
Abstract
Background:
Feelings of shame are linked to increased risk for depression. Little is known about protective factors that may buffer this effect, particularly in men. Using prospective data from a community sample of Australian men, we examine the extent to which shame is associated with depressive symptoms, and the protective role of psychological wellbeing, specifically environmental mastery and purpose in life.
Methods:
Participants (n = 448) were from the longitudinal Men and Parenting Pathways (MAPP) Study. Measures were the Event Related Shame and Guilt Scale for shame, the DASS-21 for depressive symptoms and Ryff’s Scales of Psychological Well-Being for environmental mastery and purpose in life. Linear regressions were used to test associations between shame and depressive symptoms concurrently and 1-year later, and the moderating effects of mastery and purpose in life.
Results:
Shame was strongly associated with concurrent depressive symptoms (βunadj = .76, p < .001; βadj = .63, p < .001). This effect was weaker in men with high compared to low environmental mastery (β+1 SD = .46, p < .001; β−1 SD = .55, p < .001) and purpose in life (β+1 SD = .48, p < .001; β−1 SD = .62, p < .001). Shame also predicted subsequent depressive symptoms after adjustment for prior depressive symptoms (βunadj = .59, p = .001; βadj = .34, p = .004), although environmental mastery or purpose in life did not moderate these associations.
Conclusions:
Our findings suggest that promoting a sense of psychological wellbeing in men may confer protective proximal effects in the context of shame, potentially attenuating depression severity. The current study aligns with calls for strength-based approaches to reducing mental health problems in men.
Lifetime prevalence of depression in men is estimated at 14.7% (Hasin et al., 2018) and is increasing (Moreno-Agostino et al., 2021). Resulting social and economic costs include loss of income, reduced productivity, escalation of physical and psychiatric comorbidities and heightened risk of suicide (Arnaud et al., 2022; Haregu et al., 2020; Martin et al., 2013; McTernan et al., 2013; Schofield et al., 2019; Schuch et al., 2014; Zajac et al., 2022). A frequently reported and modifiable precursor of depression is a sense of shame (Andrews et al., 2002; Mills et al., 2013; Stuewig & McCloskey, 2005). Shame is a negative self-conscious emotion experienced when one believes they have failed to actualise internalized social standards (Orth et al., 2010; Tracy & Robins, 2004). It encompasses a reproachful evaluation of the self, feelings of worthlessness and the desire to hide (Ferguson et al., 1999; Kim et al., 2011). Few longitudinal studies have investigated the mental health impact of shame in adult men. Further, protective factors that moderate the relationship between shame and depressive symptoms in men are yet to be explored, despite the potential for such studies to inform targets for intervention.
Shame is associated with depression-related cognitions such as attributing negative events to global and stable causes and perceiving the self as flawed (Tilghman-Osborne et al., 2008). A meta-analysis of 86 cross-sectional studies reported a substantial mean-weighted unadjusted effect size for the relationship between shame and depressive symptoms (r = .43; Kim et al., 2011). Only four of the included studies reported specifically, or mostly (>70%), on men (range r = .23–.53; Bybee et al., 2009; Farmer & Andrews, 2009; Tangney et al., 2007; Tiggemann & Kuring, 2004). High-quality evidence implicating men’s shame in subsequent depression is lacking. Prior longitudinal studies in young, mixed gender samples suggest shame may precede depression (Andrews et al., 2002; Mills et al., 2013; Stuewig & McCloskey, 2005). Men may experience specific vulnerability to shame-induced depression arising from internalised pressure to conform to unachievable masculine ideals (Rice et al., 2016). High conformity to restrictive traditional masculine values such as self-reliance has been linked to depressive symptoms in older men and suicidal ideation in younger men (Herreen et al., 2021; King et al., 2020). Both conformity, which obstructs access to support, and failure to conform, which may elicit feelings of powerlessness and inadequacy, can precipitate internalised shame and associated depressive symptoms (Rice et al., 2016).
Men are less likely than women to access mental health care when needed (Coates et al., 2019; M. G. Harris et al., 2016; Yousaf et al., 2015) and experience gender specific barriers to accessing that care (Macdonald et al., 2022). Once in therapy, feelings of shame upon presentation are one factor associated with greater risk of dropout (Seidler et al., 2021). Thus, it is necessary to identify factors that may mitigate effects of shame and promote therapeutic engagement. Potential interventions may be those that align with the recent shift to a strength-based approach to masculinities in treating men’s mental health (Seidler et al., 2018; Wilson et al., 2022). Such approaches have had success in reduction of depressive symptoms and may be particularly effective when they focus on existentially-oriented strengths such as psychological wellbeing (Bolier et al., 2013).
