
Abstract
Background:
Caregivers have a key role in providing social and practical support for individuals with bipolar disorder. As such, their perspectives are uniquely important when collaborative decisions are made on management priorities and potential treatment options.
Aims:
This study aims to identify common concerns that caregivers have in the management of an individual with a bipolar disorder.
Method:
111 caregivers were recruited from online advertisements and social media support groups. They completed a questionnaire that obtained demographic and clinical feature details, in addition to whether a series of generic and phase-specific (i.e. depressive or hypo/manic) management concerns reflected their experiences of caregiving.
Results:
Concerns about work capacity and family impacts were almost ubiquitous, as were general feelings of ineffectiveness and irritation. Depressive phases were more likely to elicit fears of suicide by caregivers, while during hypo/manic phases caregivers were more likely to be angered, have concerns for their own safety, call emergency services or to take safety precautions. There were no differences between bipolar subtypes with regards to concerns during depressive phases, but concerns around safety, reputational damage and risky behaviours were more likely in relation to those experiencing bipolar I manic phases compared to bipolar II hypomanic phases.
Conclusions:
The concerns identified by caregivers in this paper are consistent with clinical expectations, with concerns regarding insularity and externalisation being prominent for depression and hypo/mania respectively. Not all of these caregivers’ concerns would necessarily be communicated in a healthcare setting, highlighting the need for an embracive approach to improve management outcomes. Additionally, caregivers’ emphasis on their distinctive altruistic concerns highlights their commitment to care despite the challenges, and thus further highlights the potential for clinicians to implement a more proactive role for them in patient care.
Introduction
The bipolar disorders are severe psychiatric conditions, estimated to have a combined lifetime prevalence of up to 4% (Kessler et al., 2005). Social connections are important in aiding individuals with a bipolar disorder in living with and managing their condition (Owen et al., 2016). Caregivers therefore hold an important and central role; indeed, by virtue of their personal connection to the care recipient (CR), caregivers are often the first individuals to identify symptoms (often before the CR themselves). Their observations and insights into the behaviours and practical consequences of their CR’s bipolar disorder are commonly central in assisting clinician management and even nuanced treatment options.
While being a caregiver can be rewarding, it is commonly demanding. However, the concept of ‘caregiver burden’ is often neglected by clinicians (Adelman et al., 2014). One of the difficulties in conducting research in this area is that there is no accepted unanimous definition of caregiver burden. Multiple definitions ultimately lead to issues with generalising results and hindering the ability of research to influence health decisions and policy (Bastawrous, 2013). However, it is generally agreed that caregiver burden is multidimensional, involving stressors and impairments related to physical, emotional, financial and social factors (George & Gwyther, 1986; Zarit et al., 1986). This poses a problem for caregiver burden measurement. Multiple measures exist that address different aspects of caregiver burden, but definitional inconsistencies are often compounded by impracticalities (i.e. their insensitivity to the limited time and finances of clinicians) which make their practical usage limited (Deeken et al., 2003). Meanwhile, psychometric approaches to caregiver burden may be inherently limited anyway, given their lack of ability to account for contextual factors that provide a fuller account of the caregiver experience (Bastawrous, 2013). Clearly, these conceptual issues highlight the importance of further research into caregivers. And this is even before considering the obvious health impacts, namely the impact of caregiving on the caregiver themselves (e.g. physical health, sleep deprivation, depression/anxiety, suicide) (Adelman et al., 2014) and the fact that high caregiver burden increases the likelihood of their care recipient’s needs not being met (Siegel et al., 1991). Through sensitivity to caregiver burden, we can potentially identify what assistance might be provided to caregivers and also what treatment outcomes to target.
Multiple studies have detailed the demands and burden faced by those caring for an individual with a psychiatric disorder (Baronet, 1999; Schulze & Rössler, 2005), while caregiver burden has been suggested to be greater for psychiatric conditions than for other chronic medical conditions (Ampalam et al., 2012). For bipolar disorder specifically, broad factors such as symptom severity, stigma and a lack of support have been specifically linked to greater caregiver burden (van der Voort et al., 2007). However, the impact of specific and differing bipolar symptoms remains under-researched. Even less research exists comparing any differential impact of bipolar I (BP-I) and bipolar-II (BP-II) disorder subtypes on caregivers, though one study by Arciszewska et al. (2015) of caregiver spouses identified the greater burden posed during BP-I manic phases (compared to depressive phases) and BP-II depressive phases (compared to hypomanic phases).
Individuals with a bipolar disorder appear more likely to be concerned by their depressive phase symptoms, as evident in research showing their bias towards depressive symptom reporting (Phillips & Kupfer, 2013) and treatment seeking during depressive episodes (Bowden, 2005). By contrast, caregivers appear (from clinical observation) to have greater concerns about behaviours and risks during hypomanic or manic (hereafter referred to as (hypo)/manic) phases. In addition, there are also reports that a greater proportion of caregivers find manic phases to be more distressing to them than depressive ones (Dore & Romans, 2001), and that caregivers are required to provide a considerably greater interventional role during manic as against depressive episodes (Ogilvie et al., 2005), where they may judge the need for intervention and even hospitalisation as acute priorities.
