I would voice my agreement with the student’). A higher score indicates more discriminatory behavior.
Positivity toward other groups
Feeling thermometers were used to measure feelings toward immigrants, feminists, people with a physical disability, people on welfare, and Muslims (sample 1 α = .94; sample 2 α = .94) and toward people with depression, anxiety, anorexia, obsessive compulsive disorder, narcissistic personality disorder, substance abuse, and schizophrenia (α = .93 and .84). Participants rated their feelings on a 101-point sliding scale −50 (most negative) to +50 (most positive).
Social dominance orientation
A shortened, 6-item version of the Social Dominance Orientation scale (sample 1 α = .82; sample 2 α = .83; e.g. ‘Inferior groups should stay in their place’; Sidanius & Pratto, 1999) measured SDO. Higher scores indicate greater desire for social hierarchies.
Right-wing authoritarianism
The 6-item Very Short Authoritarianism scale (sample 1 α = .78; sample 2 α = .82; e.g. ‘There is nothing wrong with premarital sexual intercourse’ – reversed scored; Bizumic & Duckitt, 2018) measured RWA. Higher scores indicate stronger desires for social conformity and to submit to authority.
Ethnocentrism
A 6-item Ethnocentrism scale (α = .83; ‘I don’t believe that my ethnic group is any better than any other’ – reverse-scored; Bizumic, 2019) measured ethnocentrism in sample 2. Higher scores indicate a particularly high importance given to one’s own ethnic group.
Knowledge
A 10-item knowledge scale based on Thompson and Zamboanga’s (2004) 16-item Prior Psychology Knowledge Test was used to test prior knowledge of BPD in sample 1. The measure used a 5-point Likert-type scale, ranging from 1 (very sure it’s incorrect) to 5 (very sure it’ s correct). The 7-item BPD Knowledge questions (Cleary et al., 2002) was used in sample 2. Participants indicated if they agreed, disagreed, or did not know the answer for six statements related to BPD and selected the incorrect statement for the final question. The scale scores were calculated by totaling the item scores. Higher scores indicated greater knowledge of BPD (more detailed information is in Supplemental Material 4).
Social desirability
A shortened, 10-item version of the Marlow-Crowne Social Desirability scale (α = .65; Strahan & Gerbasi, 1972) assessed social desirability in sample 1. Participants indicated the accuracy of each statement on a Likert-type scale ranging from 1 (very inaccurate) to 5 (very accurate).
Results
Confirmatory factor analysis
Confirmatory factor analysis (CFA) was used to investigate the structures of the PPBPD and PPMI scales. The lavaan R package (Rosseel, 2012) was used for the analyses. Three models were tested for both the PPBPD and PPMI scales:
A one-factor model; all items loaded onto one factor.
A correlated three-factor model; items loaded onto the respective factors of Fear/Avoidance, Unpredictability, and Malevolence/Authoritarianism.
A correlated four-factor model; items loaded onto their respective factors.
The second model was designed based on a model indicated from the high correlation between the Malevolence and Authoritarianism subscales in sample 1, r = .65, p < .001. To account for method variance, a negative ‘method factor’ on which all reverse-scored items were loaded was included. The following fit indices and cut-off points were used to assess the model fit: CFI > 0.90, RMSEA close to or less than 0.06, and SRMR values of 0.08 or less (Tabachnick & Fidell, 2013). Model 3 had the best fit in all three samples (see Table 1), showing support for the four-factor structure for the PPBPD scale (Hypothesis 1). The four-factor structure of the PPMI was also replicated providing support for the structural validity of the scale.
Fit Indices of confirmatory factor analysis for the prejudice toward people with borderline personality disorder (PPBPD) and people with mental illness (PPMI) scales.
