
Abstract
Healthcare workers around the world were confronted with innumerable torments with the emergence of COVID-19. Amid the pandemic, frontline healthcare personnel serve crucial responsibilities and endure significant social, psychological and economic consequences. This cross-sectional study collected demographic data for 1 year from 385 healthcare officials from all the hospitals spread across the state of Khartoum to research the factors that affected the healthcare workers and doctors who were on the frontline to diagnose and treat the patients with potential or confirmed COVID-19. The degree of symptoms of depression, anxiety and insomnia was also assessed through validated measurement tools. The female participants showed more vulnerability to depression, anxiety and insomnia than their male counterparts. It was reported by the end of the study that the healthcare workers in Sudan are under immense psychological hazards.
Introduction
The current pneumonia epidemic, which began in early December 2019 near Wuhan City, Hubei Province, China, has been designated a Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or COVID-19 by the World Health Organization (WHO). At the time, there were 118,000 confirmed coronavirus infections in 110 countries. China was the first country to experience the devastating consequences of the widespread pandemic. Gradually the virus wreathed South Korea, Iran and Italy in February. Within no time, the virus diffused across all the continents reaching up to 177 states, the USA having the greatest number of verified cases and unfortunately the highest fatality rate (Kantamneni, 2020). The virus was highly infectious, and fatalities were reported among the patients who had weak immune systems and were most vulnerable to the disease, those over 60 and those with pre-existing medical issues. The most serious cases boosted the number of people admitted to hospitals for acute care, prompting concerns that the virus might spread across local healthcare systems.
COVID-19 is a virus that has the potential to kill. Bats appear to represent the COVID-19 viral reservoir, according to phylogenetic analysis of available whole-genome sequences, but the intermediate host has yet to be discovered (El-Sayed & Kamel, 2021). Despite the fact, three important areas of research to increase knowledge of the outbreak’s viral pathogenesis are currently ongoing in China. Early investigations into cases with symptoms in Wuhan in December 2019, ecological sampling from the Huanan Wholesale Seafood Market and other area markets, and the collection of detailed reports on the origin and type of wildlife species marketed on the Huanan market, as well as their destination after the market has closed, are all underway (Mizumoto et al., 2020).
The virus family
The virus is naturally divided into four categories that cause gastrointestinal and respiratory infections. The first two types Gammacoronavirus and Deltacoronavirus affect the birds whereas Betacoronavirus and Alphacoronavirus primarily affect mammals (Hepojoki et al., 2017; Seah & Agrawal, 2020). Human CoVs have been classified into six categories (Forni et al., 2017). HCoVHKU1, HCoV-OC43, Middle East Respiratory Syndrome Coronavirus (MERS-CoV) and Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) are members of the Betacoronavirus family while HCoV-NL63 and HCoV229E are the types of Alphacoronaviruses. Coronaviruses were not widely recognised until the 2003 SARS pandemic, which was followed by the MERS outbreaks in 2012 and, most recently, the COVID-19 outbreaks (Hilgenfeld & Peiris, 2013). The viruses of the 2003 pandemic and 2010 outbreak were deadly contagious that were transmitted from bats to humans via palm civets and dromedary camels.
The healthcare system of Sudan
To limit the danger of transmission of the deadly virus among the population, personal protective equipment (PPE), strict lockdowns, social-distancing and self-quarantine practices were implemented by the Sudanese authorities (Altayb et al., 2020). These initiatives, however, ran through several roadblocks and ultimately failed. The Sudanese healthcare system comprises of both public and private institutions. Sadly, many of such a huge system had to close down their doors owing to fear of COVID-19 spreading (Kheder et al., 2020). This worsened the conditions in the country, frustrating the citizens and they were pushed to their limits which were obvious in their dissatisfaction. They started verbally criticising and threatening to physically assault physicians and other healthcare personnel.
The challenges of the health care system
Sudan’s health system was barely keeping up with the number of patients who came to hospitals on daily basis due to the exceptional conditions. The disastrous consequences resulted in a complete reverse flow within the health care centres and hospitals with overcrowding rooms, which contributed to the spread of hospital-acquired infections among uninfected hospital employees and patients. The staff’s reaction to the pandemic was also cited as a factor in the lack of compliance with infection control protocols. A significant number of doctors misused their personal protection equipment (PPE). Furthermore, some workers fail to select owing to a lack of competence or equipment.
Another issue that these front-line workers encounter is the lack of proper lodging and transportation to and from hospitals. Taking public transportation poses a significant risk to others and actively distributes the virus (Shang et al., 2020). Some physicians return home to their homes, where they spread the sickness to their relatives. The medical practitioners had to deal with irate patients and their families regularly as a part of their job, counselling them about their COVID-19 diagnosis or conveying the news about the death of their loved ones was not an easy task, and this often infuriated the patients. Some family members questioned the diagnosis and accused doctors of falsifying the results. They utilised physical and verbal hostility against doctors, destroyed wards and apparatus, and forcibly entered doctors’ rooms during frantic assaults.