On a theoretical basis it might be hypothesised that caregivers would judge depressive and hypo/manic phases as providing quite contrasting risks. Concerns during the individual’s depressed phase might be expected to centre around issues such as an inability to function and suicide risk (Mitchell & Malhi, 2004), while concerns during hypo/manic phases might be expected to centre more around risks of disinhibition, financial recklessness or aggression (Beentjes et al., 2012).
The current study therefore aimed to investigate and identify the salient concerns and foci that caregivers of individuals with a bipolar disorder observe and face in managing their CR’s condition. In doing so, we also seek to determine whether caregivers have more concerns about their CR during hypo/manic or depressive phases, and whether the principal bipolar subtypes (BP-I and BP-II) generate differential caregiver concerns, as might be anticipated when those with a BP-I condition are more likely to have psychotic manic episodes.
Methods
The study involved an online survey hosted through Qualtrics XM (Qualtrics, Provo, Utah, USA). Participants were recruited through advertisements containing a link to the survey that was posted in two locations. The first was a large social media support group consisting of predominantly American bipolar disorder caregivers and CRs, while the second was the website and email newsletters of the Black Dog Institute in Sydney, Australia. Individuals were eligible to participate in the study if they were a fluent English-speaking adult (aged 18 or over) and a caregiver of an adult with a bipolar disorder (either BP-I or BP-II). The advertisements were active for 7 months, and after recruitment had ceased, a total of 111 caregivers had returned questionnaires.
