
Abstract
Background:
Suicide is the third leading cause of death among youth aged 15 to 29 years old globally. Guyana has the highest rate of youth suicide in the world, yet only limited research exists.
Aim:
The aim of this study is to identify key features of the suicide pathway for Guyanese children and youth and to distinguish meaningful subgroups.
Method:
The psychological autopsy (PA) method was used to generate life charts for 15 Guyanese children and youth (10–29 years) who died by suicide. Nineteen close contacts of these individuals were interviewed about the life events of the decedent between 6 months and 5 years after their death. Semi-structured interviews lasting 30 to 150 min took place between November 2021 and January 2022. The interview data were converted into life charts and these were reviewed to uncover meaningful subgroups of suicide pathways.
Results:
Three groups with distinct suicide pathways were identified: hard life (46%), mental illness (20%) and interpersonal stress (20%). There were also two male youths for whom the suicidal antecedents and pathways were unclear. Interpersonal stress, alcohol, exposure to suicide and family history of suicide were common factors identified across groups.
Conclusions:
The findings emphasise the role of both acute and protracted interpersonal stress for child and youth suicide in Guyana. The structure and dynamics of Indo-Guyanese families are discussed. Interventions recommended include enhancing child and youth community engagement, improving mental health and suicide literacy, alcohol restriction, increasing access to support services, and reducing stigma.
Introduction
Guyana defines youth as those aged between 14 and 35 years old (National Youth Policy of Guyana, 2015), whilst the OECD defines youth as people aged 15 to 29 years old (OECD, 2021). For the purposes of this study, youth are classified as those aged 15 to 29 years old while children are defined as those 10 to 14 years old. Suicide was the third leading cause of death among youth globally in 2021 (WHO, 2024a). In 2019, Guyana had the highest rate of youth suicide in the world (58.23/100,000), with the rate for males (82.72/100,000) being 2.5 times higher than the suicide rate for females (32.56/100,000; WHO, 2021). Furthermore self-harm was the leading cause of death for the age groups 10-14, 15-19, and 20-24 in Guyana in 2021 (WHO, 2024b). There is less data available for child suicide, but research indicates that Guyana was ranked among the highest nations for female child suicide for 2000-2009 (Kõlves & De Leo, 2014). Despite these high rates of child and youth suicide, a recent review of the research highlights that there is a dearth of information available on child and youth suicidality in Guyana (Shaw et al., 2022).
Guyana, situated on the northeast coast of South America, is an anglophone country that shares its border with Venezuela, Brazil, and Suriname. The country recently attained high income status due to the discovery and extraction of oil (Hamadeh et al., 2023), however institutions remain weak (World Bank, 2023). The country is divided into 10 administrative regions and approximately 90% of its population resides in the coastal regions (Bureau of Statistics Guyana, 2016). The average age in Guyana is 25.07 and children and youth aged 10 to 29 years old account for 37.7% of the population (Bureau of Statistics Guyana, 2016). Guyana is an independent republic with a complex history of colonisation by multiple European nations, involving slavery from West Africa and indentured labour from India, Portugal, and China (Premdas, 1992). This colonial history has resulted in an ethnically diverse population of approximately 750,000 consisting of 40% Indian heritage (Indo-Guyanese), 29% African heritage (Afro-Guyanese), 10·5% indigenous (Amerindian), 20% who identify as ‘Mixed’, and Chinese, Portuguese and White cumulatively contribute less than 1% (Bureau of Statistics Guyana, 2016). Despite the Africans and Indians having a shared history of hardship and resettlement, the two groups were pitted against each other by the colonialists and this has resulted in ongoing ethnic pluralism (Premdas, 1992). This ethnic pluralism is evidenced by a two-party political system catering to Afro-Guyanese and Indo-Guyanese, and ethnic geographic clustering. Since independence, each party has held power in almost equal measure and the party appealing to Indo-Guyanese is currently in office.
