
Abstract
Background:
Worldwide migration represents a major challenge of the 21st century. Despite the strong association between acculturation and mental health, research findings on underlining mechanisms remain inconsistent. Prior research urges to investigate sample characteristics in a more structured manner.
Aims:
The purpose of this study was to systematically investigate factors impacting acculturation and depressive symptoms in a large, not exclusively clinical, sample of Vietnamese migrants in Germany.
Method:
This study investigated, with multiple regressions, factors (age at arrival, gender, education, religiousness, language skills, residence status, economic status, occupational status, migration motivation, duration of stay, and depressive symptoms) impacting the two dimensions of acculturation, dominant society immersion (DSI) and ethnic society immersion (ESI), in a not exclusively clinical sample (n = 582) of first-generation Vietnamese migrants in Germany. Further, this study examined the relationship between depressive symptoms, DSI and ESI with correlations and acculturation strategies with an ANOVA.
Results:
Integration (72.5%) was the most common acculturation strategy, followed by separation (26.8%). In contrast, assimilation (0.5%) and marginalization (0.2%) were very rare acculturation strategies. As predictive factors for DSI lower depressive symptoms scores, male gender, higher education, and better German language skills were found significant. For ESI, less German language skills and older age at arrival were found to be significant. Higher ESI and DSI were correlated to lower depressive symptom scores. Compared to the three other acculturation strategies, integration was linked to the lowest depressive symptoms scores.
Conclusions:
The current study identified crucial factors in the acculturation process, such as depressive symptoms, language skills, education, gender, and age at arrival. Our findings emphasize that immersion into both the dominant and the ethnic culture plays an essential supportive role in the mental health of migrants.
According to the United Nations World Migration Report 2022, the number of international migrants almost doubled in the past 30 years, from 153 million in 1990 to 281 million in 2020, making migration one of the greatest challenges of the 21st century (McAuliffe & Triandafyllidou, 2021). Mental disorders are common in all countries ranging from 10.9% prevalence in the African Region to 13.2% in Southeast Asia, to 15.6%, in the Pan-American region as reported by the World Health Organization (WHO) in 2022. After anxiety disorders, depression represents the second most prevalent mental health condition worldwide (WHO, 2022). Depression is estimated to affect over 280 million people, accounting for 3.8% of the world’s population (WHO, 2022). In Vietnam, the National Mental Hospital reported prevalence rates of 14.2% for the ten most common mental disorders and 2.45% for depressive disorders (WHO, 2023). Vulnerability to adverse mental health outcomes can differ based on various contexts, such as young age, female gender or being part of an ethnic minority (WHO, 2022). By simultaneously considering combinations of these factors, important differences in people’s specific mental health needs can be revealed (Foo et al., 2018; WHO, 2022). Migrants are particularly vulnerable to a range of stressful experiences, which can be categorized into three main phases: pre-migration stressors, such as political persecution (Chu et al., 2013) or war (Gleeson et al., 2020); peri-migration stressors, including separation from families or loss of personal belongings (Foo et al., 2018); and post-migration stressors, such as uncertainty surrounding legal status and perceived discrimination (Gleeson et al., 2020). Extensive research has been conducted on these migration related stress factors, assuming these stressors to represent significant risk factors for depression (Berry, 2019; Foo et al., 2018; Gleeson et al., 2020). International meta-analytic data reveals a depression prevalence of 15.6% among migrants globally (Foo et al., 2018), while recent German panel data indicates that 20.6% of migrant respondents reported depressive symptoms (Bartig et al., 2023). Although the impact of the experience of migration on the mental health of migrants is evident (Berry, 2019; Bhugra, 2004; Foo et al., 2018; Gleeson et al., 2020; Jannesari et al., 2020; Kluge et al., 2019; Metzing et al., 2020; Schwartz et al., 2010; ration on the mental health of migrants is Walther et al., 2020; WHO, 2022) the underlying processes are complex and remain insufficiently studied (Balidemaj & Small, 2019; Berry, 2019; Bornstein, 2017; Choy et al., 2021; Foo et al., 2018; Kluge et al., 2019; Mesquita et al., 2019).
Vietnamese migrants in Germany
While Europe hosts the largest number of international migrants (87 million), Germany represents the second-largest host country of international migrants worldwide (16 million), following the United States (51 million, McAuliffe & Triandafyllidou, 2021). Vietnamese represent Germany’s largest Southeast Asian migrant population, with a population of 185,000 (Destatis, 2020). Despite the relatively large number of Vietnamese migrants in Germany, research on this minority group remains scarce (Kim et al., 2012; Nguyen et al., 2021; Ta et al., 2014; Wolf et al., 2020). Depression was found to be the most common diagnosis among Vietnamese migrants in Germany (Ta et al., 2014), with higher (Merbach et al., 2008) to similar (Hahn et al., 2016) levels of depressive symptoms among first-generation Vietnamese migrants compared to the native population born in Germany. Compared to other migrant groups, a lower mental health care utilization was found, making Vietnamese in Germany a relevant but underserved community (Ta et al., 2014).