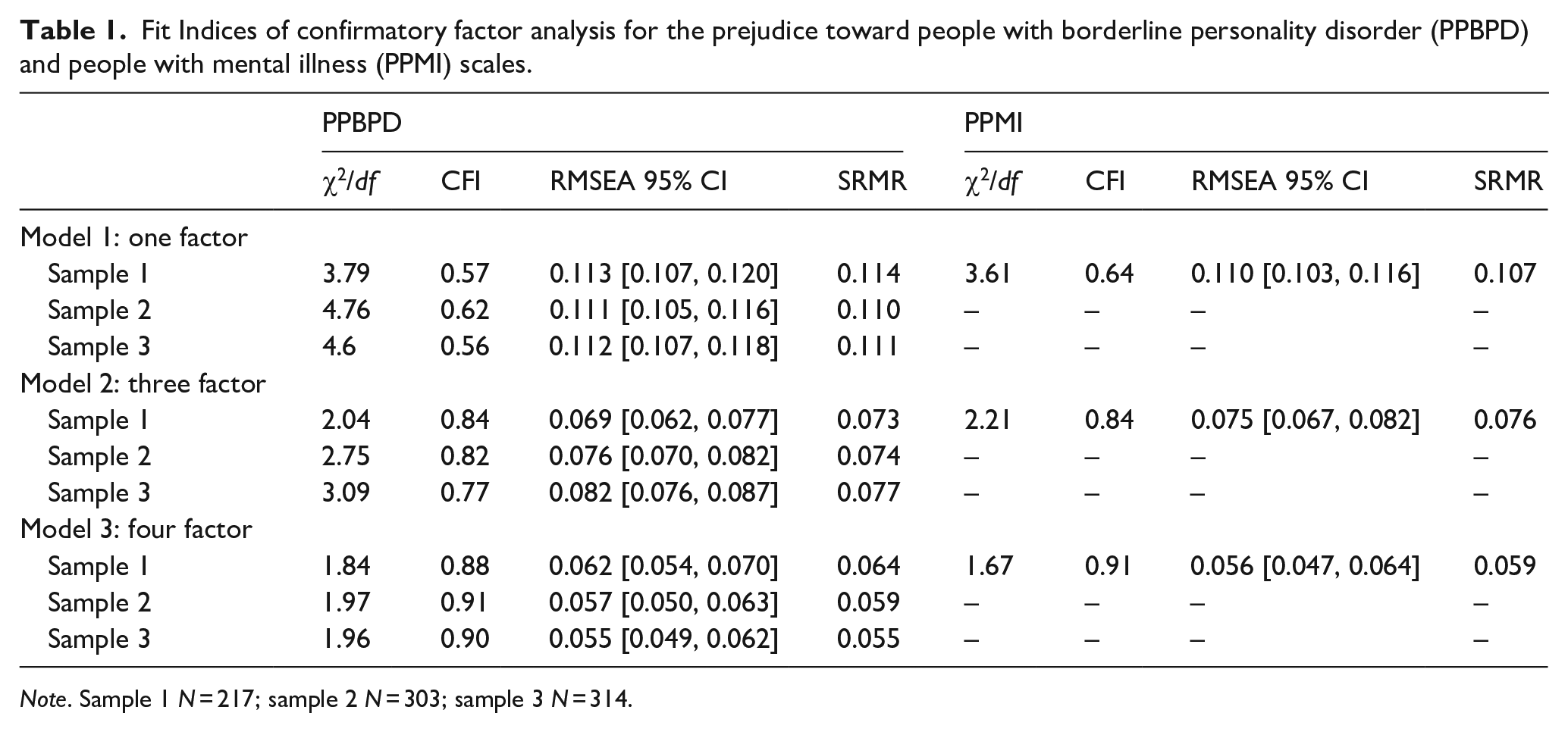
Note. Sample 1 N = 217; sample 2 N = 303; sample 3 N = 314.
No correlations between the subscales were strong enough to suggest merging factors; however, the correlation between the Malevolence and Unpredictability subscales was non-significant in sample 2 (see Figure 1). Factor loadings in all three samples were above 0.3 on their hypothesized factors (see Supplemental Material 3), except for one Malevolence item which had mixed size and significance level across the three samples. The item was retained because the item loading was statistically significant in all three samples. Significant correlations were also found between the factors of the PPBPD and PPMI scales in sample 1 (see Supplemental Material 5).
