
Abstract
Background:
Insights from mental health stigma research indicate the importance of societal and political views on mental health perceptions. Most studies originate from typical Western neo-liberal settings and focus on generic mental health issues. Our research explores these associations in Hungary, an understudied post-communist context with significant stigma levels, examining a broad range of stigmas related to both general and three specific mental illnesses: schizophrenia, depression, and alcohol use disorder (AUD).
Aims:
The study aims to connect a wide array of political dispositions to stigma associated with both general and specific mental illnesses, exploring both attitudes and behavioral intentions.
Methods:
We surveyed 492 participants (147 males, 342 females) on their political dispositions, including Right-Wing Authoritarianism (RWA), Social Dominance Orientation (SDO), general and economic system justification, and conservative political ideology, and their attitudes toward general and specific mental illnesses. Regression analyses identified key political dispositions influencing stigma.
Results:
RWA was significantly linked to most stigma outcomes, while conservative political ideology showed a selective impact. Other predictors had minimal influence on stigma outcomes.
Conclusion:
Our findings suggest that perceptions of danger, threat, and unconventionality, as indicated by RWA, are crucial for mental health stigmatization in Hungary. Intervention programs should target these factors, particularly in similar contexts.
Keywords
The existing literature on the stigmatization of mental illness is predominantly based on studies from Western countries, with only 14.6% of all papers including data from low- or middle-income countries (Angermeyer & Schomerus, 2017). The almost exclusive reliance on data from typical Western neo-liberal contexts is particularly problematic given that one of the crucial insights of stigma research is that what people think regarding political and social questions – what is a fair society, who should yield power and why, who is the ‘other’ – matters for how people think of mental health. We will refer to such individual-level differences in worldview or ideology as political dispositions. Most research in this field, particularly on how political conservatism correlates with stigmatization, originates from the US (DeLuca & Yanos, 2016; Ragsdale, 2022). The only exception may be a Swedish study that reported similar findings to those found in the US (Löve et al., 2019).
Our research focuses on Hungary, a country with notable mental health challenges, including high rates of alcohol consumption (Mihailovic et al., 2020) and suicide (Balint et al., 2020). A recent Eurobarometer survey revealed that perceived stigma is widespread among Hungarians, with those displaying symptoms of mental illness being the least likely in Europe to seek or receive professional help (European Commission, 2023). Besides providing results from a new and understudied context, we extend on existing research by (i) comparing various conceptualizations and measures of political dispositions (ii) assessing stigma multidimensionally, and (iii) assessing stigma in the context of three distinct mental disorders – depression, schizophrenia, and alcohol use disorder (AUD).
Previous research on political dispositions has often relied on simple measures like ideological left-right self-placement or vote choice. While convenient for large-scale surveys, ideological self-placement has severe limitations as a measure. Education, cultural background, and individual differences in morals and values all matter for how people understand scales such as the left-right scale (Bauer et al., 2017; Kivikangas et al., 2021; Piurko et al., 2011). On the other hand, vote choice depends on what is on offer on the ideological menu – on how political entities (e.g. party elites) in a specific cultural and historical context package economic and cultural views under specific ideological banners into particular bundles of attitudes for voters to choose from (Sniderman & Bullock, 2004). This is especially true in the Hungarian context, where the political choice for more than a decade has been between the one-party rule of an increasingly authoritarian governing party, Fidesz, and an ideologically fragmented opposition that attempted to form a fragile coalition in the last two national elections (Lönnqvist et al., 2021). The Hungarian political system is characterized by democratic backsliding and a populist turn (Krekó & Enyedi, 2018; Wunsch & Gessler, 2023). The degree of power concentration on the government side is exceptional (Krekó & Enyedi, 2018), leading to a desperate alliance of social democratic, liberal, far-right, and green parties, and diminishing the significance of traditional political ideology measures such as vote choice and ideological left-right self-placement, which, in this context, wouldnot be face-valid indicators of individual’s actual beliefs.
