
Abstract
Background:
Patients with serious mental illness (SMI) often engage in religious and superstitious activities. The implications of such engagements remain unclear, with no established guidelines for mental health professionals.
Aims:
This study aimed to survey perspectives and gather suggestions from various disciplines within mental healthcare regarding the engagement in religious/superstitious activities of SMI patients: schizophrenia spectrum disorders, bipolar disorder, major depressive disorder.
Method:
This cross-sectional study was conducted between November and December 2023 among Thai mental health professionals. Participants used 10-point Likert scales to rate their agreement levels for engaging each activity. Additional suggestions were obtained through textual responses, which were subsequently summarised and synthesised.
Results:
Of the 403 professionals participated, the majority were female (73.2%), Buddhist (87.6%) and psychiatrists (42.2%), with a median age of 34.0 years. Among patients with active symptoms, patients with major depressive disorder tended to receive the highest mean agreement scores for engagement, while patients with schizophrenia consistently scored the lowest across most activities. Similar trends were observed among patients in remission. From textual responses, two key themes were synthesised: (1) environmental factors and (2) impacts on natural courses.
Conclusions:
Patients with active schizophrenia received the lowest levels of agreement while patients with major depressive disorder tended to receive the highest mean agreement scores on engaging religious/superstitious activities.
Introduction
Serious mental illness (SMI) is broadly defined as a ‘mental, behavioural, or emotional disorder resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities’ and affects more than 1 in 20 people in the United States (Almeida & Fletcher, 2022). Individuals with SMI, especially men and those with comorbid substance misuse, exhibit higher rates of violent behaviours, necessitating proper monitoring (Roché et al., 2021). Due to the alarming nature of their symptoms, the treatment provided for this population often faces maltreatment (Daugherty et al., 2020), and self-stigma is widely reported, particularly in the Southeast Asia Region, where it is most prevalent (39.7%) compared to other regions worldwide (Dubreucq et al., 2021).
One contributing factor to the notably high prevalence of reported self-stigma is rooted sociocultural differences (Krendl & Pescosolido, 2020). This encompasses public stigmatisation related to the disclosure of having SMI and the moral or supernatural causal attributions attached to such disorders (Girma et al., 2013). In Southeast Asia, a region characterised by diverse cultural contexts, a complex interplay of religious beliefs—including Islam, Christianity, Buddhism—superstitious practices and folk traditions significantly influences societal norms and values, thereby shaping mental health treatment approaches in Southeast Asian countries (Murwasuminar et al., 2023). However, the associations between religion and mental health problems in this area are still conflicting (Tan et al., 2021).
Thailand, a country within this region, embraces varied beliefs in religions and superstitions (Suwanrath et al., 2021), often influencing patients with SMIs. While the predominant population in the country adheres to Buddhism, Christians are prevalent in the north, and the southernmost provinces are home to a Muslim majority, with over 90% of the population practicing Islam (Charoenwong et al., 2017). Superstitious beliefs play a significant role in behavioural problems related to mental health (Pravichai & Ariyabuddhiphongs, 2015), directly influencing the exacerbation of relevant psychiatric symptoms. However, these superstitious beliefs or religious practices can also be beneficial for alleviating unfavourable symptoms in patients, as seen in Buddhism meditation in patients with depression and substance-related disorders (Prakhinkit et al., 2014; Shen et al., 2020). Nevertheless, their application should be approached with caution, considering potential misalignments, such as differing concepts of the Self between Buddhism and psychoanalysis in the Western context (Oh, 2022).
Despite the widespread prevalence of such practices, there are currently no established guidelines for mental health professionals regarding whether patients with SMI could engage in these religious or superstitious activities. Therefore, our study aimed to survey encompassing perspectives from diverse disciplines within mental healthcare. By examining the viewpoints of mental health professionals, our findings could offer future recommendations, aiding professionals and patients in navigating the intersection of practicing religious and superstitious activities with mental health care for those with SMI.
Methods
This cross-sectional study was conducted from November to December 2023, targeting closed or private social online groups of Thai mental health professionals, including psychiatrists, psychiatric residents, psychologists, mental health nurses and mental health social workers. Eligibility criteria included professionals aged 18 years or older, interested in participating and proficient in Thai communication. Those with unstable medical or psychiatric conditions, impaired ability to communicate, no direct experience in providing care for patients with mental disorders were excluded. Informed consent was obtained through an online platform, and our study received approval from the Institutional Review Board of the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (COA No. 1481/2023).
Demographic data, including age, sex, region of origin, workplace location, specialisation, years of experience, religions, religiosity and religious practices were collected.
