
Abstract
Background:
The role of physical activity (PA) in addressing mental health issues across the lifespan is expanding. Although the focus is primarily on the adult population, this underestimates the potential implementation of these complementary interventions in children and adolescents.
Aim:
We synthesize the outcomes of umbrella reviews addressing the effectiveness of structured PA on young people’s mental health.
Methods:
We searched the literature following the PRISMA-ScR methodology for systematic searches consulting the electronic databases of Pubmed, Cochrane Reviews Library, PsycINFO, and PsycArticles, with pre-established eligibility criteria.
Results:
We included 13 umbrella reviews, published from 2011 to 2023, comprising 91 systematic and meta-analytic reviews. Exercise is the most frequent form of PA (11/13), followed by sports (4/13), dance (3/13), and yoga (1/13). The most consistent positive effects of PA in this portion of the population concerned depressive symptoms, followed by anxiety symptoms. Promising effects were reported for attention, hyperactivity, and impulsivity. Other mental health-related outcomes that emerged as positively influenced by PA concern suicidal ideation, self-esteem, and social functioning, with positive effects of exercise and sport.
Conclusions:
We suggest that structured PA has promising effects on youth’s mental health although more evidence needs to be gathered. Indeed, although most of the umbrella reviews were of high quality, some methodological weaknesses of primary studies were noted, such as the large data heterogeneity, which, if not adequately addressed, can lead to results that underestimate the complexity of applying PA in clinical practice. Future RCT studies are needed to verify the effectiveness of rigorous PA programs on selected psychopathologies, allowing to expand the current evidence-based recommendations and guidelines, tailoring interventions comprising sport and physical activity to the specific needs of youth.
Keywords
Introduction
Mental health issues represent a significant challenge for young people. According to a recent estimate, one in seven youths experience a mental disorder (World Health Organization [WHO], 2024a). Prevalence rates of mental health problems increase from adolescence and, if not adequately treated, tend to persist into adulthood (Guddal et al., 2019). Indeed, the transition of young people from childhood (<11 years old) to post-adolescence (25 years old) has become fragmented and more at risk (Siurala, 2005). There is thus an urgent need for evidence-based targeted interventions that enable youth to adopt healthier behaviors that affect not only their current mental health, but also their future trajectories as adults.
Over the last few years, the international scientific community has acknowledged the intrinsic value of physical activity (PA) in supporting the mental health of individuals across the lifespan (Martín-Rodríguez et al., 2024; Stubbs et al., 2018). This interest has been propelled when acknowledging the devastating effects of social isolation experienced during the COVID-19 pandemic on the general population, indicating the need for additional policy interventions targeting the most vulnerable groups, especially the youth.
PA is defined as any ‘bodily movement produced by contraction of skeletal muscles and substantially increasing energy expenditure’ and it can be spontaneous (leisure activities/work/transport) or structured and differentiated by purpose (exercise/sport/dance/yoga; Corbin et al., 2000; Malm et al., 2019). Converging evidence recommends the use of structured PA in the primary prevention and clinical treatment of a spectrum of mental disorders in adulthood (Noetel et al., 2024). PA is an effective treatment for depression, with walking or jogging, yoga, and strength training more effective than other exercises, especially when intense (Hu et al., 2020; Noetel et al., 2024). A recent meta-review of lifestyle psychiatry has found that exercise reduces symptoms’ severity in patients with panic disorder, generalized anxiety disorder, post-traumatic stress disorder, and social phobia (Firth et al., 2020). Exercise was also found to significantly improve global cognition in patients with schizophrenia, highlighting its benefits in ameliorating positive and negative symptoms (Firth et al., 2020).
Regarding the youth population, although the evidence is still limited, a growing body of data suggests that structured PA could be effective for tackling and preventing both internalizing (mood disorders, anxiety-related symptoms, low self-esteem) and externalizing (conduct dysregulation, risky behavior, school truancy, and delinquency) problems in this target group (Ashdown-Franks et al., 2020; Boelens et al., 2022; Dale et al., 2019; Firth et al., 2020; Lynch et al., 2013; Nelson & Gordon-Larsen, 2006; Panza et al., 2020; Wegner et al., 2020). Poor mental health at an early age is associated with a lower quality of life and a higher risk of developing disabilities or chronic diseases, affecting the growth trajectories of children and adolescents (Merikangas et al., 2009; Patton et al., 2014; Petersen et al., 2023). Furthermore, youth social isolation represents a major risk factor for the onset of mental disorders (Almeida et al., 2021). By contrast, PA provides an opportunity to tackle psychosocial challenges linked to growth and development in a supportive environment, fostering social integration of young people, especially the most vulnerable ones (Boelens et al., 2022; Eime et al., 2013). Notwithstanding such knowledge, the provision of PA and compliance rates among youth are not promising (Dale et al., 2019; Shao & Zhou, 2023). More than 81% of adolescents worldwide do not achieve the recommended amount of PA and adherence gradually declines with increasing age (Guthold et al., 2020). To investigate this trend, the survey of ‘Health Behavior in School-aged Children’ study (HBSC) was carried out every 4 years in collaboration with the WHO Regional Office for Europe, collecting evidence on adolescents aged 11, 13, and 15 years across 44 countries and regions in Europe, Central Asia and Canada. Only 25% of boys and 15% of girls achieved 60 min of moderate-to-vigorous physical activity every day and nearly three-fifths of adolescents met the WHO recommendation for vigorous physical activity at least three times a week (Rakić et al., 2024). In Italy, this scenario is particularly evident, since Italian youths show a lower prevalence of moderate to vigorous PA compared to those of other countries (Italian, 10% vs. international, 19%), as reported by the Italian HBSC 2018 results (Pierannunzio et al., 2022). In addition, Italian HBSC data updated to 2022 confirmed the worrying gender gap, with girls engaging in less daily PA than boys (Gruppo di Coordinamento HBSC-Italia, 2022). Overall, the available data suggest that the need to reverse youth sedentary trends and increase participation in structured PA should remain a focus of interventions in schools, families and the community. Thus, it is of paramount importance to relate the most consistent data so far gathered on the use of PA for youth mental health promotion and intervention to rapidly inform current evidence-based guidelines and recommendations for professionals in health services, youth organizations, sports clubs, and schools so that they can translate this knowledge into practice.
However, the current scientific literature focuses more on the adult population, underestimating the potential that these types of complementary interventions can have when started at an early age. The objective of this review is therefore to synthesize umbrella reviews assessing the effects of structured PA on youth’s mental health outcomes.
Methods
The present review of umbrella reviews adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist (see Supplemental Material S1; Tricco et al., 2018) and was pre-registered to PROSPERO, the international prospective register of systematic reviews and meta-analyses (id. CRD42024539718). The research team included at least one member with methodological experience in conducting reviews (CC) and at least two members with expertise in the research topic (BC, FC, and GS).