Two indicators of psychological wellbeing that may lessen the effects of shame on depressive symptoms are environmental mastery and purpose in life. Environmental mastery is an individual’s ability to choose or create environments based on their personal needs and values whilst purpose in life is defined as an individual’s capacity to have goals, intentions and a sense of direction in life (Ryff, 1989a). In prior research, these indicators of psychological wellbeing have been linked to positive outcomes such as resilience and greater longevity (Hill & Turiano, 2014; Mayordomo et al., 2016) and in men specifically, linked to reduced negative outcomes such as loneliness and psychological distress (Mansour et al., 2021; Palma et al., 2022). There is also evidence to suggest that environmental mastery and purpose in life may be negatively associated with internalised self-stigma, a core feature of which is shame (Ehrlich-Ben Or et al., 2013; Pérez-Garín et al., 2015; Rose et al., 2018). Further, in a large cohort of men and women (N = 5,566), those with low environmental mastery and purpose in life were also more likely to be depressed 10 years later (Wood & Joseph, 2010). While these results were not separated by gender, they suggest these indicators of psychological wellbeing may offer a promising target in efforts to disrupt the shame-depression nexus.
The objectives of this study were threefold. First, we sought to describe rates and domains of shame as reported by men aged in their 30s in an Australian longitudinal community cohort. Second, we aimed to assess concurrent relationships and longitudinal associations between men’s shame and depressive symptoms 1-year apart. Finally, we aimed to explore potential moderating effects of environmental mastery and purpose in life on the association between shame and depressive symptoms. We hypothesised shame would be positively associated with depressive symptoms, concurrently and 1 year later, and the strength of the association would be weaker in men who report higher levels of environmental mastery and purpose in life.
Method
Participants
Participants were from the Men and Parenting Pathways (MAPP) Study (N = 608), a longitudinal cohort study examining the mental health and wellbeing of Australian men (Macdonald et al., 2021). English speaking, Australian resident men, aged between 28 and 32 years (approaching the median age in Australia for transition to fatherhood; Australian Bureau of Statistics, 2016) were recruited between 2015 and 2017. Recruitment was through paid social media and partnerships with community organisations, adopting strategies that were shown in the Australian Longitudinal Study of Women’s Health to successfully achieve representativeness (Loxton et al., 2015). For example, during the recruitment period, sample characteristics were closely monitored guiding the targeting of social media posts and traditional media promotion towards underrepresented population sectors, locales or SES groups (Macdonald et al., 2021). At Wave 1, these strategies achieved a MAPP cohort representative of the Australian population on most key demographic characteristics, however, fewer men were born outside of Australia and a higher proportion of men were in paid employment compared to the proportion reported in the Australian 2016 census (Australian Bureau of Statistics, 2017; Macdonald et al., 2021). Data were provided via self-reported online surveys on the REDCap secure web platform (P. A. Harris et al., 2009) administered annually across five waves. Consent for ongoing participation was provided online prior to the first survey. Ethics approval was obtained from Deakin University, Faculty of Health, Human Ethics Advisory Group, project identifier HEAG-H-192-2014. Participants included in the current study (n = 448) were those who provided data on either depressive symptoms, shame, environmental mastery or purpose in life at Waves 4 or 5.
Measures
Predictor
Shame
The shame subscale from the Event-Related Shame and Guilt Scale (Orth et al., 2006) was included for the first time in the MAPP Study at Waves 4 and 5 to measure feelings of shame experienced in the previous week. There are 4 items in this scale, including ‘I felt small’ and ‘I wanted to hide’. The response options ranged from 0 = Not at all right to 5 = Completely right. Mean scores with a possible range of 0 to 5 where higher scores indicate higher shame were calculated for this analysis, consistent with the scale literature (Orth et al., 2006). Internal consistency for this scale was excellent (Wave 4; Cronbach’s α = .90, Wave 5; Cronbach’s α = .92). Men were further asked to select all that apply from four domains (i.e. work, family, partner and children) to which their feelings of shame were related.
Outcome
Depressive symptoms
The DASS-21 is a self-report inventory measuring symptoms of depression, anxiety and stress over the past week (Lovibond & Lovibond, 1995). At Waves 4 and 5, depressive symptoms were measured with the 7-item depression subscale. Participants responded using a 4-point scale ranging from 0 = Did not apply to me at all to 3 = Applied to me very much, or most of the time. The total score was calculated and then doubled to align with DASS-42 norms, as per scoring instructions (Lovibond & Lovibond, 1995), resulting in a range of possible scores from 0 to 42, where high scores reflect greater severity of depressive symptoms. Internal consistency for this scale was excellent (Wave 4; Cronbach’s α = .92, Wave 5; Cronbach’s α = .93). A continuous total score was used in analyses; however, for interpretation of results, the designated severity ranges are: normal (0–9), mild (10–13), moderate (14–20), severe (21–27) and extremely severe (28+; Lovibond & Lovibond, 1995). The DASS-21 has been validated against clinical diagnostic tools as a screening measure for depression (Ng et al., 2007) and shown construct validity in non-clinical samples (Henry & Crawford, 2005; Sinclair et al., 2012).