Serious mental illness (SMI)
We categorised SMI into three groups based on three psychiatric diagnoses (Roché et al., 2021): (1) schizophrenia spectrum disorders, including schizoaffective disorder, (2) bipolar disorder, both manic and depressive episodes and (3) major depressive disorder. Within each diagnosis, we further classified two subgroups according to their phases, in remission or with active symptoms.
Religious and superstitious activities
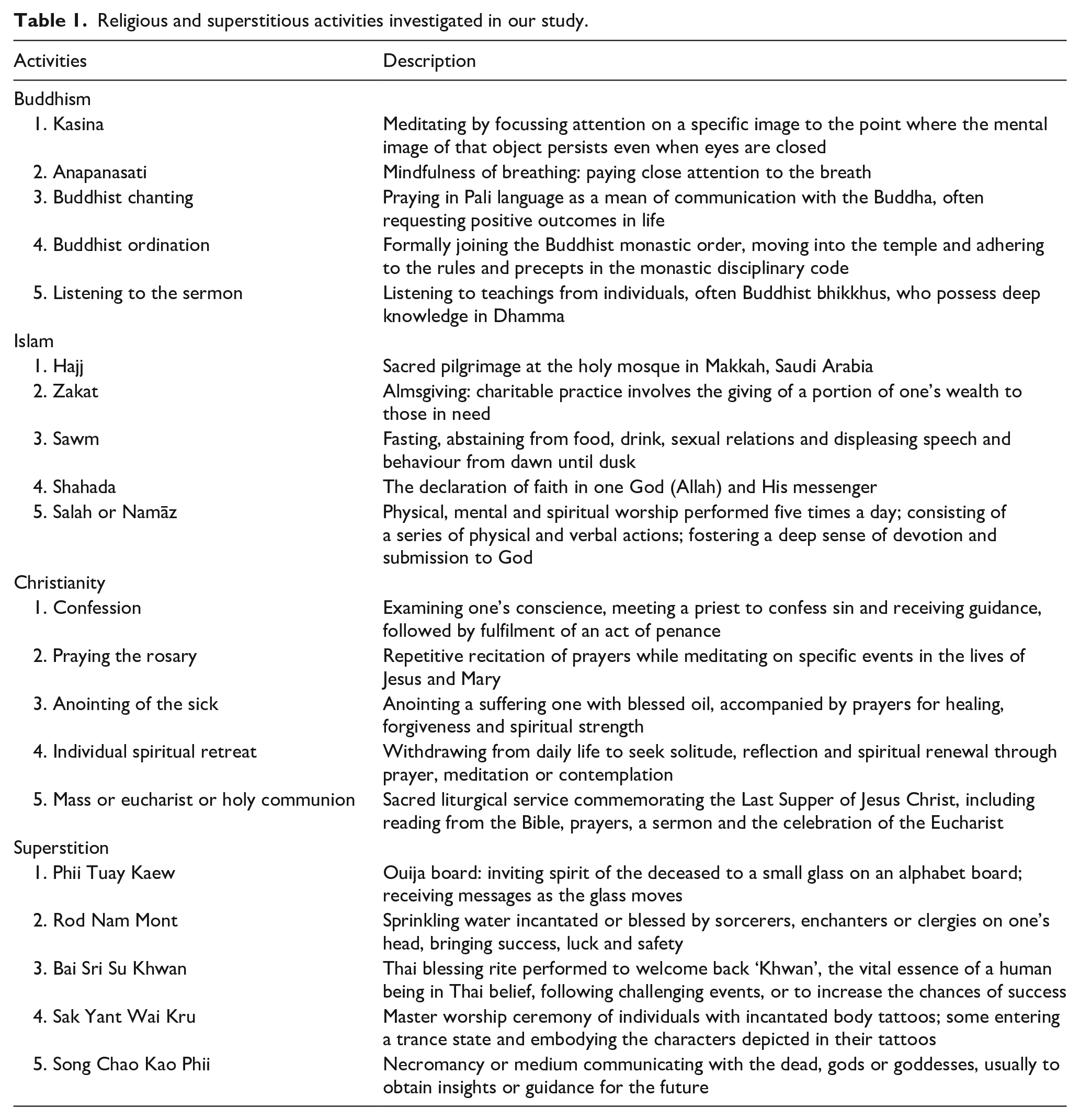
Based on their influences on mental health, five religious activities from each of the three major religions in Thailand were selected by three investigators practicing Buddhism, Islam and Catholicism. Also, five superstitious activities were proposed by one investigator with a specific interest in cultural psychiatry. All activities examined in our study received approval from all authors, and they were illustrated and briefly described in the questionnaire, as outlined in Table 1. All participants were asked to provide their perspectives, indicating their agreement on whether individuals with SMI at each stage could engage in these religious or superstitious activities, using 10-point Likert scales, from 1 = strongly disagree and 10 = strongly agree to engage in each activity. In case of unfamiliarity, ratings for such activities were not required. Additional suggestions could be offered in textual responses, which were later summarised and synthesised into a narrative format.