Adverse life events have been shown to have a strong association with suicidal behaviours for children and youth (Serafini et al., 2015) with research suggesting interpersonal problems to be of significance (Lee & Wong, 2020). However the antecedents to suicide differ between ethnic/racial groups, which is why localised research and knowledge is so important for effective prevention efforts (Lee & Wong, 2020). This paper analyses the pathway of suicidality of children and youth, utilising the life charts method (Fortune et al., 2007; Maris & Lazerwitz, 1981). According to the biopsychosocial model of suicide risk, individual risk factors can be distal, developmental or proximal (Turecki et al., 2019). Life charts are a valuable tool to explore the chronological connections among biological, psychological and social factors throughout a person’s life. Life chart analysis has been used to improve our understanding for suicide in farmers (Kunde et al., 2017), the LGBT population in Australia (Skerrett et al., 2017), people diagnosed with a mental illness (Clapperton et al., 2020) and youth in the UK (Fortune et al., 2007). Identifying key features that contribute to suicide among Guyanese children and youth could enhance insight into motivators or contributors to suicide and reveal potential opportunities for child and youth suicide prevention. The aim of this study is to identify key features of the suicide pathway for Guyanese children and youth and to distinguish meaningful subgroups.
Method
Participants
Nineteen contacts of Guyanese children and youth who died by suicide (n = 15) were interviewed for this study. The criteria for informant participation were being at least 18 years old and having had close contact with the person who died by suicide. Close contact is defined as having good knowledge of the person who died by suicide and having had recent communication with them before they died. To minimise recall bias, the death had to have occurred within the last five years. For ethical considerations related to grief, six months needed to have passed since the suicide. The informants included parents (n = 13), grandparents (n = 2), in-laws (n = 2), a spouse (n = 1) and a friend (n = 1).
Informants were recruited using: (1) promotion on a Facebook page, (2) a public media campaign, (3) distribution through networks associated with non-governmental organisations (NGOs) and (4) snowballing of informant networks. Individuals who wished to take part were encouraged to contact the primary investigator either by phone or through direct messaging. Indirect snowballing involved informants being asked to provide the details of the study to others whom they know have been affected by suicide. Reimbursement of the informant’s time in the form of GY$2,000 phone credit (US$10 equivalent) was provided at the conclusion of the interview.
Data collection and measures
Semi-structured psychological autopsy interviews of duration between 30 and 150 min (0.5–2.5 h) were conducted between November 2021 and January 2022 in Guyana at the informants’ homes and workplaces. For three of the decedents, multiple informants were interviewed as a group whilst the remaining 12 decedents had one informant each. Verbal informed consent was obtained from all informants. The interviews began with a narrative, informant lead section, involving an open-ended request, ‘Please tell me about he/she’ and included an adapted Interview for Recent Life Events (Paykel, 1997), which collected data about romantic relationships, non-romantic relationships, education, finances, mental health and suicidality, drug and alcohol use, domestic violence, legal, employment, bereavement, family health, physical health, accommodation change, suicide exposure, and natural disasters. The informants were asked about each of these topics in relation to the decedent’s life, for example ‘Did they have any legal issues during their life?’. The interviews were conducted by the first author, who is a Clinical Psychology PhD candidate and registered provisional psychologist. She is Australian, married to a Guyanese, and had lived in Guyana for eight years prior to this study.
Procedure
Life charts are a visual representation of life event chronology. From the psychological autopsy data, individual life charts were created by the first author (CS) in Microsoft Excel. Any event mentioned in an informant interview that was relevant to any of the life chart categories was plotted onto the decedent’s life chart. The life charts were then reviewed by two authors (CS and KK) to uncover meaningful groups of suicide pathways. Three subgroups with pathways were defined by agreement. ‘Typical’ life charts were created to provide a visual illustration of the representative features of the lives of each group (see Figures 1–3).

Typical life chart for Hard Life group (n=7).

Typical life chart for Mental Illness group (n=3).

Typical life chart for Interpersonal stress group (n=3).