Acculturation
The theory of acculturation has become the major theoretical concept to understand the mental impact of migration (Choy et al., 2021; Schwartz et al., 2010). Acculturation is most frequently defined by Redfield et al. (1936) as ‘those phenomena which result when groups of individuals having different cultures come into continuous first-hand contact, with subsequent changes in the original culture patterns of either or both groups’ (Berry, 2019). Earlier acculturation models viewed acculturation as the unidimensional immersion of an individual of an ethnic minority into the host society (Berry, 2019; Choy et al., 2021; Schwartz et al., 2010). Contemporary acculturation models argue that individuals can be acculturated in both the dominant and the ethnic culture without necessarily renouncing one cultural identity for another (Berry, 2019; Choy et al., 2021; Schwartz et al., 2010). The most established model for acculturation is Berry’s (1980) bidimensional acculturation model (Choy et al., 2021; Schwartz et al., 2010). It combines the two dimensions into the four so-called acculturation strategies: integration, assimilation, separation, and marginalization (Berry, 1980). Assimilation acquires the dominant and discards the ethnic culture, and separation rejects the dominant and retains the ethnic culture. Integration includes practices of the dominant and retains those of the ethnic culture. In contrast, marginalization rejects the dominant and discards the ethnic culture. Consistent with this contemporary view of acculturation, it was often found across studies that out of these four acculturation strategies, integration is usually linked to the most positive mental health outcomes, whereas marginalization is the least successful (Balidemaj & Small, 2019; Berry, 2019; Choy et al., 2021; Yoon et al., 2013). Though bidimensional models of acculturation have been established since the 1980s (e.g., Berry, 1980) and the use of bidimensional measures has increased (Mesquita et al., 2019; Yoon et al., 2011), the independent contribution of each cultural orientation to health outcomes, especially mental health, remains still understudied (Balidemaj & Small, 2019; Gupta et al., 2013; Huynh et al., 2009; Mesquita et al., 2019). Even recent reviews in the field of acculturation research show that findings remain inconsistent (Balidemaj & Small, 2019; Choy et al., 2021). These discrepancies are usually attributed to the conceptualization and measurements of acculturation and differences in sample characteristics such as ethnicity, residency, race, gender, and age (Balidemaj & Small, 2019; Bornstein, 2017; Yoon et al., 2013). As studies using the bidimensional acculturation model tend to use smaller, convenience-based samples (Schwartz et al., 2010), authors call for studies with larger or more representative samples (Maehler et al., 2019). Furthermore, according to our knowledge, previous studies on mental health mainly focused on variation in small clinical populations. Therefore, their results cannot be generalized to the overall local migrant population. To gain a deeper understanding of the process of acculturation and consequently be able to set up more specific and thus more effective policies, many authors highlight the importance of structurally examining individual and contextual factors impacting acculturation (Balidemaj & Small, 2019; Berry, 2019; Bierwiaczonek & Kunst, 2021; Bornstein, 2017; Dow, 2011; Kosic, 2006; Rudmin, 2003; Sam & Berry, 2006; Schwartz et al., 2010).
Aim of the study
To address these issues, the present study aims to systematically investigate individual factors impacting acculturation and depressive symptoms in a large, not exclusively clinical, sample of Vietnamese migrants in Germany.
This study tests the hypotheses that the dimensions of dominant cultural immersion (DSI) and ethnic cultural immersion (ESI) are unrelated (H1). Furthermore, the hypothesis that higher ESI and DSI are correlated to lower depression scores is tested (H2). Last, this study tests the hypothesis that out of the four acculturation strategies, integration is associated with the lowest depression severity (H3).
Methods
Procedure
All participants were adult Vietnamese first-generation migrants. To obtain a representative sample and capture a wide variation of depressive symptoms, the study employed two distinct recruitment pathways. The first recruitment pathway involved data collected from participants between 2011 and 2019 before their first utilization at the psychiatric outpatient clinic specializing in Vietnamese migrants at Charité Universitätsmedizin in Berlin ( n = 395). The second pathway encompassed participants recruited between 2017 and 2018 through the Vietnamese community network in Berlin, Germany, within a non-clinical environment (n = 344). Participants in this non-utilization pathway received a compensation of 5€ for public transport costs. Ethical approval was granted by the ethical committee of Charité Universitätsmedizin Berlin (EA2/116/15). Participants gave written informed consent that collected data would be used for research purposes and filled out a structured survey assessing socio-demographic, migration-related, and clinical factors (Ta et al., 2014) in Vietnamese. As no Vietnamese versions of the PHQ-9 and the SMAS have been validated yet, the German version was translated into written Vietnamese using the back-translation technique by different bilingual translators (Brislin, 1970).
Measures
DSI and ESI were measured with the Stephenson Multigroup Acculturation Scale (SMAS) (Stephenson, 2000), covering a broad range of attitudes related to language, social interaction, food, and the media. Meta-analytic data shows that the SMAS represents one of the most common acculturation measures and demonstrates good reliability (Huynh et al., 2009). The DSI subscale, originally consisting of 15 items, was adapted by replacing terms referring to Anglo-American with German. The item ‘I understand German, but I am not fluent in German’ was excluded as the connection between the two statements seemed confusing to participants. The ESI subscale originally consisted of 15 items. The item ‘I have never learned to speak the language of my native country’ was excluded because all participants were first-generation Vietnamese migrants, making the item dispensable. The item ‘When I pray, I use my native language’ was excluded, as it seemed ambiguous whether the participant’s religiousness or language use was assessed. Participants scored on a four-point Likert scale from 1 (false) to 4 (true). For each dimension, DSI and ESI, sum scores were calculated. The midpoint on the range of possible DSI and ESI sum scores was used as a cut-point to generate the four acculturation strategies (Berry, 2019; Schwartz et al., 2010). Cronbach’s alpha was good (DSI: .876; ESI: .805).