After obtaining consent, the survey asked for some basic caregiver and CR demographic details, along with their CR’s diagnostic subtype. The main component of the survey consisted of a series of questions concerning the extent to which the caregivers were concerned about certain behaviours and consequences for themselves and their CR, either generally or during their depressive or hypo/manic phases at their worst (referred to as the depressive ‘nadir’ and hypo/manic ‘peak’ respectively). Another outcome of interest involved assessing serious strategies that might need to be invoked in caring for the CR, such as any need to make a crisis call (e.g. call an ambulance, call the police) and to take safety precautions. Caregivers were therefore asked to indicate whether they had performed any of these actions.
Each of the concerns were rated as either 0 (not at all), 1 (somewhat) or 2 (a lot) in terms of impact, but items were binary formatted for analysis to capture absence versus presence (0 = no, 1/2 = yes). Response frequencies for each of the items were analysed, and the presence of any diagnostic differences in any of the individual symptoms and concerns were quantified by risk ratios. We also reported the prevalence of three practical consequences: making police calls, making other crisis calls and taking safety precautions, and analysed for any differences in response patterns between mood states by using McNemar tests. All analyses were conducted in R (version 4.2.0).
Results
Cohort characteristics
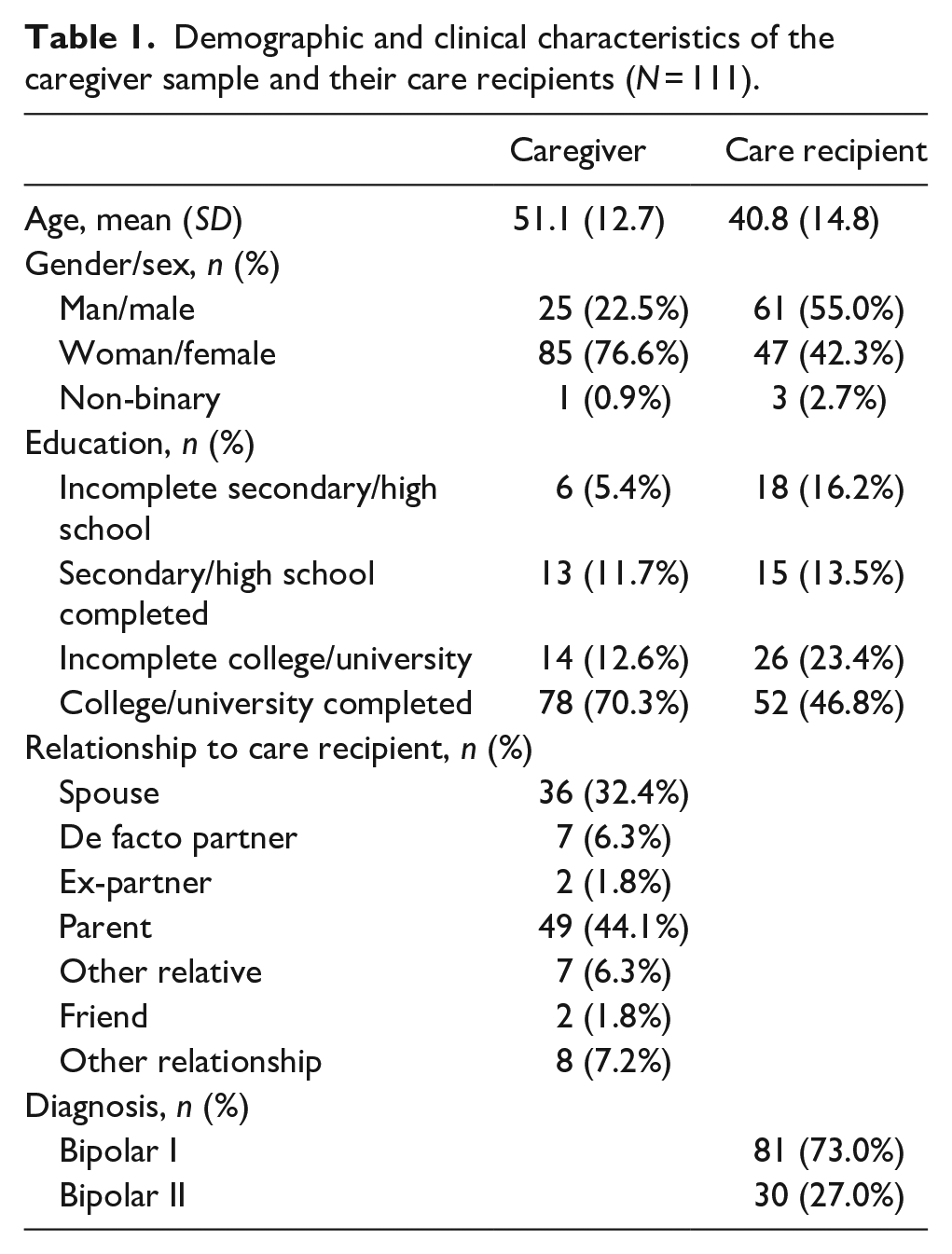
Table 1 provides a breakdown of the demographic characteristics of the sample. In short, most of the caregivers were female, tertiary educated and were either a parent or spouse of their CR. Of the CRs, most had a bipolar I disorder (81/111, 73%) and had graduated high school (93/111, 83.8%). There were also more male (61/111, 55.0%) than female CRs (47/111, 42.3%) in the sample.