Literature search and study selection
The search for relevant literature was conducted on April 24th 2024, consulting the electronic database of Pubmed, Cochrane Reviews Library, PsycInfo, and PsycArticles. Moreover, backward citation search was manually conducted. The complete research strategy with the combination of specific keywords was reported in the Supplemental material S2. The following eligibility criteria were applied: the studies had to be (1) umbrella reviews published in English and in peer-reviewed journals; (2) they had to address the effects (positive, negative, or not significant) of structured PA (specifying the type of PA employed e.g., exercise, sport, dance, or yoga) for prevention or treatment of specific mental health outcomes (e.g., depressive and anxious symptoms) and not generic ones (e.g., psychological symptoms, mental well-being); and (3) the target population had to be youth.
In the present work, we referred to the WHO definition of mental health as a state of mental well-being and no longer considered as the mere absence of mental disorders; it exists on a complex continuum, which is experienced differently by everyone, with varying degrees of difficulties and potentially different social and clinical outcomes (WHO, 2022).
Different types of structured PA are considered eligible: exercise is a ‘planned, structured and repetitive bodily movement’ aimed primarily at improving health and physical capacity (Caspersen et al., 1985); sport is defined as a subset of exercise, characterized by a common set of rules and a defined goal, and it can be undertaken individually or as a part of a team (Khan et al., 2012); dance is commonly defined as a form of performance art characterized by rhythmic movements and sequences of steps set to music (Mansfield et al., 2018); yoga is an ancient discipline that includes various practices such as posture exercises, balance exercises, deep breathing exercises, and techniques for meditation and relaxation (Khalsa & Butzer, 2016).
Given the extensive and complex nature of the transition process from childhood to adulthood, we referred to the European Youth Policy Council definitions (Siurala, 2005) for the inclusion of our target population: children <11 years; early adolescence 12 to 17 years; adolescence 18 to 24 years; post-adolescence 25 years.
We chose to select umbrella reviews as they represent one of the highest levels of scientific evidence and can summarize the results of multiple existing systematic reviews or meta-analyses, allowing easy comparison of key findings.
After completing the literature search and duplicate removal, two reviewers (BC and CC) independently proceeded to select the emerging records by first consulting the title and abstract and then the full text, applying the eligibility criteria. All disagreements about the eligibility of an article were solved by the evaluation of a third reviewer (FC).
Data extraction
From the full-text of included studies, the following data were independently extracted by two reviewers (BC and CC) and collected in a first systematic table: (1) bibliographic details (author[s] and year of publication, and journal); (2) aim of the umbrella review; (3) the number of reviews included and subjects’ characteristics; (4) PA characteristics; and (5) mental health outcomes and overall results. If an umbrella review contained findings about different interventions (e.g., psychological treatment) and/or the adult population, only the data about structured PA and youths were scrutinized and extracted.
Moreover, a second table was reported to summarize the effects (positive/negative/not significant) of several types of structured PA on specific mental health outcomes, indicating the effect size and the quality of evidence reported in the umbrella reviews included.
Based on the extracted data, the frequencies of the diverse types of structured PA employed and the specific mental health outcomes investigated were calculated, as well as for each mental health outcome the effects (positive, negative, and not significant, expressed as percentages) of the diverse types of structured PA.
The two reviewers checked for discrepancies and, if necessary, consulted a third reviewer (FC) to reach a final decision.
Assessment of methodological quality
The methodological quality assessment of the included umbrella reviews was conducted by using the JBI checklist for the critical appraisal of systematic reviews and research syntheses (Aromataris et al., 2015). The checklist displays eleven items evaluating different methodological aspects of a systematically conducted review, including the appropriateness of the search strategies and sources, the critical appraisal methods, the approach to data extraction and synthesis, potential sources of publication biases, and recommendations for policy, practice and future research. One point was assigned to each item that obtained an affirmative answer. Thus, the overall score of an umbrella review can range from zero to eleven (low-quality: from zero to four points; medium-quality: from five to seven points; high-quality: from eight to eleven points; Hossain et al., 2022). Two reviewers independently performed the methodological quality assessment (BC and CC). In case of disagreements, a third reviewer was consulted (FC).
Results
Study selection
The study selection process is reported in Figure 1 through the PRISMA 2020 flowchart. The literature search produced 262 records, and after removing books, electronic collections, dissertations, and duplicates, 208 records were screened by title and abstract, excluding 171 records. Of the remaining records, 37 full-text records were retrieved and assessed for eligibility. After the full-text screening, 13 umbrella reviews were included.
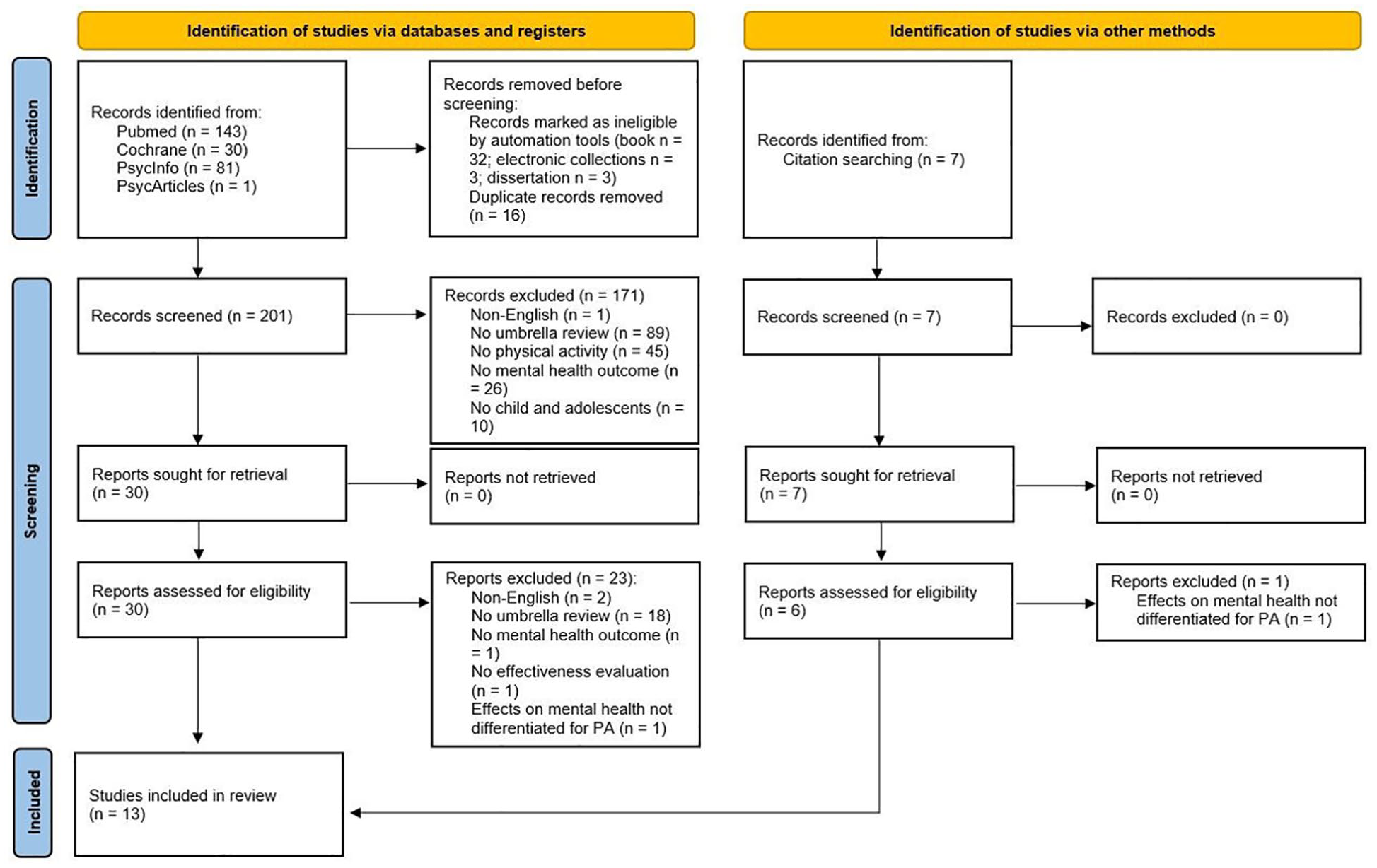
Flow chart of the literature search and selection process.