The COVID-19 pandemic has been and continues to be overwhelming even after more than 24 months of its birth. The fast-spreading virus and seriousness of the disease have caused a tremendous amount of stress, especially to health care workers (HCWs) who due to their direct and indirect contact in the diagnosis, treatment and follow-up with COVID-19 patients and suspected patients have more chances of contracting the disease. These HCWs are at a greater risk of experiencing psychological anguish as well as other mental health issues (Chen et al., 2020; World Health Organization, 2020)
The HCWs’ mental strain is not an outcome of a single element; the excessive workload, lack of sufficient PPE and specialised treatment drugs, and feelings of being under-supported are a few to name contributors. According to the study, HCWs exhibited serious psychological reactions to the 2003 SARS outbreak (Stuijfzand et al., 2020; Tan et al., 2020), which observed that HCWs feared becoming infected and spreading the infection to their families, friends and co-workers (Huang & Zhao, 2021). Many felt discouraged to go to work and wanted to quit (Preti et al., 2020) in addition to the high levels of depression and anxiety (Cai et al., 2020). Similar concerns about the mental health of HCWs working in the frontline are now arising. The COVID-19 pandemic has the potential to have a significant impact on the mental health of healthcare workers who are on the front lines of this disaster.
Materials and methods
This was cross-sectional study conducted in all hospitals and centres treating COVID-19 suspected patients in Khartoum State Sudan, over a period of 1 year (September 2020–September 2021). The questionnaire composed of four parts. The first section consisted of demographic information and job duties, such as age; sex, age, marital status, occupation, place of employment, contact with COVID-19 suspects, PPE providing and living quarter provisions. A patient health questionnaire (PHQ-9) was used to access the depression (Killgore et al., 2020), anxiety was evaluated using the Generalised Anxiety Disorder 7-item (GAD-7) scale (Lechner et al., 2020), and insomnia was assessed using the validated version of the Insomnia Severity Index (Thakral et al., 2020), both of which are validated measuring techniques.