Demographic and clinical characteristics of the caregiver sample and their care recipients (N = 111).
General management concerns
Table 2 lists the shared or differential caregiver concerns across both depressive and hypo/manic episodes, while Table 3 examines for any impact of bipolar subtype on caregiver concerns. As quantified in Table 2, virtually all caregivers expressed some degree of general worry about their CR during both depressive and hypo/manic episodes (both 108/111, 97.3%), and this was the most highly affirmed concern. Other dominating concerns during both depressive and hypo/manic episodes (respectively) included worrying about their CR’s future and work capacity (93/111, 83.8%; 94/111, 84.7%), worrying about their CR’s safety (104/111, 93.7%; 97/111, 87.4%) and concern about the CR’s impact on the family (101/111, 91.0%; 94/111, 84.7%), while there were also high rates of the caregiver feeling helpless (103/111, 92.8%; 95/111, 85.6%), ineffective (101/111, 91.0%; 97/111, 87.4%), irritated (83/111, 74.8%; 92/111, 82.9%) and frustrated (94/111, 84.7%; 96/111, 86.5%).
Response rates to general management concern questions for the whole sample and their differences across depressive and hypo/manic phases (N = 111).
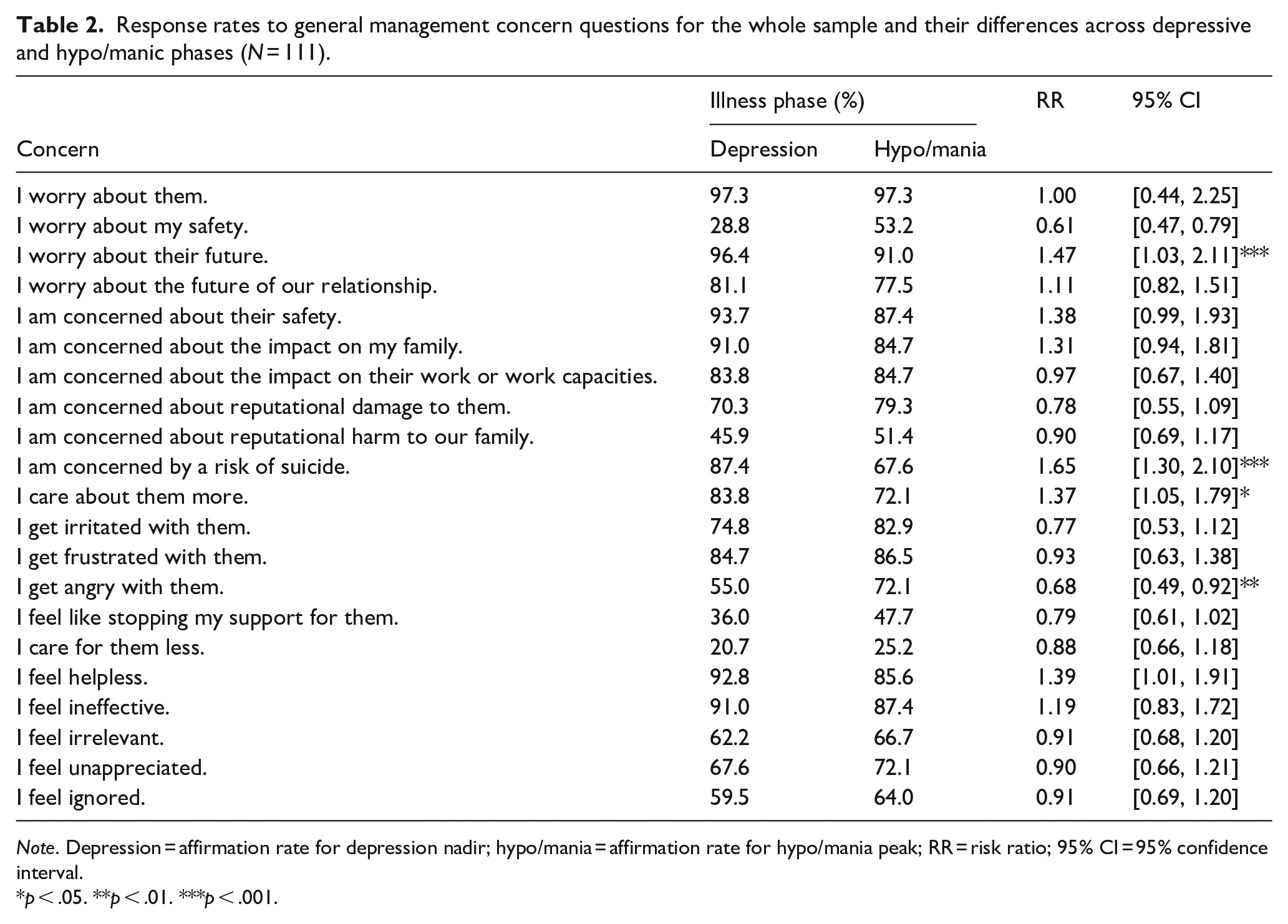
Note. Depression = affirmation rate for depression nadir; hypo/mania = affirmation rate for hypo/mania peak; RR = risk ratio; 95% CI = 95% confidence interval.
p < .05. **p < .01. ***p < .001.
Diagnostic differences in the response rates to general management concern questions in bipolar I and bipolar II samples during separate illness phases (N = 111).
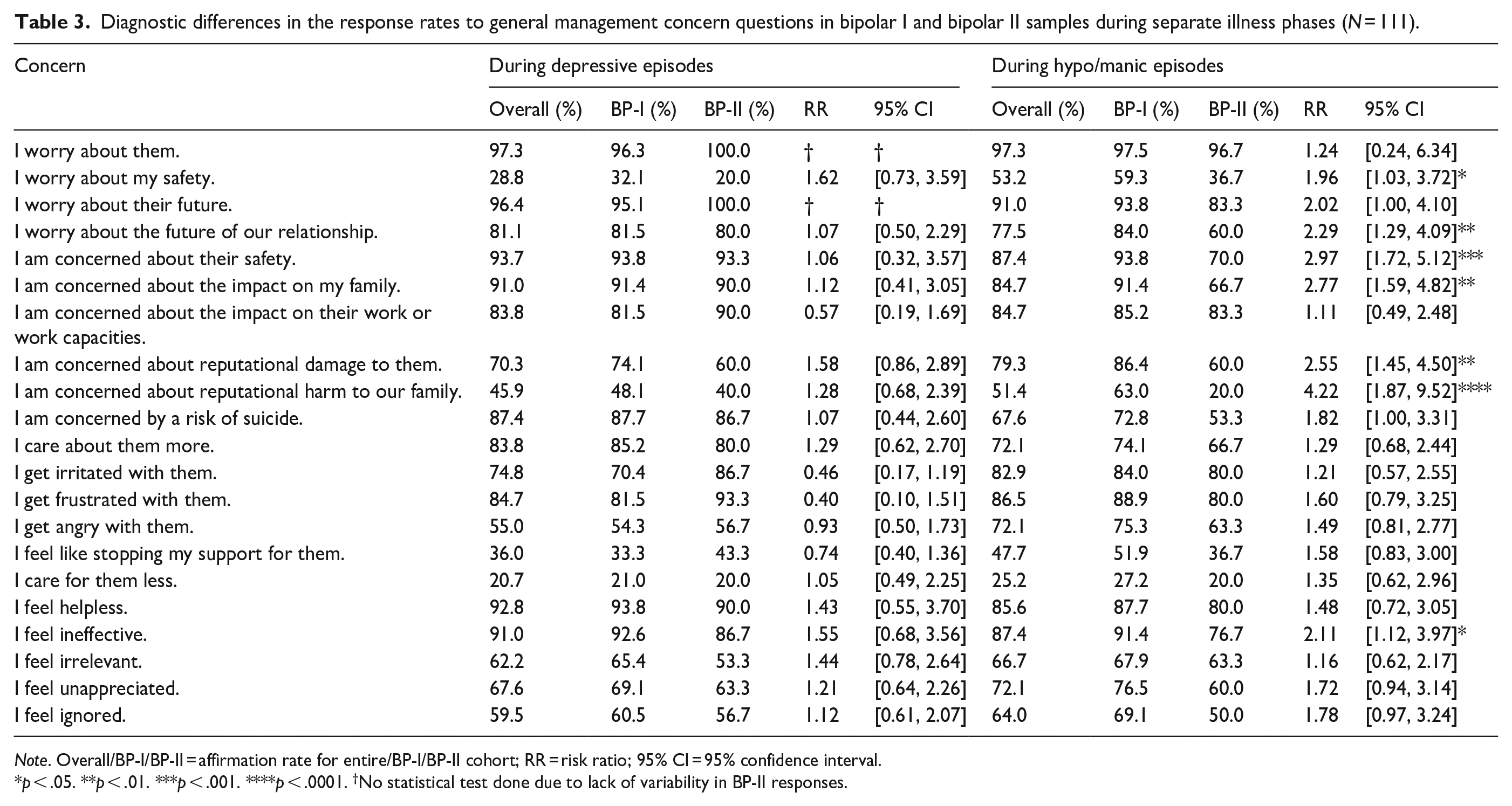
Note. Overall/BP-I/BP-II = affirmation rate for entire/BP-I/BP-II cohort; RR = risk ratio; 95% CI = 95% confidence interval.
