
Abstract
Background:
Negative affectivity of caregivers has been linked to difficulties in the caregiver-patient relationship and it is assumed to contribute to the maintenance of eating disorder (ED) symptoms.
Aims:
The present study investigated the relationship of patients’ ED symptom severity to patients’ and caregivers’ depressive symptoms, and caregivers’ involvement in a mixed sample of adult inpatients with anorexia (AN) and bulimia nervosa (BN), as well as their caregivers.
Method:
The Eating Disorder Examination and Beck Depression Inventory (BDI) were administered to 55 adult ED patients (26 AN and 29 BN), and the BDI as well as the Involvement Evaluation Questionnaire were filled in by one caregiver of each patient.
Results:
Our results showed caregivers’ depressive symptoms to be significantly related to patients’ ED symptom severity, however depressive symptoms and ED symptoms of patients were not related. No connection of involvement of caregivers and ED severity of patients was found. AN and BN patients did not significantly differ on ED severity or depressive symptoms. Caregivers of AN and BN patients did not differ significantly on depressive symptoms and involvement.
Conclusions:
Our results support the importance of mental health support for caregivers of adults with AN and BN.
Introduction
Adult eating disorder (ED) patients and their caregivers show a high prevalence of depressive symptoms (Treasure et al., 2020; Zabala et al., 2009). Caring for someone with anorexia nervosa (AN) is a risk factor for depression and other difficult mental states (Stefanini et al., 2019). Goddard et al. (2013) found evidence for an indirect connection between caregivers’ distress and AN patients’ ED symptoms through patients’ distress. However, it is unclear, if caregivers depressive symptoms can be directly associated with patients’ ED severity in adults and if this is applicable in various ED types.
Caregivers of ED patients report high involvement in comparison to those of patients with other severe mental disorders (Martín et al., 2015) although adults often refuse to involve their caregivers in the therapy (Slater et al., 2015). Involvement and depressive symptoms are significantly linked in caregivers of ED patients (Kocsis-Bogar et al., 2023; Padierna et al., 2013). However, it is not clear, if caregivers’ involvement and patients’ symptom severity are connected.
In the present study, the following hypotheses were formulated: (1a) A significant positive connection of caregivers’ and patients’ depressive symptoms and (1b) a positive connection of both of these with patients’ ED severity were expected. (2) A significant connection of caregivers’ involvement with patients’ ED symptoms was expected.
Method
Human rights statement
Ethical approval was obtained from the Research Ethics Committee of the Medical University of Vienna. All procedures in this study involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments.
Participants
Fifty-five inpatients (26 AN and 29 BN) of the Clinical Division of Social Psychiatry, Department of Psychiatry and Psychotherapy, Medical University of Vienna were included. For each patient one caregiver with the most significant supporting role – the so-called ‘key relative’ – was invited in the study. Data collection, as well as inclusion and exclusion criteria, are described in more detail in Kocsis-Bogar et al. (2023).
Measures
Eating Disorder Examination (EDE; Hilbert & Tuschen-Caffier, 2006, sample α = .91), Beck Depression Inventory (BDI; Beck et al., 1961, sample α = .84), and Involvement Evaluation Questionnaire (IEQ; Van Wijngaarden et al., 2000, sample α = .85) were applied.
Statistical analysis
IBM SPSS 26 was used for data analysis. Missing values were not substituted. AN and BN patient and caregiver groups were compared via Student’s t-test for dimensional and χ2 test for categorical variables. Hypothesis 1a was tested via Pearson correlation analysis. Hypothesis 1b and 2 were investigated via hierarchical multiple linear regression analysis adjusted for the ED diagnosis entered in the first block. Patients’ depressive symptoms were entered in the second, caregivers’ depressive symptoms in the third, and caregivers’ involvement in the fourth block. Patients’ age and duration of illness were not included due to their correlation with ED severity. Patients’ sex as was not included because of the predominance of women. Normal distribution (Kolmogorov-Smirnov, p > .84) and homoscedasticity (Breusch-Pagan test, p = .61) were checked for the variables included in the regression analysis. Level of significance was set at p < .05. Bonferroni correction was applied.
Results
Descriptive values of the sample
AN and BN patients were not significantly different regarding age, sex, length of illness, BDI or EDE total scores, restraint or eating concern, and after Bonferroni correction regarding weight concern either. BN patients had significantly higher BMI and shape concern. Caregivers of AN and BN patients did not differ regarding their age, sex, depressive symptoms, and involvement (Table 1).
Descriptive variables of the whole sample (N = 55) and comparison of AN (n = 26) and BN (n = 29) patients.