Study variables and measurements
For the treatment of depression, minimal depression is a score of 1 to 4, mild depression is a score of 5 to 9, moderate depression is a score of 10 to 14, moderately severe depression is a score of 15 to 19 and severe depression is a score of 20 to 27. For Anxiety (GAD), sum scores of 5, 10 and 15 are taken as the cut-off points for mild, moderate and severe anxiety, respectively. For insomnia, the total score categories for all seven items (questions 1–7) are: 0 to 7 indicates no clinically significant insomnia, 8 to 14 indicates sub-threshold insomnia, 15 to 21 indicates clinical insomnia (moderate severity) and 22 to 28 indicates clinical insomnia (severe).
The researcher used the Statistical Package for Social Sciences (SPSS) version 25.0, SPSS Inc. Chicago, IL, for data input and statistical analysis. The chi-squared test was performed to compare proportions in two groups after the frequency distributions for the independent and dependent variables were constructed. A p-value of less than .05 was judged statistically significant.
Results
Demographic data and working conditions
The study included 385 participants, 58.4% were females, most were 29 years and younger (62.9%), 78.2% single and 60.8% junior doctors (Medical Officer/House Officer) (Table 1).
Demographic data and working condition during COVID-19.
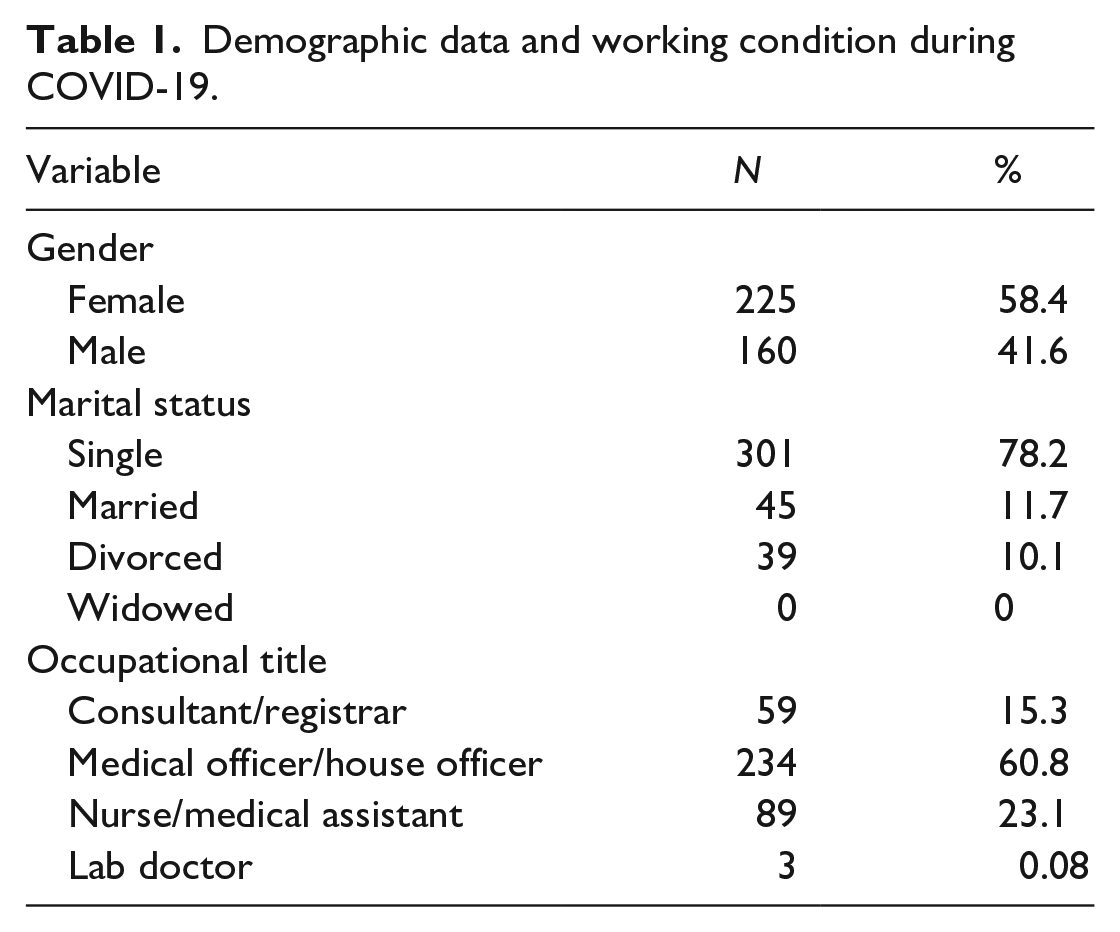
Approximately half of the participants worked in general hospitals (56.5%), and most had direct contact with COVID-19 patients and suspected patients (73.8%) (Table 2).
Work data of the participants.
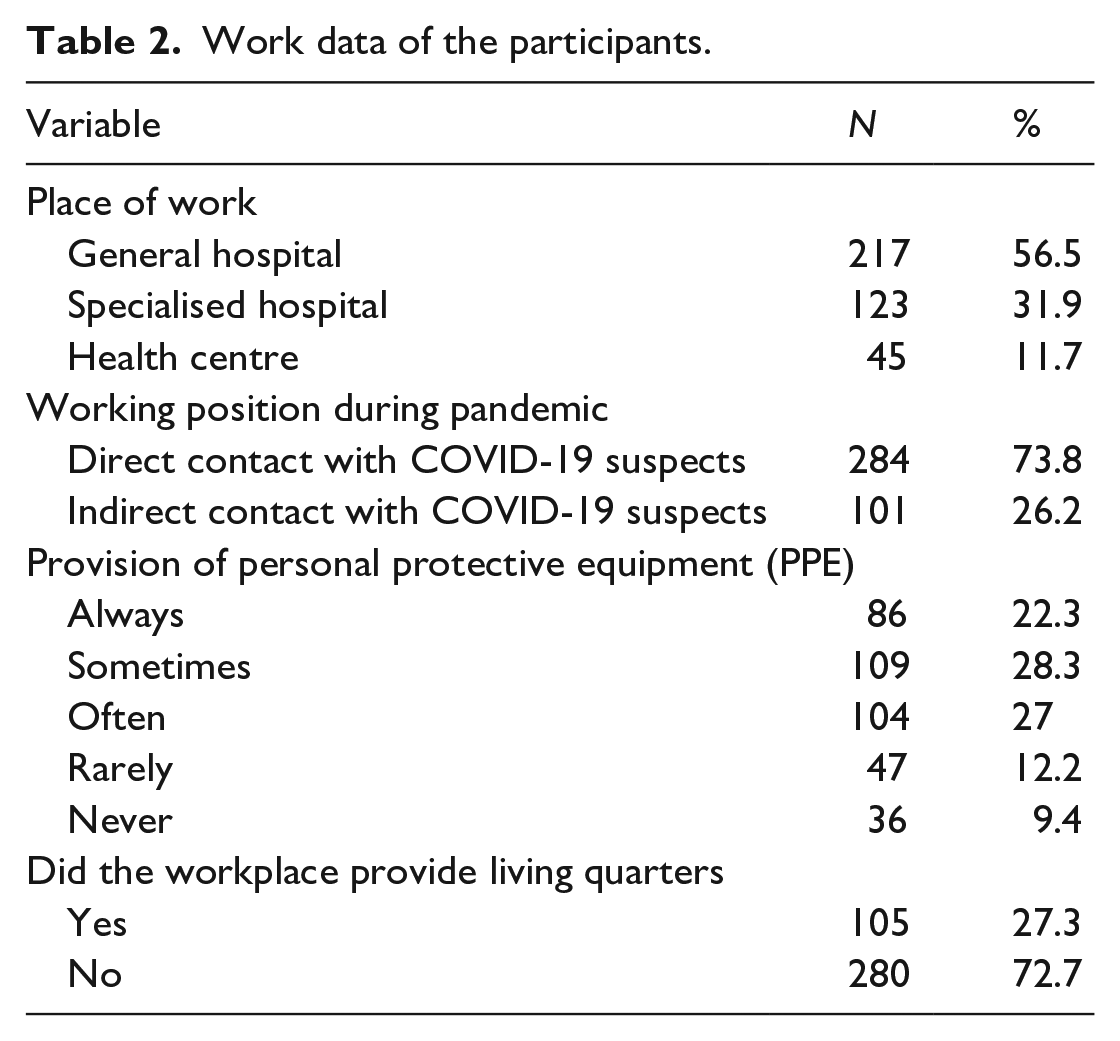
When asked about the provision of PPE, 28.3% of participants answered sometimes they were provided by PPE, followed by 27.0% often 22.3% always, 12.2% rarely and 9.4% answered never. Living quarters were provided for 27.3% (Table 2).