The PHQ-9 is a widely used 9-item self-report screening tool specific to depressive symptoms, which scores each of the nine DSM-IV criteria as ‘0’ (not at all) to ‘3’ (nearly every day) (Manea et al., 2015). The Vietnamese version of the PHQ showed comparable reliability to the German version (Dreher et al., 2017; Hahn et al., 2016). Cronbach’s alpha was excellent (.938).
Potential factors affecting DSI and ESI were taken from Berry’s (2006) model ‘Factors affecting acculturative stress and adaptation’: Age at arrival (years), gender (male, female), education (no education, education completed, studies completed), religiousness (four-point response option ranging from ‘not important’ to ‘very important’), German language skills (five-point response option ranging from ‘very good’ to ‘none’), residence status (unsafe, safe), economic status (not sufficient, moderate, sufficient), occupational status (not working, working), and migration motivation (push, pull). Based on extensive literature research, the variable duration of stay (years) was identified as a further potential factor (Baek Choi & Thomas, 2009). Additionally, the factor depressive symptoms was included to consider the potential impact of mental health on acculturation (Bornstein, 2017).
Statistical analysis
All analyses were conducted using SPSS version 27. Statistical significance was set at p ⩽ .05. First, Pearson’s correlations were used to examine the relationship between DSI and ESI. Second, multiple regressions were conducted to identify significant predictor variables for DSI and ESI. A dummy coding was used for the variables education, using no education as reference category and economic status, using poor economic status as reference category. For ESI, the wild bootstrap procedure (2000 repetitions) was employed to consider the non-normal distribution and the heteroscedasticity. Third, Pearson’s correlations were used to examine the relationship between PHQ-9 and DSI and ESI, respectively, and Pearson and Filon’s z was used to compare the strength of these correlations (Hemmerich, 2017). Fourth, a univariate ANOVA was conducted to assess differences in PHQ-9 by acculturation style. Although there was a violation of the standard distribution assumption, results should not be affected, as ANOVA is robust if the compared groups are large enough (Blanca et al., 2017) as present in this study. As there was no homogeneity of variance (Levene’s test, p = .003), the results of the Welch’s-ANOVA are reported.
Drop-out Analysis
Of the original sample of N = 739, 157 participants were excluded from the analysis due to more than 25% of missing data in the key variables (SMAS, PHQ-9), resulting in a total sample size of n = 582. To ensure no significant differences between included and excluded participants concerning age, gender, and level of education exist, a drop-out analysis was performed using Little’s MCAR. No significant differences were found (Chi-square t = 9.827, DF = 8, p = .277).
Results
Sample characteristics
The sample characteristics are presented in Table 1. Age ranged from 16 to 81 years, with a mean age of 44.8 (SD = 12.65). 66.5% of respondents were female. The average time lived in Germany was 18 years (SD = 11.52).
Sample characteristics.
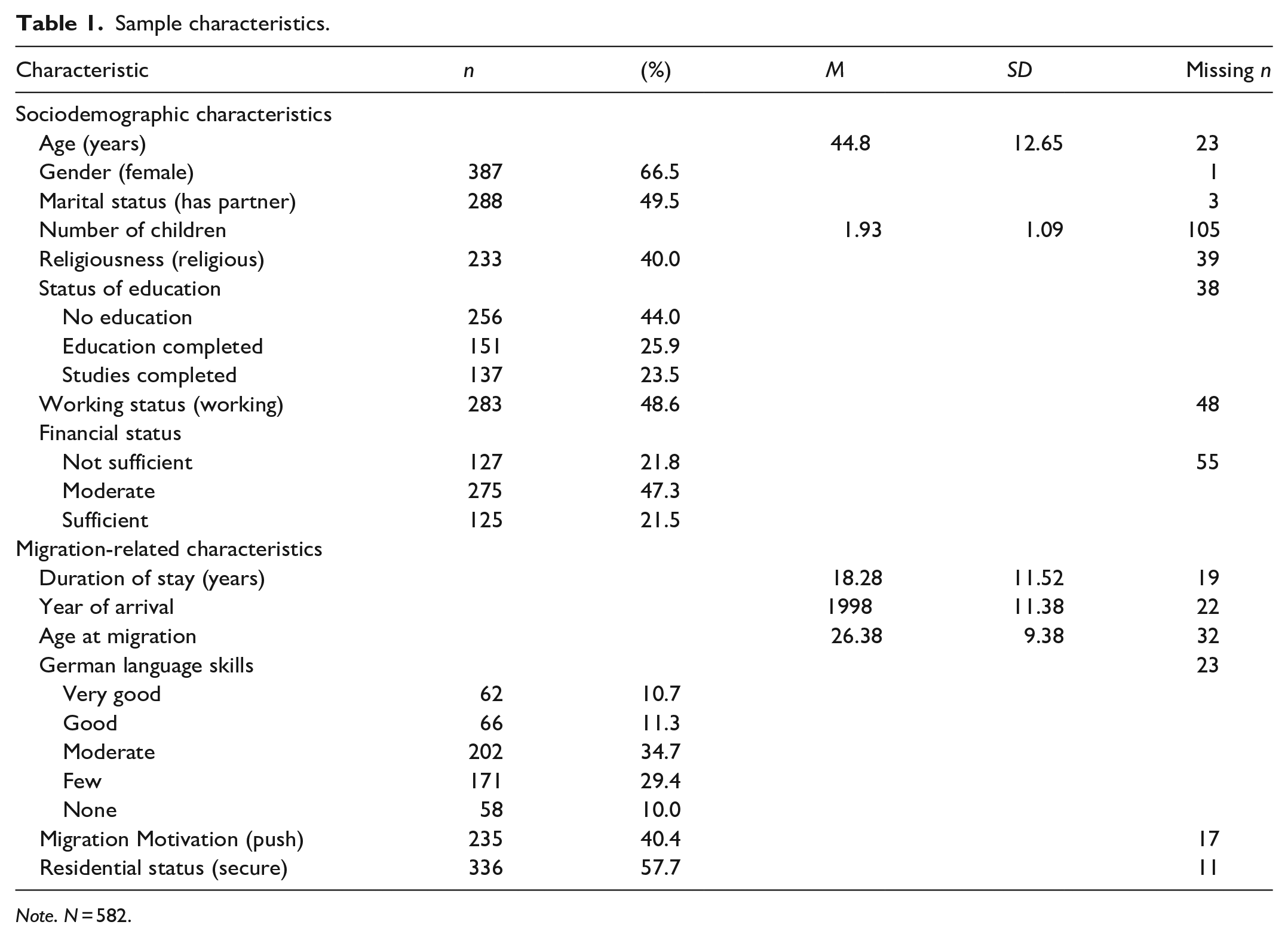
Note. N = 582.