Religious and superstitious activities investigated in our study.
Statistical analysis
We used SPSS version 29.0 (IBM) for data analysis. Descriptive statistics were utilised to report demographic data, presenting categorical variables as counts and percentage. Continuous variables were described using either mean ± standard deviation or median [interquartile range], depending on data distribution. All tests were two-tailed and a p-value of ⩽.05 was considered statistically significant.
Results
In total, 403 professionals participated in our study. Female comprised the majority (73.2%) and the median [interquartile range] age and years of experience was 34.0 [30,40] and 7.0 [4,12] years, respectively. Nearly half of the participants hailed from Bangkok Metropolitan Region (47.9%), and more than a half practiced within this area (61.5%). The predominant professionals were related to psychiatry (n = 220, 54.6%), including general psychiatrists (n = 109, 27.0%), child and adolescent psychiatrists (n = 61, 15.1%) and psychiatric residents (n = 50, 12.4%), followed by psychologists (n = 91, 22.6%) and mental health nurses (n = 78, 19.4%). In terms of religious affiliation, Buddhism was the most prevalent (n = 353, 87.6%). A majority reported themselves as moderately religious/moderate believers (n = 205, 50.9%) and practicing/engaging in religious activities at least once a year (n = 145, 36.0%). Demographic data of all participants are shown in Table 2.
Demographic data of all participants (n = 403).
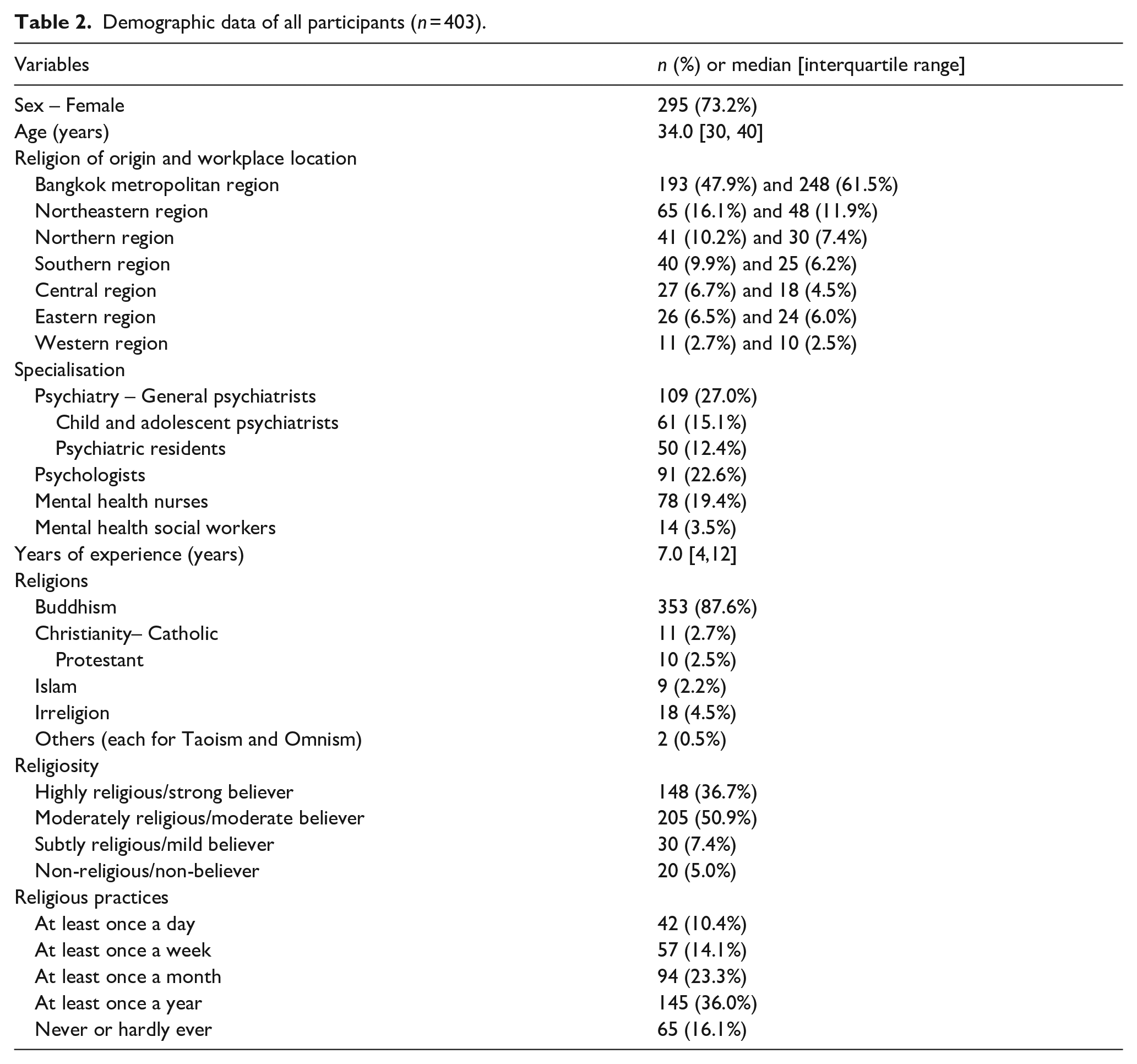
Table 3 presents the mean scores of agreement levels for each SMI diagnosis and engagement in examined activities. Participants who indicated unfamiliarity with particular activities were not required to provide ratings for those activities, leading to varying reported number of participants across activities. Notably, most participants provided ratings for superstitious and Buddhist activities, while most activities associated with Christianity and Islam