Most participants were very dissatisfied with the salary given to them (37.3%), and only 0.8% was very satisfied with the salary (Figure 1). 35.1% participants were dissatisfied with working conditions, none were very satisfied with the working conditions and only 13.5% were satisfied (Figure 2).
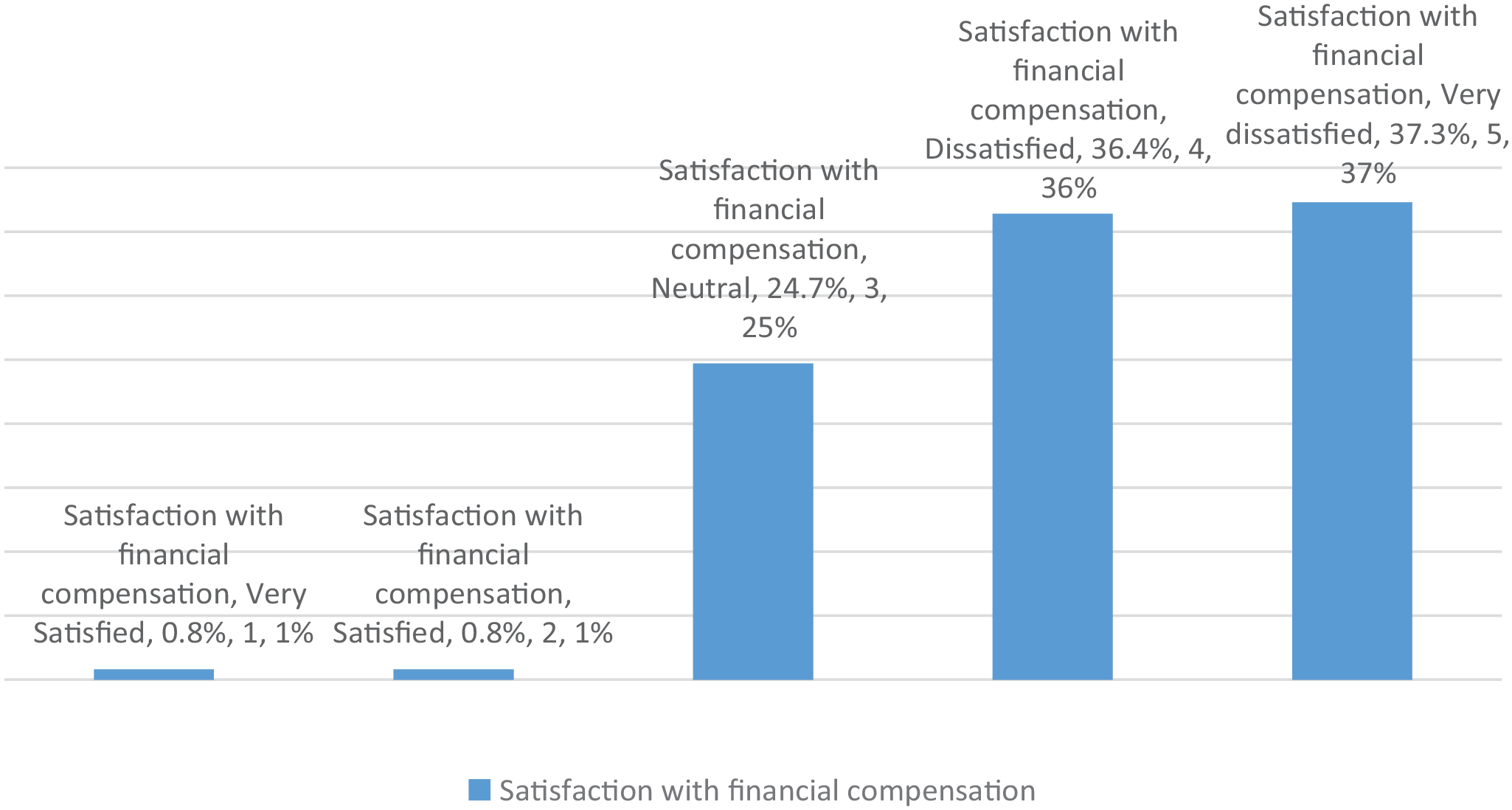
Satisfaction with financial compensation.