Moderators
Environmental mastery and purpose in life
Environmental mastery and purpose in life were measured at Waves 4 and 5 using the two 7-item subscales of the same names from Ryff’s (1989b) Scales of Psychological Well-Being. Participants responded regarding how they feel about life in general. Response options ranged from 1 = Strongly disagree to 6 = Strongly agree. Possible scores range from 7 to 42. Higher scores indicate higher levels of mastery or purpose. These subscales had good internal consistency (Wave 4; Cronbach’s α = .84 for mastery and .82 for purpose, Wave 5; Cronbach’s α = .86 for mastery and .83 for purpose) and have been assessed for construct validity (Ryff & Singer, 2006).
Potential confounders
Prior studies have shown depression is both a predictor and outcome of shame (Stuewig & McCloskey, 2005; Tilghman-Osborne et al., 2008) and future depression (Kendler & Gardner, 2010). Thus, to reduce the possibility of reverse causation (VanderWeele, 2019), analyses controlled for prior depressive symptoms by adjusting for the average of DASS-21 mean scores at Waves 1, 2 and 3. Adjustments were also made for possible demographic confounders including; country of birth (0 = Australia, 1 = Outside Australia), education at Wave 3 (0 = greater than year 12, 1 = year 12 or less) and household weekly income at below the designated household ‘poverty line’ (Wilkins, 2017), at Wave 3 (0 = greater than or equal to $AUD1,150 weekly, 1 = less than $AUD1,150 weekly).
Statistical analyses
Data were prepared and analysed in Stata v.17 (StataCorp, 2021). Data on shame, depression and well-being were first summarised. Concurrent relationships (i.e. repeated measures at Wave 4 and 5) were examined using linear regressions estimated via Generalised Estimating Equations (GEEs) with an exchangeable working correlation. Longitudinal relationships (i.e. exposure at Wave 4 and outcome at Wave 5) were examined using linear regressions. Concurrent models were first run adjusted for wave of outcome and then adjusted for wave and potential confounding factors. Longitudinal models were run unadjusted and then adjusted for potential confounding factors. Finally, both concurrent and longitudinal models were run adjusted for potential confounders and including interaction terms for each moderator. A robust variance estimator was employed in all analyses. Continuous variables were z-scored standardised for ease of interpretation. Therefore, in results, standardised betas (β) can be interpreted as standard deviation (SD) changes in depression associated with a 1 SD increase in shame.