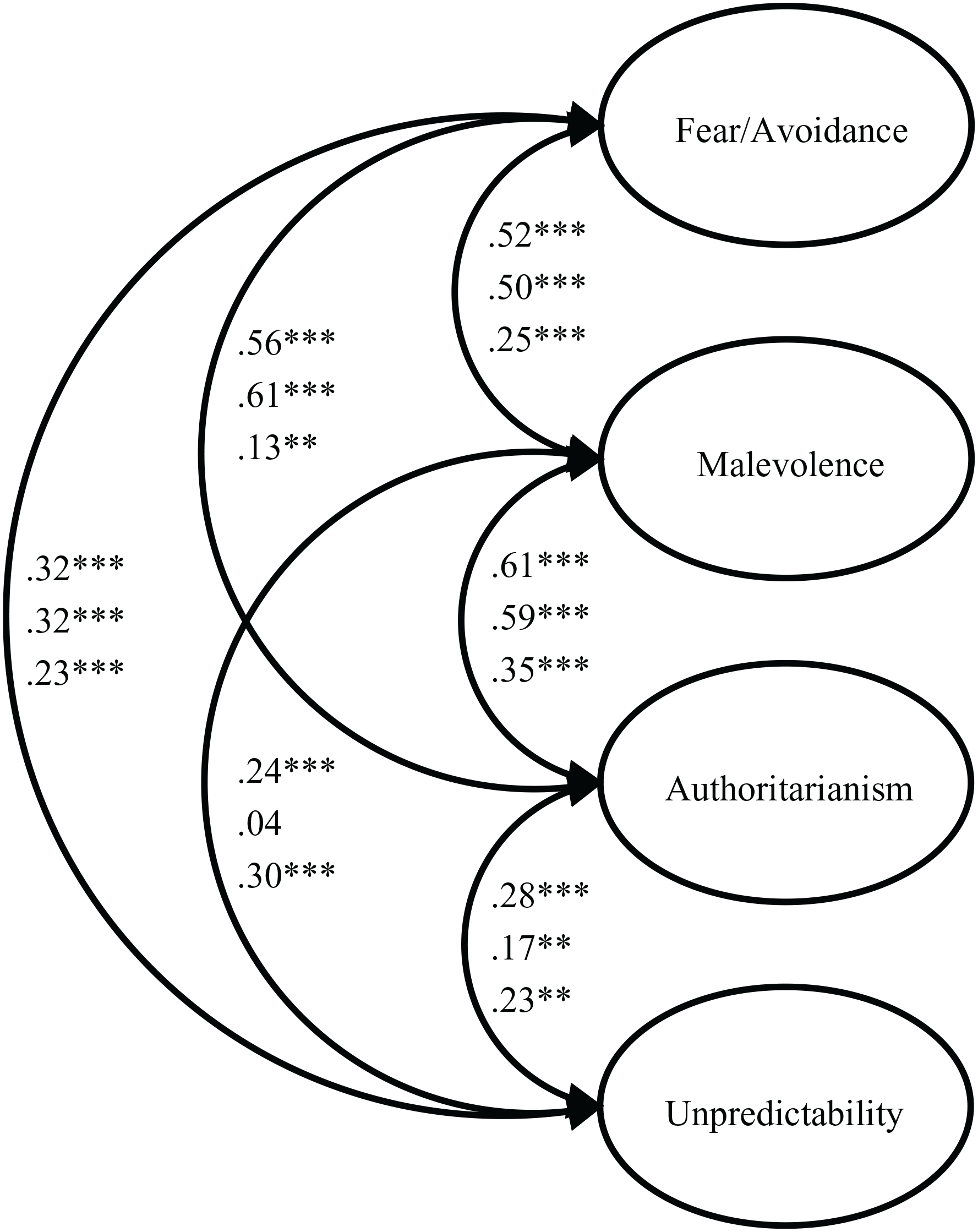
Intercorrelations between factors in the four-factor model of prejudice toward people with borderline personality disorder in each sample.
