
Abstract
Background:
Psychosis is a mental disorder that, despite its low prevalence, causes high disease and economic burden. Inadequate knowledge, lack of confidence and stigmatising attitudes of healthcare professionals (HCPs) may lead to suboptimal care.
Aim:
To review the literature exploring HCPs’ knowledge, confidence and attitudes in relation to psychosis care.
Method:
A systematic search was undertaken across three databases (MEDLINE, Embase, PsycINFO) using a search strategy encompassing the concepts: ‘healthcare professionals’, ‘knowledge, attitude, and confidence in care’ and ‘psychotic illnesses and symptoms’ to identify relevant records published from 1st January 2002 to 18th March 2022. Results were screened against predetermined inclusion and exclusion criteria by title and abstract, followed by full text. Data were extracted into tables and synthesised narratively.
Results:
Initially, 7,397 studies were identified. Following two-stage screening, 24 studies were eligible for inclusion. Of these studies, 16 explored attitudes, four explored knowledge and attitudes, one explored knowledge, one explored confidence, one explored attitudes and confidence in care and one explored all three constructs. Most HCPs in the included studies demonstrated stigmatising attitudes towards people with psychosis. Furthermore, certain HCPs, including nurses and general practitioners, demonstrated low levels of knowledge, while psychiatrists, occupational therapists, psychologists and nurses had low levels of confidence in caring for people with psychosis. Conversely, positive attitudes were also observed in some HCPs resulting from having acquaintances with lived experience of psychosis. The need for additional education and training to improve HCPs’ knowledge and confidence in relation to caring for people living with psychosis was identified.
Conclusions:
Most attitudes identified were negative and stemmed from stigma, while some were positive due to HCPs’ compassion and familiarity with psychosis. The level of knowledge and confidence identified were mostly suboptimal, and so further research is required to develop and evaluate tailored interventions to address this gap.
Keywords
Introduction
Psychosis is a feature of several chronic and severe illnesses, and symptoms of this mental condition are commonly associated with both high economic and health burden (Carr et al., 2003; de Oliveira et al., 2016; Jablensky et al., 2000; Rössler et al., 2005). For instance, the most common psychotic disorder, schizophrenia, has accounted for annual costs ranging from US$94 million to US$102,396 million in various countries since 2013 (Chong et al., 2016) and those diagnosed with the disorder are eight times more likely to die by suicide compared to the general population (Sher & Kahn, 2019; World Health Organization, 2021). According to previous psychosis literature, these health outcomes are potentially suggestive of inadequate health interventions (Carr et al., 2003; Chong et al., 2016) and thus, to improve and ultimately prevent these occurrences, causes of these inadequacies need to be explored.
While healthcare professionals (HCPs) are at the forefront of mental healthcare and have the responsibility of improving the health and well-being of people living with mental illness, including conditions which feature psychosis (World Health Organisation, 2021), negative attitudes towards mental illness are still prevalent among HCPs (Henderson et al., 2014; Thornicroft et al., 2016). Evidence shows that negative attitudes towards psychosis are significantly more common across various healthcare professions and healthcare settings compared to other mental health conditions (Mestdagh & Hansen, 2014; Rao et al., 2009; Valery & Prouteau, 2020). This is of concern as people with psychosis have been reported to be at a higher risk of suboptimal access to health and social services. They are also more vulnerable to human rights violations such as long-term confinement in institutions (Rüsch et al., 2005; World Health Organisation, 2019) based on ‘perceptions of dangerousness, unpredictability and permanence’ (Crisp et al., 2005). Therefore, attitudes present in HCPs when caring for people with psychosis need to be reviewed to determine factors that may cause negative attitudes and those that may nurture positive attitudes.
Furthermore, the knowledge and confidence HCPs have in treating mental illnesses and conditions are also constructs that contribute to the determination of health outcomes (Compton et al., 2007; Shinde et al., 2014). Previous reviews have identified that HCPs generally possess inadequate levels of knowledge and confidence with the exception of observed improvements when HCPs were exposed to educational interventions or specialised training (Boukouvalas et al., 2020; Dalky et al., 2020; Elyamani & Hammoud, 2020; Szajna et al., 2021). However, these findings have only been explored extensively in relatively more common mental health conditions or mental health in general, and no study has yet to review these constructs specifically focusing on psychosis. As such, the aim of this systematic review was to examine existing literature exploring HCPs’ attitudes, knowledge and confidence in caring for people with psychosis.