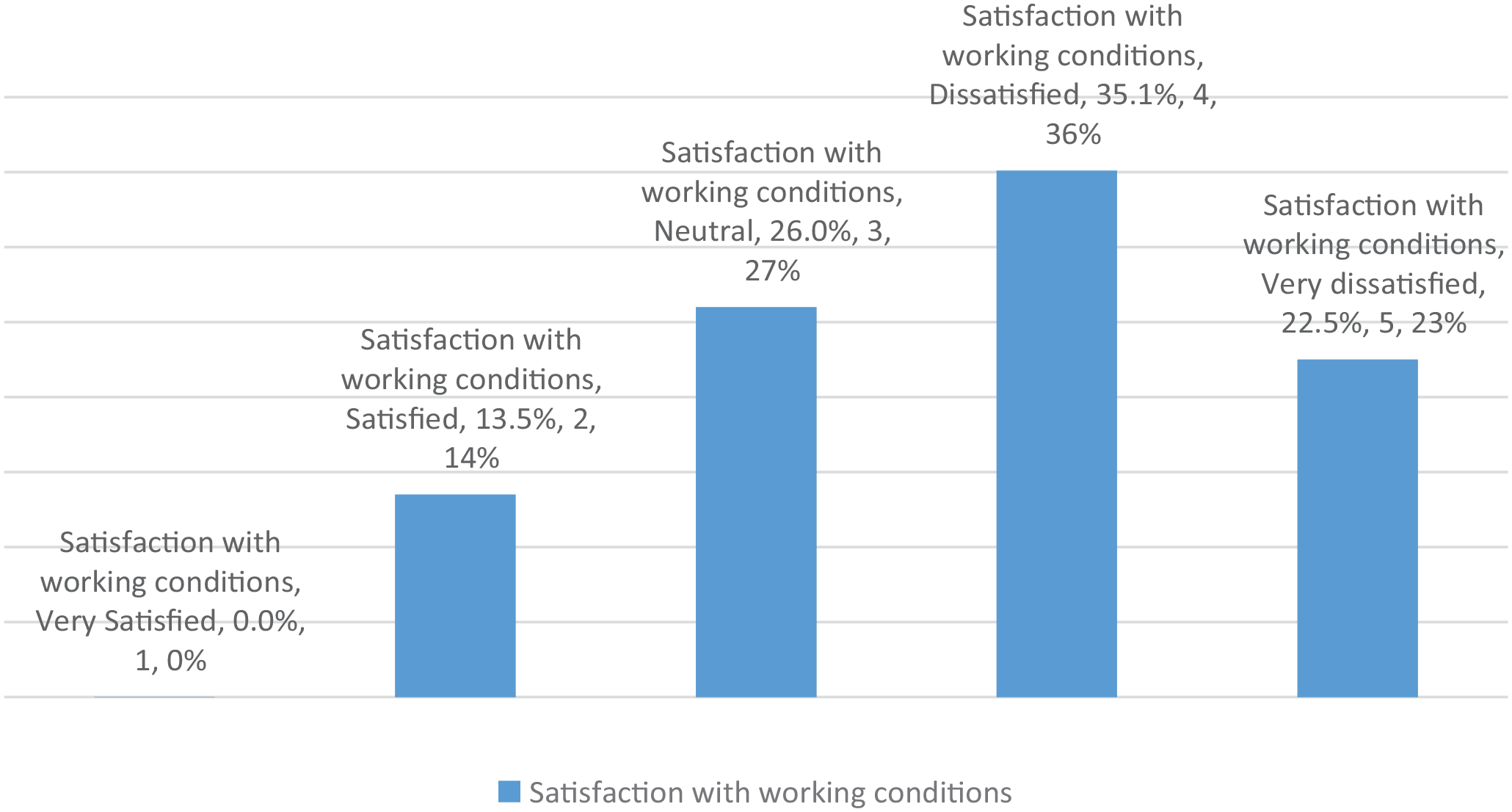
Satisfaction with working conditions.