p < .05. **p < .01. ***p < .001. ****p < .0001. †No statistical test done due to lack of variability in BP-II responses.
Table 3 extends these analyses by examining for any differential impact of bipolar subtype. During depressed phases, diagnostic subtype appeared to have no distinct impact in that the prevalence rates for the differing concerns and responses were generally comparable. However, during hypo/manic episodes, caregivers of BP-I CR’s (compared to caregivers of BP-II CRs) were more likely to be concerned about their CR’s safety (RR = 2.97, 95% CI [1.72, 5.12]), their future (RR = 2.02, [1.00, 4.10]), the impact of their condition on the family (RR = 2.77, [1.59, 4.82]) and reputational damage to the CR (RR = 2.55, [1.45, 4.50]), while they were also more likely to feel ineffective (RR = 2.11, [1.12, 3.97]).
Acute management concerns
Table 4 reports prevalence data for concerns about common symptoms experienced by those with a bipolar disorder during differing depressive and hypo/manic phases. Concerns about sleep disturbance were the most highly nominated caregiver concern across both depressive (104/111, 93.7%) and hypo/manic phases (102/111, 91.9%). During depressive nadir times, the caregiver was most concerned about the CR lying in bed (98/111, 88.3%), not socialising (94/111, 84.7%) or interacting (92/111, 82.9%), and being suicidal (93/111, 83.8%). During peak hypo/mania, CR irritability was an almost ubiquitous concern (104/111, 93.7%). Other dominating concerns during such periods were the CR not sleeping (102/111, 91.9%), being grandiose (98/111, 88.3%), ignoring rules (89/111, 80.2%), being non-compliant in taking their medication (92/111, 82.9%), spending money excessively (92/111, 82.9%) and being rude and disrespectful (89/111, 80.2%). Bipolar subtype did not appear to impact on concern rates during depressive phases. However, during hypo/manic peaks, caregivers of CRs with bipolar I were more likely than caregivers of CRs with bipolar II to be concerned about their CR’s lack of sleep (RR = 2.27, 95% CI [1.15, 4.46]), alcohol intake (RR = 1.85, [1.00, 3.42]), use of illicit substances (RR = 1.90, [1.01, 3.55]), verbal abuse (RR = 2.16, [1.20, 3.88]), physical violence (RR = 2.35, [1.21, 4.56]) and sexually indiscrete behaviour (RR = 1.85, [1.01, 3.36]).
Response rates to concerns when individuals’ depressive and hypo/manic episodes are at their most severe, both for the whole sample and in those with separate bipolar subtypes (N = 111).