Comparison with prejudice toward people with mental illness
Hypothesis 2 was investigated by comparing the mean levels of reported prejudice in sample 1.Table 2 shows the means and standard deviations of the PPBPD, PPMI, and each subscale. Unpredictability was the highest scoring subscale for both scales. Prejudice toward people with BPD was more negative than toward people with mental illness across both total scales and the subscales. The largest mean difference was between the Fear/Avoidance subscales. A significant difference between the means was found for the total scales, t(216) = 18.28, p < .001, the Fear/Avoidance subscales, t(216) = 16.42, p < .001, the Malevolence subscales, t(216) = 17.39, p < .001, and the Unpredictability subscales t(216) = 11.04, p < .001. Nevertheless, there was no significant difference between the means of the Authoritarian subscales, t(216) = 0.39, p = .701. Table 2 shows prejudice toward people with BPD scores were most negative in sample 3 for the PPBPD scale and Fear/Avoidance, Malevolence, and Authoritarianism subscales, and most negative in sample 2 for the Unpredictability subscale. Malevolence attitudes were the least negative in samples 1 and 2, and Unpredictability attitudes were the least negative in sample 3.
Means and standard deviations of the PPBPD, PPMI, and subscales in all samples.
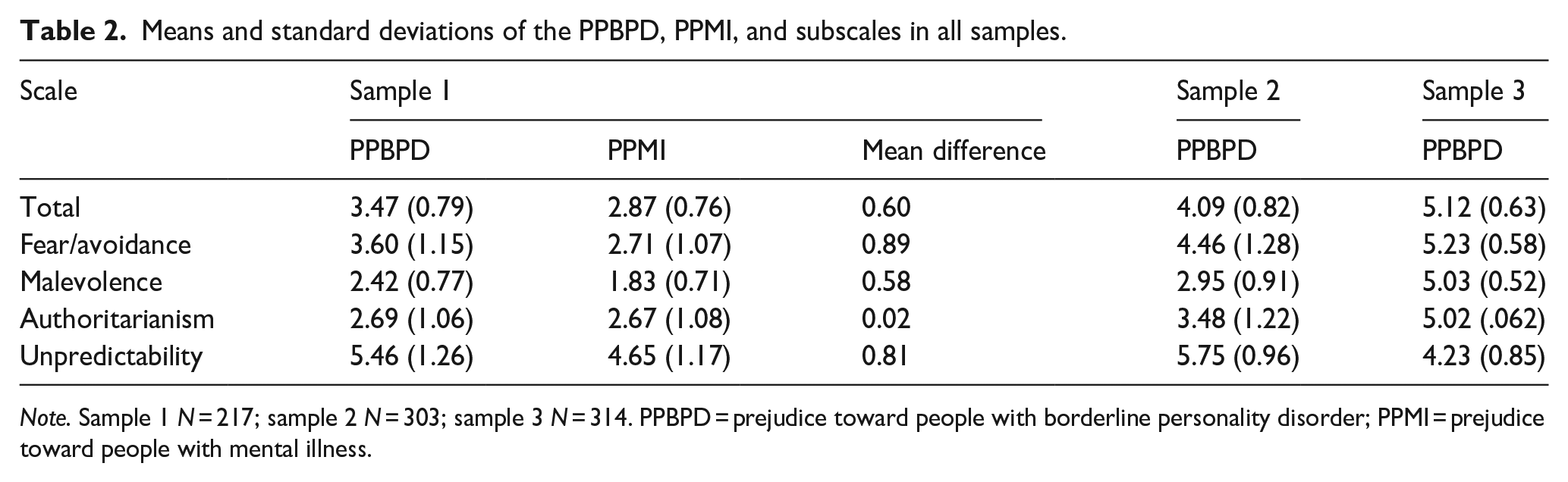
Note. Sample 1 N = 217; sample 2 N = 303; sample 3 N = 314. PPBPD = prejudice toward people with borderline personality disorder; PPMI = prejudice toward people with mental illness.