We focused on Right-Wing Authoritarianism (RWA), Social Dominance Orientation (SDO), and system justification (SJ) – previous stigma research that has moved beyond ideological self-placement and vote choice has focused on RWA and SDO, and we argue that system justification could also be relevant. RWA outlines a conservative worldview characterized by aggressiveness toward outgroups, submission to authorities, and adherence to traditional values (Altemeyer, 2006). In the US, RWA has been correlated with various dimensions of stigma, including negative stereotypes, negative attributions and affect, and social distance toward generic mental illness (DeLuca & Yanos, 2016; DeLuca et al., 2018). In France and Greece, RWA predicted social distance from schizophrenia (Lampropoulos et al., 2021), and in Australia, it was associated with negative attitudes (e.g. blame, perceived dangerousness) and low social acceptance toward schizophrenia and depression (Kvaale & Haslam, 2016).
RWA is included in dual-process models of prejudice, in which it is complemented by Social Dominance Orientation (SDO). SDO refers to the extent to which individuals endorse a hierarchical perspective of society, desire intergroup dominance, and oppose equality (Duckitt et al., 2002; Pratto et al., 1994) – it reflects a motivation to distance oneself from subordinated groups (Hadarics & Kende, 2018). Two of the above-referred studies on RWA and mental health stigma have been conducted within the framework of the dual-process model. In France, Greece, and Australia, SDO, as compared to RWA, appears to be a somewhat weaker predictor of mental health stigma toward schizophrenia and depression (Kvaale & Haslam, 2016; Lampropoulos et al., 2021).
Both SDO and RWA can be interpreted as part of a family of psychological dispositions – a need for security and certainty, mental rigidity and inflexibility, preference for familiarity, order and structure – that underlie political conservatism (e.g. Jost, 2021; Jost et al., 2009). System justification theory suggests that the social and psychological need to defend, bolster, and justify prevailing social, economic, and political arrangements—that is, to see the status quo as good, fair, natural, desirable, and even inevitable is a unifying theme that defines conservatism (Jost, 2021). People who believe in a system that strongly stigmatizes mental illness could be expected to also stigmatize those with mental illness themselves. Besides general system justification beliefs (GSJ), economic system justification (ESJ) – the tendency to legitimize economic inequality (Jost & Thompson, 2000) – could be relevant. A general aversion to economic egalitarianism (ESJ) could motivate mental health stigma – in cultures dominated by capitalist values, individuals struggling with mental health issues are often viewed as burdens on society due to their limited economic productivity and are blamed for this shortfall (Scheff, 2017; Yang et al., 2014).
Besides being limited to Western samples, the current literature on political attitudes and mental health stigma suffers from its focus on generic mental health (Angermeyer & Schomerus, 2017). In the present research, we focused on three types of mental illness: schizophrenia, depression, and AUD. The first two are, we believe, the most studied mental health illnesses in the literature on stigma. AUD was included, in part, because of its high prevalence in the East-Central European context, and therefore its high relevance from a public health perspective (Mihailovic et al., 2020).
Not only the determinants of mental health stigma but also the concept of stigma itself is inherently complex and calls for a multidimensional understanding. There is no universally accepted single definition or measure of stigma. Despite this, most researchers have relied on one dimension or a global scale (Pescosolido & Martin, 2015). Given that we measured a wide variety of psychological motivations that could underlie stigma, and that we included three very different mental health illnesses, we found it important to also assess the different dimensions of stigma as specifically as possible. That is, besides traditional prejudice and negative stereotypes and attitudes, we also measured desired social distance in various interactions, specific attributions, support for discrimination, and categorical beliefs.
In summary, the purpose of the present research was to assess a wide array of political dispositions and connect these to three distinct mental illnesses, schizophrenia, depression, and AUD, as well as a wide variety of different types of stigmas, ranging from attitudes to behavioral intentions. Importantly, this was conducted in Hungary, an understudied post-communist context with high levels of stigma associated with mental illness.
We propose that RWA, SDO, and General and Economic System Justification, alongside Conservative Political Ideology, will predict mental health stigma, both generally and for specific mental illnesses like depression, schizophrenia, and AUD. However, previous empirical work does not allow for more specific predictions with regards to what political dispositions go with what type of stigma. One aim of the present study is to start filling this gap in the literature.
Methods
Participants and procedure
Initially, 551 participants completed the survey questionnaire, but after excluding those with over 10 missing responses or monotonic responses, the final sample included 492 respondents (147 males, 342 females; MAge = 29.02, SD = 12.71). The majority were educated, with 297 having at least a high school diploma and 177 holding university degrees. The sample featured 255 university students, 210 employees, and 27 others (e.g. retired). In terms of subjective socioeconomic status (SES), the distribution was 27 very high (‘I do not have any financial problems’), 355 high (‘I do not have financial problems, but I have to live within my means’), 102 low (‘I can’t buy everything I want and usually run out of money before the end of the month’), 6 very low (‘I have serious financial troubles’), with 2 not responding.