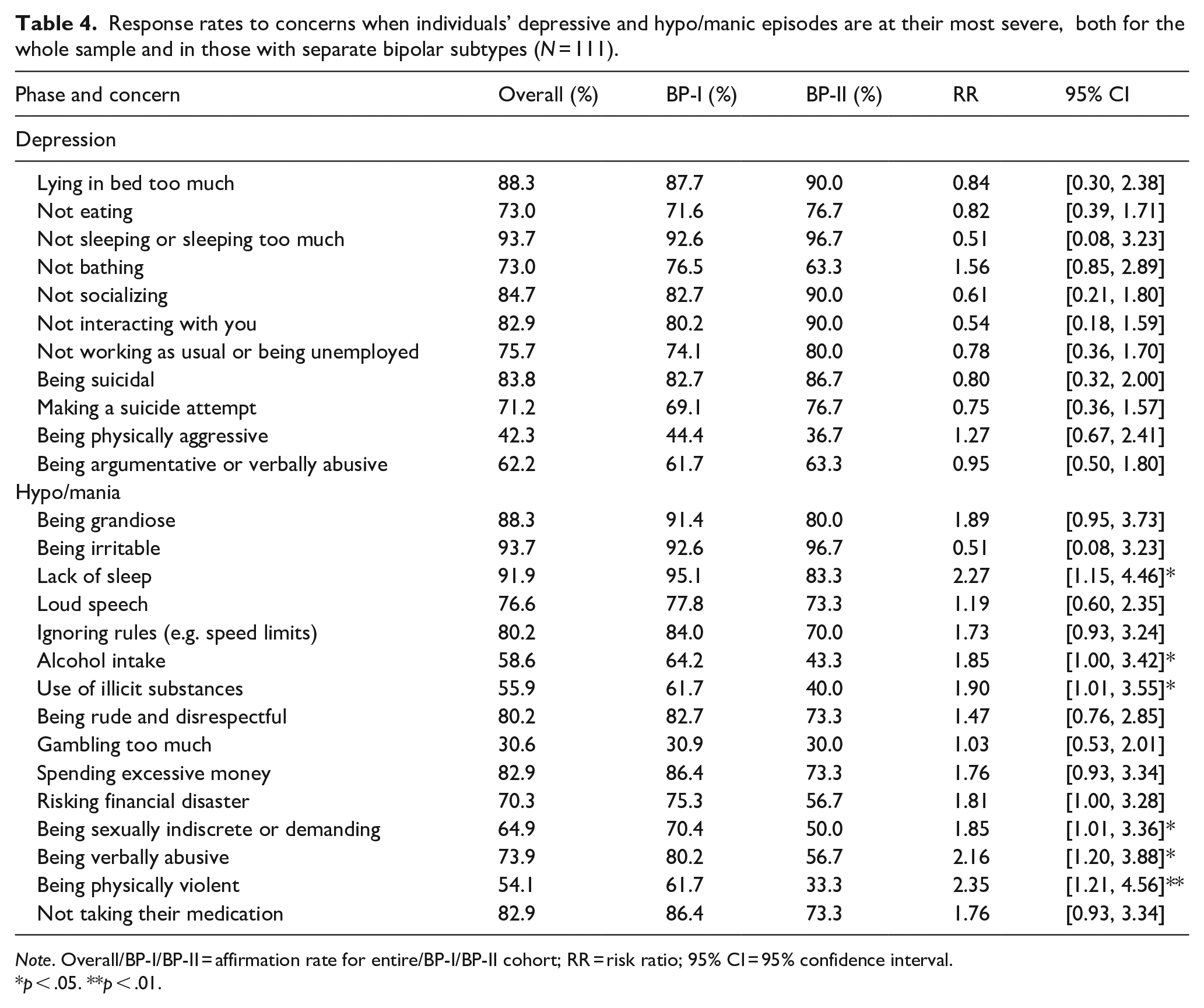
Note. Overall/BP-I/BP-II = affirmation rate for entire/BP-I/BP-II cohort; RR = risk ratio; 95% CI = 95% confidence interval.
p < .05. **p < .01.
Practical consequences
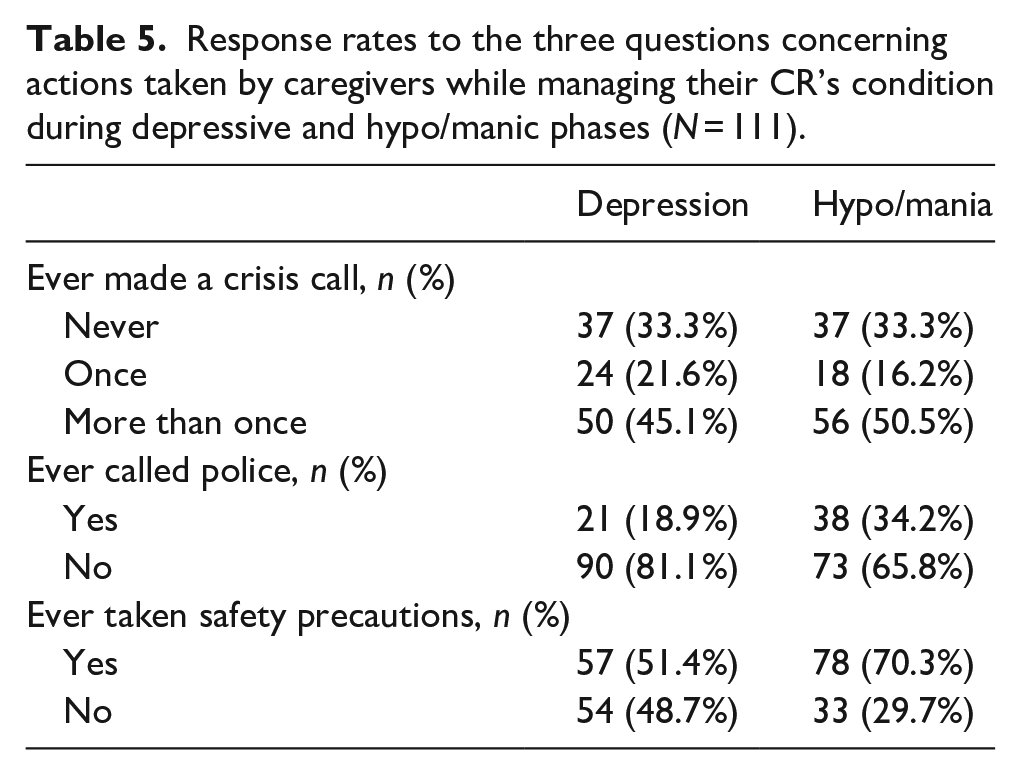
Table 5 provides prevalence data on caregiver response patterns for three practical consequences for those in depressive and hypo/manic phases. Rates for making a crisis call (i.e. never vs. at least once) did not appear to differ across depressive and hypo/manic phases (χ2 = 0, p = 1). However, taking safety precautions (χ2 = 10.26, p = .001) and calling the police (χ2 = 9.32, p = .002) were more likely to occur when CRs were in a hypo/manic as against a depressive state.