Methods
Search strategy
A systematic literature search was conducted across three databases (MEDLINE, Embase and PsycINFO; all hosted via Ovid®) and reported in accordance with the updated PRISMA guidelines (Page et al., 2021). Relevant subject headings and keywords synonymous with the three searchable concepts ‘healthcare professionals’, ‘knowledge, attitude, and confidence in care’ and ‘psychotic illnesses and symptoms’ were combined using Boolean operators (‘and’ or ‘or’) to form a search strategy capturing relevant studies (Supplemental File, Appendix 1). Additionally, limits were applied to only include human studies published in English between 1st January 2002 to 18th March 2022, to capture the current literature in this area. A review protocol was not registered.
The primary author (JCh) drafted the search strategy under the guidance of the two other authors (SE and JCo). The draft search strategy was piloted in each of the databases by JCh, and then reviewed by SE and JCo. Following this, all three authors met to finalise the search strategy.
Eligibility criteria
Of the records identified across the three databases, studies were included based on the following inclusion criteria:
(a) published in the form of a primary research article; AND
(b) explored HCPs’ knowledge of people with psychosis; AND/OR
(c) HCPs’ beliefs and/or attitudes towards people with psychosis; AND/OR
(d) HCPs’ confidence in caring for people with psychosis; AND
(e) participants were HCPs, which was operationally defined as any accredited health professionals who had fully completed their education or training in their respective field of practice.
The exclusion criteria were as follows:
(a) non-primary research such as conference abstracts, grey literature, editorials, reviews, commentaries, letters, OR
(b) non-healthcare professional participants including family members, friends, or other informal carers of people with psychosis, government officials, trainees, students, OR
(c) participants were HCPs who had lived experienced of psychosis themselves, OR
(d) studies that did not have a central focus on the state of psychosis or conditions wherein psychosis is a typical feature of (e.g. bipolar disorder) OR the definition of the psychotic disorder/s included in the study did not specify the presence of psychosis (e.g. depression), OR
(e) studies that included mixed participant populations including both HCPs and non-HCPs where findings could not be separated.
For the purpose of this systematic review, people with psychosis were operationally defined as individuals who have experienced psychosis as part of a psychotic illness or as a symptom of a general medical condition. While intervention studies were included, they were not the primary emphasis of this review.
Screening
Systematic search results were exported to EndNote X9 (Clarivate Analytics, PA, USA) before duplicates were identified and excluded using EndNote X9’s automated de-duplication tool and manual means. The remaining records were screened against the inclusion and exclusion criteria, based on titles and abstracts. Following title and abstract screening, an independent random audit of 25% of excluded records was performed by JCo. Finally, the inclusion and exclusion criteria were applied to the full text of the remaining records. Any records with ambiguous eligibility were discussed among three authors (JCh, SED, JCo) to reach consensus.
Data extraction and quality appraisal
Data relevant to the aims of the review were extracted from each included study and compiled into purposed-designed tables. Specific data extracted included the author names, year of publication, country(ies) the study was conducted in, HCP specialisation(s), HCP sample size, mental illness(es) or symptom(s) explored, instrument(s) used, construct(s) explored and the key finding(s).
Quality appraisal was conducted using the Mixed Methods Appraisal tool (MMAT) version 2018 (Hong et al., 2018). MMAT is designed with the purpose of appraising studies with study designs that are qualitative, quantitative randomised controlled trials, quantitative non-randomised, quantitative descriptive, or mixed methods. Quality appraisal of the included studies was undertaken by JCh and LP and then discussed until consensus was met regarding the quality of each study.
Results
Upon systematic searching of three databases,7,397 records were identified (Figure 1), from Embase (n = 2,746), MEDLINE (n = 1,335) and PsycINFO (n = 3,316). Duplicated records (n = 1,956) were removed through automatic and manual means, resulting in5,441 records eligible for title and abstract screening. A further5,369 records were removed during title and abstract screening, leaving 72 full-text records to be screened. The independent random audit performed resulted in no excluded studies been re-included, and 24 records were finally deemed eligible for inclusion in the systematic review and underwent data extraction.