The study aimed for a sample size capable of detecting small effect sizes A priori power analysis with G*Power 3.1.9.7. (Faul et al., 2009) suggested a minimum of 402 participants was needed for five predictors, a small effect size of 0.05, 95% power, and an alpha of 0.05. Aiming to include four demographic variables as covariates, the target was at least 481 participants.
Recruitment occurred through course credit for university students and voluntary participation via social media and personal contacts for others. A link to an anonymous online survey in Qualtrics was shared with university students who signed up for a research credit course. Other participants were reached through social media, where we posted the link to the anonymous survey and asked our acquaintances to fill out the survey and share the link. University students voluntarily helped us distribute the link, reaching a diverse audience. We also sent the link to some acquaintances in private messages.
After consenting, participants answered questions on political dispositions. Following this, participants responded to questions assessing their attitudes toward mental illnesses in general.
Subsequently, participants were asked to read three vignettes depicting a target person experiencing a specific mental health problem. The vignettes were adapted from Link et al.’s (1999) research. The vignettes depicted János, Mihály, and Zoltán who were described as experiencing the symptoms of major depression, schizophrenia, and AUD, respectively. The names of the three target persons were typical Hungarian male first names. Following each vignette, several measures were employed to assess stigma toward the respective target person.
Finally, participants were thanked and debriefed. University students who participated for course credit were able to provide their identification details through a separate link, with the assurance that their responses would remain anonymous. This procedure was approved by the ethics committee of [Anonymous] University.
Measures
Predictor variables: Political dispositions and political ideology
RWA was assessed using 10 items based on the Hungarian adaptation of the RWA Scale by Enyedi (2004) and Fábián (1999), originally developed by Altemeyer (1981). An example item is, ‘It is always better to trust the judgment of the proper authorities in government and religion than to listen to the noisy rabble-rousers in our society, who are trying to create doubt in people’s minds’.
SDO was assessed using the 16-item SDO7 scale (Ho et al., 2015), adapted to Hungarian by Faragó & Kende (2017). An example item is, ‘We should not push for group equality’.
GSJ was assessed using the eight-item GSJ Scale (Jost et al., 2003), adapted to Hungarian by Berkics (2009). An example item is ‘In general, you find the Hungarian society to be fair’.
ESJ was measured using the 17-item ESJ Scale (Jost & Thompson, 2000), translated into Hungarian by Jost and Kende (2020). An example item is ‘If people work hard, they almost always get what they want’.
Liberal-conservative ideological self-placement was assessed using three items: ‘In political/economic/societal-cultural matters, people sometimes talk about conservatives and liberals. How would you generally describe your views on this scale?’
Items for RWA, SDO, and liberal-conservative self-placement were rated on 7-point scales from ‘strongly disagree’/‘extremely liberal’ to ‘strongly agree’/‘extremely conservative’. For ESJ and GSJ, 9-point scales from ‘strongly disagree’ to ‘strongly agree’ were used. Indexes for these variables were calculated by averaging the scores of all respective items.
Outcome variables
Generic scales assessing mental illness-associated stigma
The Attitudes Toward Mental Illness (AMIS; Kobau et al., 2010) is a 7-item scale designed to measure two subscales of mental health stigma: negative stereotypes associated with mental illnesses (AMIS-1; ‘I believe a person with mental illness is a danger to others’), and beliefs about recovery (AMIS-2; ‘I believe a person with mental illness can eventually recover’).
Participants’ openness to future interactions with individuals who have mental health problems was assessed using a 4-item version of the Reported and Intended Behavior Scale (RIBS; Evans-Lacko et al., 2011). An example of an item is ‘In the future, I would be willing to work with someone with a mental health problem’.
Items were assessed using 5-point scales, ranging from ‘strongly disagree’ to ‘strongly agree’. Indexes for these variables were calculated by averaging the scores of all respective items. Positively worded items were recoded so that index scores reflect negative stereotypes and behavioral intentions.
Specific measures assessing stigma related to specific mental illnesses
After reading each vignette, participants’ attitudes toward the individuals depicted with a specific mental illness (namely schizophrenia, depression, and AUD) were assessed using various measures. These included assessments of social distance, support for structural discrimination, and the belief in a continuum of symptom experience.