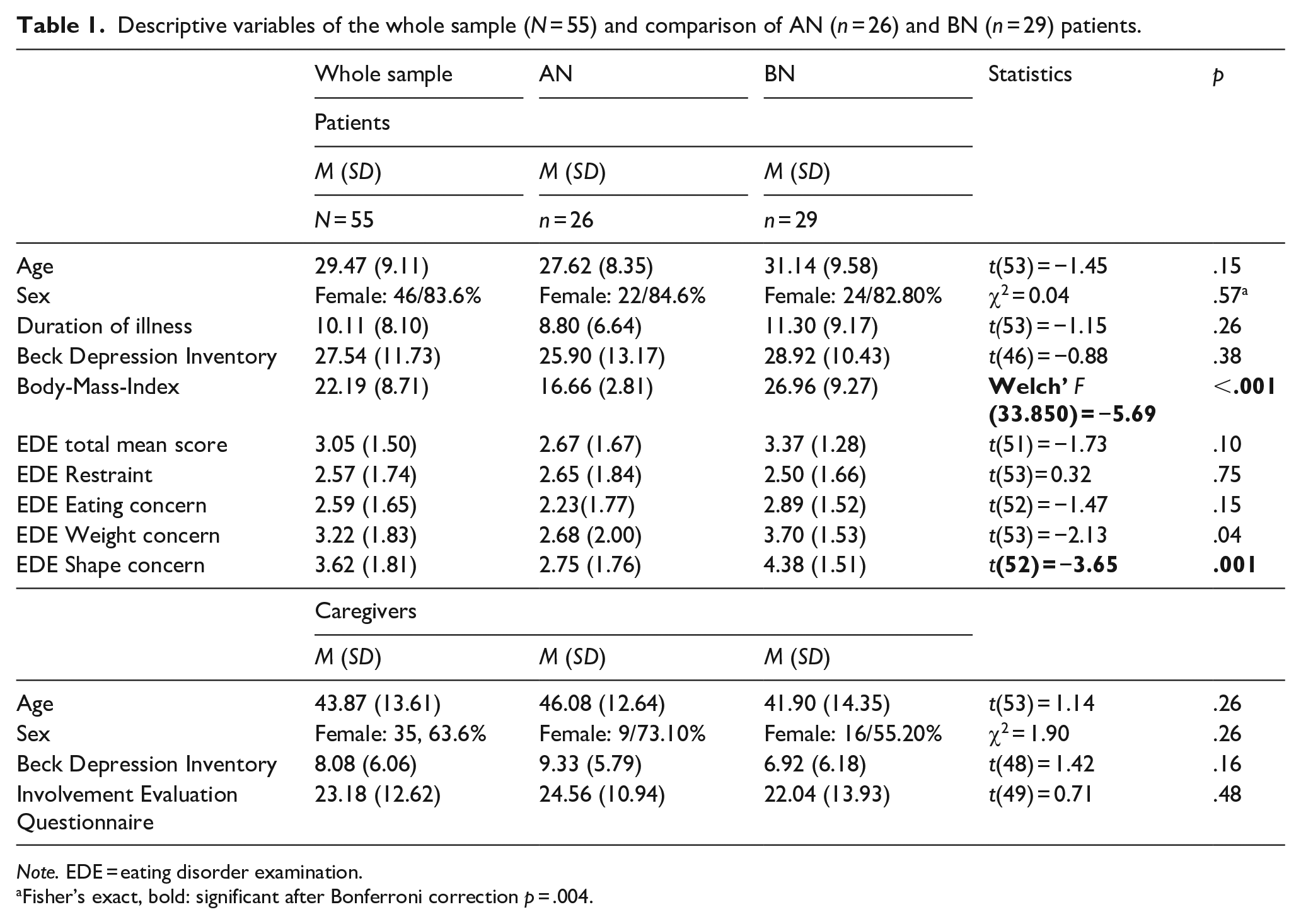
Note. EDE = eating disorder examination.
Fisher’s exact, bold: significant after Bonferroni correction p = .004.
Connection of patients’ and caregivers’ depressive symptoms, caregivers’ involvement, and patients’ ED severity
Depressive symptoms of patients and caregivers were not significantly associated (r = −.07, p = 0.64, N = 43). Regarding the hierarchical regression analysis, only model 3 reached significance, according to which only caregivers’ depressive symptoms were significantly linked to patients’ ED severity, whereas the diagnosis and patients’ depressive symptoms remained insignificant. This was the only model with a significant amount of change. Adding caregivers’ involvement did not result a significant further change and model 4 remained non-significant (Table 2).
Hierarchical regression model of factors associated with ED severity in the sample of AN and BN patients (N = 55).