Study characteristics
The 13 umbrella reviews, published from 2011 to 2023, collected, and analyzed the results of 91 systematic and meta-analytic reviews that assessed the effects of structured PA on mental health in the young population (Table 1). They included both female and male participants, including youth from 3 to 25 years (Table 1). Other relevant sociodemographic data of the young participants were not systematically reported in the included umbrella reviews, and only a few of them provided information on ethnicity and socioeconomic status (see Supplemental Material S3). The umbrella reviews covered different types of structured PA: exercise, intended as planned, repetitive PA performed on a regular schedule (chronic) with deliberate intention and with different intensity levels (i.e., low, moderate and vigorous); sport, intended as organized, adult-supervised, role-based PA performed regularly on an individual or team basis; dance intended as the execution of body movements to the rhythm of music, focusing on the expressive rather than executive dimension; and yoga intended as performing planned PA (e.g., posture, balance, breathing exercises) for meditation and relaxation. Exercise (e.g., aerobics, resistance, weight, fitness) is the most common category of structured PA (11/13), followed by sports (4/13), dance (3/13), and yoga (1/13). Regarding mental health outcomes, depressive symptoms are the most investigated (10/13), followed by anxiety symptoms (8/13) and attention deficit hyperactivity disorder (ADHD)-related symptoms (attention, hyperactivity, impulsivity, and behavioral functioning; 3/13). Other mental health outcomes are reported in the umbrella reviews such as self-esteem (7/13), social functioning (3/13), and suicidal ideation (1/13).