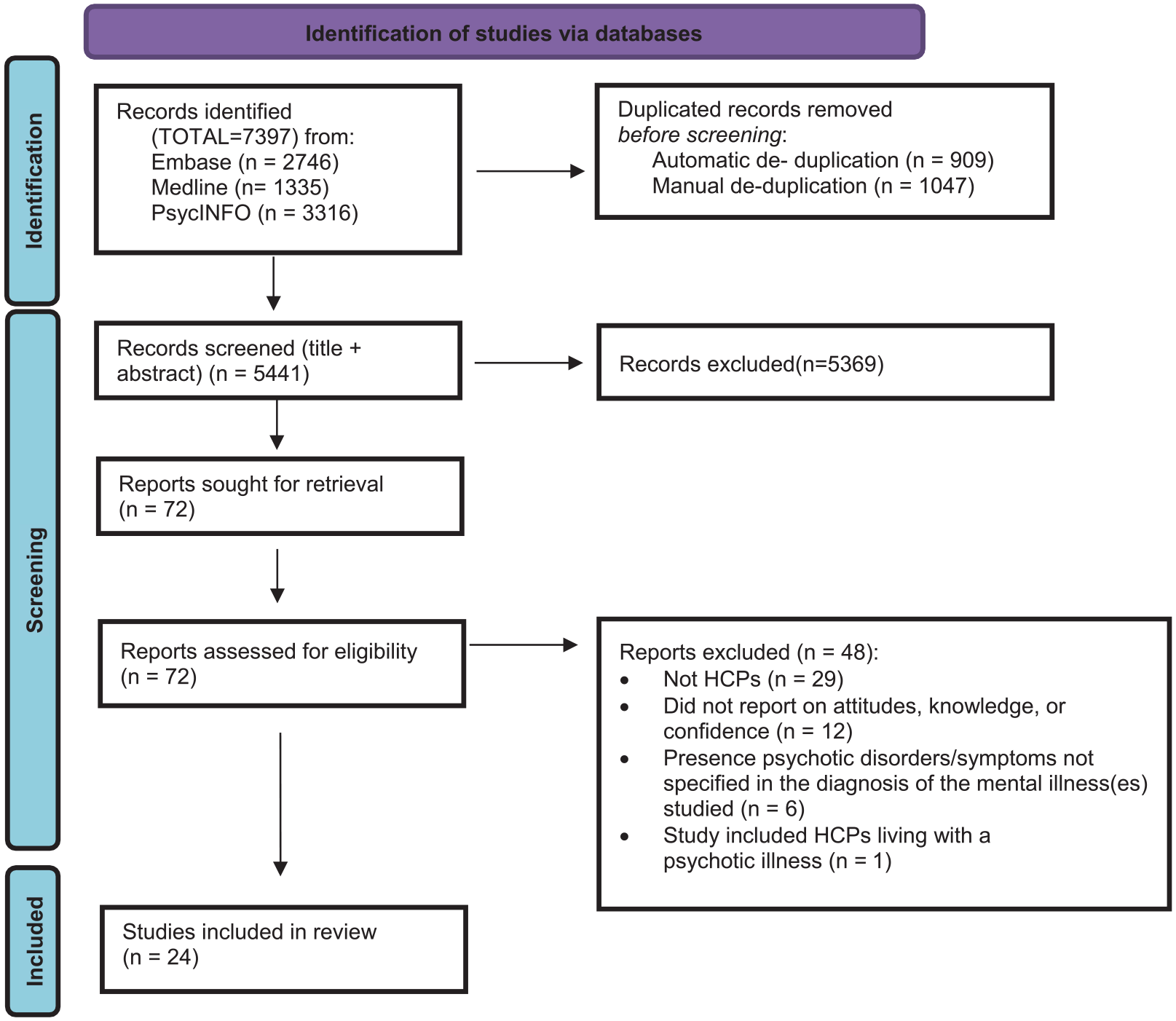
PRISMA flow diagram of the study selection process (Page et al., 2021).
Study characteristics
The included studies consisted of quantitative studies that used questionnaires (n = 15) as well as a mixed method study that used written surveys and focus group discussions (n = 1) (Table 1). The remaining studies were qualitative with research designs including semi-structured interviews (n = 4), focus group discussions (n = 2) and an open-ended questionnaire (n = 1) (Table 2). It was noted that no studies incorporated randomised controlled trials, one study had a pre-post design (Ucok et al., 2006), and the remaining were cross-sectional.
Quantitative descriptive and mixed method studies on HCPs’ knowledge of, attitudes towards and confidence in caring for people with psychosis.