Results
The sample of Guyanese children and youth who died by suicide included 10 males and 5 females aged 10 to 29 years (M = 20.86, SD = 5.5), three of whom were aged between 10 and 14 years. In a majority of the cases, the children and youth lived with family (93%), identified as Hindu (73%), were male (66%), Indo-Guyanese (73%) and from Region 3 of the country (60%; see Table 1). Seven of the males (70%) and two of the females (40%) died by hanging and the remaining by pesticide poisoning. The informants were interviewed between 7 months to 4 years 9 months after the suicide (M = 2.1 years).
Characteristics of the study sample (n = 15).
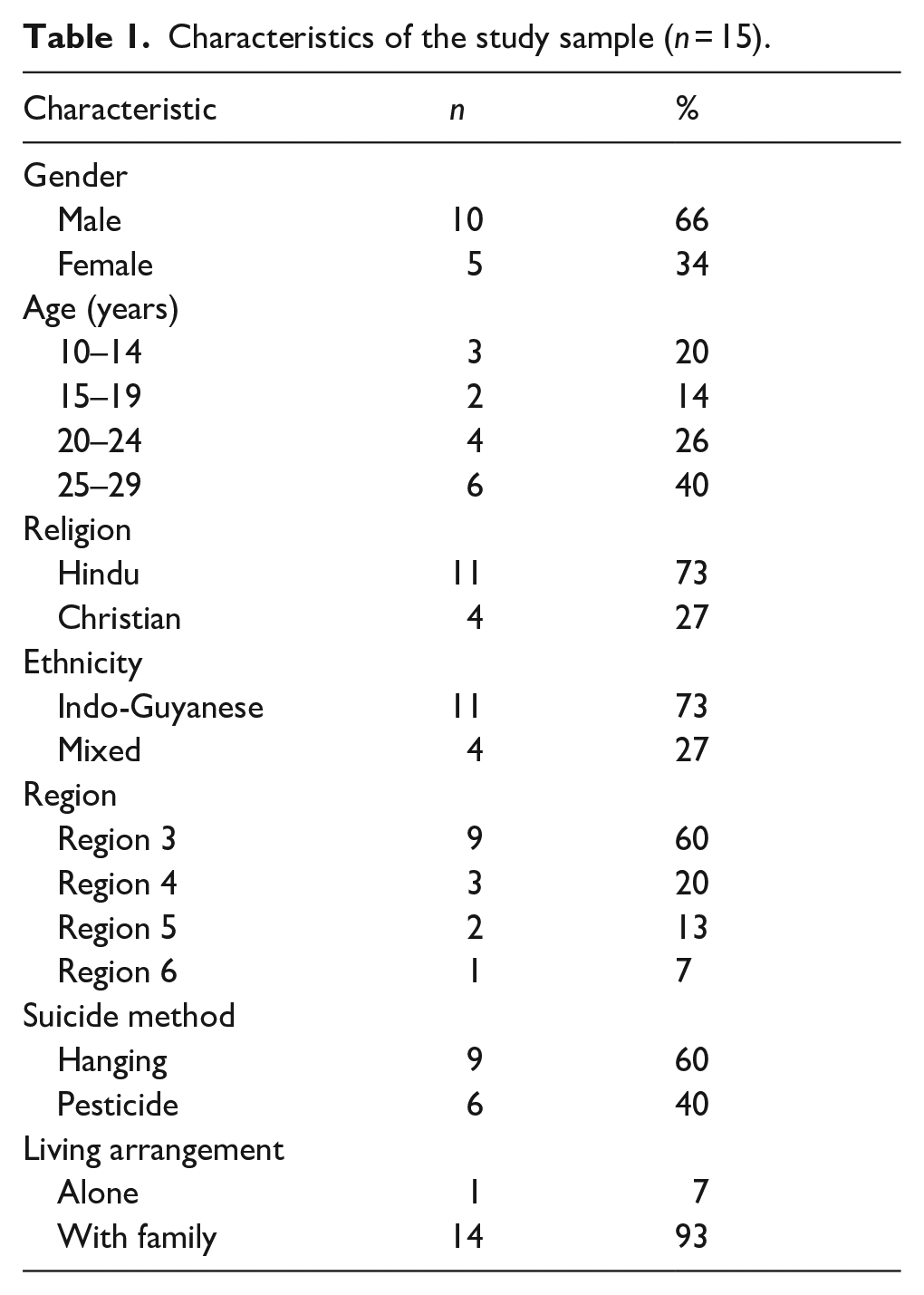
Exposure to suicide, family history of suicide, and alcohol use were identified as common factors across the sample. Ten (66%) of the decedents were exposed to suicide in their lifetime, in that they knew of people who had died either within their village, through friends or family. The means used commonly matched the means of the suicide exposure, such that if their friend died by hanging, they too died by hanging. Ten (66%) of the decedents had a family history of suicide, which they may or may not have known about, including grandparents, uncles, aunts or cousins, often multiple people. Seven (46%) of the youth were intoxicated when they died, six of them male. Half of the male youths (n = 5) reportedly regularly drank alcohol to excess. None of the decedents were known to be accessing mental health treatment. One youth had reportedly tried to access the suicide prevention helpline unsuccessfully.