Depression data
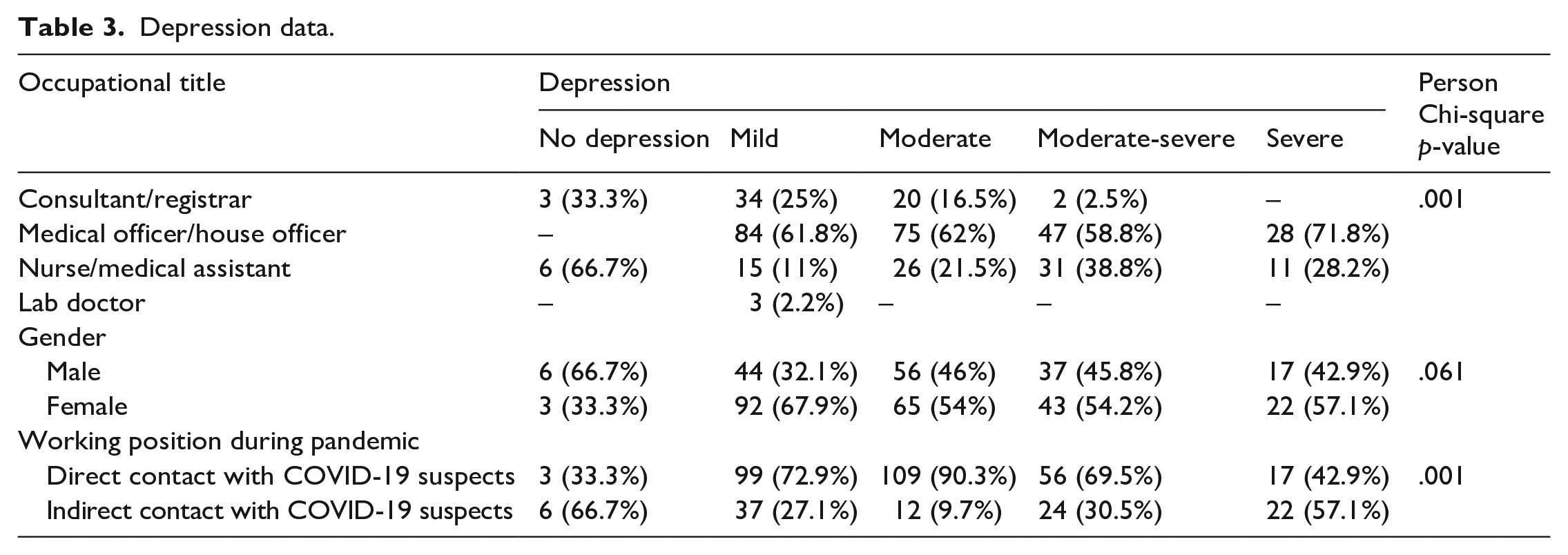
Only 2.3% of all participants had no depression while the remaining 97.7% had some degree of depression. The most frequent severity of depression was mild; 35.3%, followed by 31.4% moderate.
Normal or no depression was most frequent among 66.7% nurses and all of the junior doctors had some level of depression (p = .001).
Two-thirds of normal or no depression was found among males. All other severity levels of depression were more among females; mild, moderate, moderate-severe and severe 67.9%, 54.0%, 54.2% and 57.1% respectively (p = .061).
Normal or no depression was 66.7% in those who had indirect contact with COVID-19 suspected patients. While other severity levels; mild, moderate, moderate-severe and severe were most among HCWs who had direct contact with COVID-19 suspected patients 72.9%, 90.3%, 69.5% and 42.9%, respectively (p = .001) (Table 3).
Depression data.
Anxiety data
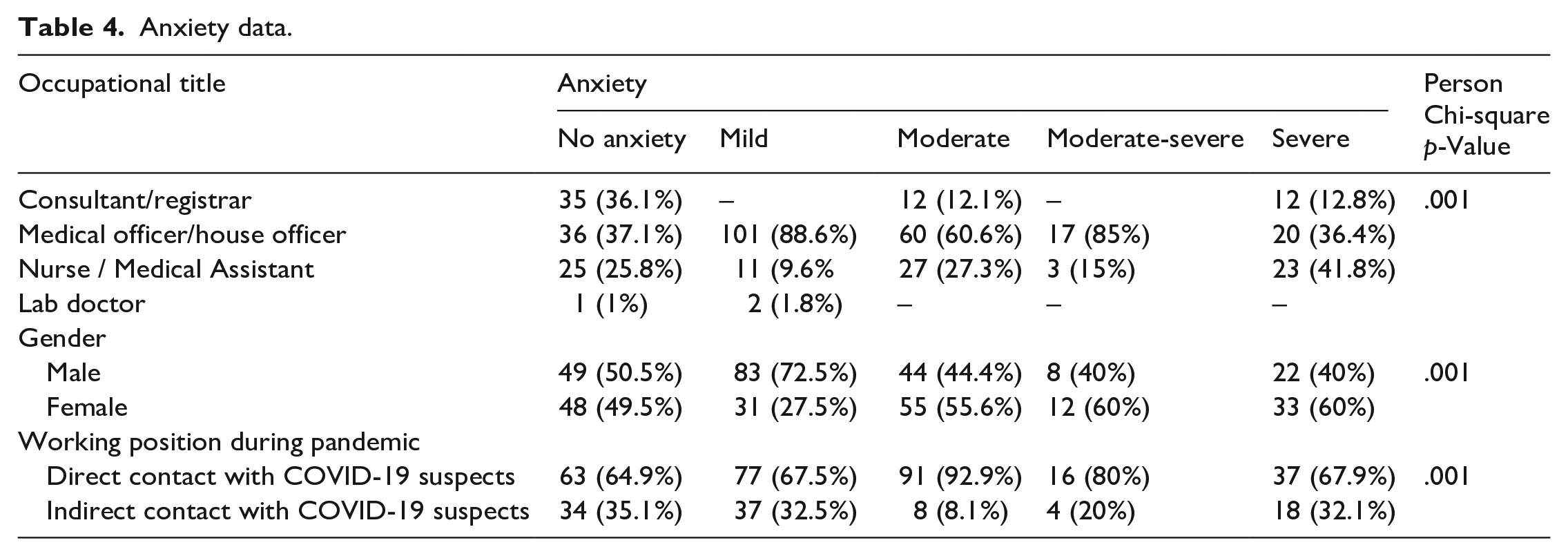
Of all participants a quarter (25.1%) had no anxiety while the remaining (74.9%) had some degree of anxiety. The most frequent level of anxiety was mild (29.6%), normal or no anxiety was mostly found among junior doctors (47.4%), as well as mild (88.6%), and moderate (60.6%), while severe anxiety was most frequently found among nurses (36.4%) (p = .001).