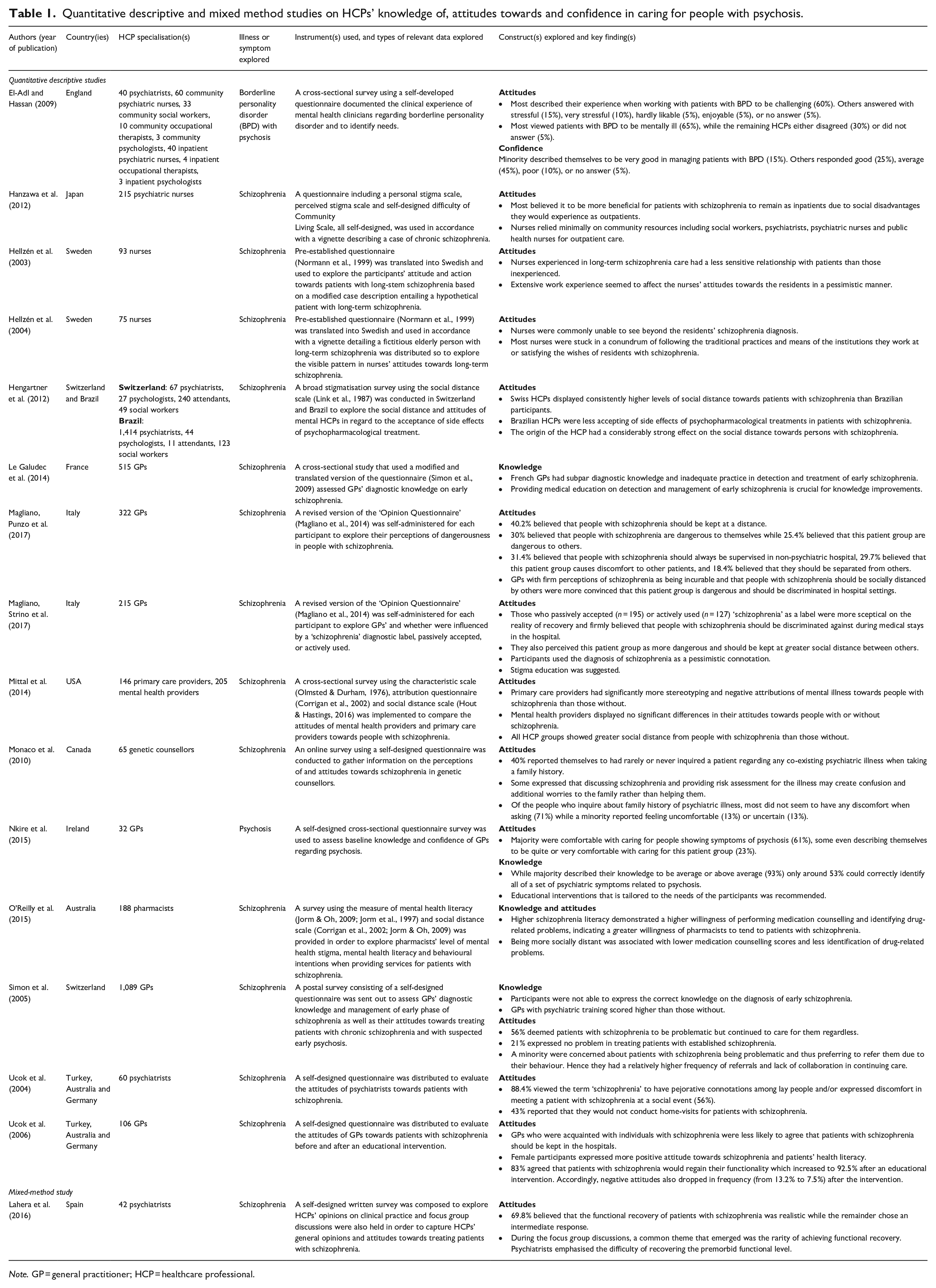
Note. GP = general practitioner; HCP = healthcare professional.
Qualitative studies on HCPs’ knowledge of, attitudes towards and confidence in caring for people with psychosis.