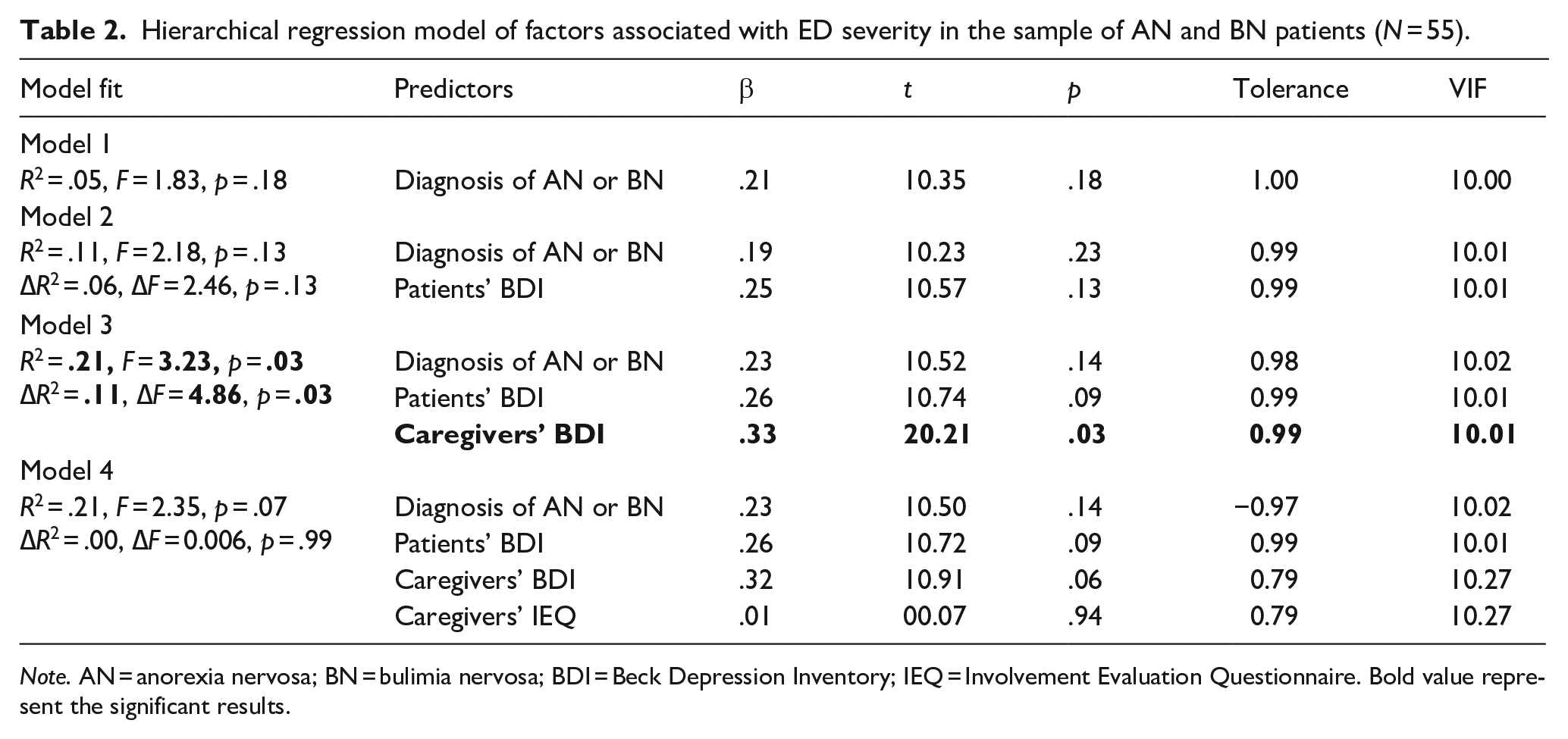
Note. AN = anorexia nervosa; BN = bulimia nervosa; BDI = Beck Depression Inventory; IEQ = Involvement Evaluation Questionnaire. Bold value represent the significant results.
Discussion
The main finding of the present study was the direct relationship between caregivers’ depressive symptoms and patients’ ED severity. This can be interpreted in terms of the cognitive-interpersonal model of negative emotions in family members in association with ED symptoms (Treasure & Schmidt, 2013). Caregivers’ burden can compromise their relationship with the patient (De La Rie et al., 2005) which can in turn contribute to more severe ED symptoms (Treasure et al., 2020). Contrary to Goddard et al. (2013), patients depressive symptoms had no significant connection to ED severity or caregivers’ depressive symptoms, possibly because of patients’ relatively high and caregiver’s only slightly elevated BDI scores. Unlike Goddard et al. (2013), the present sample included BN and AN patients living mostly independently of their caregivers with a higher mean age. A possible explanation for the lack of connection between patients’ depressive and ED symptoms is that chronic depressive symptoms in ED patients are comorbid but not directly connected to ED symptom severity but other factors such as quality of life (Martín et al., 2017).
No connection between caregivers’ involvement and patients’ ED severity was found. Contrary to expressed emotions or accommodating (Goddard et al., 2013), involvement has some positive (such as urging and supervision) aspects from the patients’ point of view which can be experienced as caring. Further, involvement was measured by a self-report questionnaire and thus may not correspond to patients’ perception of their caregivers’ involvement.
It is a cross-sectional examination, which makes it impossible to draw causal conclusions. The limitations of it are described in detail in Kocsis-Bogar et al. (2023). Our results support the importance of considering the needs of caregivers of adult ED patients in the treatment (Treasure et al., 2020) to reduce burden for caregivers (Hibbs et al., 2015) as well as health care services (Treasure et al., 2020).
Footnotes
Acknowledgements
The authors are grateful to all the patients and caregivers for their participation as well as to the medical, nursing, and therapy team of the hospital for their support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the Medical-Scientific Fund of the Mayor of Vienna (project number: 09032)
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, no AI or AI-assisted technologies were used.
Data availability statement
The data underlying thsis article will be shared on reasonable request to the corresponding author.