Correlations between prejudice and external variables
Correlation analysis investigated the nomological network of the PPBPD scale (see Table 3). The descriptive statistics and intercorrelations of the antecedents and consequences are in Supplemental Material 6. In partial support of Hypothesis 3, the PPBPD and the Fear/Avoidance, Malevolence, and Authoritarianism subscales related positively to SDO, RWA, ethnocentrism, and discriminatory behaviors. SDO had the strongest positive correlations with prejudice. Zero-order correlations, however, show the Unpredictability subscale did not significantly relate to any of these variables.
Zero-order (r) and semipartial (sr) correlations of the PPBPD and the subscales with antecedents and consequences in samples 1 and 2.
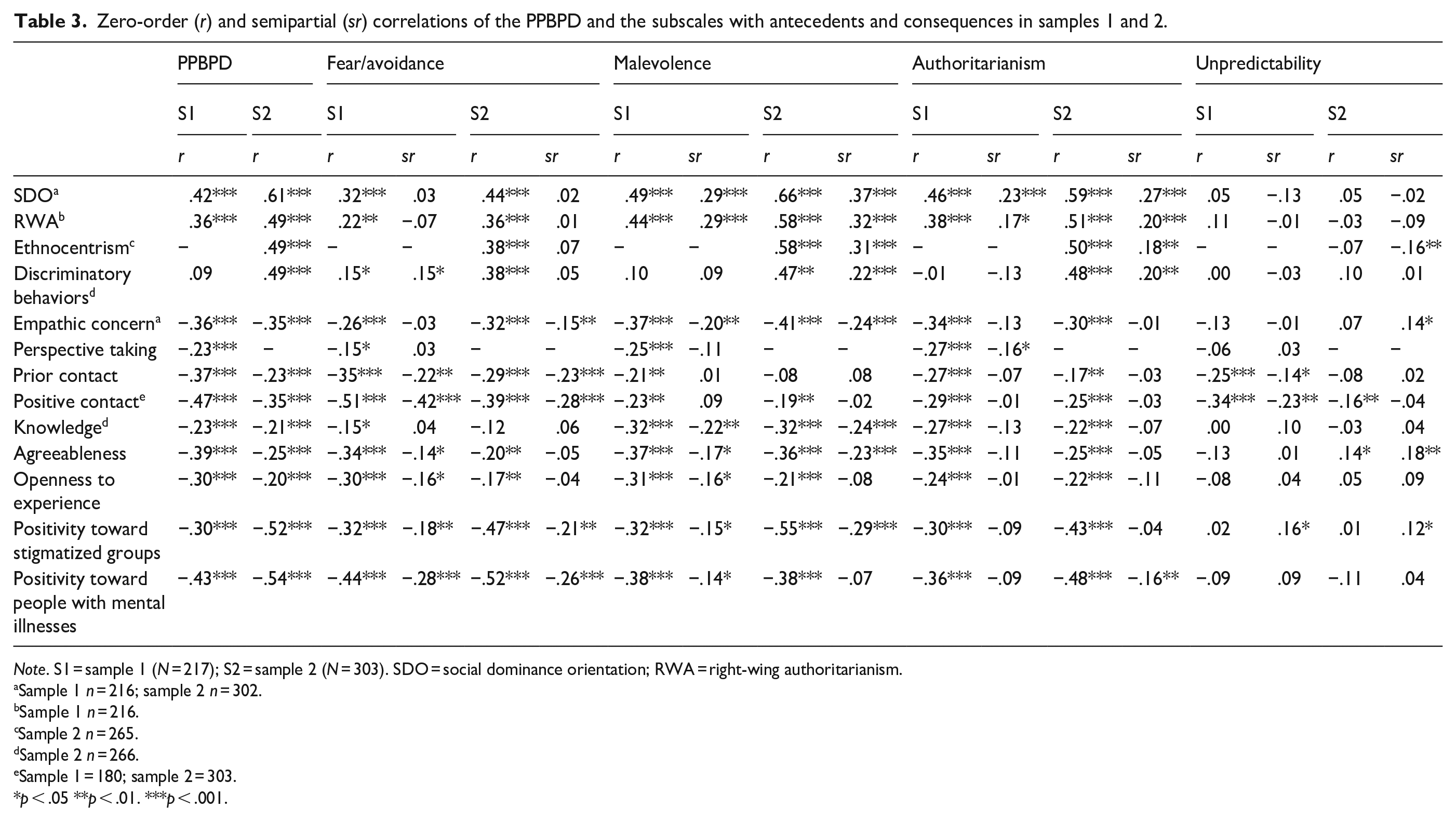
Note. S1 = sample 1 (N = 217); S2 = sample 2 (N = 303). SDO = social dominance orientation; RWA = right-wing authoritarianism.