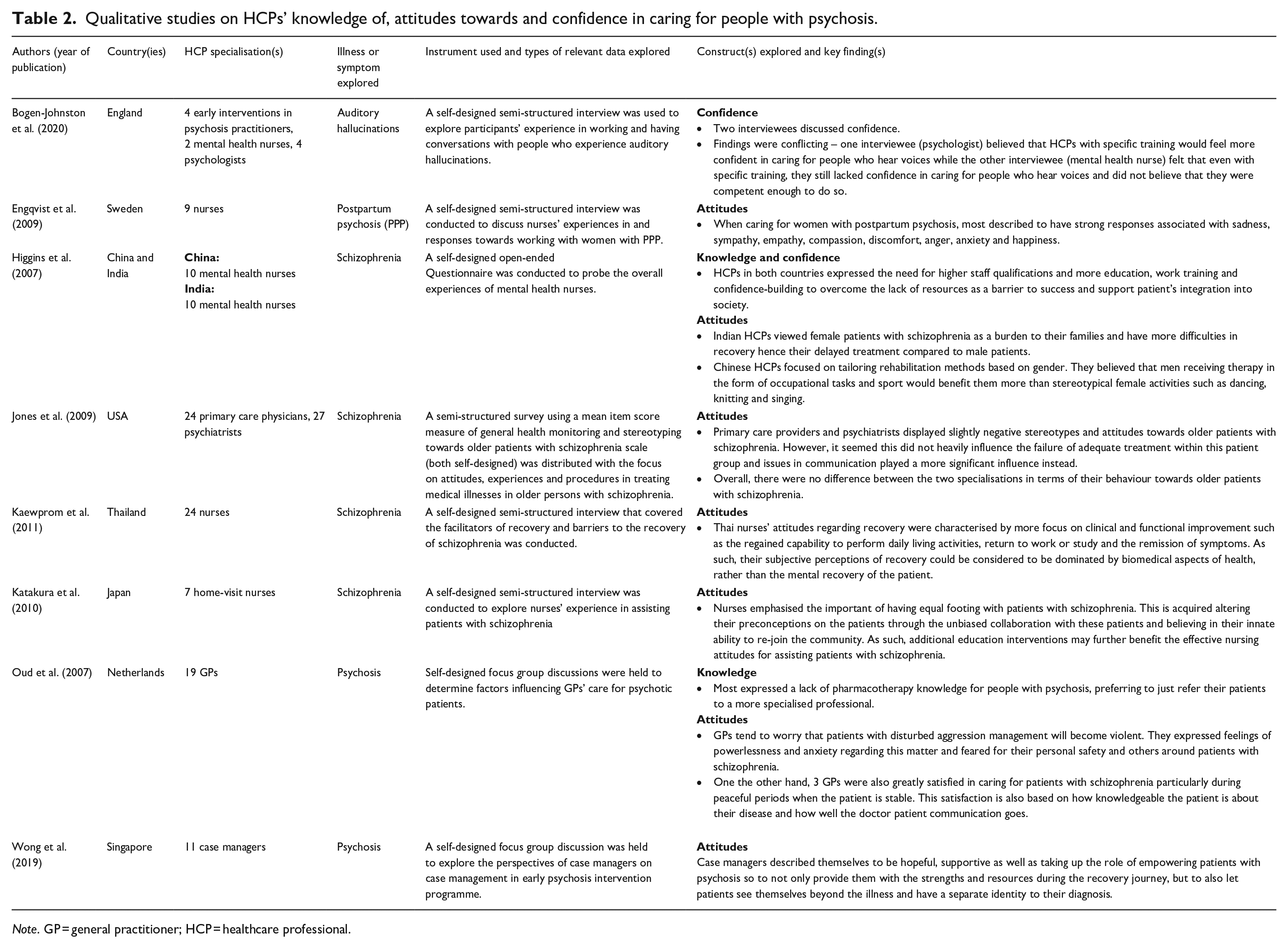
Note. GP = general practitioner; HCP = healthcare professional.
Illnesses or symptoms explored included schizophrenia (n = 18), psychosis (n = 4), auditory hallucinations (n = 1) and borderline personality disorder with the presence of psychosis (n = 1). Most studies were conducted within a single country including Sweden (n = 3), England (n = 2), Japan (n = 2), USA (n = 2), Italy (n = 2), France (n = 1), Canada (n = 1), Ireland (n = 1), Australia (n = 1), Switzerland (n = 1), Spain (n = 1), Thailand (n = 1), Netherlands (n = 1) and Singapore (n = 1). The remaining studies were conducted across multiple countries, including Turkey, Australia and Germany (n = 2), Switzerland and Brazil (n = 1), and China and India (n = 1). Studies that explored one type of HCP explored specialisations including general practitioners (GPs; n = 7), nurses (n = 7), psychiatrists (n = 2), genetic counsellors (n = 1), pharmacists (n = 1) and case managers (n = 1). The remaining explored mixed populations of HCPs (Tables 1 and 2). Finally, most studies were identified to have explored HCPs’ attitudes (n = 16), knowledge (n = 1), or confidence (n = 1) as sole constructs while the remaining studies explored combinations of knowledge and attitude (n = 4), attitude and confidence (n = 1), or all three constructs (n = 1).