Response rates to the three questions concerning actions taken by caregivers while managing their CR’s condition during depressive and hypo/manic phases (N = 111).
Discussion
This study sought to address a key gap in the literature considering bipolar disorder management. The importance of clinicians encouraging caregivers to take a collaborative, proactive role in managing the health conditions of their CRs is a priority (Adelman et al., 2014). However, particularly in the context of bipolar depression and hypo/mania, caregiver perspectives on which management concerns are the most salient and that are consistent with their lived experience are limited.
One key theme that emerged in our study, particularly in relation to caregivers’ general concerns, was that caregivers tend to have selfless (and potentially altruistic) priorities. Caregivers had high rates of ‘caring more’ for their CRs during illness episodes (rates exceeding 70% in both depressed and hypo/manic phases) and very high rates of ‘worrying about’ their CR and ‘worrying about their future (rates exceeding 90% in both illness phases). In both illness phases, caregivers were highly likely to report concerns about their CR’s capacity to work, reputational risk and the future of their shared relationship, as well as concerns about their CR’s safety and risk of suicide, while the most distinctive negative caregiver concerns were the caregiver feeling helpless, ineffective and frustrated. Such findings are consistent with previous observations that caregivers for individuals with bipolar disorder are committed to their role despite the multiple challenges (Dore & Romans, 2001). Meanwhile, the specific concerns of safety, occupational functioning and suicide (among others) align with clinical priorities, which provides some evidence that at least some aspects of standard clinical care are aligned with caregivers’ needs. However, it also provides a point of caution since this CR-centric approach shared by both clinicians’ and caregivers’ risks overlooking the needs of the caregiver themselves. This could be one reason for the lack of focus caregivers receive, as noted and referenced earlier (Adelman et al., 2014).
We also quantified the impact of illness phases, with the data indicating that the caregiver ‘cared’ more for their CR during depressive phases (and rated suicide risk as a higher concern at such times) while being more likely to be angry with their CR and concerned about their own safety during hypo/manic phases. This is consistent with our caregiver actions data, which indicated that, at least in this sample, calling the police and taking more safety precautions were more common during hypo/manic rather than depressive episodes. This somewhat less CR-centric view with regards to hypo/mania is understandable given the externalising behaviours typical of mania, such as aggressiveness and reckless spending, which more directly affect caregivers, and have previously been identified as clear burdens to them (Beentjes et al., 2012). Table 3 data repeated some of those findings in terms of illness phase prevalence rates of caregiver responses and in relation to bipolar subtype. The greater prevalence of these concerns in caregivers of BP-I CRs is not surprising, given the greater severity of mania (BP-I) compared to hypomania (BP-II). The lack of any appreciable differences between bipolar subtypes during depressive phases suggests that the difficulties associated with mania may simply be ‘in-the-moment’ concerns, which may not transfer to their level of care generally. Nevertheless, while clinicians should be sensitive to issues associated with both depression and hypo/mania, for individuals with BP-I, one might be justified in prioritising addressing concerns on managing mania to minimise adverse impacts to the caregiver and ensure they remain engaged with the care process. Indeed, it is even possible that this will have an impact on general caregiver resilience, given previous evidence suggesting that relatives of individuals with bipolar depression experience lower levels of burnout than relatives of individuals with major depression or psychotic disorders (Cuijpers & Stam, 2000).
Table 4 data examined symptoms and consequences frequently experienced and observed in those with a bipolar disorder and during differing phases, with the aim of determining those that were common and examining for differential impact. Of the features investigated, caregivers were most concerned about their CR’s sleep, insularity, lying in bed and not working during depressive episodes. This focus on lethargy is not surprising from a clinical perspective, given the centrality of impairment in social and occupational functioning in defining bipolar disorder (American Psychiatric Association, 2022) and the clear effect that lethargy would have on impairment levels. However, bipolar subtype did not influence rates in reporting for any concern. This finding is consistent with the notion that there are minimal differences between BP-I and BP-II depressive episodes. And indeed, from our list of concerns, the only potential difference we may have expected was a greater concern about suicide in caregivers of individuals with BP-II (Mitchell & Malhi, 2004). No significant difference was observed here, though the affirmation rates for both groups were quite high. Ultimately, the primacy of concerns related to lethargy and suicidal behaviours appear to be quite commonplace amongst all caregivers, thus highlighting the need for clinicians to focus on specific interventions for these concerns during depressive episodes.
