
Abstract
Background:
Despite a significant clinical and social burden, there is a relative scarcity of epidemiological studies on Personality Disorder (PD).
Aim:
To determine the current prevalence of PD and the psychosocial correlates associated with this in the Andalusian population.
Method:
We carried out a cross-sectional population mental-health survey in Andalusia, southern Spain. Thus, 4,518 randomly selected participants were interviewed following sampling using different standard stratification levels. We used the Spanish version of the SAPAS to estimate PD prevalence. In addition, a full battery of other instruments was utilized to explore global functionality, childhood abuse, maltreatment, threatening life events, personality traits (neuroticism, impulsivity and paranoia), medical and psychiatric comorbidities, family history of psychological problems and other potential risk factors for PD.
Results:
PD prevalence (10.8%; 95% CI [9.8, 11.7]) and ran two different multivariate models for PD. We obtained the highest PD prevalence in those affected by any mental disorder plus those reporting having suffered childhood abuse, particularly sexual abuse. Additional potential risk factors or correlates of PD identified were: younger age, lower levels of functioning, less social support, poorer general health, having suffered maltreatment, threatening life events, higher suicidal risk scores and higher levels of both neuroticism and impulsivity.
Conclusions:
This study reports PD prevalence and risk correlates in consonance with similar findings reported in other Western populations. However, longitudinal studies are needed to elicit a more thorough group of prospective determinants of PD.
Introduction
Personality disorders (PDs) are persistent and frequently severe mental conditions that affect an individual’s inner experience and social interactions. PD associates with behaviours that lie outside the individual’s cultural expectations and that cannot be directly attributed to either somatic illness or another psychiatric mental disorder. PD also affects the way an individual relates with himself and with other people and is usually accompanied by difficulties in social adaptation. PD tends to appear in childhood or adolescence and persists into adulthood (American Psychiatric Association, 2013; World Health Organization, 2000). Although PDs constitute a serious public health problem and present a high comorbidity with other mental disorders (Tyrer et al., 2015), there is limited epidemiological data. Furthermore, no previous epidemiological studies have been published on prevalence and correlated factors in Andalusia, the largest region in Spain.
Up to date, previous prevalence reports show a considerable degree of heterogeneity due to the use of different assessment methods and samples. Thus, reported prevalence ranges from 2% to 20% approximately (Winsper et al., 2019) with higher figures among surveys taking place in higher-income countries (Lenzenweger et al., 2007; Pedersen & Simonsen, 2014; Torgersen et al., 2001; Trull et al., 2010; Volkert et al., 2018) than among reports on low and middle income countries (Huang et al., 2009; Santana et al., 2018). Indeed, the World Mental Health Survey (Huang et al., 2009), including 13 developed and developing countries and a total very large sample of 21,162 participants, reported a point prevalence of 6,1%, lower than those reported by two recent systematic reviews (Volkert et al., 2018; Winsper et al., 2019), that is, 7.8% and 12.16%, respectively. The latter focussed on western countries (U.S.A., Sweden, Germany, Turkey, Australia, UK and The Netherlands). Additionally, two other studies from Norway (Torgersen et al., 2001) and Denmark (Pedersen & Simonsen, 2014) found higher PD prevalences of 13.4% and 14.9%, respectively.
Regarding risk factors for PD, exposure to traumatic or adverse events, such as childhood abuse (Dereboy et al., 2014) or maltreatment, has been found to associate with PD in a variety studies (Afifi et al., 2011; Baryshnikov et al., 2017; d’Huart et al., 2022; Reising et al., 2019; Solmi et al., 2021; Tyrer et al., 2015). Among them, one review highlights the role of childhood adversity reported to increase PD risk by fivefold (Solmi et al., 2021). In addition, older age, higher educational levels and being employed inversely association in most studies (Coid et al., 2006; Volkert et al., 2018; Yang et al., 2010). Being male appears to be also a risk factor (Coid et al., 2006; Samuels et al., 2002). Other risk factors, such as marital status or urban dwelling seem to have an unresolved association with PD (Coid et al., 2006; Ekselius et al., 2001).
PDs also tend to have a high comorbidity among them and with other psychiatric disorders (Coid et al., 2006), particularly anxiety disorders, affective disorders and, to a lesser extent, substance abuse disorders. PD often worsens the prognosis and treatment outcomes of comorbid mental disorders (Tyrer et al., 2015). Besides, people with PD have higher mortality, which can be explained partly by an increased incidence of suicide (Tyrer et al., 2015). Thus, scientific literature shows that impulsivity might mediate the association between PD and suicidal behaviour (McHugh & Balaratnasingam, 2018). Moreover, both impulsivity and neuroticism are personality traits that seem to have an essential role in the development of PD (Baryshnikov et al., 2017, McHugh & Balaratnasingam, 2018). Regarding comorbidity between PD and physical conditions, several studies have found an association between PD and cardiovascular disease (Dixon-Gordon et al., 2018; Moran et al., 2007; Quirk et al., 2015), arthritis and gastrointestinal illness (Quirk et al., 2015), sleep problems, obesity and chronic pain (Quirk et al., 2015). A recent review (Dixon-Gordon et al., 2018) compiles the latest findings in the relationship between PD and the most relevant associated medical conditions and the possible mechanisms underlying this relationship, stressing the importance of taking into account the diagnosis of PD due to its significant contribution to health burden.