Males had a higher frequency of normal or no anxiety and mild anxiety; 50.5% and 72.5% respectively, while females had a higher frequency of moderate and severe anxiety; 60% each (p = .001).
All levels of anxiety were more among participants who had direct contact with COVID-19 suspected patients; no anxiety, mild, moderate and severe anxiety 64.9%, 67.5%, 80% and 67.9% respectively (p = .001) (Table 4).
Anxiety data.
Insomnia data
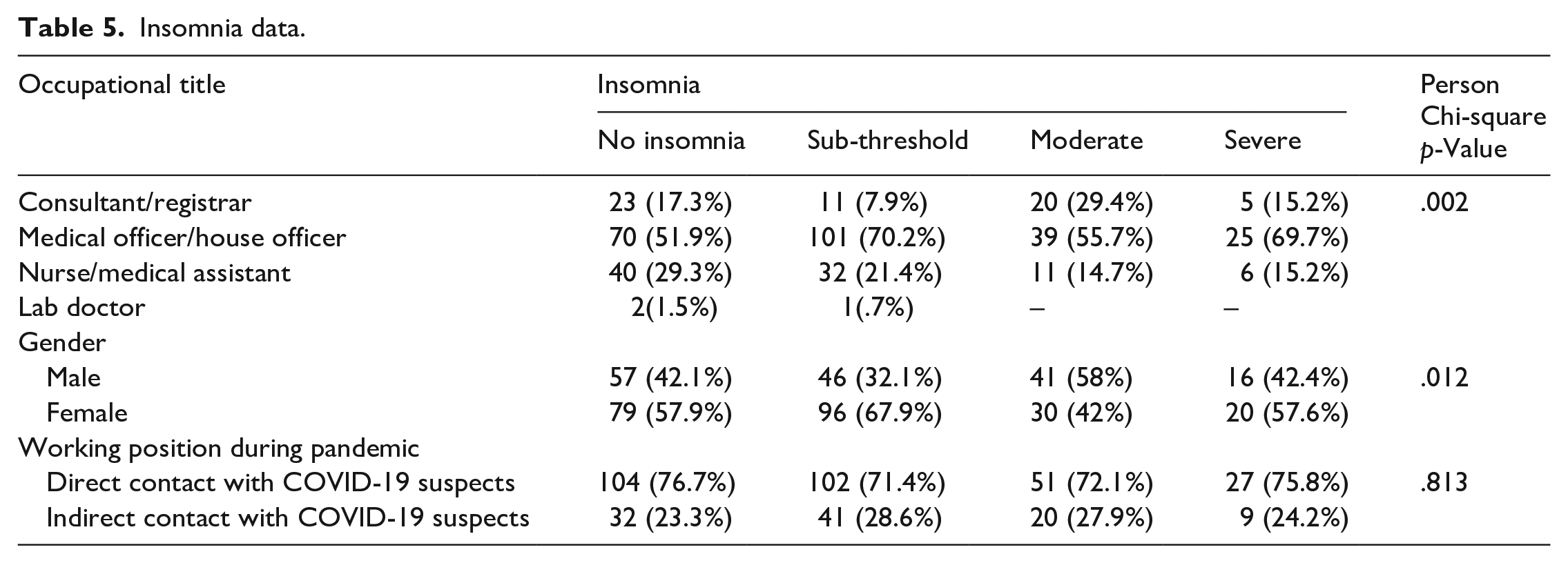
Of all participants, 35% had no insomnia while the remaining 65% had some degree of insomnia.
All severities of insomnia were more among junior doctors in comparison to others; No insomnia, sub-threshold, moderate and severe insomnia were recorded as 51.9%, 70.2%, 55.7% and 54.5% respectively, (p = .002).
No insomnia and sub-threshold insomnia were more among 57.9% and 67.9% females respectively, while moderate insomnia was more frequent among males (58%). Severe insomnia was more frequent among females (57.6%) (p = .012).
All insomnia severities were more among participants who had direct contact with COVID-19 suspected patients (p = .813) (Table 5).
Insomnia data.