Attitudes of HCPs
Ten studies exploring attitudes had heavy emphasis on findings that were relatively negative or apathetic. Findings included nurses believing that people with psychosis should be hospitalised (Hanzawa et al., 2012), or that extensive experience in psychosis care desensitised them which, as a result, led to the development of negative attitudes towards these patients (Hellzén et al., 2003). Moreover, GPs were reported to believe that people with psychosis should be kept at a distance from others and be supervised (Magliano, Punzo et al., 2017), or that they are problematic and dangerous in nature (Simon et al., 2005). GPs also found people with psychosis to be frightening as patients would become violent and harm others (Oud et al., 2007), or had sceptical outlooks on the reality of recovery in people with psychosis (Magliano, Strino et al., 2017). Other HCPs, such as mental health clinicians, found working with people with psychosis to be challenging (El-Adl & Hassan, 2009), genetic counsellors avoided discussing family histories of psychotic illnesses and symptoms with patients (Monaco et al., 2010), and primary care physicians and psychiatrists both expressed equal levels of discomfort towards older patients (Jones et al., 2009). Finally, three studies focusing on nurses, mental health nurses and psychiatrists respectively viewed people with psychosis more so under clinical perspectives rather than seeing beyond their psychiatric diagnoses (Hellzén et al., 2003; Kaewprom et al., 2011; Ucok et al., 2004).
Four studies focused on more positive attitudes and outlooks towards people with psychosis and their continuing progress. These findings were credited to having acquaintances with psychosis (Ucok et al., 2004) or having compassion for people with psychosis (Katakura et al., 2010; Lahera et al., 2016; Wong et al., 2019). Home visit nurses expressed their appreciation towards the importance in treating people with psychosis respectfully and fairly (Katakura et al., 2010), while case managers remained hopeful and were willing to provide support as part of the recovery journey (Wong et al., 2019). There were also findings describing HCPs’ optimistic outlook on psychosis recovery. These included psychiatrists’ belief that patients can regain functionality and that functional recovery is realistic, despite statistics that suggest otherwise (Lahera et al., 2016), as well as GPs’ dismissal of stigmatising beliefs such as confining people with psychosis to hospitalisation as a result of having acquaintances with psychosis (Ucok et al., 2006).
One study conducted by Engqvist et al. (2009) also reported findings which demonstrated mixed attitudes. Through a qualitative design of semi-structured interviews among nine Swedish nurses in response to their work with mothers with postpartum psychosis, feelings of sadness, sympathy, empathy, compassion, discomfort, anger, anxiety, or happiness were expressed among this participant population (Engqvist et al., 2009).
Relationship between types of HCPs and their attitudes
Two studies that explored mixed populations of HCPs and their differences in attitudes towards people with psychosis. In particular, Mittal et al. (2014) found that overall, mental health providers, including psychiatrists, psychologists and mental health nurses, had significantly less negative attitudes towards people with schizophrenia than primary care providers. Meanwhile, Jones et al. (2009) demonstrated that primary care providers and psychiatrists showed no significant differences in attitudes towards patients with schizophrenia, albeit the study only focused on the elderly.
Relationship between HCPs’ country(ies) of practice of and their attitudes
Of the studies that were conducted across multiple countries, Hengartner et al. (2012) demonstrated that HCPs including psychiatrists, psychologists, professional attendants and social workers were more likely to socially distance from people with schizophrenia if they were based in Switzerland compared to those originating from Brazil. Meanwhile, it was found that Brazilian HCPs had more reluctance in acknowledging the side effects of psychopharmacological treatments received by patients with schizophrenia (Hengartner et al., 2012). These differences may have occurred due to the possible differences in socio-cultural background and medication availabilities between the two countries. On the other hand, Higgins et al. (2007) found that mental health nurses’ views on gender with regard to patients living with schizophrenia were influenced by their country of origin. In India, mental health nurses associated female patients with schizophrenia with negative connotations regarding their status within their family as well as in the community. As a result, HCPs would delay their treatment compared to male patients with the same illness (Higgins et al., 2007). Comparably, Chinese mental health nurses incorporated gender stereotyping to tailor of patient-specific rehabilitation methods rather than that of prejudice. For instance, male patients with schizophrenia were more likely to receive occupational tasks and sport as activities of rehabilitation while female patients were implemented leisure activities of dancing, knitting and singing instead (Higgins et al., 2007).
Level of knowledge in HCPs and the importance of educational interventions
Five studies that explored HCPs’ knowledge in psychosis noted the importance of educational interventions. Higgins et al. (2007) explored concerns of Chinese and Indian mental health nurses regarding their knowledge on schizophrenia and the need for improvement, Le Galudec et al. (2014) assessed the diagnostic knowledge of schizophrenia of French GPs, Nkire et al. (2015) compared Irish GPs’ self-rated level of knowledge to their objective ability in identifying psychotic symptoms, O'Reilly et al. (2015) explored the correlation between knowledge and the provision of service in patients with schizophrenia among Australian pharmacists and Simon et al. (2005) objectively measured the knowledge of Swiss GPs in diagnosing early schizophrenia. While Le Galudec et al. (2014), Nkire et al. (2015), Simon et al. (2005) and O'Reilly et al. (2015) used quantitative analysis of survey responses to examine knowledge, Higgins et al. (2007) qualitatively analysed open-ended responses to self-designed surveys.