Characteristics of the included umbrella reviews.
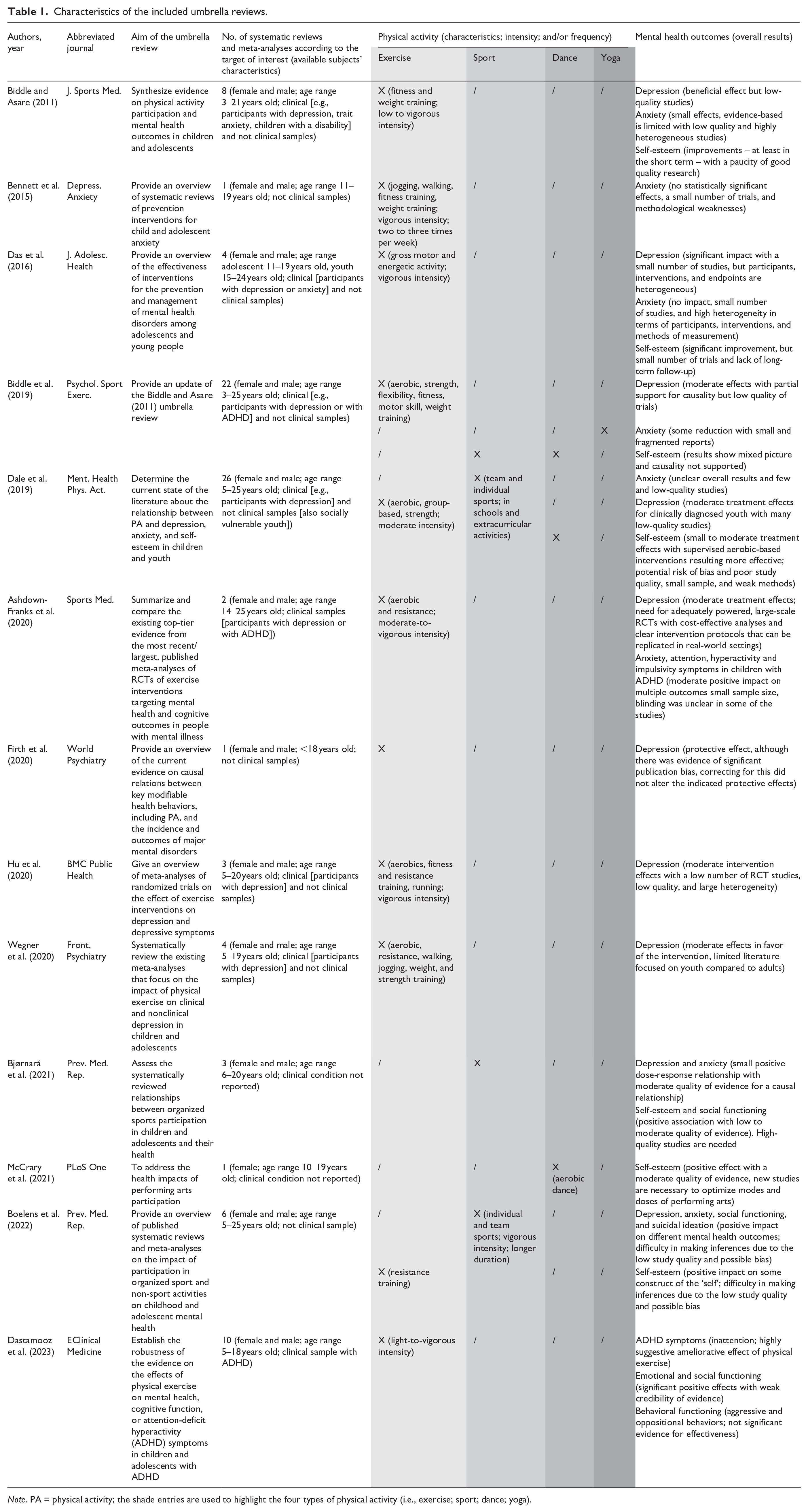
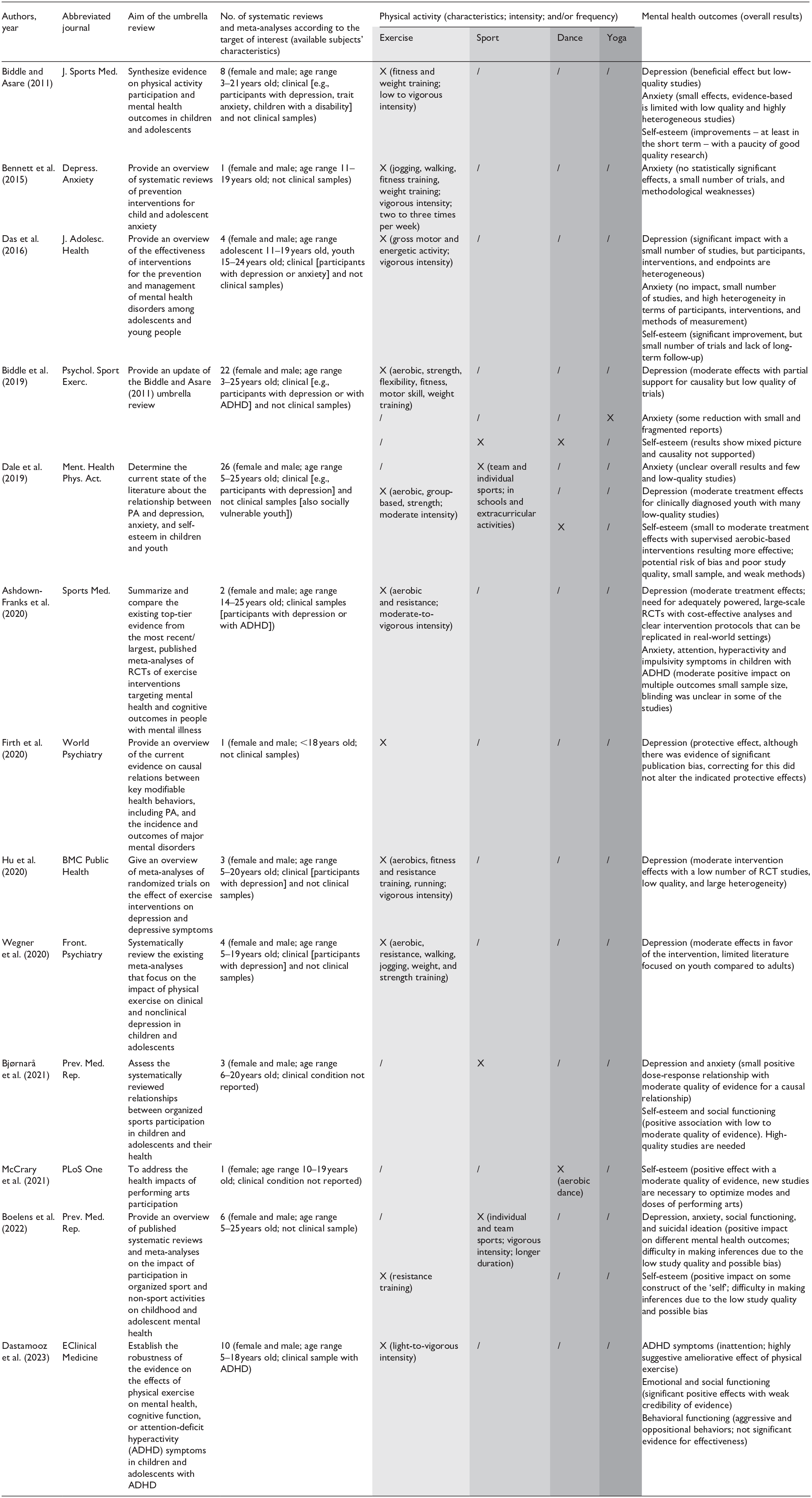
Note. PA = physical activity; the shade entries are used to highlight the four types of physical activity (i.e., exercise; sport; dance; yoga).
Effects of structured physical activity on specific mental health outcomes
The effects of specific structured PA on mental health outcomes are reported in Table 2. Physical exercise is associated with positive effects on depressive symptoms (8/8, 100%), attention, hyperactivity and impulsivity symptoms (2/2, 100%), self-esteem (4/4, 100%), and social functioning (1/1, 100%); mixing effects are reported for anxiety symptoms (2/4, 50% positive effects and 2/4, 50% not significant effects); not significant effects are reported for behavioral functioning of children with ADHD (1/1, 100%). Sport is associated with positive effects on depressive symptoms (3/3, 100%), self-esteem (3/4, 75%), social functioning (2/2, 100%), suicidal ideation (1/1, 100%), and to a lesser extent on anxiety symptoms (2/3, 66.7% positive effects and 1/3, 33.3% not significant effects). Dance is associated with promising effects on self-esteem (2/3, 66.7% positive effects and 1/3, 33.3% not significant effects). Lastly, yoga shows positive effects on anxiety symptoms (1/1, 100%).
Results on the effects (positive, negative, or not significant) of specific types of structured physical activity on each mental health outcome.