Methods
Design and framework
Our main objective was to establish the prevalence of PD and to identify its associated factors among the Andalusian population. For this purpose, we designed a cross-sectional study that included a representative sample of adults aged between 18 and 75 years living in the region of Andalusia (Spain). All interviews were thoroughly trained by our team although they were employees of a local survey company specialized in conducting extensive epidemiological health surveys. Data collection lasted over a year and was performed in 2013 and 2014. The current PISMA-ep PD study is part of a larger and broader study on most mental disorders and their risk correlates, that is, the PSIMA-ep Study (Cervilla et al., 2016).
The sample
We approached a broad stratified and representative sample of the adult population (18–75 years old) living in the Andalusian community. A company specialized in health surveys carried out the data collection in the homes of the participants and accomplished the sampling using different successive stratification levels: (a) proportional stratification between two geographical areas, east and west of Andalusia; (b) stratification by population density of the cities in each of the two geographical areas; (c) stratification based on the population of each of the eight Andalusian provinces and (d) within each province, we used simple randomization to select between one and five municipalities of each type of location (urban, intermediate and rural). Finally, the final sampling areas were selected using a simple random assignment method and taking into account the age and sex quotas, the census tracts and the districts of each locality. Therefore, the final sampling units were persons of both sexes, ages 18 to 75 years, interviewed after choosing one in four consecutive households within the predetermined street routes of the pre-identified tracts and census tracts selected at random. We calculated a sample size from an estimate of 2% for mental disorder prevalence with an accuracy of ±0.5%, with 95% confidence intervals and for an estimated effect size of 1.5. To ensure inter-rater reliability, all interviewers attended a two-week training course imparted by the principal investigator (JC). They demonstrated sufficient knowledge of interview techniques, protocol scales and inventories. The interviewers carried out a pilot phase to study the suitability and intelligibility of the wordiness of all the questions.
Regarding substitution and response rate, 70.8% of the addresses initially selected did not respond after four attempts or did not have participants within the sex and age range of the study. Therefore, they had to be replaced by addresses from the next available household within the default path. Finally, 4,507 participants out of 5,496 households approached completed the interview (response rate 83.7%). After the interviews, we implemented a double-check procedure to ensure data quality. The error rate accepted was up to 1%. A complete report on the methods of the PISMA-ep study have been published elsewhere (Cervilla et al., 2016).
Assessment of PD and associated factors
PD diagnosis
We ascertained PD diagnosis utilizing the Standardized Assessment of Personality-Abbreviated Scale (Moran et al., 2003). The SAPAS comprises of eight elements providing a dimensional score from 0 to 8 points representing the participant’s probability of having a PD. We used the Spanish version of SAPAS for psychiatric patients in which a score of 4 or above is highly sensitive (0.89) and specific (0.58) to detect cases of PD with high probability (Muñoz-Negro et al., 2020). These psychometric properties are very similar to the English version (Moran et al., 2003). In non-clinical populations, SAPAS is less accurate. Thus, a cut-off point of 4 or more correctly classified 58% of participants, sensitivity 0.69% and specificity 0.53%, (Fok et al., 2015). Nevertheless, another study found an increased SAPAS sensitivity (78%) using the IPDE scale as a gold standard (Ball et al., 2017).
Assessment of social factors
We collected data on sociodemographic factors such as age, sex, civil status, unemployment rate, rurality (urban >10,000 inhabitants, intermediate 2,001–10,000 and rurality <2,001) and educational level. We used these sociodemographic factors to estimate the participants’ IQ using a Spanish version (Seisdedos & Bilbao Bilbao, 2004) of the Barona Index (Barona et al., 1984). Family psychiatric history was established using the Spanish version of the Family Interviews for Genetic Studies (NIMH Repository and Genomics Resource). Childhood maltreatment experiences was assessed on three types of abuse suffered during childhood: psychological, physical mistreatment and sexual abuse utilizing an abbreviated version of the Childhood Trauma Questionnaire (Fink et al., 1995). Each item in the questionnaire ranged from 1 to 5, depending on the degree to which participants agreed with every statement. We then calculated a summary variable of childhood abuse after adding the scores on the three types of maltreatment. As for exposure to threatening life events, we utilized a validated reference list of 12 categories of life events having occurred in the previous 6 months (Brugha et al., 1985). Social support was assessed using a self-report inventory of participant’s thoughts about their relationship with the family and friends, relationship with spouse or partner and ability to maintain relationships in general (Blaxter, 1990).