Desire for social distance was assessed using five items based on Link et al. (1999). An example of an item is ‘How willing would you be to move next door to the person depicted in the vignette?’
Support for structural discrimination of the target person was measured with two items: ‘If the person in the vignette does not consent to medical treatment, he should receive compulsory treatment’ and ‘The person in the vignette should not be allowed to have a driving license’ (Schomerus et al., 2019).
Belief in a continuum of symptom experience was assessed with two items: ‘Basically, we are all sometimes like the target person, it is just a question of how pronounced this state is’ and ‘To some extent, everyone experiences similar problems as the target person’ (Schomerus et al., 2013).
Each Likert item, following the vignettes, was rated on a 5-point scale, and responses were recoded so that higher values indicate a greater desire for social distance, more support for structural discrimination, and less belief in a continuum of symptom experience.
Control variables: Demographic variables
We collected demographic data, including age (continuous), gender (dichotomous: 0 for male, 1 for female), educational level (four response options from ‘unfinished primary school’ to ‘completed master’s/Ph.D.’), and SES (four response options from ‘serious financial troubles’ to ‘money for everything’). In the linear regression analyses, we controlled for the effects of age, gender, and SES (educational level was excluded due to high homogeneity). SES was simplified to a dichotomous variable, with 0 representing low and very low SES, and 1 representing high and very high SES.
Data analysis
The statistical analysis was conducted using IBM SPSS 25.00 (IBM Corporation, Chicago, 2017). Initially, we explored zero-order correlations between study variables. We then conducted multiple linear regression models, with political dispositions and ideology as predictors and indicators of mental health stigma as dependent variables.
We controlled for age, gender, and SES in our models. To address the risk of Type I error inflation from multiple comparisons, we applied the Bonferroni correction, adjusting our alpha level. This resulted in a corrected p-value threshold of .0008 (.05 divided by 60) for analyses without demographic covariates, and .0005 (.05 divided by 96) for analyses with demographic covariates.
Results
Descriptive analysis
Table 1 presents descriptive statistics, reliability estimates, and Pearson correlations for study variables.
Descriptive statistics, correlation coefficients, and reliability measures for study variables.
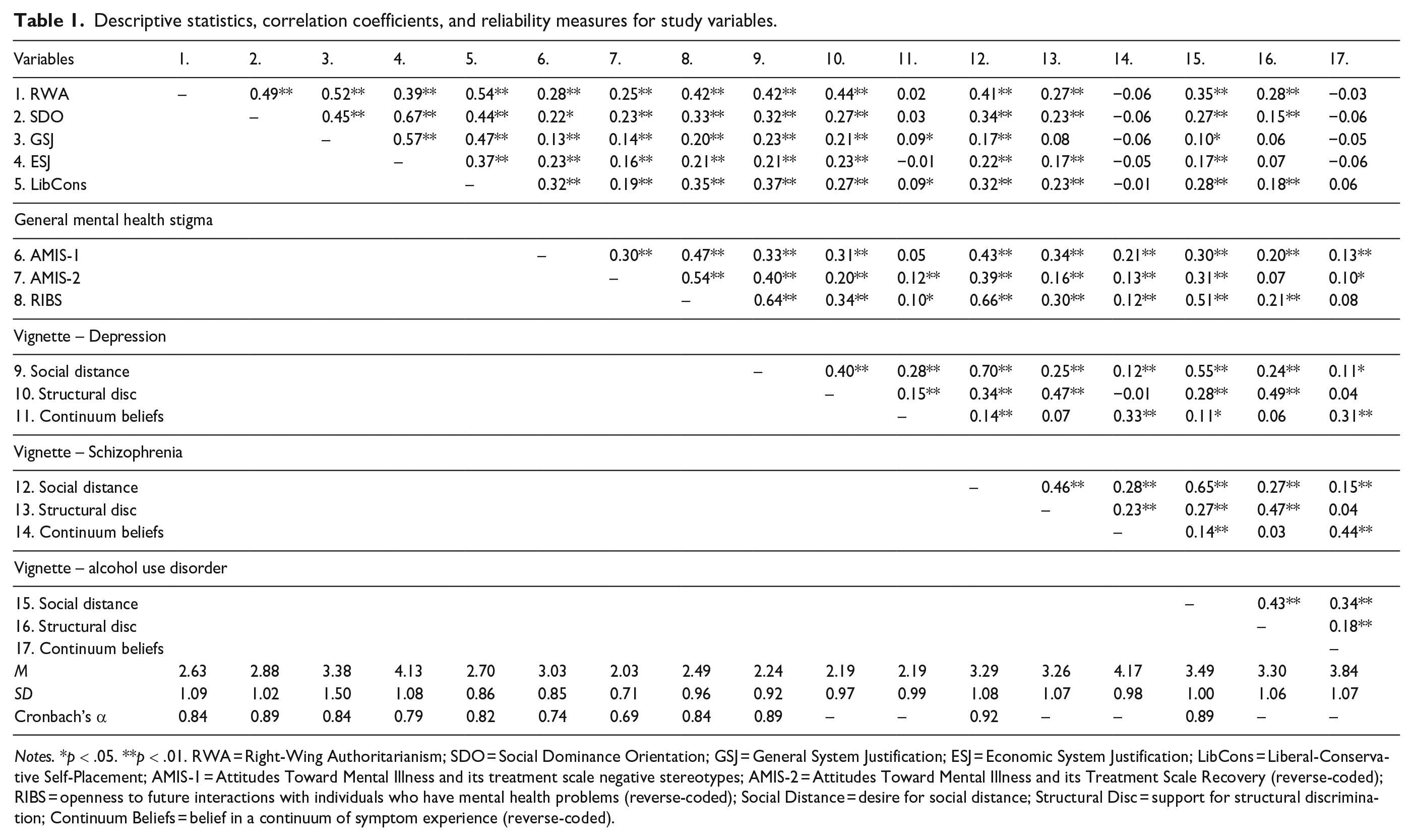