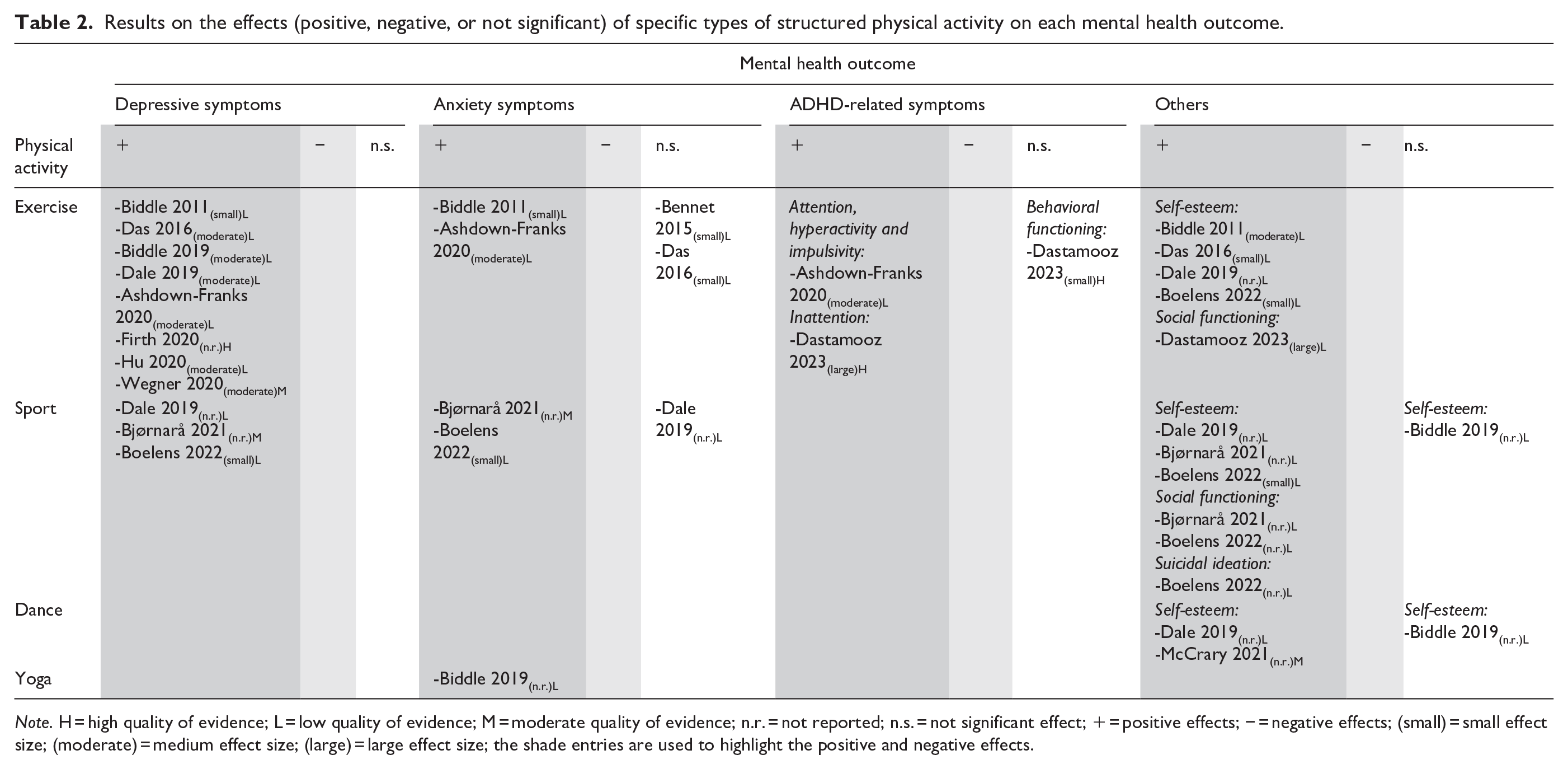
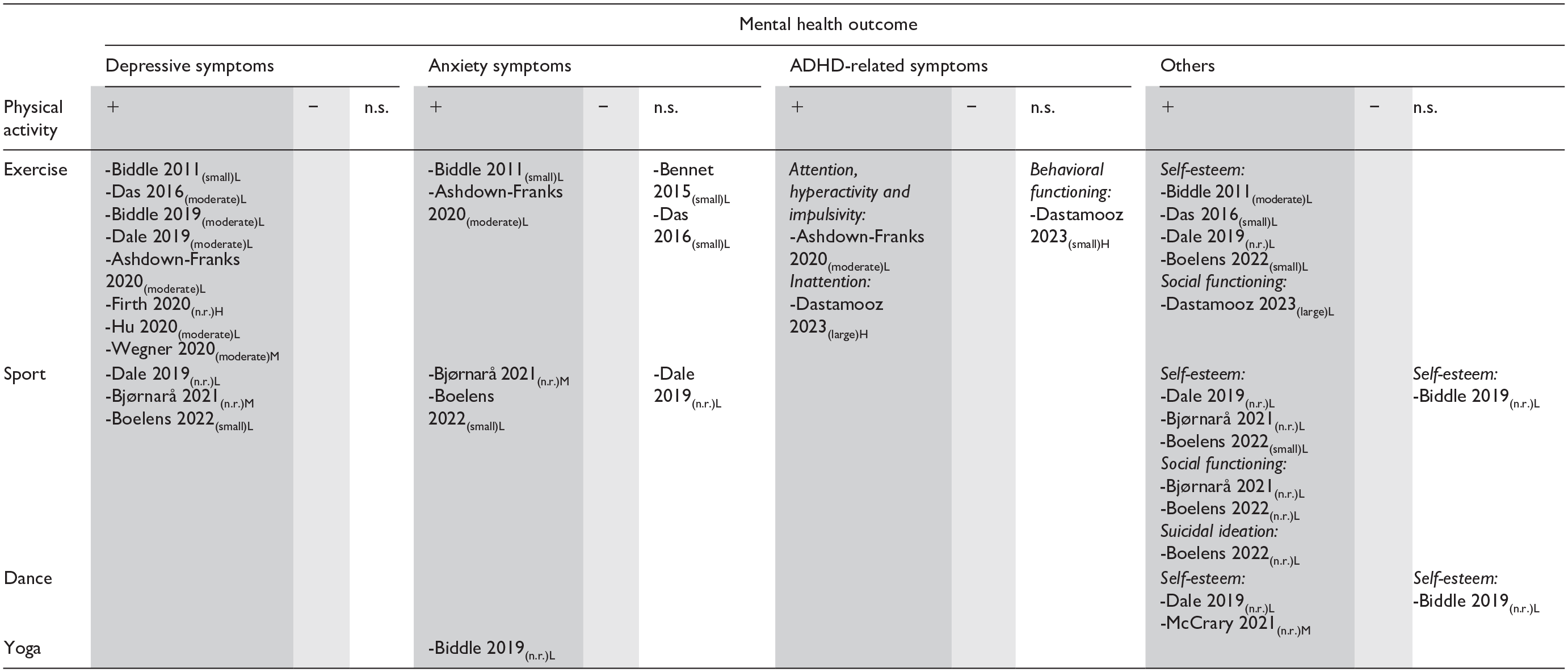
Note. H = high quality of evidence; L = low quality of evidence; M = moderate quality of evidence; n.r. = not reported; n.s. = not significant effect; + = positive effects; − = negative effects; (small) = small effect size; (moderate) = medium effect size; (large) = large effect size; the shade entries are used to highlight the positive and negative effects.
Overall, the effects are small-to-large with mixed quality of evidence (from low to high), due to the limited number of high-quality studies, small samples with a great variety of participants, and methodological weakness (heterogeneity of interventions and methods of measurement; Tables 1 and 2).
Methodological quality of included umbrella reviews
The results of the critical appraisal of the included umbrella reviews are reported in Table 3. The majority of the umbrella reviews (11/13) received a high-quality rating, while only two received a medium-quality rating. All the umbrella reviews reported a clearly stated review question with appropriate inclusion criteria, resources for literature search and directives for future research. Nearly all the umbrella reviews had an appropriate search strategy (10/13), criteria for appraising review (12/13), methods for combining studies (10/13), and assessment of publication bias (10/13). Only 9 out of 13 umbrella reviews clearly stated that the critical appraisal was conducted by two reviewers independently. Not all the umbrella reviews (9/13) used appropriate methods to minimize errors in data extractions. Finally, only 3 umbrella reviews provided clear recommendations for policy and practice.
Results of the quality assessment of the included umbrella reviews.