Of the children and youth who exhibited non-fatal self-harm behaviour (n = 5), those who had harmed using poisoning (medications, pesticide), eventually died by pesticide poisoning and those who had harmed using intentional injury (cutting) died by hanging. Suicidal ideation (n = 7) varied from explicit communication about wanting to die to indirect communication including talking about wanting to join a loved one in afterlife and giving away possessions. For the children and youth who expressed suicidal ideation, this was first identified by the informants 1 to 5 years prior to suicide. Six decedents did not express suicidal ideation nor engage in non-fatal self-harm behaviour as far as the informants were aware. The pesticide was ingested with at least one witness present. Whilst those who died by hanging did so privately. There was, however, one child who hung themselves in the presence of a younger child. No suicide notes were reported by informants.
Life charts generated from the psychological autopsy interviews evidenced three groups with different suicide pathways; hard life, mental illness and interpersonal stress (see Table 2).
Groups by defining features of life charts of Guyanese children and youth who died by suicide (n = 15).
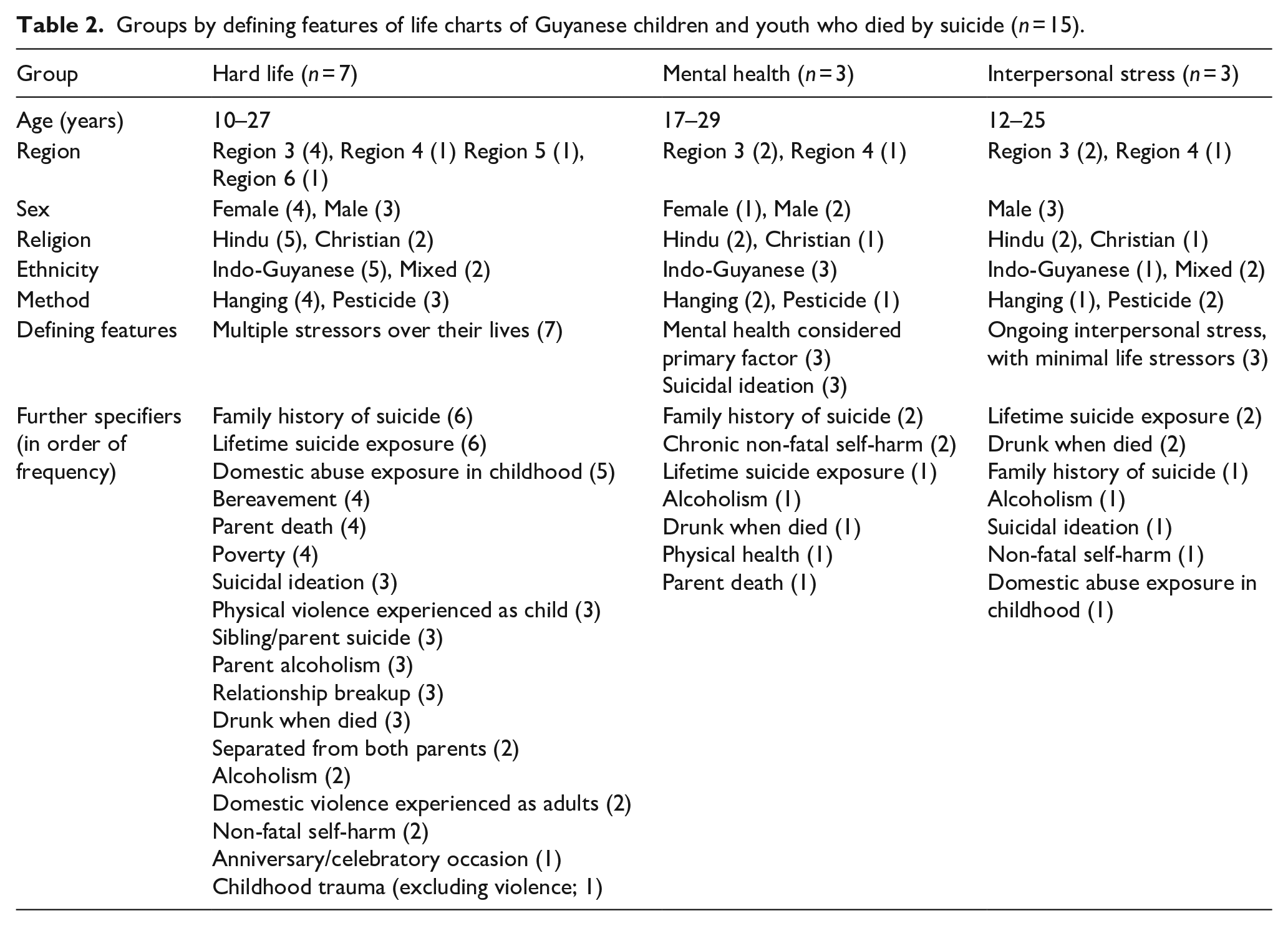
Hard life (n = 7, 46%) – this pathway was characterised by multiple adverse experiences across the lifespan, including domestic abuse exposure in childhood (n = 5, 71%), bereavement (n = 4, 57%), and parental death (n = 4, 57%) (see Figure 1). A proximal adverse interpersonal event such as family rejection (n = 1), suicide death of peer (n = 1), domestic violence (n = 2), and romantic rejection (n = 1) was present for five of the deceased. However, no proximal adverse event was reported for two of the cases.