Notes. *p < .05. **p < .01. RWA = Right-Wing Authoritarianism; SDO = Social Dominance Orientation; GSJ = General System Justification; ESJ = Economic System Justification; LibCons = Liberal-Conservative Self-Placement; AMIS-1 = Attitudes Toward Mental Illness and its treatment scale negative stereotypes; AMIS-2 = Attitudes Toward Mental Illness and its Treatment Scale Recovery (reverse-coded); RIBS = openness to future interactions with individuals who have mental health problems (reverse-coded); Social Distance = desire for social distance; Structural Disc = support for structural discrimination; Continuum Beliefs = belief in a continuum of symptom experience (reverse-coded).
A moderate positive correlation exists among political dispositions and ideology measures, indicating they share a psychological basis but are distinct constructs. RWA, SDO, and conservatism were associated with stigma related to mental illnesses, except disbelief in a continuum of symptom experience. Higher scores on these scales were correlated with negative stereotypes, reduced optimism about recovery, and an increased desire for social distance, showing a pattern of reluctance to engage with individuals with mental health problems generally, and schizophrenia, depression, or AUD specifically. Additionally, there was a greater willingness to support structural discrimination.
The correlations between GSJ and ESJ with mental health stigma were less consistent. Although there were significant correlations with some stigma indicators, these were generally weak. Furthermore, many indicators of mental health stigma showed non-significant correlations with both forms of system justification.
Interestingly, the strengths of the correlations between various indices of mental health stigma varied considerably. Measures of social distance tended to be moderately or highly correlated with each other across mental health issues. Specifically, individuals who desired distance from one form of mental health issue also tended to desire distance from individuals with other types of mental health issues. However, measures of support for structural discrimination and (dis)belief in a continuum of symptom experience had lower correlations across different mental health issues and with measures of social distance.
Main analysis
We conducted regression analyses to identify the key political dispositions and ideologies underlying mental health-related stigma. The dependent variables were regressed on political and demographic measures. Results, presented without covariates in Table 2 and with covariates in Supplemental Table S1, show RWA’s significant association with most outcomes, highlighting its critical role in shaping mental health stigma.
Results of regression analysis with political dispositions and ideologies as predictors and mental health-related stigma as outcomes.