Multivariate normal imputation was used to address missing data; 50 data sets were imputed and combined to derive proportions and model estimates (Rubin, 2004). Binary variables were imputed as continuous variables and then transformed after imputation, using adaptive rounding (Bernaards et al., 2007).
Results
Missing data and descriptive statistics
One hundred and sixty participants were excluded from analyses due to no data on any key variables at relevant waves. Table 1 presents the Wave 1 (baseline) characteristics of the analytic sample (n = 448) compared to the excluded sample. Compared to the excluded participants, participants in the analytic sample were more likely to be those who at Wave 1 had higher household income and higher education. In the retained sample, missing data for the predictor, outcome and moderator variables ranged from 10% to 15%. Mean age at Wave 4 was 33.15 years (SD = 1.41).
Baseline analytic sample characteristics compared to excluded participants.
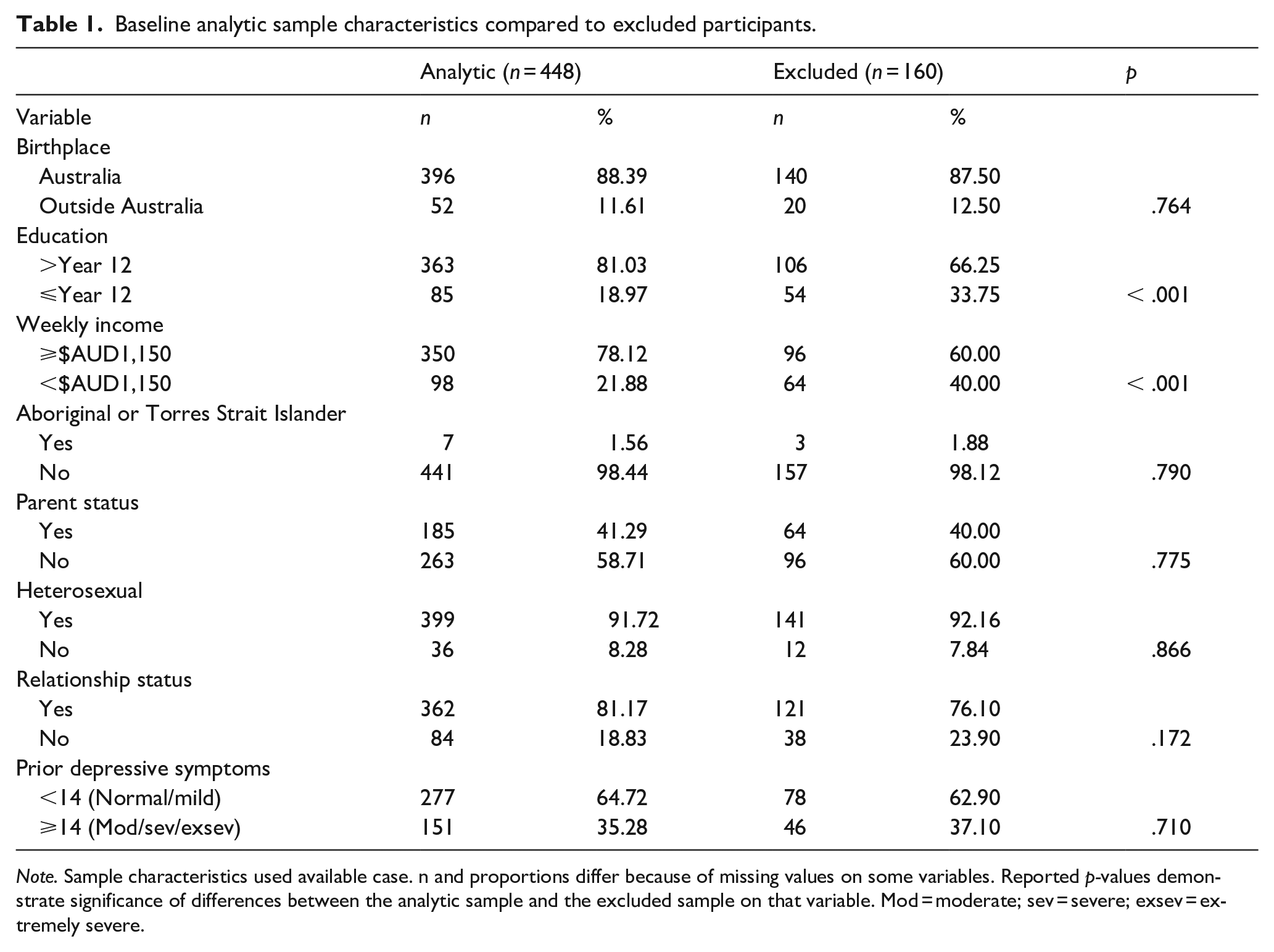
Note. Sample characteristics used available case. n and proportions differ because of missing values on some variables. Reported p-values demonstrate significance of differences between the analytic sample and the excluded sample on that variable. Mod = moderate; sev = severe; exsev = extremely severe.
Table 2 presents means, standard deviations and correlations for the key study variables. All variables were significantly correlated. In comparison to shame scores reported in the validation study (M = 0.97, SD = 1.24; Orth et al., 2006), scores at Wave 4 (M = 1.01, SD = 1.22; p = .736) and Wave 5 (M = 1.10, SD = 1.30; p = .294) were not different. At Waves 4 and 5, 29% to 31% of all participants reported no shame (i.e. endorsed ‘not at all’ to all items). For those who endorsed feeling shame, 47% to 48% reported their shame related to more than one domain. Within domains, 60% to 62% of men reported their shame related to work, 35% to 38% related it to family and 33% to 35% related it to their partner. In the subgroup of men who were fathers (Wave 4: n = 236, Wave 5: n = 257), 28% to 30% reported shame related to their children. The sample means for depressive symptoms at Waves 4 and 5 were within the DASS-21 ‘mild’ range. Means for environmental mastery and purpose in life at Waves 4 and 5 were approximately at the midpoints of the scales.
Descriptive statistics and correlations of key study variables.
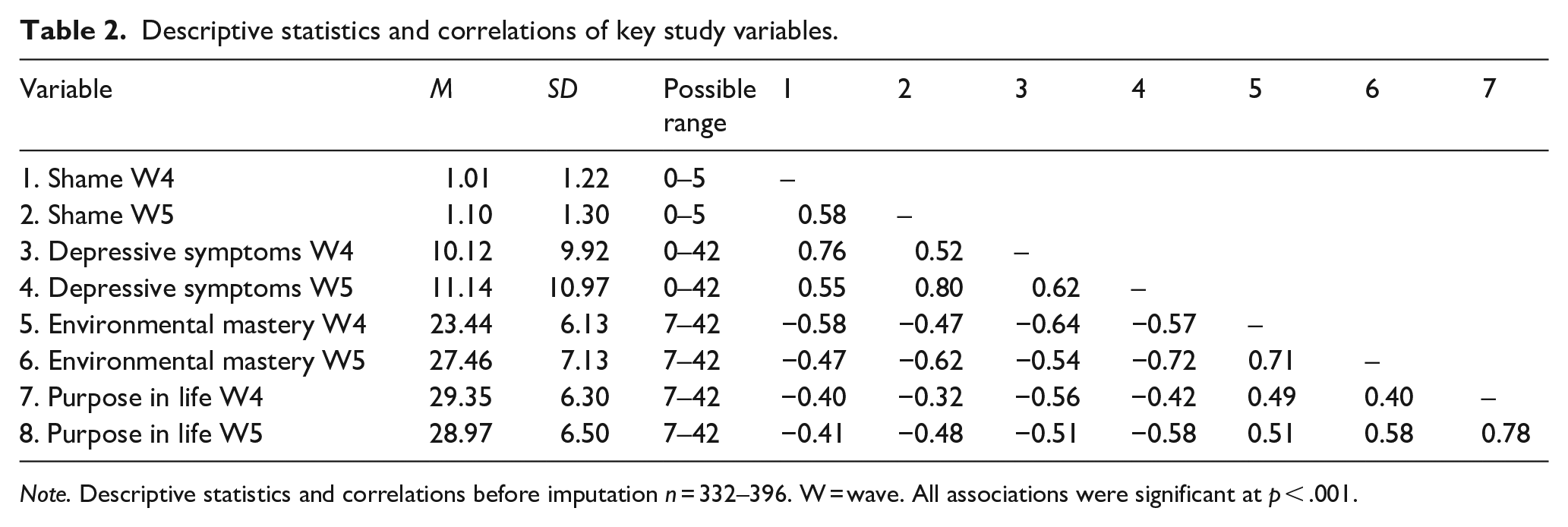
Note. Descriptive statistics and correlations before imputation n = 332–396. W = wave. All associations were significant at p < .001.