Mental illness (n = 3, 20%) – this pathway was characterised by the likely presence of a medium term (3–4 years) undiagnosed mental health disorder, with few life event stressors evident (see Figure 2). No proximal adverse events were identified by informants. Suicidal ideation was present for all in this group and two youth had a history of chronic non-fatal self-harm requiring medical intervention.
Interpersonal stress (n = 3, 20%) – this pathway was characterised by ongoing (1–5 year) interpersonal conflict in the absence of other life stressors (see Figure 3) this group was all male and conflict was in the context of peers (1), romantic (1), and family (1) relationships. An acute stress response was reported for two people in this group, such that they died directly after an interpersonal conflict interaction.
There were two decedents for whom no stressors were identified by informants. The youth in this group were Indo-Guyanese males in their 20’s who died by hanging.
These typical life charts are made from an aggregate of life charts from each group (Figures 1–3).
Discussion
In this paper, life charts created from psychological autopsy study data were used to identify key features of suicide pathways for 15 Guyanese children and youth to distinguish meaningful subgroups. Based on these life charts, three groups were identified: hard life, mental illness, and interpersonal stress. There were also two youth for whom the pathway to suicide was unclear. Lifetime exposure to suicide, family history of suicide, and alcohol use, were identified as prevalent factors across all groups.