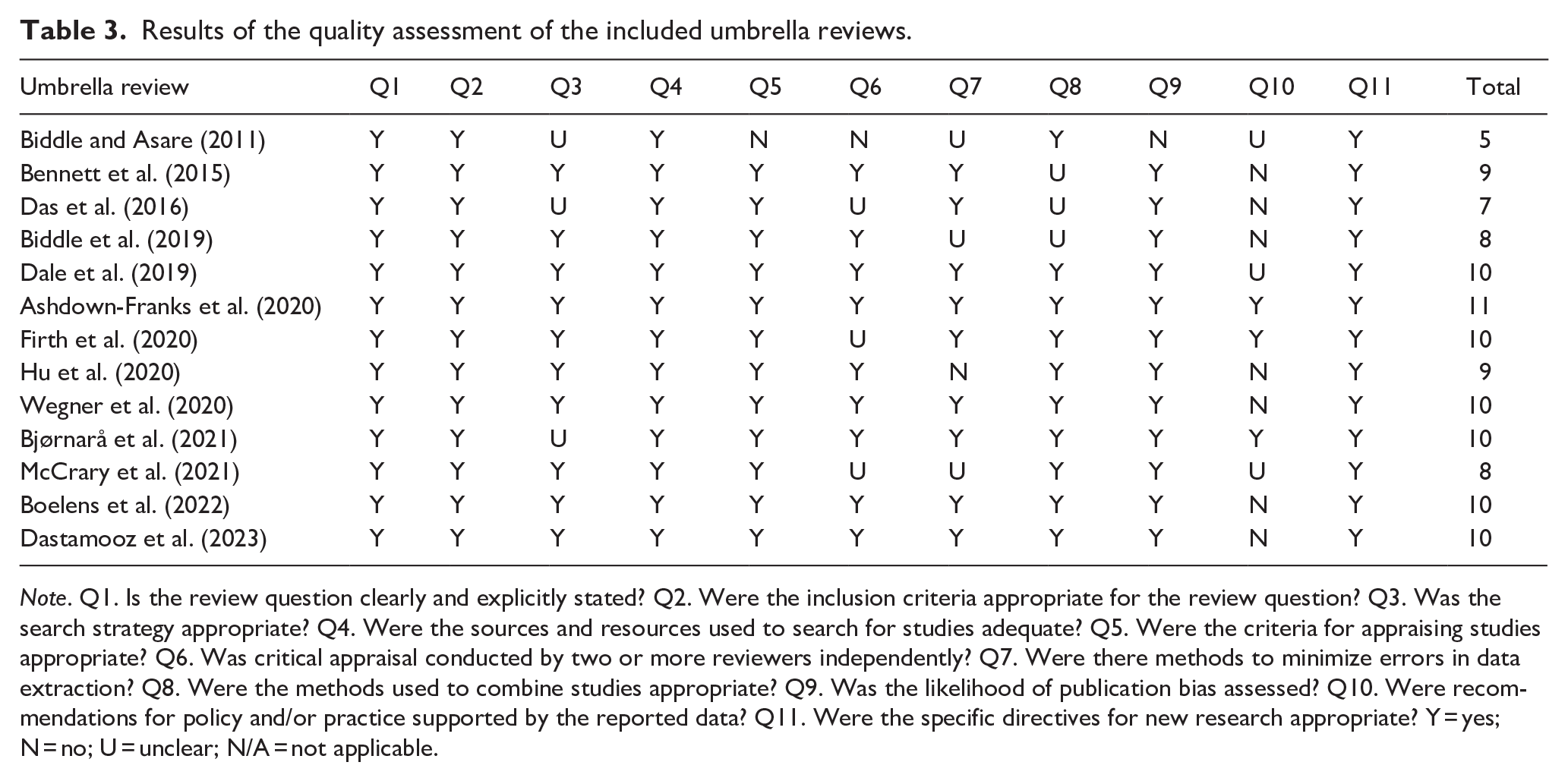
Note. Q1. Is the review question clearly and explicitly stated? Q2. Were the inclusion criteria appropriate for the review question? Q3. Was the search strategy appropriate? Q4. Were the sources and resources used to search for studies adequate? Q5. Were the criteria for appraising studies appropriate? Q6. Was critical appraisal conducted by two or more reviewers independently? Q7. Were there methods to minimize errors in data extraction? Q8. Were the methods used to combine studies appropriate? Q9. Was the likelihood of publication bias assessed? Q10. Were recommendations for policy and/or practice supported by the reported data? Q11. Were the specific directives for new research appropriate? Y = yes; N = no; U = unclear; N/A = not applicable.
Discussion
This review aims to synthesize umbrella reviews evaluating the effects of structured PA on young people’s mental health outcomes and compare results with current evidence-based guidelines and practice recommendations for youth mental health promotion and intervention.
The literature on the role of structured PA in improving young people’s mental health focuses on depressive symptoms (10/13 umbrella reviews). Research has increased significantly since the first umbrella review was published in 2011 (Biddle & Asare, 2011; Biddle et al., 2019). Early evidence on the youth population demonstrated the inverse association between exercise and depression but compared to literature on the adult population, the causal link between the variables could not be established due to low-quality studies, most of them with cross-sectional designs (Biddle & Asare, 2011). More recent reviews report that exercise programs have comparable effects with psychosocial interventions in reducing depressive symptomatology in youth (Das et al., 2016). The greatest effectiveness is found in children and adolescents clinically diagnosed with depression (participants with depression effect size = −0.43 to −0.61 vs. healthy samples effect size = −0.26 to 0.52; Biddle et al., 2019). Despite the overall positive results regarding diverse types of PA, supervised aerobic-based group exercise with moderate-to-vigorous intensity, engaged in multiple times per week over at least 7 to 8 weeks (about 2 months), is the most widely used intervention (Dale et al., 2019; Wegner et al., 2020). Regarding sports participation, dose-response studies are needed because levels of involvement (intensity or frequency) have not been described in detail (Bjørnarå et al., 2021; Boelens et al., 2022). A recent meta-analysis of randomized controlled trial (RTC) studies has reported that, compared with individual exercise (e.g., running or walking), team sports or group forms of exercise can help young people with depression relieve symptoms more promptly (Zhang et al., 2023). Interpersonal relationships, peer support, and guidance from sports professionals in group PA can represent some of the elements improving the levels of anhedonia and lack of motivation, promoting communication and social inclusion (Zhang et al., 2023). A recent RCT involving adolescent inpatients found that PA intervention is effective in reducing symptoms of depression and in promoting the establishment of a therapeutic alliance (Philippot et al., 2022). From a preventive perspective, umbrella reviews have revealed the value of sports in reducing the risk of suicide, which is often associated with depressive conditions (Boelens et al., 2022). Importantly, a 5-year longitudinal study reported that young people involved in team sports from middle school onwards were less likely to have suicidal ideations (including both thoughts and intentions) during high school than young people who never participated in sports (Taliaferro et al., 2011).