were frequently indicated unfamiliar. Among patients with active symptoms, patients with major depressive disorder tended to receive the highest mean scores. In contrast, patients with schizophrenia consistently received the lowest mean scores across most activities, with the exception of Zakat, Islamic alms-giving, where patients with bipolar disorder registered the lowest level of agreement to engage. This trend of lowest scores in patients with schizophrenia, followed by bipolar disorder and then major depressive disorder, was also observed among patients in remission. The darker shades of red and green indicate lower and higher mean agreement scores, respectively, with a neutral point represented by white at 5.50.
Level of agreement on engagement of each superstitious or religious activity.
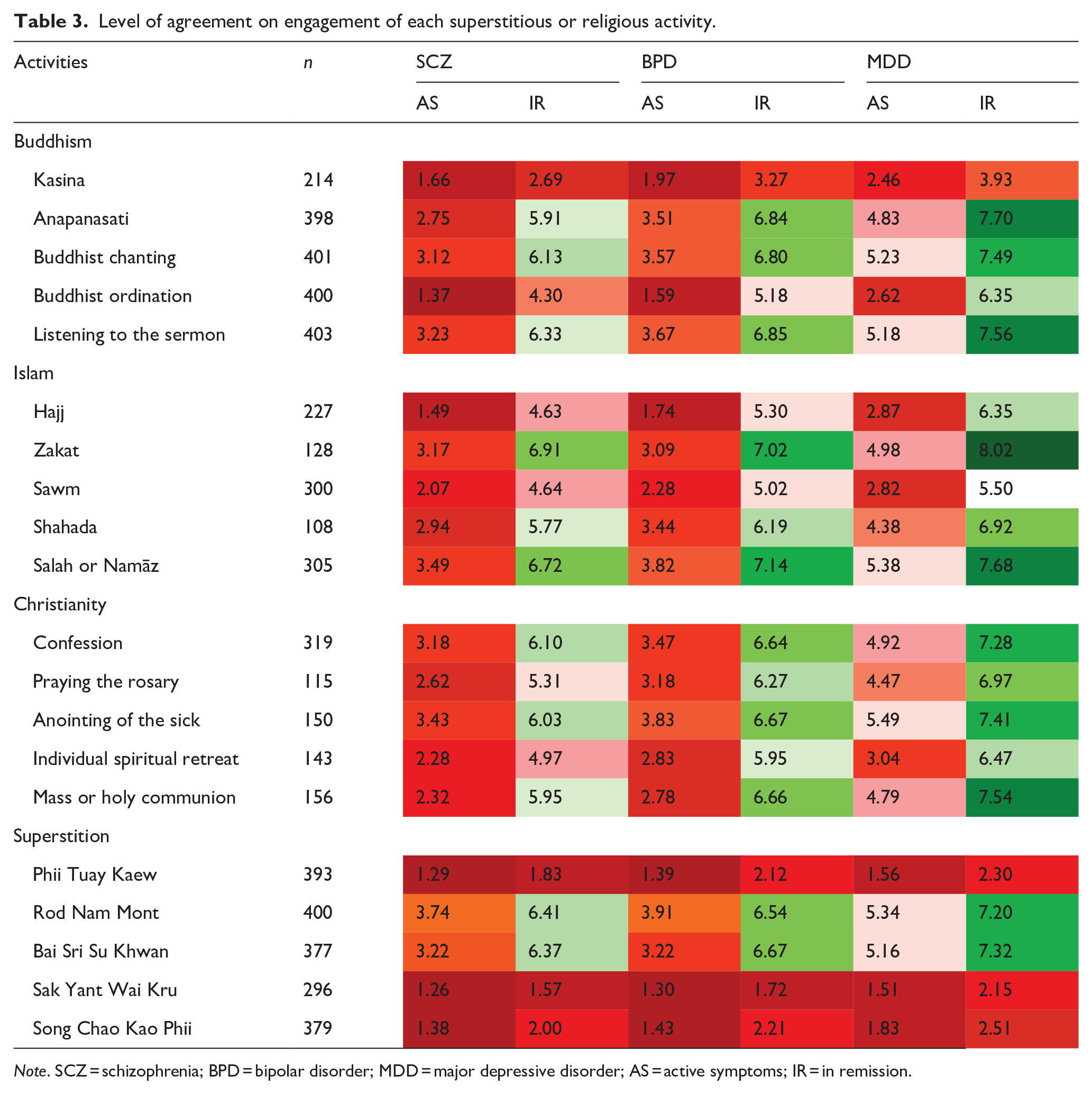
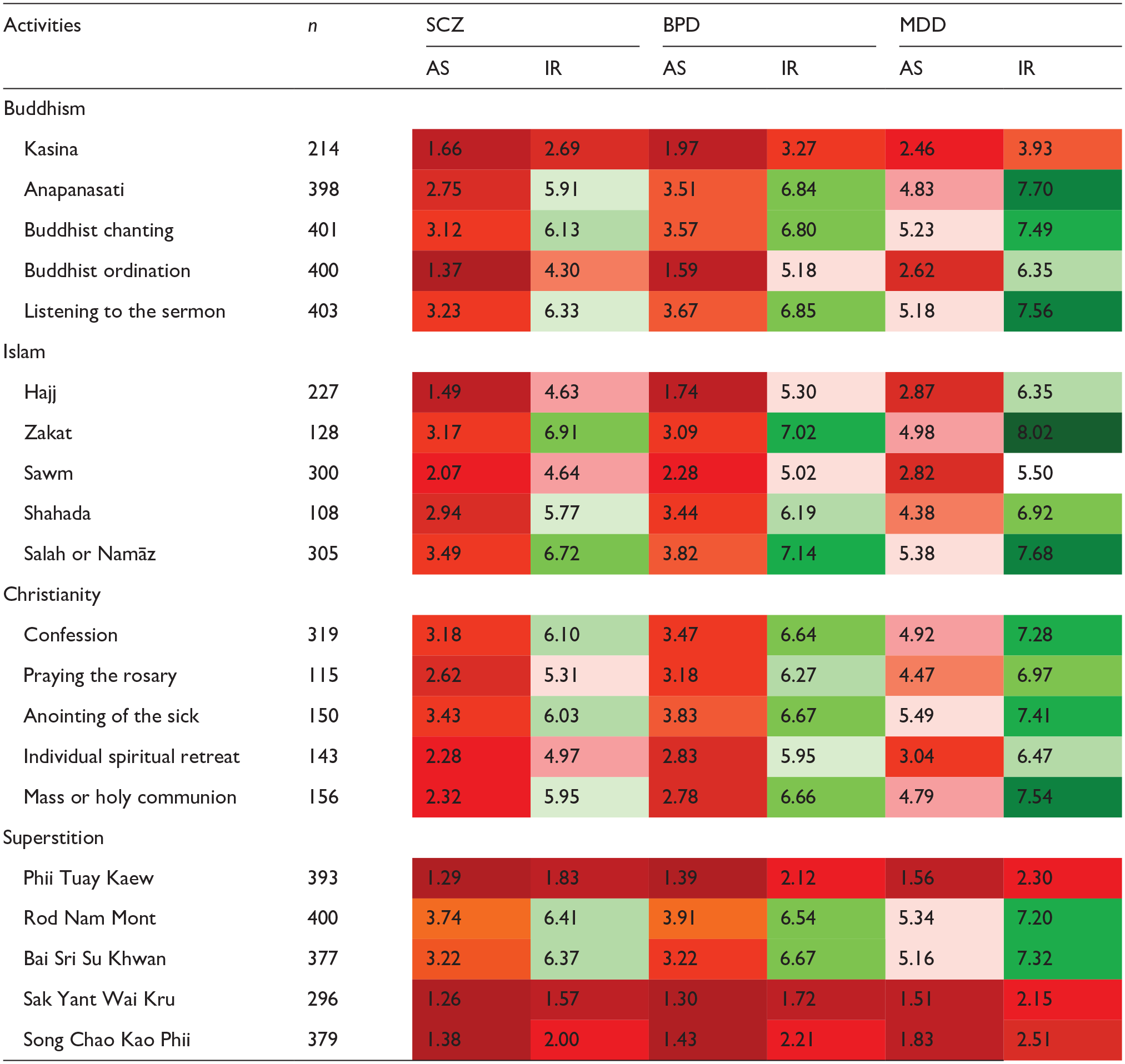
Note. SCZ = schizophrenia; BPD = bipolar disorder; MDD = major depressive disorder; AS = active symptoms; IR = in remission.