Assessment of psychological factors
Screening for common mental disorders other than PD was performed using the Mini-International Neuropsychiatric Interview (MINI; Sheehan et al., 1998). This is a relatively brief diagnostic structured psychiatric interview eliciting diagnoses compatible with DSM-IV and CIE-10 criteria. The MINI has demonstrated a high inter-evaluator reliability, a correct sensitivity and a low rate of false positives in the community. Personality traits such as neuroticism and impulsiveness were explored with the corresponding sections of the Zuckerman–Kuhlman Personality Questionnaire (Boyle et al., 2008). Finally, we also measured the level of paranoia by administering the Spanish version (Ibáñez-Casas et al., 2015) of the Green Paranoid Thought Scales (GPTS; Green et al., 2008).
General health and global functioning
General health during the last 4 weeks was assessed using the SF-12 questionnaire (Jenkinson et al., 1997), a 12-item reduced version of the SF-36 health survey questionnaire. The SF12 provides two summary scores (physical and mental health components). The score ranges from 0 to 100, where the higher the score the better health-related quality of life. The Fagerström Test for Nicotine Dependence was used to measure exposure to tobacco smoking. This is a standard tool for assessing the intensity of physical addiction to nicotine (Heatherton et al., 1991). A total score was obtained by adding all individual items scorings allowing identification of participants with high nicotine dependency (from 6 to 10 points). Similarly, alcohol consumption was assessed using the Cage questionnaire for alcoholism. The CAGE questionnaire (Ewing, 1984). The CAGE is considered a screening instrument for alcohol abuse in which scores of 2 or more points out of a maximum of 4 suggest abusive consumption. The CAGE has been reported to have a specificity of 76% and sensitivity of 93% for identifying excessive consumption and a specificity of 77% and sensitivity of 91% for identifying alcoholism (Bernadt et al., 1982). Finally, we also measured global overall functioning with the Global Assessment of Functioning (American Psychiatric Association, 1994) and the Objective Social Outcomes Index (SIX; Priebe et al., 2008). The Global Assessment of Functioning (GAF) comprises a single score obtained after classifying the participant between 0 (worse functioning possible) to 100 (good activity). The SIX assesses social functioning and comprises four elements: employment, accommodation, partner/family and friends. Its administration provides a total score up to a maximum of 6 points in which a higher score means better social functioning.
Statistical analysis
Firstly, we conducted a descriptive analysis of the sample and calculated the PD prevalence of using SAPAS score ⩾4. Secondly, we used the chi-square and Student’s T tests test to explore univariate associations with PD. We explored the following variables: sex, civil status, rurality, unemployment, family history of mental disorder, physical abuse, psychological abuse, sexual abuse, any kind of abuse, educational level, adverse life events, obesity, physical exercise, substances abuse and dependency and current psychotic, anxiety or mood disorder, functionality, tobacco consumption, general health, paranoia and social support, suicidal risk, neuroticism and impulsivity. Once we established univariately associated factors, we calculated the different prevalences for each risk group. Finally, we ran a logistic regression multivariate model (method enter) to calculate the probability of having a PD and another linear regression model (method enter) using the SAPAS score as a dimensional approximation to PD diagnosis. The latter included a diagnosis of collinearity. We consider a statistical significance of p ⩽ .05 for all two-tailed hypothesis tests. We utilized the SPSS programme version 28.0.1.0 for our statistical analysis.