Despite the variations in the country(ies) where studies were conducted, diagnosis, or HCP population studied, the general consensus across the five studies was that HCPs had an inferior level of knowledge needed to provide optimal care for people with psychosis. In conjunction, the implementation of educational interventions was frequently recommended to improve knowledge in HCPs regarding people with psychosis. In particular, Simon et al. (2005) identified that Swiss GPs who had a history of educational training in psychiatry had better diagnostic knowledge on early schizophrenia than those who did not attend prior psychiatry education.
Level of confidence in HCPs and the need for improvement
Three studies focussed on assessing HCPs’ confidence in caring for people with psychosis. The study conducted by El-Adl and Hassan (2009) surveyed a mixed population of nurses, social workers, occupational therapists and psychologists, on managing borderline personality disorder with psychosis. As a result, 15% answered very good, 25% answered good, 45% answered average, 10% answered poor and the remaining 5% did not answer. Moreover, Higgins et al. (2007) provided questionnaires for 10 mental health nurses from Beijing and 10 mental health nurses from Calcutta regarding schizophrenia rehabilitation across culture. Accordingly, it was concluded that the success of rehabilitation programmes in China and India was impeded due to a lack of resources, inadequate work-training and confidence-building amongst staff, ultimately highlighting the need to implement more educational interventions and requirements for higher qualifications to improve confidence levels. Meanwhile, Bogen-Johnston et al. (2020) presented conflicting findings upon interview a mixed population group of early intervention in psychosis practitioners, mental health nurses and psychologists whereby one psychologist believed special training in the management of auditory hallucinations would improve HCPs’ confidence while one mental health nurse believed otherwise.
Interplay between multiple constructs
While five studies explored multiple constructs, only O'Reilly et al. (2015) looked into the interplay between them. Specifically, the study attributed higher schizophrenia literacy in pharmacists to a higher willingness to tend to patients with the disorder (O'Reilly et al., 2015).
Quality assessment
A summary of the critical appraisal using MMAT (Hong et al., 2018) is shown in Appendix 2 (Supplemental File), with detailed assessments included in Supplemental Tables A2–A4 for quantitative descriptive, mixed method and qualitative studies respectively. Assessment with MMAT identified 14 of the 24 included studies to be of high quality, five were of moderate quality and the remaining five were of low quality.
Discussion
This systematic review explored HCPs’ knowledge of, attitude towards and confidence in caring for people with psychosis. A variety of attitudes were identified, ranging from negative attitudes, positive attitudes, to mixed attitudes. Furthermore, there was a notable suboptimal level of both HCPs’ knowledge of and confidence in caring for people with psychosis, demonstrating a need to improve the standard of education and training for HCPs who care for people with psychosis. Additionally, the review identified potential associations between healthcare specialisations, country of practice and HCPs’ attitude towards people with psychosis.
Majority of the studies in this review demonstrated HCPs across various healthcare settings to have stigma towards psychosis and psychotic symptoms. To improve these attitudes, being in contact with individuals with psychosis has been noted as a positive influence. Despite Ucok et al. (2006) being the only included study to report on this notion whereby GPs who had acquaintances with schizophrenia were observed to have more positive attitudes towards the disorder than those who did not, a randomised controlled trial conducted on student nurses demonstrated that using filmed or live social contact with people with psychosis as a means of reducing stigma was effective (Clement et al., 2012). Furthermore, various studies from broader literature have also been able to correlate contact has been effective to reduce mental illness stigma among the general population (Corrigan et al., 2007; Couture & Penn, 2003), as well as HCPs and students (Lien et al., 2021), and so more studies need to be conducted to explore the idea of tailoring contact with people with psychosis into anti-stigma programmes for HCPs.