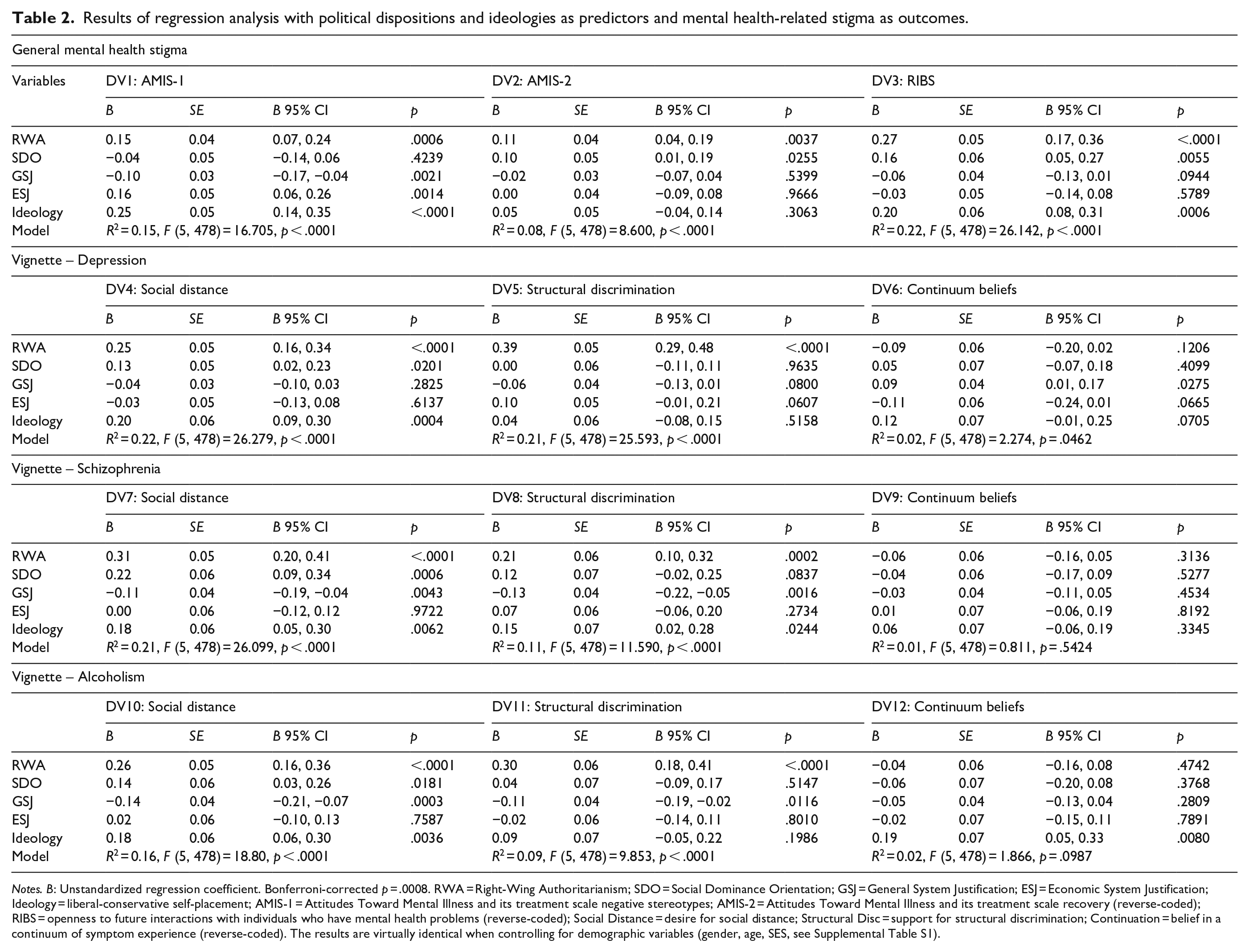
Notes. B: Unstandardized regression coefficient. Bonferroni-corrected p = .0008. RWA = Right-Wing Authoritarianism; SDO = Social Dominance Orientation; GSJ = General System Justification; ESJ = Economic System Justification; Ideology = liberal-conservative self-placement; AMIS-1 = Attitudes Toward Mental Illness and its treatment scale negative stereotypes; AMIS-2 = Attitudes Toward Mental Illness and its treatment scale recovery (reverse-coded); RIBS = openness to future interactions with individuals who have mental health problems (reverse-coded); Social Distance = desire for social distance; Structural Disc = support for structural discrimination; Continuation = belief in a continuum of symptom experience (reverse-coded). The results are virtually identical when controlling for demographic variables (gender, age, SES, see Supplemental Table S1).