Results
Description of the sample, PD prevalences and potential risk group
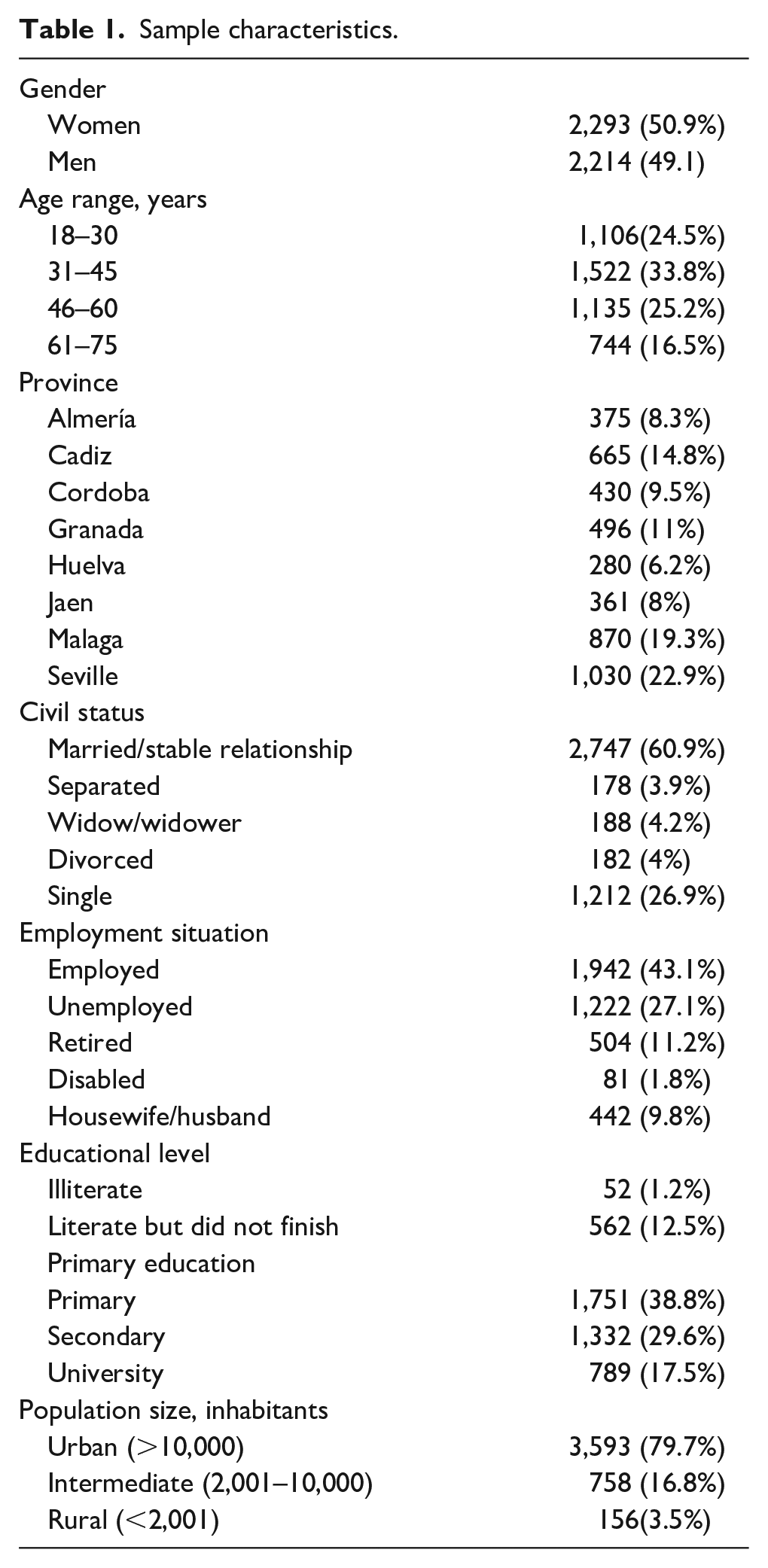
Table 1 describes the main sociodemographic variables. The current PD prevalence in our sample was 10.8% (95% CI [9.8, 11.7]). A higher current PD prevalence was observed in the following groups: rural living (14.1%) versus urban (10.3%), χ2 = 5.067, p ⩽ .079; having a positive family psychiatric history (17.2%) versus not (9.5%), χ2 = 37.892, p ⩽ .000; having suffered threatening life events (13.9%) versus not (7.3%), χ2 = 49.265, p ⩽ .000; having suffered physical maltreatment (24.2%) versus not (10%), χ2 = 51.6, p ⩽ .000; having suffered psychological maltreatment (27.6%) versus not (9.4%), χ2 = 111.168, p ⩽ .000; having suffered sexual abuse (31.3%) versus not (10.6%), χ2 = 21.041, p ⩽ .000; being single or alone (12%) versus being married or in a relationship (10%), χ2 = 4.607, p ⩽ .032; primary studies group (12.1%) versus people with university degree or PhD (8.8%), χ2 = 9.13, p ⩽ .01; people affected by a current or lifetime abuse to one substance (16.5%) or more than one (32.7%) compared to those without substance abuse (10.1%), χ2 = 38.097, p ⩽ .000; people with dependence to more than one substance (44.4%) or one substance (25.1%) compared to those without substance dependence (10%), χ2 = 72.774, p ⩽ .000; Finally, people suffering any current disorder (18.9%) versus those who do not (10.1%), χ2 = 63.702, p ⩽ .00; people diagnosed of particular psychiatric conditions: psychotic disorder (52.1%) versus not (9.9%), χ2 = 173.411, p ⩽ .000; anxiety disorder (38.1%) versus not (9%), χ2 = 231.284, p ⩽ .000; mood disorder (39.6%) versus not (8.3%), χ2 = 332.682, p ⩽ .000.