The results of the umbrella reviews on depressive symptomatology are in line with the general recommendation by the WHO to promote PA in children and adolescents (5–17 years old): young people should practice at least 60 min of moderate-to vigorous-intensity PA daily to reduce the severity of depressive symptoms (WHO, 2010, 2020). These recommendations were supported also by American and Canadian Guidelines for PA (Piercy et al., 2018; Sampasa-Kanyinga et al., 2022). Daily PA should include aerobic exercises (most of the 60 min, with vigorous intensity at least 3 days a week) as well as muscle- and bone-strengthening activities (as part of the 60 min at least 3 days a week; Piercy et al., 2018; Sampasa-Kanyinga et al., 2022; WHO, 2010, 2020). The American Guidelines provide a detailed classification of recommended PA (e.g., planned exercise, sports, play, games, transportation, active recreation) according to their intensity (Piercy et al., 2018). The guidelines issued by the National Institute for Health and Care Excellence (NICE) of the United Kingdom suggest that young people with depression should be encouraged to follow a structured, supervised PA program that typically involves up to 3 weekly sessions of moderate duration (45 min–1 hr) between 10 and 12 weeks (National Institute for Health and Care Excellence, 2019). Spanish guidelines emphasize the importance of accounting for patient preferences when recommending the type of PA program associated with the treatment plan and assessing whether the severity of the clinical picture does not prevent its implementation (Ministerio de Sanidad y Consumo, 2018). Indeed, severe depressive symptoms can interfere with a young person’s ability to adhere to PA recommendations, and attention must be paid that this does not induce feelings of guilt and failure (Campisi et al., 2021).
Compared with the literature on depression, the umbrella reviews have highlighted only preliminary findings on the anxiolytic effect of structured PA, concerning sports, and yoga. The evidence does not seem to have expanded in recent years and remains fragmented, both for intervention and prevention studies, with insufficient details on the intensity and frequency of PA and with a high heterogeneity in the participants (e.g., characterized by clinical anxiety, ADHD symptoms or no overt psychopathology; Biddle et al., 2019; Bjørnarå et al., 2021; Boelens et al., 2022; Dale et al., 2019). Sports, through the enhancement of social relationships and community participation, could help prevent anxiety symptoms (Boelens et al., 2022; Panza et al., 2020). In addition, the available data suggest a beneficial effect of yoga in anxiety management and emotional regulation, due to the added value of breathing and body awareness exercises that are known to reduce arousal (Biddle et al., 2019; Carter et al., 2021).
No guidelines on effective structured PA programs for anxiety management in young clinical populations have been devised, due to limited evidence. However, mindfulness-based PA interventions have been devised showing a good degree of improvement in symptomatology (James-Palmer et al., 2020). New and larger RCT studies, with clinical samples and well described methodologies, are needed to enable the development of official recommendations, which are especially needed as anxiety is one of the most frequently reported mental health problems among children and adolescents.
Over the past 20 years, a growing body of evidence has focused on the effects of structured PA on the young population with ADHD (Ashdown-Franks et al., 2020; Dastamooz et al., 2023; Purgato et al., 2024; Réol, 2024). The umbrella reviews included in the present work highlight the positive effects of exercise on core symptomatology (attention, hyperactivity, and impulsivity), as well as anxiety and social functioning (Ashdown-Franks et al., 2020; Dastamooz et al., 2023). No significant effects were noted on specific indices of behavioral functioning, such as aggressive and oppositional behaviors (Dastamooz et al., 2023). The mechanism behind the positive effects has not yet been determined, however, exercise could benefit children by supporting brain development and maturation (Dastamooz et al., 2023; Réol, 2024). It has also been suggested that participation in exercise interventions can promote a positive learning experience, fostering social interactions, self-regulation mechanisms, and the employment of physical skills, that require attention and inhibition of irrelevant stimuli, thus counteracting the main ADHD symptomatology (Dastamooz et al., 2023). Despite the interesting results, the mixed quality of the evidence does not allow for clear conclusions on effectiveness (Réol, 2024). Considering the significant increase in the number of children diagnosed with ADHD, and the general reluctance to administer drug therapies at a young age, it is necessary to plan new studies that clearly identify areas of efficacy, with specific recommendations on the proper dose-response balance, to develop specific guidelines on the use of exercise for improvements on ADHD-related symptoms.
Adopting a broader perspective that considers mental health not only as the absence of disorder-related symptoms but as a state of well-being experienced differently by each individual with different social and clinical outcomes (WHO, 2022), it is important to note that the collected umbrella reviews report interesting results on other mental health-related outcomes (self-esteem and social functioning), that complement those more specifically related to the clinical symptomatology. Indeed, the umbrella reviews support the notion that participation in PA can help young people improve their mental health through increased levels of self-esteem, with positive effects of exercise, sport, and dance. The scientific evidence on the topic has gradually increased over time, showing a complex picture: the literature on the young population supports the strength and coherence of the association between exercise and self-esteem, although causality is only partially supported. This is due to the low quality of the available evidence. In addition, the heterogeneity of definitions of self-esteem within the studies contributes to mixed results. Self-esteem refers to evaluations of one’s significance or worth as an individual and it can be considered a multidimensional and hierarchical construct, with a global dimension at the apex of context-specific subdomains such as physical self-worth (e.g., perceived competence or body attractiveness), emotional self-worth, social self-worth, and academic self-worth (Fox & Corbin, 1989). In this regard, the strongest evidence of effectiveness has been found for the subdomain of physical self-worth and for aerobic exercise, which seems to be a more promising intervention tool than sports (Dale et al., 2019). In the case of sport, its competitive characteristic implies the possibility of losing, and this can have negative repercussions on the youngsters’ self-esteem; to avoid this, coaches should emphasize the opportunity for growth that derives even from a result that does not correspond to expectations (Spruit et al., 2016). Interestingly, data indicate that creative dance may be an appropriate activity for children and adolescents, with and without mental disorders, to empower relevant aspects of the self (Schwender et al., 2018). Creative dance is based on the processes of movement exploration and improvisation, and on cooperative work that nevertheless allows for self-expression with performance modes based on physical abilities and individual preferences (Schwender et al., 2018).
Despite promising preliminary evidence, there is still variability in the effects of sports and dance, which may be attributable to the influence of possible moderators, such as participants’ sociodemographic characteristics (e.g., gender, social background, or family environment) and intervention settings (e.g., school/gym, detention facilities, clinical, or recreational environments). However, due to the limited data reported, it is difficult to account for the moderation effects on the effectiveness of sports and dance. Preliminary moderator analyses suggest that, in general, structured PA can equally affect the self-esteem subdomains of different young populations (e.g., typically developing, with disabilities, socially vulnerable, overweight), with some differences by sex and age (Dale et al., 2019). In particular, positive effects on physical self-worth seem to be more pronounced in boys than in girls, while those on perceived competence and body attractiveness increase as adolescence progresses (Babic et al., 2014; Dale et al., 2019). Despite these interesting findings, there are no conclusive recommendations on how to plan structured interventions, pointing to the importance of increasing knowledge on the areas most affected by PA, allowing to extend current guidelines also to include psychological domains related to self-esteem, which are fundamental for mental health and quality of life.