During hypo/manic episodes, carers were most concerned about their CRs being irritable, not sleeping, being grandiose, not being compliant with medication, spending excessively and ignoring rules. Caregivers of those with a bipolar I disorder were more likely to report concerns about a number of those ‘acting out’ behaviours, which again is consistent with the greater severity of mania compared to hypomania. More generally, it is notable that despite the increased direct risk to caregivers in hypo/mania the most affirmed concerns were once again CR-centric. Such a finding is important given the limited research into the specific impacts of hypo/mania (Beentjes et al., 2012; Ogilvie et al., 2005). Such data are encouraging, and provides further impetus for increasing the role of caregivers in clinical care.
Clinicians managing those with a bipolar disorder would find many of our findings consistent with their clinical observations, especially in suggesting that depression in those with a bipolar disorder tends to be marked by insularity and retreat from the world phases, while hypo/manic phases are marked by externalising, acting out phases. We had anticipated that caregivers would report distinctly lower rates of caring for their CRs and greater irritation, frustration and anger during hypo/manic phases, but any such differences were relatively minor. In essence, they cared somewhat equally across both illness phases, which might reflect a sample bias (i.e. respondents were generally unremitting carers) or a lack of distinct illness phase impact. The data do provide important information on caregivers’ concerns in looking after someone with a bipolar disorder, with not all nuances considered here necessarily being communicated to the managing clinician or health care service. It may well be useful for carers to fill out embracive checklists of their concerns for consideration by clinicians so that nuanced management plans might be jointly derived, further enhancing the role of caregivers and advancing their contribution to a collaborative management model. Adelman et al. (2014) offers several potential talking points to encourage clinician enquiry into the health of both caregiver and their CRs, and many of the concerns identified in this study could be easily integrated into these discussions.
There are some key study limitations that need to be acknowledged. Firstly, our data are based on questionnaires returned by volunteers. This strategy would almost certainly weight caregiver representation to those who are highly concerned about their CR. Secondly, the total sample number was relatively small and weighted to two geographical regions (with respondents living in the USA or Australia). Thirdly, we accepted the caregiver’s nomination of their person’s bipolar status (as bipolar I or II) at face value and did not seek to validate such judgements. Fourthly, there was distinctly greater percentage of those with a bipolar I as against a bipolar II condition, suggesting our diagnostic analyses may have been underpowered and did not capture all meaningful illness type generated differences at the formal statistical level of significance. Fifthly, our study had a primary focus on broad concerns related to features of the care recipient’s bipolar disorder, and the moderating effects of any variables associated with individual differences in caregivers themselves (e.g. caregiver health, personality variables) are yet to be specifically assessed.
A further limitation is that this study did not consider cultural differences. We did not collect ethnicity data, however, given our recruitment strategies, our participants were likely predominantly from so-called WEIRD societies (white, educated, industrialised, rich, democratic) (Henrich et al., 2010). While this is a neglected area of research (Schulze & Rössler, 2005), it is highly likely that management concerns identified by participants from non-WEIRD societies may differ from our results given the known cultural differences that exist for caregiver burden. As one example, non-Western collectivist cultures place greater emphasis on the family unit, thus potentially meaning that caregivers are more accepting of their situation (Bastawrous, 2013). There are extra challenges in conducting this targeted research that would have made it impractical for the current study: the difficulties that measures have in accounting for context mean that cultural factors may go unnoticed (Bastawrous, 2013), while direct survey-based measures may be hindered by cultural-based stigmas associated with what could be perceived as complaining (Calderón & Tennstedt, 1998). Examining cultural differences would clearly be an important future area of research. Nevertheless, given the lack of previous research into the phase-based management concerns of caregivers, this paper still makes a valuable contribution.
Conclusion
Ultimately, the findings of this study were largely consistent with what might be expected from clinical experience and what is known about caregiver burden more generally. In managing bipolar disorder, caregivers’ concerns about their CR’s safety, lethargy, general functioning and suicidality predictably emerged as key concerns. Meanwhile, the CR-centric nature of many of the most salient concerns bodes well for encouraging caregiver proactivity in the care process to improve CR outcomes. Further research would benefit from examining caregivers’ perspectives from more diverse populations and contexts, while integrating this knowledge in caregiver burden studies could help to explicitly link targeted interventions to improved health outcomes for caregivers themselves. Additionally, future interventions for CRs would also benefit greatly from caregiver involvement and consultation.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by a grant (#1176689) to Prof. Parker from the Australian National Health and Medical Research Council (NHMRC). The contents of the published material are solely the responsibility of the individual authors and do not reflect the views of the NHMRC.