Depressive symptoms scores, acculturation scores, and acculturation styles
The average PHQ-9 score was 7.99 out of 27 (SD = 7.58). For the SMAS, the mean score of DSI was 34.52 out of 56 (SD = 8.44), and for ESI, 53.03 out of 64 (SD = 6.11). Sample distributions of DSI and ESI and their classifications into acculturation strategies are illustrated in Figure 1. Regarding acculturation strategies, 422 participants (72.5%) were classified with an integration, 156 participants (26.8%) with a separation, 3 participants (0.5%) with an assimilation, and 1 participant (0.2%) with a marginalization strategy.
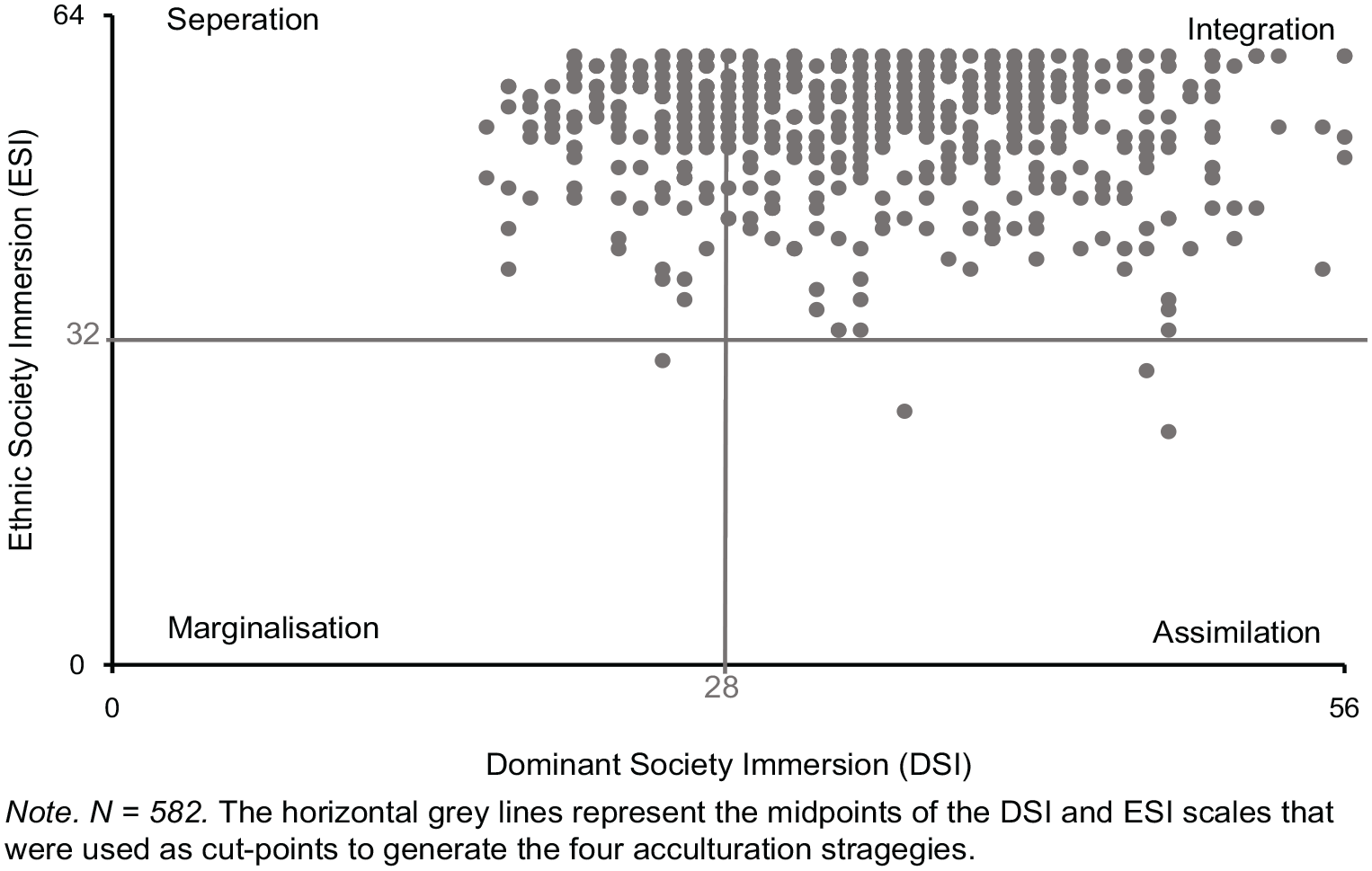
Sample distribution of the acculturation dimensions and the acculturation styles.