Discussion
The study included 385 participants, (58.4%) were females, most were 29 years and younger (62.9%), single (78.2%) and junior doctors (60.8%) (Table 1). Approximately half of the participants worked in a general hospital (56.5%), and most had direct contact with COVID-19 patients and suspected patients (73.8%). When asked about the provision of PPE, 28.3% of participants answered sometimes, followed by 27.0% often, 22.3% always, 12.2% rarely and the least answer was never (9.4%). Living quarters were provided for 27.8% only (Table 2).
37.3% participants were very dissatisfied with the salary given to them, and only 0.8% was very satisfied with the salary (Figure 1). Most participants were dissatisfied with working conditions (35.1%), none were very satisfied with the working conditions and only 13.5% were satisfied (Figure 2).
The psychological disorders and mental strain of the HCWs who are in direct contact with the COVID-19 patients and suspected patients are reported in this study and can be attributed to these stressful, unsatisfactory working conditions. The overall discovered values were that 97.6% had some degree of depression, 74.8% had some degree of anxiety and 64.9% had some degree of insomnia. These, in comparison with another study found that the prevalence of anxiety symptoms and depressive symptoms were 15.9% (95% CI [150, 171]) and 34.6% (95% CI [332, 359]), respectively (Juan et al., 2020). In the same article, it was discovered that being a female and/or a junior doctor were linked to having more severe sadness, anxiety and insomnia (all p = .5).
Another research study conducted in Singapore during the COVID-19 pandemic, that used different Depression, Anxiety and Stress Scales (DASS-21) to assess mental status, found that 14.5% of participants screened positive for anxiety (Tan et al., 2020), whereas another study using the 7-item Generalised Anxiety Disorder scale, which we used in this study (Zhu et al., 2020), found that 44.6% of participants had some degree of anxiety, which is lower than ours, that is, 74.7%. Another research conducted in Peshawar, Pakistan, between March and April 2020 to analyse the personal and professional impact of COVID-19 on health care providers found that participants were apprehensive, frustrated and stressed out (Sethi et al., 2020). The participants in the stated study were largely females (56.5%), comparable to our study’s female participants (58.4%), and our findings were generally agreed upon.
Female and junior doctors with fewer years of experience reported more severe symptoms. The reason being that there job requirement demands them to be in constant practice and learning due to which they have to be in compact and frequent contact with patients, thus they are at a higher risk of infection. Previous investigations (Peter et al., 2022; Rashid et al., 2022) found similar results, and another research done among emergency department HCWs confirmed our findings (Serrano-Ripoll et al., 2020).
Having direct contact with COVID-19 patients and suspected patients or working in the front line was a risk factor and was associated with severe anxiety, moderate-severe depression and moderate insomnia (p < .5, for all). These findings raise alarm regarding the psychological health of HCWs involved in the COVID-19 outbreak. Similarly to this current study in a previous one; 89% of health care workers who were in direct and indirect contact with patients and suspected patients had psychological symptoms during an acute SARS outbreak (An et al., 2020).
As previously stated, all psychosomatic reactions to an infectious illness outbreak are complicated, adding to the fact that HCWs are at the centre of this. They are even more stressed, because of the feelings of vulnerability or being in an uncontrolled situation, concerns about their health and the fear of becoming a vector and spreading the virus to their families and friends, in addition to this, the changes in work routine, and being isolated (Zaçe et al., 2021).
The shortages of supplies or lack thereof as present in our study and an increasing influx of suspected and confirmed cases of COVID-19 are risk factors for the worsening psychological health of HCWs (Chan-Yeung, 2004). Again similar to this study another previous one during an epidemic stated that HCWs were not provided with adequate PPE (Billings et al., 2021).
Conclusion
As a result of the pandemic and the rising health catastrophe medical workers faced a slew of physiological and psychological challenges. Feelings of vulnerability or lack of control, anxiety for their health, the transfer of the virus to their family and others, and isolation heighten physicians’ discomfort. They also have to deal with patients who are extremely ill and are more prone to develop problems and die. It resulted in extra work and stress for doctors, as well as violent attacks. Despite having little money and, in some cases, no equipment or prescription, these people are ready to put their lives and the health of their families on the brink of risk to save others. Unsurprising the percentage of people who are stressed at work is higher.
Due to insufficient working conditions and compensations, as well as a lack of suitable PPE, healthcare personnel in Sudan during the COVID-19 crisis were under a great deal of stress, which had harmed their mental health. Occupational fatigue and emotional exhaustion among doctors may have been exacerbated in recent months by a variety of miscellaneous factors. Following COVID-19, new leadership will have an opportunity to learn and develop the health system even further by boosting investments in health infrastructure and staff. If the Sudanese public health system can accommodate the shock of this pandemic and contain it without a rise or explosion in the number of patients, the funding, resources and logistics that were swiftly assigned to the COVID-19 response will be helpful. This might aid in reorienting health policy and government financial objectives.
Footnotes
Acknowledgements
I am grateful to my colleagues and mentors at Sudan Medical Specialization Board, Khartoum, Sudan.
Author contributions
The authors have contributed to writing, designing, compiling and editing the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The authors have sought approval from the Sudan Ministry of Health.