The hard life group included children and youth who had experienced multiple adverse events across their lifetime inclusive of domestic abuse exposure in childhood, loss of a parent, bereavement, physical violence experienced as a child, parent/sibling suicide, domestic violence experienced as an adult, parent alcoholism, and poverty. Adverse experiences are recognised as a risk factor for suicide (Séguin et al., 2014) and there is evidence of a dose response effect (Li et al., 2008). Research from Guyana has identified difficulties coping with stressful life events as a potential risk factor for child and youth suicide (Arora et al., 2020). Research suggests that stressful life events increase suicidality by increasing psychological distress and decreasing perceived social support (Yıldız, 2020). For most of the children and youth in this group, the suicide appears to have been precipitated by a proximal interpersonal stressor, such as family rejection, suicide death of peer, domestic violence or romantic rejection.
Interpersonal stress was identified as another pathway to suicide. This all-male group was characterised by a stable life with few stressors, except for an ongoing interpersonal conflict in the context of peers, a romantic relationship or family, which culminated in a conflict interaction proximally precipitating the suicide. The association of acute and protracted interpersonal stress with suicide aligns with evidence that the perception of social disapproval from others is significantly correlated with non-fatal self-harm in a Guyanese child and youth sample (Denton et al., 2017). Therefore, it appears that interpersonal stress is an important factor for child and youth suicide in Guyana, as it is in other cultures (Lee & Wong, 2020). This gives credence to positive social support and community engagement as potential protective factors for child and youth suicide in Guyana (Arora et al., 2020).
This sample of children and youth was predominantly of Indo-Guyanese ethnicity, and research suggests that Indo-Guyanese have the highest rate of suicide in Guyana (Shaw et al., 2022). People of Indian indentured labour heritage are also over-represented for suicide in Fiji (Morris & Maniam, 2000), Malaysia (Armitage et al., 2015), Suriname (Graafsma et al., 2016), and Trinidad and Tobago (Maharajh & Abdool, 2005), with rates believed to be higher than in India. Researchers from Trinidad and Tobago and Fiji have implicated the family structure of Indo-Trinidadian and Indo-Fijian homes, stating that they typically have strict patriarchal households, with prolonged collective supervision, resulting in transgenerational cultural conflicts between children and youth and their parents (Ali & Maharajh, 2005; Grambeau, 2007; Maharajh & Abdool, 2005). Research purports that these children and youth cannot speak openly to their parents due to tensions arising between traditional and modern values, such as wanting to date before marriage (Ali & Maharajh, 2005; Grambeau, 2007).
This family dynamic theory has also been hypothesised in relation to Guyana (Edwards, 2016). Edwards (2016) describes the Indo-Guyanese culture as having high mechanical solidarity and low social solidarity in the wider social system, due to holding values and norms that are inconsistent with those of the wider society. He posits that this results in Indo-Guyanese operating as a closed group with high regulation of children and youth. Thus it is possible that Indo-Guyanese children and youth feel isolated, due to the limited ability to express themselves within the home whilst also having limited social resources to draw from outside of the family system. Accordingly, after they experience adversity, they are not able to access important social supports, which compounds their distress. A similar theory has been put forth about suicide in rural China, stating that the insularity of the family structure results in a lack of social support system which reduces a person’s coping ability during interpersonal crisis (Zhang et al., 2010). There is evidence highlighting the importance of family relationships for Indo-Guyanese young adults, with family support found to mediate and moderate the association between life satisfaction and depressive symptoms, whereas ‘friend’ and ‘other significant’ support were non significant (Roopnarine et al., 2016).