Conservative political ideology had a more selective impact, significantly predicting negative stereotypes related to mental illnesses in general, as well as the desire for social distance from individuals exhibiting symptoms of mental illness in general and specifically from those with symptoms of depression, schizophrenia, and AUD. The other predictors – GSJ, ESJ, and SDO – largely failed to predict outcomes, suggesting minimal contributions beyond RWA to mental health stigma.
Discussion
Our study aimed to conceptually replicate and extend research on the role of political dispositions and ideology in mental health stigma. First, we sought to replicate findings from the U.S. and Sweden indicating that RWA predicts mental health stigma (DeLuca & Yanos, 2016; DeLuca et al., 2018; Löve et al., 2019). Secondly, we aimed to expand upon these findings. Previous research in this context has focused mainly on RWA and self-reported political ideology or affiliation. By including a wider array of measures, we intended to explore whether other belief systems associated with a politically conservative ideology could add to our understanding of the processes underlying mental health stigma.
The concepts that we studied, RWA, SDO, and system as well economic justification, could, in theory, have been expected to be associated with mental health stigma through different processes. An association between RWA and stigma could be due to the perceived dangers associated with mental health issues. On the other hand, an association between SDO and stigma would indicate the importance of distancing oneself from perceived subordinate groups. In turn, those who believe in the (economic) system could be expected to blame individuals for their misfortunes. Finally, those who identify as conservative, with its emphasis on the status quo, norms, uniformity, and homogeneity, may dislike those who deviate from and thereby perhaps question standards of ‘normality’.
Our study compared the above dispositions and ideologies as predictors of various types of mental health stigma in Hungary, a novel context for this type of research. Hungary’s high prevalence of mental illness, significant stigma against mental health patients (Buchman-Wildbaum et al., 2018; European Commission, 2023; Krupchanka & Winkler, 2016), and the dominance of right-wing ideologies (Bíró-Nagy et al., 2022; Lönnqvist et al., 2021; Várnagy, 2023) present a unique backdrop for examining how individual political orientations influence mental health stigma. Given both the strength of mental health stigma and right-wing ideologies, one could have expected stigma to be normalized to the degree that there would be little if any room for the explanatory power of individual differences. Hungary was, in this respect, a setting that allowed for a hard test of the notion that what people think regarding political and social questions can help understand mental health stigma. Our results suggest that even in this context, individual differences in political dispositions, RWA in particular, can help understand a wide range of stigmas associated with various mental health issues. These findings corroborate previous research from the U.S. and Sweden, providing evidence for the replicability of these results across very different types of national contexts.
Although individual-level results cannot be generalized to explain group (or country) level phenomena, our results suggest that a political leadership that has built its electoral success on protecting the normative Hungarian way of life from, for instance, the liberal financial elite and foreign intelligence agencies, who have allegedly tried to impose for instance, forced immigration and an LGBQT agenda (Szabó, 2020), may have created a mass public that fears everything ‘other’, including people with mental health issues, Hungary has very low levels of help-seeking behavior, inadequate professional support for mental health issues, and the pervasive perception of differential treatment of mental health patients (European Commission, 2023). If, as our results suggest, RWA –characterized by fear of the dangerous other – influences mental health stigma, then the Hungarian leadership may have successfully cultivated an electorate fearful of all that is not ‘normal’.
Concepts like ‘Otherness’ and ‘Othering’ have become influential in explaining not only stigma and racism but also the perpetuation of social injustices. The governing party’s framing of the majority ingroup as hegemonically normative and minority outgroups as alien (Bhugra et al., 2023) can embed harmful institutional patterns within policies, laws, and social practices (Akbulut & Razum, 2022). Othering legitimizes disadvantageous institutional structures and social practices and is structurally embedded in power and representation discourse (Akbulut & Razum, 2022). Discrimination and stigmatization of individuals with mental health issues may be by-products of constructing the ‘Other’ (Bhugra et al., 2023). Such social identity formulations and related national policies significantly influence beliefs about people with mental illnesses, such as perceived dangerousness, as evidenced by a study of U.S. public view trends from 1996 to 2018 (Pescosolido et al., 2019).
Understanding the role of perceived threat in mental health stigma is key to developing effective interventions in Hungary. This perception may explain why individuals with symptoms of schizophrenia and AUD, often linked to danger, face greater stigma than those with depression, seen as less threatening (Kilian et al., 2021; Mannarini & Boffo, 2015; Marie & Miles, 2008; Penn et al., 1999). Although similar differences were found in a study employing U.S. samples (Pescosolido et al., 2019), depression may also be seen as more normative in Eastern Europe where general life satisfaction is lower (Djankov et al., 2016).