Factors impacting DSI
The R² for the overall model was .387 (adjusted R² = .366), indicative of a high goodness-of-fit (Cohen, 1988). Out of the eleven initially considered candidate variables, the multiple regression model yielded a total of four significant predictors: PHQ-9 (β = −.173, p < .001), male gender (β = .086, p = .045), education (βeducation completed = .101, p = .028; (βstudies completed = .110, p = .025), German language skills (β = −.443, p < .001) (Table 2).
Multiple regression model for factors impacting DSI.
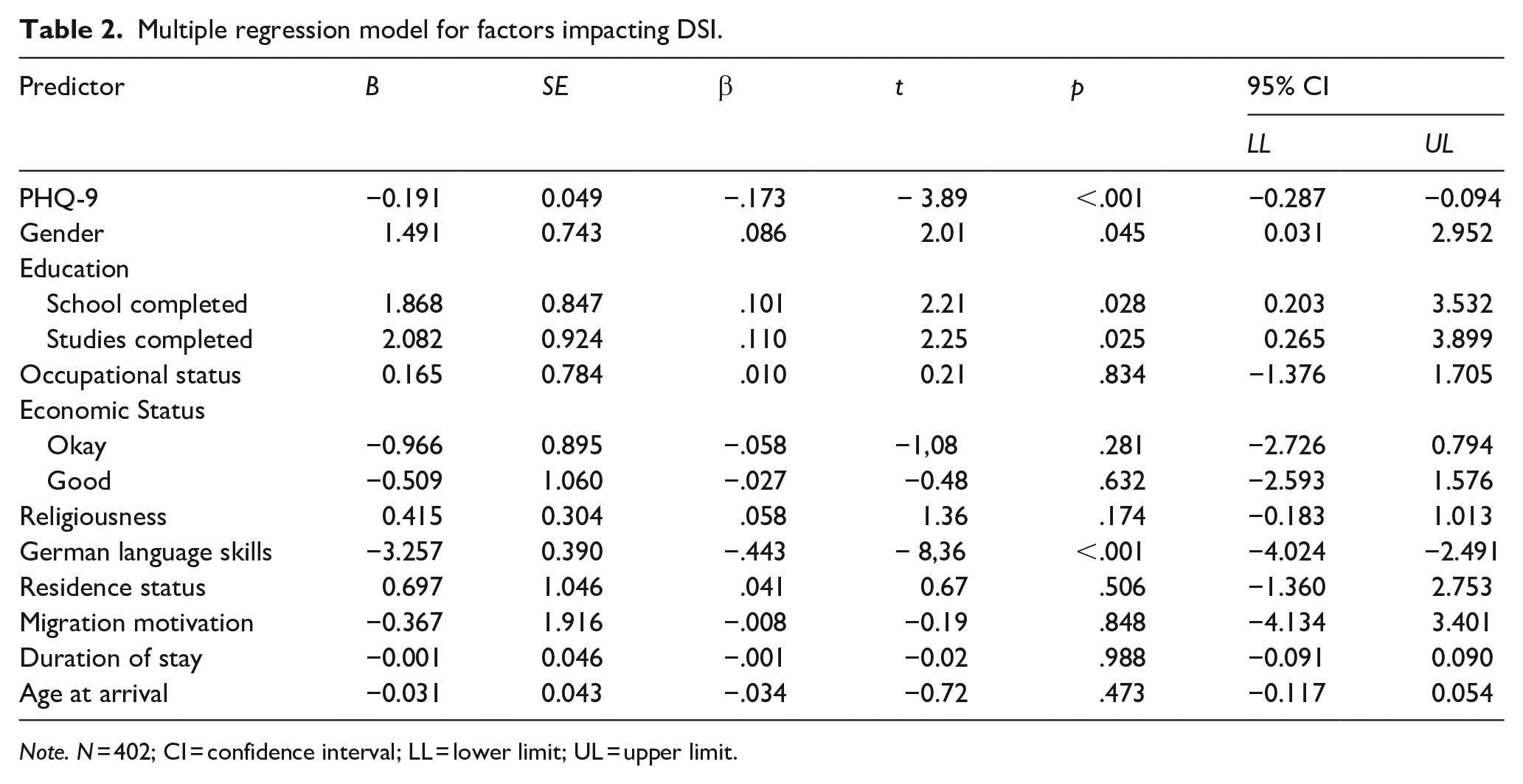
Note. N = 402; CI = confidence interval; LL = lower limit; UL = upper limit.
Factors impacting ESI
The R² for the overall model was .115 (adjusted R² = .085), indicative of a moderate to small goodness-of-fit (Cohen, 1988). Out of 11 initially considered variables, the multiple regression model yielded in total three significant predictors: PHQ-9 (β = −.225, p < .001), German language skills (β = .207, p < .001), age at arrival (β = .153, p = .008) (Table 3).