The mental illness pathway to suicide likely involved an undiagnosed mental health condition. Prior to their death, the youth in this group exhibited symptoms of mental distress such as psychosis, insomnia, non-fatal self-harm, and chronic suicidal ideation, that spanned three to four years, whilst their lives were relatively stable and their social connections were strong. Undiagnosed mental illness is a known suicide risk factor (Bertolote et al., 2004) and none of the youth in this group had accessed mental health support. In fact, although almost two thirds of the children and youths in this study had expressed suicidal ideation or engaged in non-fatal self-harm, none of them had ever received mental health treatment nor other targeted support. One youth was known to have called the suicide prevention hotline the week of their death, however, they reportedly did not receive support. This potentially indicates limited mental health awareness of families, mental health stigma, and or deficiencies in existing support services as barriers to obtaining professional support. Limited help seeking could also be related to the criminal status of attempted suicide at that time. In relation to barriers to mental health help seeking among Guyanese children and youth, Arora and Persaud (2020) identified shame and stigma, fear of negative parent response, and limited awareness of mental health services. Whilst Indo-Guyanese adults have identified stigma and confidentiality concerns related to support services (Groh et al., 2018).
There were two male youths for whom there appeared to be no indicators of stress or suicidality and their families reported their suicides as a mystery. This could be due to limited emotional intimacy between these men and their families, potentially related to the aforementioned Indo-Guyanese family dynamic. It is also possible that the informants were not comfortable sharing the life story of the decedent, however this seems unlikely given the self-identification recruitment strategy.
Male youths in Guyana have a 2.5-time higher rate of suicide than female youth and the disparity is greater across the lifespan (males 3.5 times higher; WHO, 2021). Indeed males have a higher rate of suicide than females in most countries in the world WHO, 2019). Suicide in young men has been linked to a preference for high lethality means and higher rates of substance use (Pitman et al., 2012). In our sample, males died by hanging in higher proportion than females and alcohol use was implicated for male suicide. Many male youths were intoxicated when they died and/or regularly drank to excess. Acute alcohol use is known to increase the risk of suicide due to disinhibition and depressed mood, whilst chronic use can increase impulsivity, impair cognitive function and depress mood (Kõlves et al., 2022). Data from 2005 indicated that Indo-Guyanese had the highest rates of alcohol overuse in Guyana when compared with other ethnic groups (Lacey et al., 2016). Moreover a more recent survey indicated that Indo-Guyanese were the ethnic group most likely to have had a drink in the last month (UNICEF, 2019). These findings suggest that alcohol use may be an important feature of Indo-Guyanese male youth suicide in Guyana.
Exposure to suicide was a common factor across groups and is a known suicide risk factor (Hill et al., 2020). Our results indicated that children and youth often used the same method as that which they had been exposed to, suggesting a possible imitation effect. Family history of suicide was also identified as common across groups, which may be due to the high rates of suicide in the population. Exposure to suicide was identified as a risk factor by Guyanese school staff and students, who referenced children and youth becoming desensitised to suicide in their communities and that this normalisation of suicide may lead young people to more easily consider suicide as an option (Arora et al., 2020). Literature has explored the impact of the cultural script on youth suicide and suggests that the way a culture conceptualises suicide impacts it’s prevalence (Abrutyn et al., 2020). Therefore cultural perceptions of suicide is an important area of future research in Guyana.
Implications
The findings of this study have implications for child and youth suicide prevention in Guyana. Acute and protracted interpersonal stress was implicated and research has suggested that Indo-Guyanese children and youth face tension within their homes, potentially as a result of cultural insularity, and have low social resources to draw from during times of crisis (Edwards, 2016). Increasing social support available through community activities is thought to be effective in reducing suicidality among children and youth exposed to stressful life events (Yıldız, 2020). Acculturation literature details the importance of sport for promoting a sense of community (Jones et al., 2021; Rich et al., 2015). Promoting the creation of safe youth friendly recreational spaces was listed as a goal in the National Youth Policy of Guyana (2015) and the government has recently increased the budget for sport. Research from Pakistan has demonstrated the mental health benefits of playing cricket for male youth (Ali et al., 2023), which is the leading sport in Guyana. The youths who played cricket had significantly lower rates of depression, anxiety, and suicidal ideation than non-cricketers. A community intervention which expands supportive social resources for children and youth is recommended for suicide prevention.