Concurrent and longitudinal associations between shame and depressive symptoms
Table 3 presents the concurrent and longitudinal associations between shame and depressive symptoms. Shame was concurrently associated with depressive symptoms when adjusting only for wave (β = .76, p < .001) and when additionally adjusting for potential confounding factors (β = 0.63, p < .001). In longitudinal models (1 year later), effects remained but were slightly attenuated (confounder unadjusted β = .59, p = .001; confounder adjusted β = .34, p = .004).
Concurrent and longitudinal associations between shame and depressive symptoms (n = 448).
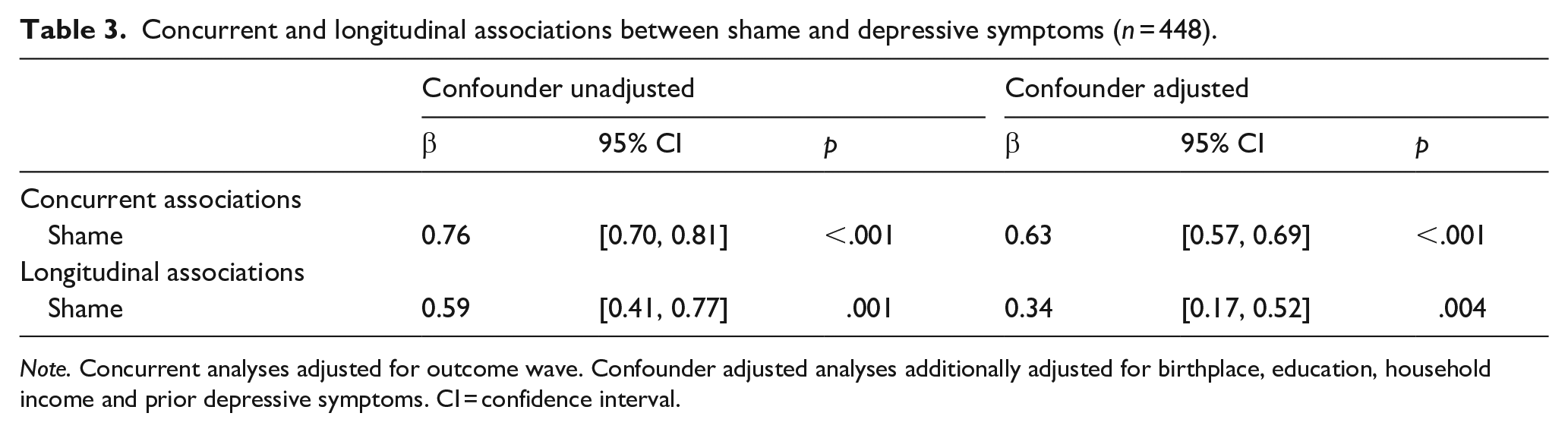
Note. Concurrent analyses adjusted for outcome wave. Confounder adjusted analyses additionally adjusted for birthplace, education, household income and prior depressive symptoms. CI = confidence interval.
Psychological wellbeing moderation
Figure 1 presents a graphic illustration of the interactions between psychological wellbeing indicators (i.e. environmental mastery and purpose in life) and shame in predicting depressive symptoms. In the concurrent analyses, after accounting for potential confounders, evidence suggests that both environmental mastery (p = .034) and purpose in life (p = .002) moderated the association between shame and depressive symptoms. Simple slope analyses suggested that the association between shame and depressive symptoms was higher when psychological wellbeing was low (−1SD) in comparison to high (+1SD) for both environmental mastery (β−1SD = .55, 95% CI [0.49, 0.61], p < .001; β+1SD = 0.46, 95% CI [0.35, 0.56], p < .001) and purpose in life (β−1SD = 0.62, 95% CI [0.56, 0.68], p < .001; β+1SD = .48, 95% CI [0.37, 0.59], p < .001). No interactions were evident in the longitudinal models for either environmental mastery (p = .274) or purpose in life (p = .132).