Sample characteristics.
Univariately having a PD was associated with the following potential risk factors: poorer social functionality (t = 5.679, p ⩽ .000), lower levels of GAF (t = 10.531, p ⩽ .000); lower estimated Intelligence Quoficient score (t = 3.743, p ⩽ .000); higher alcohol consumption (t = -3.847, p ⩽ .000); higher tobacco consumption (t = -5.089, p ⩽ .000); higher suicidal risk score (t = -3.399, p ⩽ .001); lower social support (t = 7.511, p ⩽ .000); worse general health (t = -8.054, p ⩽ .000); higher neuroticism levels (t = -19.260, p ⩽ .000); higher impulsivity scores (t = -12.355, p ⩽ .000) and increased paranoia scores (t = -10.372, p ⩽ .000).
Multivariate model for the categorical definition of PD
We obtained a multivariate model with a parsimonious group of factors associated with PD (Cox and Snell R2 = .128; Nagelkerke R2 = .259). This model correctly predicted 89.9% of the cases, detecting 98.8% of the patients with PD. The variables included in the final model were younger age, global functioning (GAF), higher suicidal risk scores, having less social support, poorer general health, having suffered childhood maltreatment, having had at least one threatening life event over the previous 6-month period, increased neuroticism scores and higher impulsivity scores (see Table 2 and Figure 1).
Categorical model for PD.
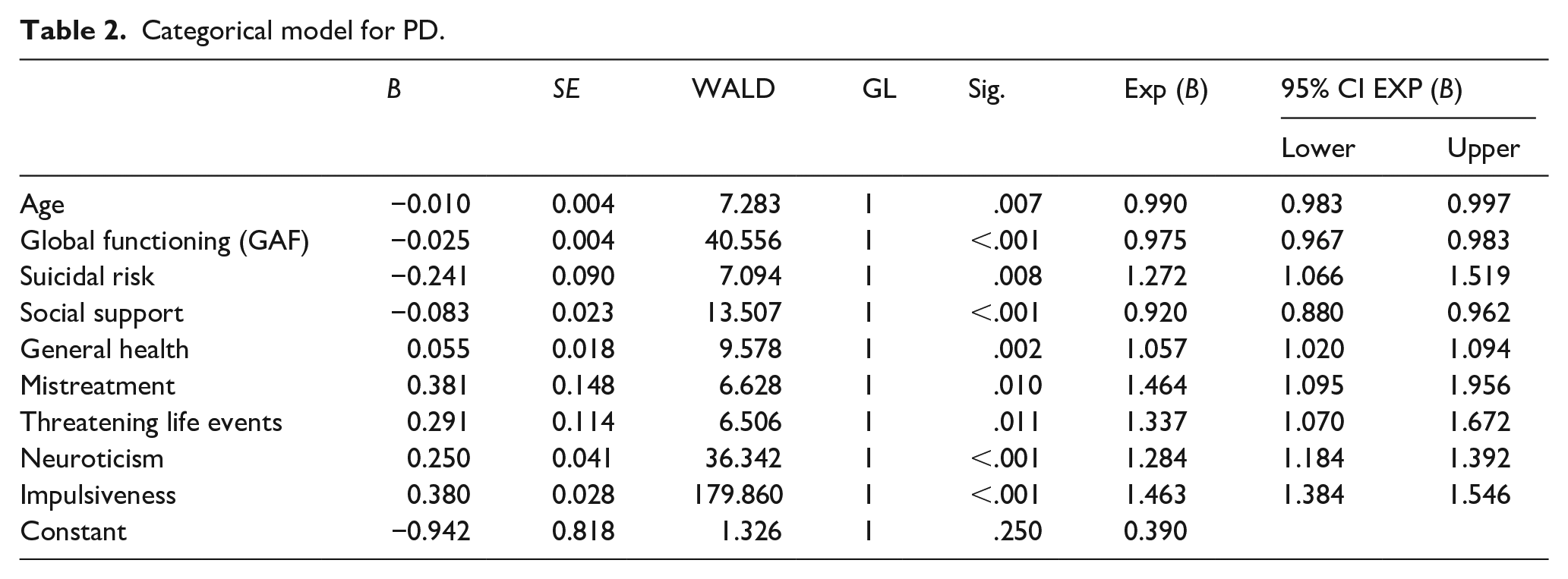
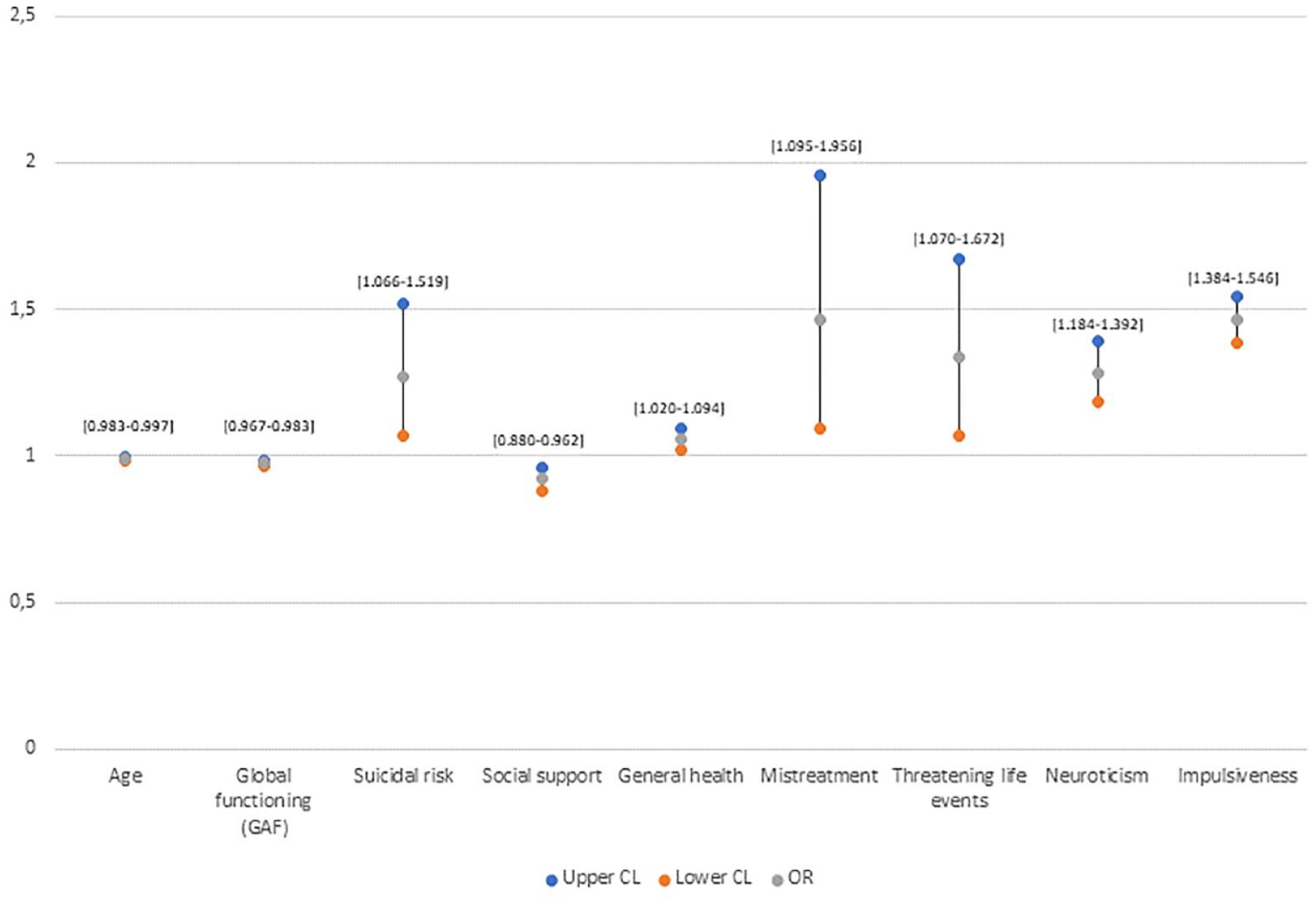
Factors associated with PD.