In this review, HCPs also possessed an overall low level of knowledge regarding psychotic illness diagnoses and recognising psychotic symptoms, and the need for more training and educational interventions was identified in all four studies that assessed HCPs’ knowledge (Higgins et al., 2007; Le Galudec et al., 2014; Nkire et al., 2015; Simon et al., 2005). However, only one study assessed the effect of education on HCPs’ knowledge of people with psychosis, particularly that of the GP population (Simon et al., 2005). Improving HCPs’ pre-existing low confidence in caring for people with psychosis through education and training was recommended among studies assessing HCPs’ confidence (Higgins et al., 2007). The potential of exploring the role of training in improving confidence in caring for people experiencing poor mental health is supported by a study conducted in the United States by Jacobson et al. (2012) who found that by completely a 2-day suicide training programme, clinicians reported a significant improvement in their confidence to care for patients at risk of suicide. Furthermore, it is also found effective across healthcare in general among healthcare students (Alanazi et al., 2017). As such, future work should examine the effect of education and training on improving HCPs’ knowledge in and confidence in caring for people with psychosis as well as exploring the specific training that needs to be conducted for different HCP specialisations in different settings and stages of practice.
Discrepancies were observed when comparing studies exploring knowledge due to differences in the instruments used to measure this construct. Notably, all but one study (O'Reilly et al., 2015) used self-developed instruments which may not be validated and make drawing comparisons difficult. The lack of standardisation in assessing HCPs’ knowledge of mental illnesses such as psychosis may be explained by the difficulty in establishing universal measures that can be implemented internationally and accommodate for different practice settings and health disciplines (Stanton et al., 2014). It is also difficult to prioritise specific items when addressing constructs as broad as knowledge. As such, further work is required to develop psychometrically sound instruments to assess HCPs’ knowledge in this space. Similarly, there is a lack of standardised instrument to measure HCPs’ confidence in caring, although these exist in other areas of mental healthcare such as perinatal bereavement care (Kalu et al., 2020). The lack of standardised instruments to measure knowledge and confidence in caring of people with psychosis, may have disproportionately contributed to the smaller number studies investigating these constructs compared to HCPs’ attitudes.
Ultimately, when considering the three constructs explored in the current review simultaneously, there seems to be a lack of data regarding the interplay between the three, unlike previous reviews of similar nature such as Boukouvalas et al. (2020) who postulated a strong relationship between knowledge, confidence and attitudes under the context of HCPs’ response to people at risk of suicide. This may be due to the notion that the psychiatric circumstance of focus was drastically different, one being on suicide risk (Boukouvalas et al., 2020) and the other on psychosis which may have evoked differing responses among the included study participants of each review. Furthermore, Boukouvalas et al. (2020) reported a significant emphasis on the effect of HCPs’ knowledge on their attitudes and confidence among the included studies of their review, while the studies of this current review had minimal findings on knowledge and had a heavier sole focus on HCPs’ attitudes instead. Hence, further research exploring how attitudes and knowledge impact confidence in providing care to people with psychosis is needed, and indeed, how these in-turn result in practitioner behaviour.
Strengths and limitations
A strength of this systematic review lies in the continuous discussions and reviews that were conducted by all three authors to reach consensus regarding the search strategy, study screening and data extraction. Furthermore, the systematic review is strengthened by the robust transparency in reporting by following the PRISMA guidelines (Page et al., 2021). Limitations of this review must also be considered. Only the main author JCh was responsible for the entire screening of the studies as well as the data extraction process. Whilst an audit was performed by a co-author, it was only conducted for the title and abstracting screening phase. Additionally, due to the language and date limitations set upon the databases during the initial identification of records, not all relevant studies may have been included within our search strategy. However, it is also noted the specified time limitation was implemented as the area of study explored is constantly evolving and so restricting the time of publication of the included studies allowed for a synthesis of the most contemporary literature. Finally, healthcare students and trainees were not included in this review as well and so these populations should be explored in future work.
Conclusion
This systematic review generates insights regarding HCPs’ knowledge of, attitude towards and confidence in caring for people with psychosis. In particular, it was observed that stigma as well as suboptimal knowledge of and confidence in caring for people with psychosis existed among majority of the HCPs studied, highlighting the need for further education and training in this area. As such, the design and implementation of discipline-specific interventions with the intention of optimising knowledge, attitudes and confidence should be explored in the future. Accordingly, intervention-based studies demonstrating the impact of these interventions should also be explored so to measure how these interventions translate to actual patient outcomes and care.
Supplemental Material
sj-docx-1-isp-10.1177_00207640231194490 – Supplemental material for Healthcare professionals’ knowledge, confidence and attitudes in relation to psychosis care: A systematic review
Supplemental material, sj-docx-1-isp-10.1177_00207640231194490 for Healthcare professionals’ knowledge, confidence and attitudes in relation to psychosis care: A systematic review by Jenny Chen, Sarira El-Den, Lily Pham, Claire L O’Reilly and Jack C Collins in International Journal of Social Psychiatry
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval not required as this article does not contain research conducted with human or animal participants.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.