We received 22 textual comments related to superstitious activities, 14 regarding Buddhist activities, 3 concerning Islam and 2 associated with Christianity. Upon review, we categorised these responses into two distinct domains: (1) environmental factors, encompassing both during the ceremony and its aftermath, and (2) impacts on natural courses, especially prior to receiving appropriate mental health care.
Environmental factors, encompassing both during the ceremony and its aftermath
Many activities involve multiple individuals and environmental factors, including officiants, attendants and venues. When considering engagement in such activities, professionals should be mindful not only of the immediate ceremony but also of potential ongoing consequences. Both professionals and caregivers should recognise the unique characteristics of each setting their patients will encounter, particularly potential risks during vibrant and vigorous ceremonies.
. . generally, (I) support engaging activities; but, large gatherings, Upathan Mhoo (Thai term for collective psychogenic illness), loud noises, and heightened sensitivities during ceremonies could exacerbate psychiatric symptoms.
- mental health nurse’s comment for Islam activities
Additionally, after ceremonies conclude, patients may be relocated to other venues like those for Buddhist ordinations, where they are not under the direct care of their usual caregivers and often face significant adjustment to their daily routines, increasing the risk of symptom relapse.
For sermons, it depends on monks and ordination relies on temple. If they (patients) are in a good spot and things are done right, then I will give higher agreement scores.
- psychologist’s comment for Buddhist activities
Regarding Buddhist ordination, not recommend, (as it) reduces social engagement, enhances self-isolation, potentially fostering false beliefs. (It may be) more suitable for those in remission.
- psychologist’s comment for Buddhist activities
Impacts on natural courses, especially prior to receiving appropriate mental health care
Symptoms of SMIs are occasionally perceived as superstitious phenomena, such as possession or punishment from the supernatural. As a result, some patients are first brought to religious clergy, exorcists or necromancers. Despite significant expenses incurred by caregivers, the symptoms often persist without improvement, delaying their eventual treatment by mental health professionals. Hence, establishing healthcare collaborations fostering connections between traditional practitioners and mental health professionals could prove beneficial.
Some patients and their families go to extreme lengths, even selling their lands and properties to fund these traditional treatments, leading to delays in receiving (medical) care, . ., and fortune tellers, if they (fortune tellers) are adequately trained in mental health, could serve as valuable resources. Many patients, especially at during bargaining or starting frustrated, might turn to fortune tellers as readily as phoning 1323, mental health hotline.
- mental health nurse’s comment for superstitious activities
In addition to participating in activities, patients also have the opportunity to form relationships with other attendees at these events. Such connections can positively influence their mental well-being, and vice versa.
. . encouraging patients to connect with the community, thereby allowing the community to alleviate (their distress).