Multivariate model for the dimensional definition of PD
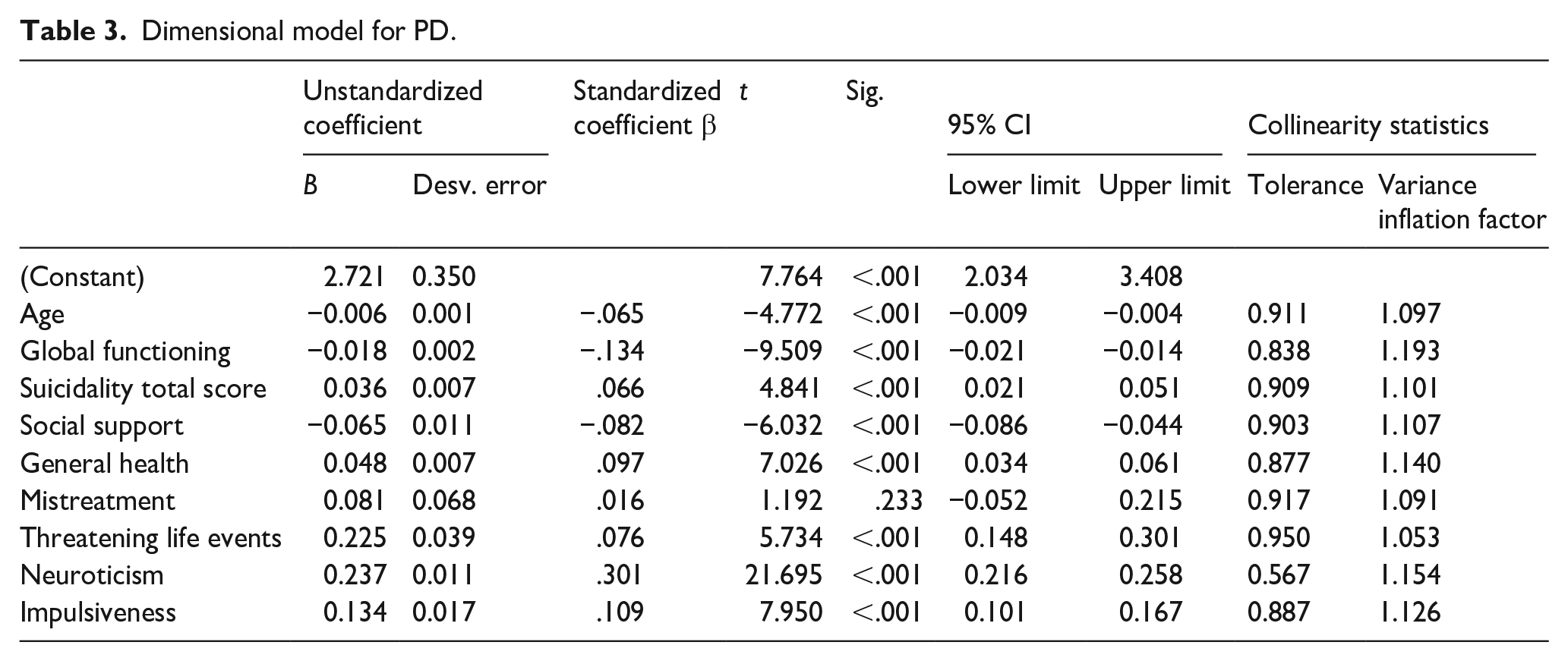
A linear regression model using increasing SAPAS scores as main outcome variable confirmed the following variables: age, global functioning (GAF), suicidal risk, social support, general health, threatening life events, neuroticism and impulsiveness. Childhood maltreatment did not associate independently to increasing SAPAS scores (see Table 3).
Dimensional model for PD.
Discussion
There are hardly any studies on the prevalence and risk factors of PD in the general population in Spain. Spain contributed to the ESEMeD epidemiological study but to the best of our knowledge, data on PD have not been published on a country basis. An earlier previous study (N = 1,185) using DSM-III criteria was carried out in Zaragoza (Seva et al., 1991), reporting an unusually low prevalence of PD (1%). Our study adds, nonetheless, novel information on PD prevalences, factors and comorbidities. And it is, so far, the largest study on the prevalence and risk factors for PD conducted in Spain. We must remark that the prevalence found in our study was within the average of the rest of the studies developed in the general population of other European countries. Notably, the highest prevalences of PD were found among those individuals who also met criteria for other psychiatric disorders, such as psychosis, substance dependence, mood disorders or anxiety disorder. We identified as potential risk factors for PD having suffered childhood abuse, especially sexual abuse, younger age, poorer functioning, poorer social support, poorer general health, social adversity (maltreatment, poor social support and facing threatening life events), higher levels of suicidal risk and higher scores on two personality traits (neuroticism and impulsivity).
When we compare our data with those of other studies, we observe that our point prevalence (10.8%) is quite similar to 12.16% found by the rest of the studies carried out in the Western world (Volkert et al., 2018), 9.6% in high-income countries (Winsper et al., 2019) or 9.1% in USA (Trull et al., 2010) and higher than 4.3% in low-and middle-income countries (Winsper et al., 2019) or 6.8% in big cities as Sao Paulo (Santana et al., 2018), and much higher than the prevalence found in the study carried out in Zaragoza in 1991 (Seva et al., 1991). Our study was conducted in Andalusia, a region in southern Spain with a population of 7,758,809 million inhabitants and generally with worse socioeconomic indicators than the mean Spanish region and a much higher unemployment rate (18.05%) than the Spanish average (INE, 2023). All these factors could cause the prevalence found to be higher than what could be expected for the rest of Spain. However, we took into account several socioeconomic factors such as educational level, unemployment or rurality, without finding any statistically significant association with PD. It is noteworthy that both our study and many of the previous ones have used ICD-10 diagnostic criteria. Currently, the ICD-11 has abandoned the categorical classification, changing to a strictly dimensional system structured in two successive steps. The first one distinguishes between different grades of severity: no personality dysfunction, personality difficulty (Z code) or mild, moderate or severe personality disorder. The second step describes the nature of PD within its previously assigned severity, using five personality-trait dominions linked to the ‘big-five’ general personality model: negative affectivity, anankastia, detachment, dissociality and disinhibition. This new classification not only has more empirical basis, but also offers advantages to clinicians and researchers, and is also the result of a pragmatic solution between clinicians and researchers, especially those interested in somehow maintaining the validity of borderline disorder as a descriptor once the severity levels have been determined (Tyrer et al., 2019). In addition, as a consequence of these diagnostic changes, the prevalence of personality disorders could increase by 2%, as some studies indicate (Tyrer et al., 2014).