Sample 1 n = 216; sample 2 n = 302.
Sample 1 n = 216.
Sample 2 n = 265.
Sample 2 n = 266.
Sample 1 = 180; sample 2 = 303.
p < .05 **p < .01. ***p < .001.
Most predicted negative relationships between the prejudice scales and empathy, prior contact, knowledge about BPD, agreeableness, openness to experience and positivity toward stigmatized groups and other mental illnesses emerged (Table 3), providing some support for Hypothesis 4. Again, the Unpredictability subscale did not relate as expected to these antecedents. It did have a moderate negative relationship with prior contact in sample 1, but this was not replicated in sample 2, and a positive, although very weak, relationship with agreeableness in sample 2. Moderate negative relationships were found between the remaining prejudice scales and these variables. Nevertheless, prior contact did not significantly correlate with Malevolence in sample 2, and knowledge had no significant relationship with Fear/Avoidance.
Analysis of semi-partial correlations investigated the unique relationships of each subscale of the PPBPD and the antecedents when controlling for the other three subscales. Fear/Avoidance had the strongest negative relationships with prior contact and positivity toward people with other mental illnesses. Malevolence had the strongest positive relationships with SDO, RWA, and ethnocentrism, and the strongest negative relationships with empathic concern and knowledge. Authoritarianism had the only significant correlation with perspective-taking.
Discussion
The current study aimed to test a new measure for prejudice toward people with BPD and place it within a nomological network. In support of Hypothesis 1, the four-factor structure of the PPMI scale was replicated in the PPBPD scale, suggesting prejudice toward people with BPD consists of the bipolar expressions of Fear/Avoidance, Malevolence, Authoritarianism, and Unpredictability. The factor structure was replicated in two samples, including a general population sample. To our knowledge, this is the first measure of prejudice toward people with BPD that can be used outside a healthcare population, and the first adapted measure that has been empirically tested and replicated.
Reported prejudice toward BPD was higher than toward people with mental illness in general, supporting Hypothesis 2. This is congruent with the results of previous research (e.g. Lawn & McMahon, 2015; Purves & Sands, 2009; Sheehan et al., 2016). Authoritarian attitudes were not significantly different, suggesting participants held similar views on controlling people with BPD and people with mental illness more generally. Malevolence was the lowest scoring dimension in both the PPBPD and PPMI scales in sample 1 and in the PPBPD in sample 2, with mean attitudes reflecting agreement with supportive items and rejection of prejudicial items. Malevolence was also found to be the lowest scoring dimension when measuring prejudice toward people with depression or schizophrenia (Bizumic & Gunningham, 2022). Almost all the scales were more negative in the general population sample (sample 3), compared to the university samples, suggesting the need for a prejudice scale suitable for use outside the health care provider setting to better assess and understand public prejudice.
In partial support of Hypotheses 3 and 4, prejudice and its expressions of Fear/Avoidance, Malevolence, and Authoritarianism all related positively to SDO, RWA, ethnocentrism, and discriminatory behavior, and negatively to measures of empathy, prior contact, knowledge about BPD, agreeableness, openness to experience and positivity toward stigmatized groups and other mental illnesses. This replicates the results of previous research exploring prejudice toward mental illness, depression, and schizophrenia (Bizumic & Gunningham, 2022; Kenny et al., 2018)
Contrary to Hypotheses 3 and 4, the only predicted relationship found in the Unpredictability expression was a negative relationship with prior contact in sample 1. Unexpected relationships between Unpredictability and ethnocentrism (negative), and empathic concern, agreeableness, and positivity toward other stigmatized groups (positive) emerged. The lack of significant associations between Unpredictability and the antecedents may be a function of the nature of BPD. Definitions of BPD often invoke thoughts of Unpredictability, e.g. ‘instability of self-image, personal goals, interpersonal relationships, and affects,. . .’ (Black et al., 2011, p. 460), potentially predisposing the negative Unpredictability items to be viewed as fact regardless of other reported prejudicial attitudes, personality types, or ideological beliefs. When measuring attitudes toward mental illness, depression, or schizophrenia, the Unpredictability dimension has related to these theoretically related variables (see: Bizumic & Gunningham, 2022). Further research to improve understanding of this phenomenon is required to appropriately approach reducing negative Unpredictability attitudes.