- psychologist’s comment for Christian activities
Furthermore, responses included a range of superstitious and Buddhist rituals that have not yet to be included and warrant careful consideration. Specifically, practices related to ghosts, spirits and other intangibles should be approached with caution. These rituals vary geographically:
(1) In the northern and northeastern regions – Tok Sen (hammering along muscular lines; a form of massage using a hammer tapping), Phii Fah (sky ghost; a ritual involving spirits believed to assist those with illness through dance and music) and Mo Dham (doctor of Dhamma; a local traditional practitioner trained from both Buddhist and superstitious tracks and keeping in good practices)
(2) In the southern region – Kru Mo Nora (Nora professional teachers; ancestral spirits believed to oversee their descendants’ legacies; when these spirits aid individuals, they are honoured through Nora, a traditional dance from southern Thailand. Conversely, if individuals fail to acknowledge or accept these spirits as their mediums, they risk facing adverse outcomes, such as illness), and Bor Mor (practitioners specialise in each of various areas, including life-cycle rituals, curing disease, finding lost or stolen items within some Thai-Malay Muslim communities; this belief diverges from mainstream Islamic teachings)
(3) Across the country, though typically not practiced outside Thailand, Thai-Buddhist rituals include Bhana Yaksa (Pali language for informing the giant; an traditional and thunderous Buddhist chat aimed at warding off negativity), and Kae Karma (Karma solving; rituals intended to transform negative karma into positive outcomes
Discussion
Lower levels of agreement were observed among SMI patients with active symptoms, particularly patients with schizophrenia, given their heightened susceptibility to harmful behaviour due to impaired decision-making capacity (Moritz et al., 2016). Interestingly, some practices, like mindfulness-based approaches such as meditation or Anapanasati, where are generally perceived as beneficial for mental health, can paradoxically worsen psychotic symptoms (Joshi et al., 2021). Therefore, such activities are suitable for patients during remission as shown in favourable mean agreement scores (5.91–7.70) found from our study.
Bipolar disorder, though it can present symptoms akin to major depressive disorder, garnered lower agreement levels than unipolar depression. This was explained by the potential severity of developing manic episodes. Religious/superstitious activities that influence sleep patterns, such as Buddhist ordination or Sawm (Islamic fasting) during Ramadan, can disrupt biological rhythms, potentially precipitating bipolar disorder (Chen et al., 2020).
For patients with active major depression, while the overall mean scores were more positive relative to other diagnoses across all examined activities, none surpassed the neutral cut-point of 5.50. This suggested that, based on our findings, SMI patients with active symptoms were advised against engaging in the religious/superstitious activities surveyed.
During remission phases, certain activities consistently received diminished agreement levels across all diagnoses. These included Sawm or Islamic fasting, advanced Buddhist meditation Kasina and three Thai superstitious rituals related to the intangible world, ghosts and spirits: Phii Tuay Kaew (Ouija board), Sak Yant Wai Kru and Song Chao Kao Phii. Conversely, superstitious rituals like Rod Nam Mont and Bai Sri Su Khwan, devoid of direct association with ghosts, were viewed more favourably, suggesting their non-harmful and supportive attribute.
Islamic fasting, particularly during Ramadan, introduces challenges for patients, potentially triggering symptom exacerbation, despite patients were in during remission as our highest mean agreement score were at 5.50 (neutral) for major depressive disorder with remission. Additionally, it can disrupt the timing and absorption of medications that require food for optimal uptake. Recommendations addressing these concerns have been outlined (Furqan et al., 2019).
The Kasina meditation demands prolonged attention and may lead to distorted reality testing, posing risks for psychiatric conditions (Narayan et al., 2013). The mentioned superstitious rituals have associations with altered consciousness or dissociation, thereby adding risks for SMI patients (Karpel & Jerram, 2015). Presently, aside from Islamic fasting, there exist no formal guidelines regulating activities like Kasina or these risky superstitious practices. Addressing this multifaceted issue necessitates enhanced psychoeducation for patients and their families. Additionally, it calls for the formulation of policies regulating such practices for SMI patients and forging connections between superstitious practitioners and mental healthcare services to address unforeseen circumstances. A nuanced understanding of each activity is paramount, as echoed by suggestions from our textual responses.
When considering environmental determinants, a holistic approach encompassing social and spiritual aspects is indispensable. The surroundings during ceremonies should neither be perceived as negative-events nor conductive to inducing psychiatric symptoms (Guang et al., 2017) or practices related to paranormal beliefs, potentially exacerbating mental illnesses (Shiah et al., 2010). Beyond merely attending these ceremonies, ramifications of non-participation, such as societal ostracisation, must also be contemplated as some society members of SMI patients prioritised taking patients to spiritual healers, along with modern psychiatric treatments (Shah et al., 2022). Routines following the rituals, such as those during Ramadan or Buddhist ordination, warrant thorough scrutiny to ensure that they will not disrupt patients’ treatment and practitioners understand how best to care for patients, enabling professionals to leverage these activities for improved treatment outcomes.
Incorporating religious/superstitious practitioners into the mental healthcare system can alleviate treatment delays. This integration aids in the timely detection of symptom changes and offers psychosocial support (Heseltine-Carp & Hoskins, 2020), as comments found from our textual responses. Given its societal integration, this approach may face reduced stigma, prompting individuals with early symptoms to seek assistance from these practitioners prior to reaching mental health professionals. Additionally, leveraging this as a potent social instrument for the long-term rehabilitation of SMI patients holds promises, and better connections within patients’ families sharing similar cultural beliefs and values. Nonetheless, research on these aspects within Thai or broader Asian contexts has remained limited and warranted further exploration before policy implementation.