Help seeking was only evident for one youth in this sample and no children or youth had accessed formal support. Notably, mental health symptoms spanned three to four years prior to suicide and suicidal ideation was first expressed at least one year prior to suicide, which affords opportunity for intervention. Therefore, youth suicide prevention efforts in Guyana should focus on improving mental health and suicide literacy, access to support services, and reducing mental health stigma as important population level interventions. In terms of suicide literacy, it would be important to increase awareness of warning signs for suicide for family members of high risk groups, such as children or youth who have attended the emergency room for non-fatal self-harm. Progress regarding access to support services is already being achieved as a Suicide Prevention Bill was passed in parliament in November 2022, resulting in the decriminalisation of suicide in Guyana and thus the removal of a significant help seeking barrier.
Male youths have a higher rate of suicide than females (WHO, 2021) and alcohol use was implicated for male youth suicide in this sample, therefore alcohol use interventions may play a role in youth suicide prevention. Research has indicated that restrictions on alcohol availability at a population level, for example, via sales restrictions and/or increased cost via taxation of alcohol, are associated with decreased suicide rates, particularly for males (Kõlves et al., 2022). Therefore restricting alcohol availability could be considered as part of youth suicide prevention in Guyana.
Limitations and Future Research
It is important to recognise the constraints of this study. The limited convenience sample used is not representative of child and youth suicide in Guyana. Whilst epidemiological data related to child and youth suicide in Guyana are not available, the overrepresentation of males and people of Indo-Guyanese ethnicity in this sample is consistent with the lifespan profile of suicide in Guyana (Shaw et al., 2022). In addition, informants were interviewed within a timeframe ranging from six months to five years following the suicide which could introduce varying degrees of recall bias, a limitation frequently observed in psychological autopsy studies (Kõlves et al., 2021). A limitation of life charts analysis is that it is not possible to know the extent to which individual life events played a role in the individual’s decision to end their life (Skerrett et al., 2017). Furthermore, life charts were noted to be less detailed than those from previous life chart studies (Fortune et al., 2007; Kunde et al., 2017), potentially due to the the predominance of parents as informants. Young people are in the developmental process of individuation, with typically higher levels of disclosure with peers than family. This may have contributed to the limited data points on the life charts and indeed the two youth for whom no stressors were identified. Whilst other life chart research appears to have more detail, it is worth noting that the study of youths in UK identified similar suicide pathways (Fortune et al., 2007).
Future research should focus on a representative psychological autopsy study and interviews with a non-fatal self-harm sample. Research on mental health and suicide literacy, help seeking challenges, and cultural suicide scripts would also contribute to an improved understanding of child and youth suicide and thereby guide interventions.
Conclusion
This is the first study of suicide pathways of Guyanese children and youth. Life charts were created for 15 Guyanese children and youth and differences in the suicidal pathways were observed across three groups. The results from this study emphasise the role of both acute and protracted interpersonal stress. Cultural family dynamics may increase distress and limit social resources for Indo-Guyanese children and youth. The suicide pathway indicates that there is opportunity for intervention, however this may be limited by support service access, mental health stigma, or limited mental health and suicide literacy. Therefore improved access to support services and advancements in mental health and suicide literacy would support child and youth suicide prevention in Guyana. Population wide efforts to increase social resources available to children and youth and restrict alcohol availability are recommended.
Footnotes
Acknowledgements
None.
Author contributions
Charlotte Shaw: Conceptualisation, formal analysis, investigation, data curation, writing – original draft, writing – review and editing, visualisation, project administration. Jaimee Stuart: Conceptualisation, methodology, writing – review and editing. Troy Thomas: Writing – review and editing. Kairi Kolves: Conceptualisation, methodology, validation, formal analysis, writing – review and editing, supervision. All authors contributed to and have approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Australian Government Research Training Program Scholarship through Griffith University Australia. The funder of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. This research was approved by the Griffith University Human Research Ethics Committee (GU Ref: 2021/809) and the Ministry of Health Guyana Institutional Review Board (132/2021).
Informed consent statement
Verbal informed consent was obtained from all informants.
Consent for publication
Not applicable.
Data availability statement
The participants of this study did not give consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.