The convergent validity of the PPBPD is supported by associations between the dimensions of prejudice and the external variables. Positioning the PPBPD within a nomological network provides information about the development and outcome of these attitudes, and potential routes for reducing prejudice. The differential pattern of associations between each factor of prejudice and the antecedents and consequences suggests different paths of development and outcomes for each dimension.
The creation of the PPBPD measure has multiple practical implications. Adapting the PPMI allows for more direct comparison of prejudice toward different mental illnesses, which will improve clarity of the content of stigma and allow for integration across research. The PPBPD scale could be used across populations, allowing researchers to measure and compare community, carer, family, healthcare provider, and workplace attitudes. The present scale allows us to better measure, comprehend and address prejudice toward people with BPD. This can aid clinicians in understanding challenges faced by people with BPD and their own personal biases, leading to greater self-awareness and provision of more effective care. Additionally, it can help them better understand the prejudice held by other healthcare professionals, enabling them to educate their colleagues about difficulties that people with BPD face in both life and healthcare settings.
A greater understanding of the underlying expressions of prejudice can promote the development of more effective, targeted interventions. Application of the scale before and after interventions can help us understand their effectiveness across each dimension. Research supports that some interventions are more successful at tackling certain aspects of stigma than others (Modgill et al., 2014), suggesting value in understanding the specific dimensions of prejudice when designing and implementing different interventions. Interventions can be tailored to target each of the specific dimensions of prejudice toward people with BPD. For example, in this study Unpredictability only significantly related to contact, implying interventions that increase contact with people with BPD may have greater success reducing Unpredictability attitudes than other interventions, such as education programs. Accordingly, the PPBPD scale shows promise in developing better interventions aimed at reducing prejudice among the general public and clinicians.
Despite these implications, limitations of this study should be considered. First, the order of the PPBPD and PPMI measure in the survey of sample 1 may have impacted the mean comparison findings. Reading the description of BPD, and potentially completing the PPBPD, before completing the PPMI may have primed participants to reflect on BPD when responding to mental illness items. Second, the investigation of the nomological network only included correlational analysis. As such, we cannot imply causation or confirm external variables as antecedents or consequences. Future research may expand upon the nomological network, potentially identifying antecedents that are specific to prejudice toward people with BPD.
This study created a measure of prejudice toward people with BPD, validated its structure in three samples, and undertook a preliminary assessment of its nomological network. This new scale will enable prejudice toward BPD to be more accurately measured and will aid in identifying attitudes to target in future interventions to reduce the high levels of prejudice and discrimination faced by people living with BPD.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231155056 – Supplemental material for Prejudice toward people with borderline personality disorder: Application of the prejudice toward people with mental illness framework
Supplemental material, sj-docx-1-isp-10.1177_00207640231155056 for Prejudice toward people with borderline personality disorder: Application of the prejudice toward people with mental illness framework by Hannah Sheppard, Boris Bizumic and Alison Calear in International Journal of Social Psychiatry
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alison Calear is supported by an NHMRC Fellowship (1173146).
Ethical approval
Samples 1 and 2 were approved by the Australian National University Human Research Ethics Committee (Protocol: 2019/753). Sample 3 was approved by the Australian National University Human Research Ethics Committee (Protocol: 2020/345).
Data Availability
Following the study’s approved ethics protocol, the averaged data are available from the authors upon a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.