Concerning associated factors, the multivariate model confirmed risk factors for PD that had also been found in other studies, as well as comorbidity with other mental disorders such as mood, anxiety and substance use disorders (Coid et al., 2006; Trull et al., 2010), with medical conditions (Dixon-Gordon et al., 2015, 2018; Moran et al., 2007; Quirk et al., 2015). Thus PD has previously shown to associate with exposure to child maltreatment (Afifi et al., 2011; Baryshnikov et al., 2017; d’Huart et al., 2022; Reising et al., 2019; Solmi et al., 2021), younger age (Yang et al., 2010), poorer functioning (Trull et al., 2010), higher suicidal risk (Trull et al., 2010; Tyrer et al., 2015), lower social support (Trull et al., 2010), impulsivity (McHugh & Balaratnasingam, 2018) and neuroticism (Baryshnikov et al., 2017; McHugh & Balaratnasingam, 2018). It is notorious that when we retested the results of the multivariable risk model using a continuous measure of PD rather than the dichotomous one, childhood maltreatment did not associate significantly with increasing SAPAS scores. But the categorical model did so. It is plausible that childhood maltreatment, once occurred, influences only full-blown PD rather than minor personality abnormalities. Overall, our study did not confirm previously suggested risk factors such as gender, educational level, marital status, unemployment or urbanicity. The high comorbidity with other mental disorders could be due to risk factors shared with other mental disorders and underlying psychopathological dimensions shared with other mental disorders, such as an earlier-described general p factor (Caspi et al., 2014). The different PDs share a general factor that cuts across all (Sharp et al., 2015). Despite many associated factors, much of the total variability could not be explained. This may be due to factors such as the absence of genetic or biological data, or not having measured potential psychosocial and cultural determinants, such as fractures in social cohesion, social capital or the greater or lesser degree of individualism/collectivism in society (Winsper et al., 2019). Not surprisingly, the relationship between mental disorders and social factors, such as bad character formation and bad education, has been suggested since the time of Plato (Ahonen, 2019).
Our study’s main limitations include its cross-sectional nature, the limitations of the SAPAS in the general population and also the fact that the latter is merely a brief self-reported screening instrument indicating probable PD rather than properly diagnosing it. Further, the lack of genetic or biological data might have limited the comprehensiveness and generalizability of the reported explanatory models. Nonetheless, we must say that although cross-sectional studies do not allow us to verify causal hypotheses, they might enable us to propose new research hypotheses. In this case, we must highlight that most of the variability of the sample was not accounted for by the model. It will probably be necessary to include new sociological, cultural, environmental or genetic variables to increase the level of explanatory accuracy for PD. Concerning the limitation of the SAPAS, we must emphasize that it is valid as a screening measure suggesting probable PD, and that it cannot replace a global clinical assessment of personality carried out by a clinical interviewer, this kind of limitation could be a source of bias and misclassification that should be emphasized. Moreover, it has been observed that self-applied measurement instruments tend to overestimate the prevalence (Volkert et al., 2018), however, our data were quite similar to those found in other studies. Despite all these limitations, the SAPAS has shown to perform adequately in the general population (Ball et al., 2017; Fok et al., 2015). In addition to being an easy-to-use instrument with a short application time, which makes it useful in population studies. Since 2018, a new self-administered version of the SAPAS, the SAPAS-PD (Olajide et al., 2018), has been available. This not only screens PD using ICD-11 criteria but also incorporates the ability to distinguish between mild and moderate cases of PD. It is an important advantage as the impact of personality traits on functioning and harm to self and others is a core diagnostic criterion for PD in ICD-11. For this reason, although it was not available at the time of the interviews, it would be important to validate it in Spanish in order to use it in future studies.
Finally, the first large epidemiological study of PD carried out exclusively in Spain confirms a prevalence and possible risk factors similar to those found in other Western countries. However, many unexplained factors in the development of PD still remain and it is necessary to design and develop prospective longitudinal studies including new biological, psychosocial and cultural exposures.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially financed with a subsidy from the Department of Economy, Innovation and Science of the Regional Government of Andalusia (10-CTS-6682).