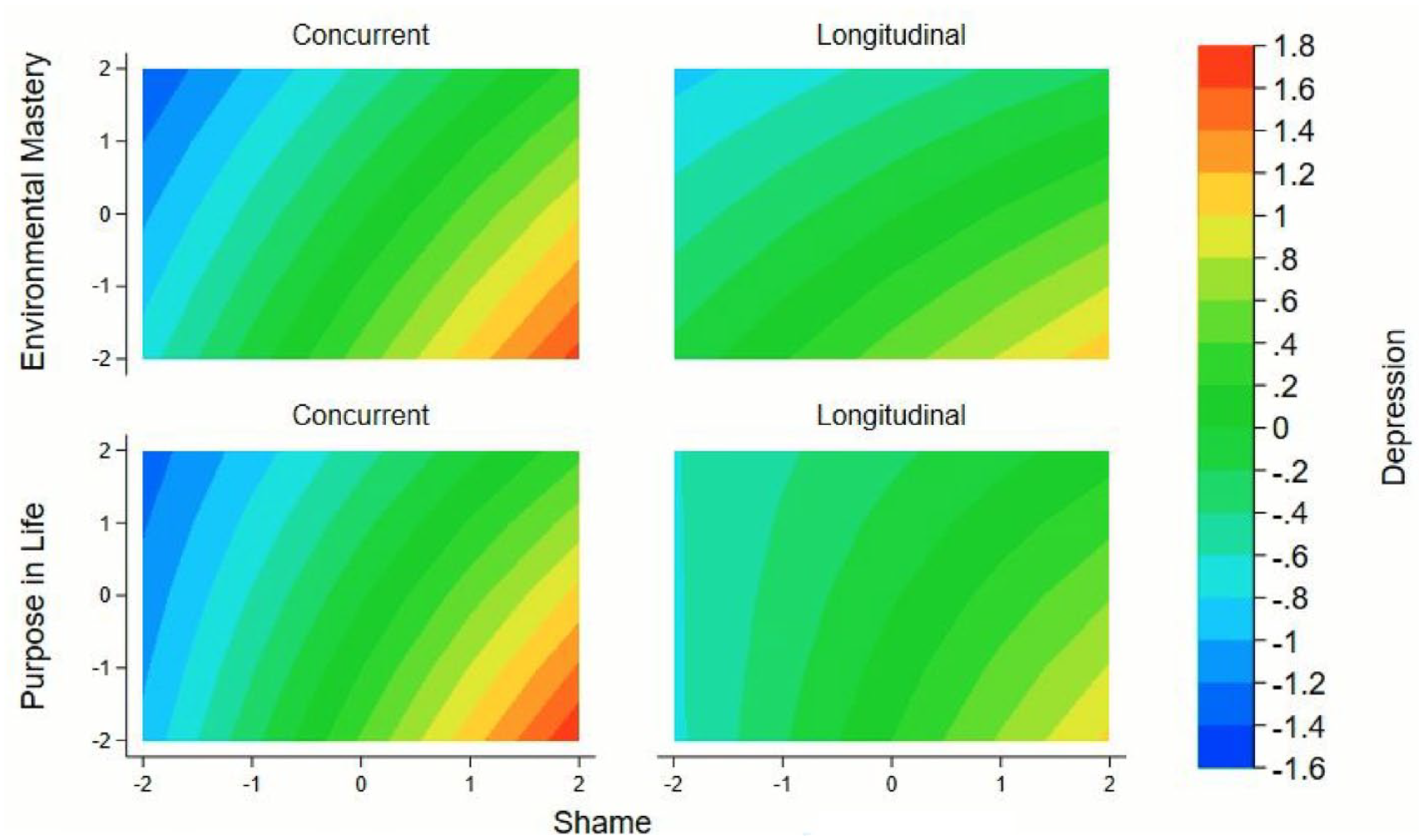
Contour plots presenting participants with elevated depressive symptoms at levels of shame and psychological wellbeing.
Discussion
In an Australian cohort, more than two thirds of men reported experiencing shame. Among these men, two thirds experienced shame related to work, over a third experienced shame related to their partner and over a third to family. Among those who were fathers, more than a quarter reported their shame was related to their children. Shame was associated with depressive symptoms concurrently and 1 year later. We also found that environmental mastery and purpose in life moderated concurrent, but not longitudinal, associations between shame and depressive symptoms. These findings implicate feelings of shame in risk for future depression in men. They also suggest that environmental mastery and purpose in life may offer some proximal protection against depressive symptoms in the context of shame, although may not be protective long term.