Multiple regression model for factors impacting ESI.
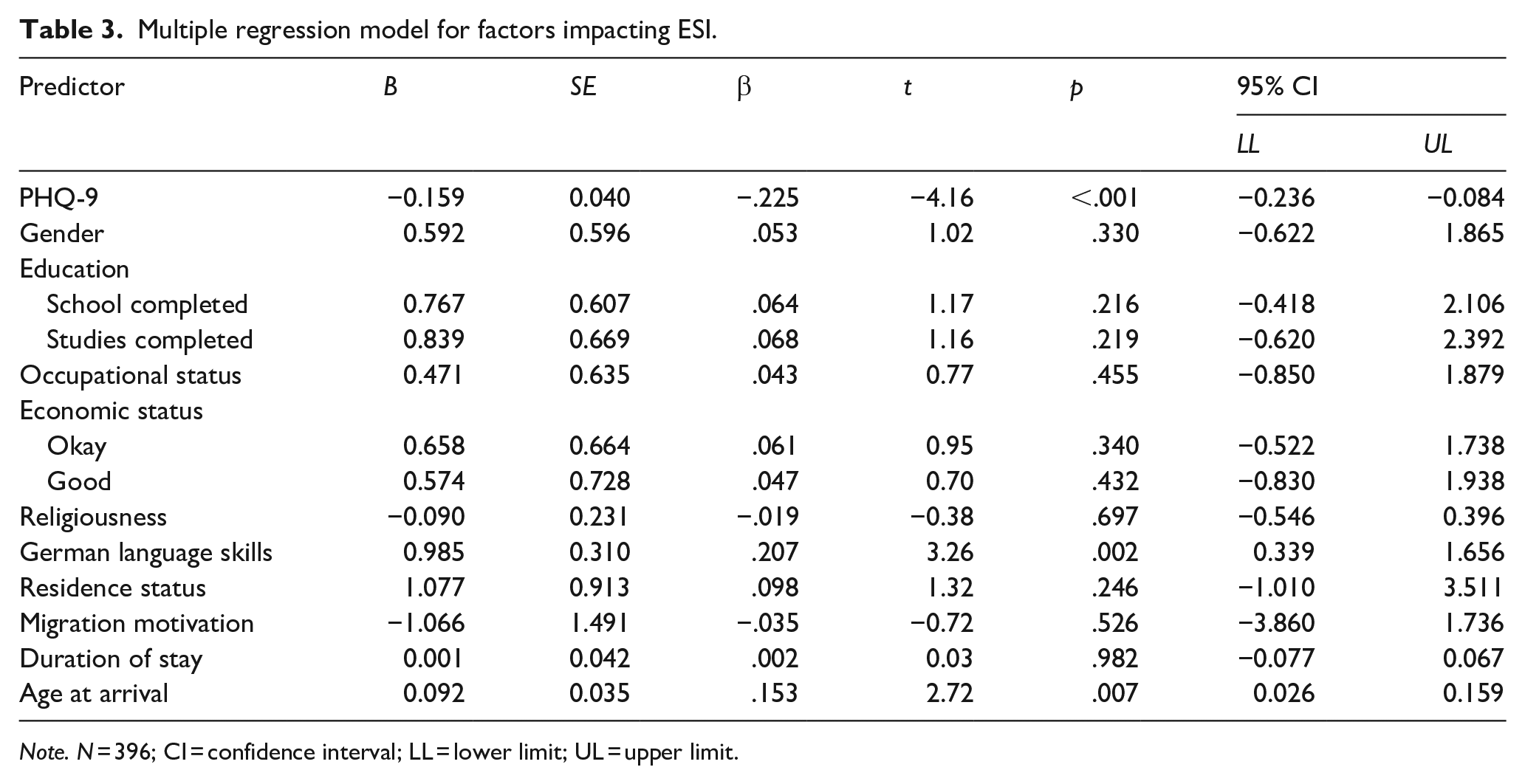
Note. N = 396; CI = confidence interval; LL = lower limit; UL = upper limit.
Relationship between DSI and ESI
Consistent with H1, ESI and DSI had no significant correlation, r = −.054, p = .191.
Relationship between DSI, ESI, and depressive symptoms
Consistent with H2 predicting that DSI and ESI are negatively associated with depressive symptoms, there were significant negative correlations between the two acculturation dimensions and the PHQ-9 score (DSI r = −.317, p < .001; ESI= r = −.208, p < .001). The correlations’ size did not differ significantly (Pearson and Filon’s z = −1.830; p = .067).
Acculturation strategies and depressive symptoms
Acculturation strategies were split into two categories: integration (N = 422, M = 6.75, SD = 7.06) and the other three acculturation strategies (separation, assimilation, and marginalization; n = 160, M = 11.26, SD = 7.96). The level of depressive symptoms differed statistically significantly for the different acculturation strategies, Welch’s F(1,259.33) = 39.68, p < .001, η² = .07, supporting H3 predicting that out of the four acculturation strategies integration is linked to the lowest depressive symptoms scores.