Mental health stigma reduction programs often focus, understandably, on the targets of stigma, and concentrate on micro-level factors to improve conditions for people living with mental illness. These interventions typically employ strategies of education contact, or a combination of both, to mitigate stigma, both among those directly and indirectly affected (Corrigan et al., 2001; Gronholm et al., 2017; Morgan et al., 2018). Recent research, however, has expanded our understanding of stigma, with Tyler and Slater (2018) emphasizing its use as a tool for social control through political and cultural power, and Kapadia (2023) advocating for recognizing its structural dimensions. Our findings support the notion that interventions should not only focus on those directly experiencing stigma but also address individuals and the broader context that perpetuates it. While acknowledging the benefit of education and social contact, our research, in conjunction with other studies (Kapadia, 2023; Kohrt et al., 2018; Tyler & Slater, 2018), highlights the complex connections between macro-level political ideologies and micro-level perceptions of threat. This complex web of influences suggests that stigma reduction efforts need to be multifaceted, addressing both individual attributes and the larger societal and political structures that sustain them.
While advocating for broad societal changes in response to mental health issues might seem overly ambitious, acknowledging the influence of political dispositions and ideologies on mental health stigma is crucial. Interventions should target the core concerns of those stigmatizing others, including the perceived threats posed by mental illnesses. Future research should aim to identify exactly ‘what is at stake’ (Yang et al., 2014); that is, why do people feel threatened, and explore ways to alleviate perceived threats posed by non-conventional identities.
Limitations and strengths
The study has several limitations. First, the study does not allow for causal inferences. Causal pathways are seldom if ever possible to identify in survey studies (for an excellent discussion on the role that colliders, confounders, and mediators can play in any results, see Wysocki et al., 2022). Secondly, our sample, being relatively well-educated and middle-class, might not accurately represent the general Hungarian population, possibly affecting the generalizability of our findings. The impact of SDO and system justification could vary across different socioeconomic groups. Thirdly, all vignette subjects were male. Some research has shown that gender-typical disorders (e.g. a male with AUD) might be targets of harsher stigma; such cases may be less likely to be perceived as genuine mental disturbances (Wirth & Bodenhausen, 2009). Future research should collect a more diverse sample in terms of education and socioeconomic status and consider the target person’s gender as a potential moderator in the associations between political ideology and stigma.
The study’s strengths include the simultaneous investigation of multiple indicators of political ideology as determinants of a broad spectrum of stigma outcomes. Conducted in an understudied context in which mental health stigma is both very prevalent and a significant barrier to utilizing professional mental health services, this research may offer both theoretical and practical insights. Importantly, our findings indicate that perceived danger, threat, and unconventionality, as indicated by RWA – not derogation indicated by SDO nor belief in an (economically) just system – are key in mental health stigmatization. This is what intervention programs should target. This research is particularly relevant for researchers and practitioners in contexts with dominant right-wing conservative ideologies and strong hostility toward non-conventional identities.
Supplemental Material
sj-docx-2-isp-10.1177_00207640241267803 – Supplemental material for Right-wing authoritarianism, social dominance, system justification, and conservative political ideology as predictors of mental health stigma: The Hungarian case
Supplemental material, sj-docx-2-isp-10.1177_00207640241267803 for Right-wing authoritarianism, social dominance, system justification, and conservative political ideology as predictors of mental health stigma: The Hungarian case by Zsolt Péter Szabó, Jan-Erik Lönnqvist, Nóra Anna Lantos and Jussi Valtonen in International Journal of Social Psychiatry
Research Data
sj-sav-1-isp-10.1177_00207640241267803 – for Right-wing authoritarianism, social dominance, system justification, and conservative political ideology as predictors of mental health stigma: The Hungarian case
sj-sav-1-isp-10.1177_00207640241267803 for Right-wing authoritarianism, social dominance, system justification, and conservative political ideology as predictors of mental health stigma: The Hungarian case by Zsolt Péter Szabó, Jan-Erik Lönnqvist, Nóra Anna Lantos and Jussi Valtonen in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The authors would like to thank all participants involved in the study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Data availability statement
The data analyzed in this study are included with the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.