Consistent with and extending on past longitudinal research in child and adolescent and predominantly female samples (Andrews et al., 2002; Mills et al., 2013; Stuewig & McCloskey, 2005), we show that adult men’s experiences of shame predict subsequent depressive symptoms. That the association remained strong, after adjustment for prior symptoms of depression and confounding variables, suggests a potentially causal role of shame in men’s subsequent depressive symptoms. A plausible explanation for this relationship is that shame involves continued appraisals of the self as flawed, comparable to representations of the self as lacking worth, a common feature of depressive presentations (Zahn et al., 2015). Given that depression is a risk factor for suicide in men (Zajac et al., 2022) and that men around the median age for fatherhood may be at risk for depressive symptoms and suicidal ideation (Giallo et al., 2023), it is critical to understand and intervene on shame that may be experienced for men in this stage of life.
We found evidence suggesting that psychological wellbeing indicators, specifically environmental mastery and purpose in life, buffer, although do not fully suppress, the relationship between shame and concurrent depressive symptoms. These aspects of psychological wellbeing may be protective because they are characterised by future-focussed, goal-oriented states (Ryff, 1989a). Such states are the antithesis of rumination, evident in negative stable attributions about the past, inflexible coping and a sense of hopelessness, which are features of both shame and depression (Leonardi et al., 2020; Nolen-Hoeksema & Morrow, 1991). Consistent with this idea, environmental mastery and purpose in life have both been shown to be negatively correlated with rumination (Harrington & Loffredo, 2010). Because of this, both may provide some protection against the onset or maintenance of depressive symptoms in the context of shame by replacing rumination with goal-directed cognitions.
The moderating role of psychological wellbeing in the context of shame offers provisional support for the consideration of a strength-based approach when treating men who experience shame. Current interventions for shame use approaches such as cognitive behavioural therapy and mindfulness which effectively reframe shameful experiences and challenge cognitions (Goffnett et al., 2020). For men in particular, strengths-based (existentially-oriented) approaches may complement these conventional approaches. Men may be more likely to engage in treatment that promotes building strengths and focussing on goals (Seidler et al., 2018; Wilson et al., 2022). This may have the dual benefit of attenuation of depressive symptoms and motivation for ongoing engagement in treatment. Given that neither environmental mastery nor purpose in life were protective long term in this study, the importance of interventions that directly target shame remains.
It is also possible that the relationship is bi-directional, with depressive symptoms also contributing to feelings of shame. For men, stigma for mental health is widely reported and a barrier to accessing help (McKenzie et al., 2022). Seidler et al. (2019) investigated barriers to mental health services in a sample of men and found half of these men endorsed the item ‘I would feel embarrassed or ashamed to see a psychotherapist (counselor)’. Therefore, it is possible that shame occurs or may be exacerbated in the context of depressive symptoms. Given the impact of shame and self-stigma on men’s help seeking behaviour, further investigation in this area is warranted. To date, no studies have explored cross-lagged shame and depressive symptoms in men.
In this study, men experienced shame across several domains including work, and relationships with partners, family and children. Between 60% and 62% of men reported shame related to work. Prior research suggests workplace shame is more likely when employees make negative internal attributions about outcomes, such as a lack of ability (Daniels & Robinson, 2019), a similar construct to low mastery. Given men often place high value on paid work and income and on competencies within occupational and provider roles (Thébaud, 2010), organizational shame may arise from a sense of failure or inadequacy. This presents a role for organisations to be aware of mastery and attributions in the workplace and ensure adequate feedback and recognition about men’s strengths in their organisational roles. For fathers in this study, between 28% and 30% reported shame related to their children. Prior evidence from a systematic review links shame during the postnatal period with heightened symptoms of stress, anxiety and depression (Caldwell et al., 2021), with depression associated with detrimental ramifications for child development and wellbeing (Sweeney & MacBeth, 2016). Additionally, 33% to 35% of men reported shame related to their partner. Shame experienced within relationships is associated with impaired intimate relationship functioning and has been linked to psychological abuse in dating (Black et al., 2013; Harper et al., 2005). Given these implications, further investigation is needed on the content of shame related cognitions associated with children and relationships.
The domains in which men in this study experienced shame may be reflective of their current life stage, recently identified as ‘established adulthood’ (30–45 years; Mehta et al., 2020), during which the demands of career progression intersect with normative expectations such as maintaining relationships and caring for children (Mehta et al., 2020). Prior research suggests work strain and work-family conflict is highest for those in this age group because this is a time when pressures and demands from work and family are the most taxing on resources (Huffman et al., 2013; Rauschenbach & Hertel, 2011). At this stage, individuals are more likely to be working longer hours and seeking to define themselves in their career which means less time spent with their children, contributing to an increased sense of conflict between roles (Huffman et al., 2013). Some fathers feel disappointment when they miss key milestones during their children’s development, viewing work as an obstacle to their parental involvement (Scheibling, 2020). Thus, a perceived failure to fulfil the responsibilities of each role identity, central to this stage of life, may contribute to feelings of shame. The current study has extended the literature beyond associations between shame and adherence to restrictive masculine ideologies (Rice et al., 2016) by demonstrating men, particularly in established adulthood, may experience vulnerability to shame-induced depression associated with conflict around family and workplace role identities.