Discussion
This is the first study to examine factors impacting acculturation broadly and to investigate further the relationship between depressive symptoms and acculturation among Vietnamese migrants in a large, not exclusively clinical, sample in Germany. Regarding acculturation strategies, the integration strategy was predominant in almost three-quarters of the sample; about a quarter was classified with a separation strategy, whereas a marginalization strategy and assimilation strategy were virtually non-existent. As predictive factors for DSI lower depressive symptoms scores, male gender, higher education, and better German language skills were found significant. In contrast, occupational status, age at arrival, religiousness, residence status, economic status, migration motivation, and duration of stay were non-significant. For ESI, lower depressive symptoms scores, lower German language skills, and older age at arrival were significant. Finally, compared to the three other acculturation strategies, integration was linked to the lowest depressive symptoms severity.
More in detail, the finding of lower depressive symptoms scores, higher education, and better German language skills predict DSI support prior findings of studies reviewed by Choy et al. (2021) concluding that mental health conditions, low education status and poor language skills negatively impact DSI. Sharing a common language is essential to communicate with locals and immersing into their culture (Dow, 2011; Schwartz et al., 2010), reflected in our data as language skills were the most impactful predictor for DSI. Education might contribute to improved adaptation because problem-resolution skills and knowledge about different cultures are usually acquired through formal education (Berry, 2006). Also, education in the host country might bring migrants into contact with the dominant culture through teaching content and peers. The importance of the opportunity to interact with members from the dominant society to increase DSI is also highlighted by our finding that females were less immersed in the dominant society, while both genders were equally immersed in their ethnic society. This gender difference is in line with prior research summarized by Berry (2006). However, more recent research does not find gender differences (Choy et al., 2021; Park et al., 2020) or points out that women would be more oriented toward the dominant society (Lui, 2015). A potential explanation for these inconsistencies can be found in a meta-analysis on the reliability of acculturation scores by Huynh et al. (2009). The meta-analysis finds no substantial gender differences in internal consistency for ESI scores but lower internal consistency for DSI scores in samples with more women (Huynh et al., 2009). The authors argue that, for men, all the items measure DSI. In contrast, for women, items measure DSI and the opportunity to interact with the dominant society outside the home. Prior research shows a traditional division of gender roles in Vietnamese families in Vietnam, as well as in Vietnamese migrant families, where women, in general, are responsible for most domestic activities and care-related work (Do et al., 2023; Knodel et al., 2005; Nghe et al., 2003; Nguyen et al., 2021). Thus, it seems plausible that, while both genders stay equally embedded into their ethnic society, women might have fewer opportunities to immerse into the dominant society because they are busy with domestic activities and care work (in our sample, 64% of men were working, compared to only 47% of women). This is particularly interesting, as research on newly arrived female refugees in Germany shows that women have a positive attitude toward DSI as they see migration as an opportunity to assume more emancipated roles in education, employment and romantic relationships (Walther et al., 2021), while at the same time being less likely to attend integration courses or being employed than their male peers (Walther et al., 2020). Qualitative research revealed that female Vietnamese migrants in Germany report distress because of a lack of support from their partners in household tasks (Nguyen et al., 2021). Thus, it seems possible that although women are motivated to immerse themselves into the dominant society, they need more opportunities to overcome traditional role divisions. The result that participants who came to Germany at an older age were more rooted in the Vietnamese culture can be explained by them having more time to immerse into the Vietnamese culture during their upbringing (Chung et al., 2000).
Notably, in our sample, factors usually expected to impact acculturation, such as religiousness, migration motivation, duration of stay and occupational, economic, and residence status, were non-significant. By determining the relevance of such factors, this study helps to design better targeted and, thus, more efficient migration and mental health policies. In earlier conceptions as well as in migration and integration policies, acculturation used to be seen as unidimensional, assuming that aspects and practices of the majority culture are mainly adopted by giving up practices of their heritage culture (Berry, 2019; Schwartz et al., 2010). Our finding that DSI and ESI were statistically independent challenges this unidimensional approach and supports the bidimensional approach. Consistent with previous empirical evidence (Berry, 2019; Choy et al., 2021; Schwartz et al., 2010), our findings show that an integration strategy is linked to the lowest depressive symptoms scores. This suggests that the coexistence of ESI and DSI in an individual is not only possible but beneficial. Correspondingly, our finding that higher levels of ESI and DSI were correlated to lower depressive symptoms scores is in line with a meta-analysis conducted by Gupta et al. (2013) examining the relationship between acculturation and depression among Asian US-Americans. These results suggest that immersion in any culture can serve as a resource against adverse mental health outcomes and is primarily supported by previous research (Nguyen et al., 2017; Schwartz et al., 2010). Cultural immersion provides an individual with a sense of belonging. Studies have demonstrated that belonging, defined as an emotionally charged position in social structure, experienced through identification, embeddedness, connectedness, and attachments (Pfaff-Czarnecka, 2013), represents an essential factor for the well-being of migrants in Germany (Fuchs et al., 2021; Nguyen et al., 2021). Effectively, Schwartz et al. (2010) argue that it is unlikely for a person to develop a cultural identity without using their ethnic or dominant cultural context and associated practices. The virtual nonexistence of the marginalization strategy in our study, which was also reported by other studies using clustering methods (Rudmin, 2003; Schwartz et al., 2010), supports this reasoning.