Social inequalities, discrimination, poverty, and growing up in dysfunctional families or environments can increase the likelihood of early adverse experiences, putting the mental well-being of children and adolescents at risk (WHO, 2024a). The umbrella reviews reported some evidence that social functioning can be improved by sports, although data are limited. The recommendations of the ‘National Youth Sports Strategy’ highlight that the sports environment fosters bonding among team members, provides opportunities to work with others to achieve common goals, and increases perceptions of social acceptance, allowing youth to experience community integration (Logan et al., 2019; U.S. Department of Health and Human Services, 2019). Sports participation is associated with positive social outcomes, including greater positive affect and learning social skills (e.g., effective communication, conflict resolution, and empathy), which are important determinants of mental health (Babiss & Gangwisch, 2009; Eime et al., 2013; Logan et al., 2019). In this regard, good practices have been put in place to prevent social exclusion, enhance social functioning, and promote the mental well-being of vulnerable children and adolescents through programs based on team sports. As an example, team sports (e.g., ice hockey, soccer, and floorball) are the core of Icehearts’ program, which is an evidence-based and successful practice from Finland (Appelqvist-Schmidlechner et al., 2023). The players in the team are gradually selected between the ages of 6 and 12 among children who need special support or who are at risk of social exclusion. Once established, the team of about 20 children remains together for 12 years under the supervision of a professionally qualified coach (Icehearts mentor) who provides long-term support. The results of the program show that team sports provide an opportunity for social connectedness as well as the development of self-regulation and coping skills that positively influence mental health (Appelqvist-Schmidlechner et al., 2023). A dedicated team spirit and a positive coaching attitude are considered crucial for the achievement of the above-mentioned results. Coaches play a key role in creating and maintaining a supportive environment in which young people can have meaningful and balanced sporting experiences, as well as find support, emotional security, and caring (Appelqvist-Schmidlechner et al., 2023). This underlines the importance of considering the expertise and training of the multidisciplinary working team involved in the PA program, as they could influence the effectiveness of the intervention.
Previous data suggest that children and adolescents may feel more comfortable with sports or fitness coaches than therapists because of the stigma that is too often associated with psychological and psychiatric therapies, highlighting the need to adequately train coaches on the mental health problems of young people (Williams et al., 2023; WHO, 2024b). In this context, the Sport Healing Rehabilitation project (SPHERE), co-financed by the European Commission under the Erasmus+ program, developed a set of guidelines providing recommendations for PA practitioners (such as sports coaches, fitness instructors, etc.) and mental health professionals (such as psychiatrists, physical therapists, mental health nurses, etc.), on the design, implementation, and evaluation of organized PA programs for rehabilitation of individuals with mental disorders (Cross-Villasana et al., 2019). These guidelines were put into practice in the context of the European Alliance for Sport and Mental Health (EASMH) Erasmus+ project by an international network of collaborators, researchers, and stakeholders with diverse backgrounds. This international ‘alliance’ was created to develop an innovative training program for PA practitioners, improving their ability to relate to people with severe mental disorders, as well as implementing PA-based rehabilitation interventions (Sampogna et al., 2022).
This review of umbrella reviews has been conducted to provide the state of the art on the benefits of structured PA for young people’s mental health, highlighting strengths and limitations. This choice has facilitated a rapid synthesis and easy comparison of key findings, although it has the limitation of excluding the most recent experimental studies that potentially led to the latest updates on the topic. Furthermore, only articles published in English and in peer-reviewed journals have been included, which allowed for the selection of the most reliable evidence, with the limitation of excluding works in other languages, introducing language bias that might limit the generalizability of the results, and from the grey literature that could potentially describe promising local interventions. In addition, although the methodological quality assessment revealed that the majority of included umbrella reviews were of high quality, some limitations were noted. Not all included umbrella reviews reported a clear search strategy, as in a few cases, some PICO components of the review question were omitted. Furthermore, for a few umbrella reviews, it is unclear whether adequate precautions to minimize bias or systematic errors were undertaken, such as conducting a critical appraisal and data extraction by two independent reviewers and addressing heterogeneity statistically. All these limits are particularly relevant because of the large variability found in the literature, which, if not properly addressed, may lead to effect estimates that do not account for confounding variables and moderators. Lastly, only three umbrella reviews provided clear recommendations for policy and practices. However, this is not related to the quality of umbrella reviews but rather to the paucity of high-quality primary studies, as also indicated by our inconsistent findings on the quality of evidence. The umbrella reviews effectively highlight several methodological weaknesses: studies with heterogeneous samples, including subjects with or without a clinical diagnosis; a wide variability in operational definitions and assessments of different form of structured PA (i.e., exercise, sport, dance, and yoga) as well as mental health outcomes; lack of data on dose-response, potential adverse events and cost-effectiveness, with the only partial exception of studies examining the effects of exercise on depressive symptoms.
Current clinical practice guidelines focus on depressive symptoms, while anxiety and behavioral problems are also a pressing need. These guidelines suggest that group activities involving supervision and an aerobic component, if done three times a week for at least 7 weeks, may be an effective integrative strategy for reducing depressive symptoms (Campisi et al., 2021). Noteworthy, involving young participants in developing the exercise program, considering their preferences, may lead to better results (Ministerio de Sanidad y Consumo, 2018). In addition, a very recent overview of the literature suggests that light-intensity and resistance exercises were the most appropriate for anxiety symptoms (Singh et al., 2025). While this scenario supports the integration of tailored exercise programs into clinical services, it also confirms the need to regulate their provision by exploiting appropriate healthcare policies, such as social prescribing. For other mental health conditions, the advisability of recommending a structured form of PA as part of the treatment strategy should be carefully assessed on an individual basis, considering the clinical and psychosocial characteristics of the young person.
Future RCT studies and new trials with follow-up measurements, subgroup and moderator analyses are strongly recommended to determine which PA-based intervention components work best for which target population. This knowledge can also boost the development of new guidelines, supporting the implementation of innovative health policies embracing social prescription, facilitating young people’s access to interventions based on sport and PA, for mental health prevention and promotion, and reducing the stigma of mental illness.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251342425 – Supplemental material for Impact of structured physical activity on youth’s mental health: A review of umbrella reviews
Supplemental material, sj-docx-1-isp-10.1177_00207640251342425 for Impact of structured physical activity on youth’s mental health: A review of umbrella reviews by Chiara Ciacchella, Barbara Collacchi, Andrea Fiorillo, Gaia Sampogna and Francesca Cirulli in International Journal of Social Psychiatry
Footnotes
Acknowledgements
This work was conceptually supported by the Erasmus+ Sport project ‘EASMH’ grant agreement: 622832-EPP-1-2020-1-IT-SPO-SCP and the Joint Action ‘MENTOR – Mental Health Together’ grant agreement: 101162928.
Author contributions
Chiara Ciacchella: Conceptualization, Methodology, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. Barbara Collacchi: Conceptualization, Methodology, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. Andrea Fiorillo: Writing – review & editing. Gaia Sampogna: Writing – review & editing. Francesca Cirulli: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was developed in the framework of the ‘HOORAY’ Erasmus+ Sport project (grant number 101090537).
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.