Strengths and limitations
Strengths of the current study include analysis of rare prospective data in an adult male sample, as well as adjustment for prior depressive symptoms and a range of potential confounding variables. This addressed limitations of previous research on shame and depression in men and increases confidence in the proposition made in prior research that shame is an antecedent of depression.
Several limitations must also be acknowledged. Typical of longitudinal studies, the MAPP cohort study experienced loss to follow up. Some of these missing data were managed with imputation. However, bias attributable to exclusion of those with no data at any of the relevant waves could not be addressed. Specifically, participants who were lost to follow-up had lower income and education levels. Evidence suggests income levels affect levels of environmental mastery and purpose in life (Kaplan et al., 2008; Navarro-Carrillo et al., 2020), therefore we were not able to determine if associations between shame and depression held for very low income men. Further, the current study underrepresented men born outside of Australia, and therefore underrepresented the potential heterogeneity in experiences of shame that may exist across groups of diverse backgrounds. Future research should replicate these findings in diverse samples which include low-income men.
The DASS-21 is a screening tool, not a diagnostic instrument. Future studies should examine whether these associations hold when depression is assessed with clinical diagnostic tools. Further, we acknowledge the conceptualisation of shame in the current study is one derived from research within Western, Educated, Industrialized, Rich and Democratic (WEIRD) backgrounds (Henrich et al., 2010) and therefore, may not reflect cultural variation in notions of shame. For example, there exists a specific cultural understanding of shame within Australian Aboriginal culture that may differ from how shame was presented in the current study (McKnight et al., 2018). Prior research suggests shame is a universal emotion, with potential differences in external and internal shame proneness existing across cultures, possibly explained by collectivistic and individualistic values (de Groot et al., 2021; Matos et al., 2023; Sznycer et al., 2012). Given the current study underrepresented men born outside of Australia, we could not explore the potential heterogeneity in experiences of shame that may exist across groups of diverse backgrounds.
Finally, we included several potential confounders but there is the potential for non-measured confounding factors to explain the association between shame and depression. For example, shame and depression are higher in people who have a history of trauma and abuse (DeCou et al., 2023; Ross et al., 2019) which we were not able to adjust for in this study.
Conclusions
Addressing an under-representation of adult men in longitudinal cohort studies, this study investigated the relationship between shame and depressive symptoms and the moderating role of psychological wellbeing. Over two thirds of men in this study reported experiencing shame. Of these men, over two thirds related their shame to work and over a quarter of fathers related their shame to their children. This may be reflective of their current life stage which involves transitioning between and navigating multiple role identities. Shame was found to predict later depressive symptoms, and psychological wellbeing appears to offer an important but limited protective role in this relationship. Overall, these novel findings contribute to the literature by demonstrating shame may be an antecedent factor in subsequent depressive symptoms in adult men. In the short-term, strength-based treatments may help to attenuate the association. Replication of these results is needed, particularly in diverse groups of men. Nevertheless, these findings highlight a clear contribution of shame to men’s future risk of depression.
Footnotes
Acknowledgements
The authors would like to thank the men who are participants in the Men and Parenting Pathways study for their time and invaluable contributions to each annual survey. We acknowledge the investigators and project managers who are not authors on this manuscript but have nevertheless made substantial contributions to the establishment and development of the cohort: Professors Jo Williams, Helen Skouteris, Tess Knight, Jeannette Milgrom, Associate Professor Richard Fletcher and Doctors Laura Di Manno, Bengianni Pizzirani and Briony Hill. We also thank the MAPP students and interns for their valuable contributions to the study.
Author contributions
GM contributed to the conceptualisation of the current study, conducted analyses, interpreted the results and led the write-up of the manuscript. LF and KM contributed to the collection of data, prepared data and advised on code for analysis and critically reviewed and revised the manuscript for important intellectual content. CG provided statistical oversight and critically reviewed the manuscript. CO critically reviewed and revised the manuscript for important intellectual content. JM conceptualized and designed the study, and led the collection of data, interpreted the results, supervised the write-up of the manuscript and critically reviewed and revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants to JM from the Australian Medical Research Future Fund [MRFF2026823] and to CAO from the National Health and Medical Research Council of Australia [GNT1175086, GNT1082406].
Data availability statement
The data analysed in this study are subject to the following licenses/restrictions: As per our data sharing policy, MAPP ethics approvals do not include participant consent for public availability of our data, however, requests for reuse of data for validation, verification or confirmation of past research are supported. Requests to access these datasets should be directed to the corresponding author.