Nevertheless, many studies found evidence for adapting all four acculturation strategies (Berry, 2019; Schwartz et al., 2010). However, this is not only due to actual differences between the samples but also because of heterogeneous methods in which the four acculturation strategies are classified (Berry, 2019; Schwartz et al., 2010). Classifying practices that favor assigning an equal number of participants to each acculturation strategy could lead to overestimating variation in acculturation strategies. This overestimation of variation could lead to the oversimplified impression that an acculturation strategy would result from specific individual choices and neglect the importance of demographic and contextual factors (Bierwiaczonek & Kunst, 2021; Rudmin, 2003; Schwartz et al., 2010). By identifying relevant factors in the acculturation process, such as language fluency, education, age, and gender, this study could help to find more nuanced approaches to efficient policy making.
Practical implications include empowering migrants by empowering women or funding education and language services to effectively support them in developing pro-integration attitudes. Simultaneously, mental health services should be targeted at segregated people, for example, by extending services in their mother tongue. The importance of culturally sensitive treatment for first-generation migrants is further highlighted by the overall high ESI, as found in our sample. Meta-analyses and reviews have shown that culturally adapted treatments are not only more efficient for migrants, but also that acculturation plays a crucial mediating role in the therapeutic process (Kalibatseva & Leong, 2011, 2014; Leong & Lee, 2006). To further improve culturally sensitive treatment options, our findings suggest that cultural immersion can protect against adverse health outcomes.
Limitations
Our study results must be interpreted considering several limitations. First, causal implications cannot be drawn due to the cross-sectional study design. Besides, more depressed individuals might perceive their cultural immersion more negatively than non-depressed individuals, also known as negative attention bias (Baert et al., 2010). It should be further mentioned that depression is usually conceptualized from a Western perspective but may manifest differently in other cultures (Gupta et al., 2013; Ryder et al., 2008). Research has shown a tendency in Asians to underreport culturally stigmatized symptoms of mental health problems. However, using self-report questionnaires may be less prone to bias for social-desirable answer patterns because of perceived anonymity. Second, measuring acculturation strategies comes with specific challenges. As mentioned before, the cut-point between high and low society immersion is arbitrary, which complicates comparisons across studies (Schwartz et al., 2010). Furthermore, the SMAS, like most acculturation scales, focuses on behavioral aspects, especially language usage. Bearing that depression impairs proactive behaviors, the content measured by the SMAS might partly be confounded with the predictors of language skills and depressiveness. Furthermore, while our study provides a good-to-moderate level of fit for our cultural immersion models, it is important to acknowledge that a significant portion of variance remains unaccounted for in our regressions. This raises the question of other potential factors that could impact acculturation. Despite extensively examining a diverse range of individual factors influencing acculturation, it is necessary to recognize that we did not include additional contextual factors, such as societal attitudes or discrimination, which have been well-established as influential factors affecting both acculturation (Berry, 2019; Liebkind, 2006) and mental health outcomes (Berry, 2006; Gleeson et al., 2020; Jannesari et al., 2020). Regarding generalizability, it should be kept in mind that our sample consisted of first-generation migrants that spent, on average, the first 26 years of their life in their country of origin. ESI would likely be lower in second-generation migrants. Moreover, the sample might be slightly biased as it was mainly recruited in Berlin, where different Vietnamese communities could be more likely to emerge and influence the acculturation process because of its size and density. It is important to recognize that implementing a clinical utilization and non-utilization recruitment strategy introduced heterogeneity in the sample, particularly in terms of variations in depressive symptoms, among the two recruitment pathways. The decision to include clinical utilization as well as non-utilization participants was made to obtain a more naturalistic sample, considering previous research that postulated an under or delayed utilization of professional healthcare services among Vietnamese migrants in Germany (Ta et al., 2014; Wolf et al., 2020). Nevertheless, the possibility of biases because of the two-pathway recruitment strategy cannot be entirely ruled out. Nevertheless, this heterogeneity introduces the possibility of bias in the findings.
Future research
In line with other authors (Berry, 2019; Bornstein, 2017; Guarnaccia & Hausmann-Stabile, 2016; Mesquita et al., 2019; Schwartz et al., 2010), we argue that the bidimensional model of acculturation is too narrow and static and more flexible acculturation concepts and measures have to be applied. Instead of focusing on whether an individual immerses in a culture, how individuals integrate two (or more) cultures should be explored. Not only depressive symptoms but also acculturation strategies change over time and contexts and should be examined with longitudinal studies and more dimensions of acculturation such as knowledge, values and identity (Arends-Toth & van de Vijver, 2006; Berry, 2019; Meca et al., 2018; Ward & Geeraert, 2016). In future systematic investigations, it is essential to consider contextual factors such as the perceived and objective societal attitudes of the majority group toward a minority group. This can be achieved with cross-cultural designs that encompass different dominant and ethnic cultures (Berry, 2019). Additionally, incorporating mixed-method designs can further enhance the contextualization of results (Nguyen et al., 2021). By integrating these approaches, a more comprehensive understanding of the influences on acculturation can be attained.
Conclusion
In conclusion, the current study identified crucial factors in the acculturation process, such as depressive symptoms, language skills, education, gender, and age at arrival in a large, not exclusively clinical, Vietnamese migrant sample in Germany. Our findings emphasize that immersion into both the dominant and the ethnic culture plays an essential supportive role in the mental health of migrants.
Footnotes
Authors’ note
We have no known conflict of interest to potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted in part within the subproject A02 of the CRC 1171 ‘Affective Societies – Dynamics of Coexistence in Mobile Worlds’ granted by the German Research Foundation (DFG – Deutsche Forschungsgemeinschaft).
Data availability
Data is available from the corresponding and last author upon reasonable request.