Our study underscored the pivotal role of cultural competence and awareness among mental health professionals (Naito et al., 2019). The emphasis laid not in viewing these practices with suspicion but in harnessing them with creativity and respect. By bolstering mental health education for these practitioners and facilitating their integration into the system, patient care can be substantially and holistically enhanced. However, it is crucial that comprehensive treatments delivered are tailored to patients’ needs and preferences, going beyond just the insights and attitudes of mental health professionals.
From textual responses, numerous activities not covered in our study were suggested. Regrettably, we couldn’t encompass all these activities in a single survey. The crucial consideration, applicable to all activities, is that professionals should be mindful of environmental factors during and after ceremonies and establish potential linkages between superstitious/religious resources and mental health services. In addition, as Thailand and other nations within Southeast Asia Region shares some cultural beliefs and rituals, the further survey included broader activities would be advantageous for all countries with nearly similar sociocultural contexts. Given that Thailand and other Southeast Asian countries share certain cultural beliefs and rituals, expanding future surveys to encompass a wider range of activities could be beneficial for nations with comparable sociocultural contexts. Moreover, future collaborations among mental health professionals across Southeast Asia should prioritise the development of culturally specific guidelines for SMI patients regarding their engagement with religious/superstitious activities.
Our studies covered activities practiced worldwide under the umbrella of the three main religions and superstitious practices commonly shared in neighbouring countries of Thailand. We particularly gained valuable insights into Buddhist practices, currently applied in psychological interventions, such as the mindfulness-based approach. Our study incorporated a range of disciplines within mental healthcare, mirroring real-world practices. It offered, to the best of our knowledge, the first comprehensive insights from mental healthcare specialists on this lesser-explored topic. While we did gather suggestions via textual responses and synthesised recurring themes, readers should note that our approach wasn’t strictly qualitative.
Limitations
Some limitations should be acknowledged. Participants were enrolled with convenience sampling, leading to potential response bias. The questionnaire specifically designed for assessing perspectives on religious and superstitious practices was not available. As an alternative, we utilised 10-point Likert scales in our study, allowing for the representation of both positive and negative perspectives through divergent scoring. Categorising patients with SMI posed challenges due to the varying degrees of severity they exhibited. To address this, we provided a concise description of the SMIs included in our study, intending to offer our respondents a clearer understanding of these patient groups. Aligned with clinical importance, these SMIs were considered at risk of experiencing negative outcomes due to the interplay between their conditions and religious/superstitious activities. Most participants were Buddhist and unacquainted with non-Buddhism activities, particularly Christianity, leading to lowered number of such activities included for analysis. Limited knowledge of religions beyond their own beliefs could be implied, emphasising the need for deeper and broader understandings to provide appropriate psychoeducation in respect of patient-centred beliefs.
Conclusion
Patients with active schizophrenia received the lowest levels of agreement from mental health professionals on engaging religious/superstitious activities. Professionals should take into consideration various determinants, both during the ceremony and its aftermath, that may impact psychiatric illnesses. Establishing connections between mental health services and religious/superstitious practitioners can mitigate treatment delays and optimise care for SMI patients.
Footnotes
Acknowledgements
We express our sincere gratitude to all the participants who generously dedicated their time to contribute to our study and provide the best care for our patients. We also thank Ms Naratip Sa-nguanpanich for her generous assistance with statistical analyses.
Author contributions
Sorawit Wainipitapong: Conceptualisation, Methodology, Investigation, Resources, Formal analysis, Writing – Original Draft Somboon Hataiyusuk: Investigation, Resources, Writing – Review & Editing Chonmanan Khanthavudh: Conceptualisation, Investigation, Resources, Writing – Review & Editing Vitchayut Phetsayanavin: Investigation, Resources, Formal analysis, Data Curation, Writing – Review & Editing, Project administration Teeravut Wiwattarangkul: Investigation, Resources, Formal analysis, Writing – Review & Editing. Daruj Aniwattanapong: Conceptualisation, Methodology, Writing – Review & Editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study received approval from the Institutional Review Board of the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (COA No. 1481/2023).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
ORCID iDs
Data availability statement
Due to the textual natures and sensitive responses of this study, the data availability is not publicly accessible. The researcher requiring dataset or more information can directly contact to the corresponding author.