
Abstract
Objectives:
Judging that the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria for defining mania/hypomania (and thus bipolar I/II disorders, respectively) would benefit from review, we formed an expert taskforce to derive modified criteria for consideration. The aim of this paper is to summarise the component stages and detail the final recommended criteria.
Methods:
We first sought taskforce members’ views on the Diagnostic and Statistical Manual of Mental Disorders criteria and how they might be modified. Next, members recruited patients with a bipolar I or II disorder, and who were asked to judge new definitional options and complete a symptom checklist to determine the most differentiating items. The latter task was also completed by a small comparison group of unipolar depressed patients to determine the mood state items that best differentiate unipolar from bipolar subjects. Subsequent reports overviewed analyses arguing for bipolar I and II as being categorically distinct and generated empirically derived diagnostic criteria.
Results:
Alternatives to all the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria were generated. Modifications included recognising that impairment is not a necessary criterion, removing hospitalisation as automatically assigning bipolar I status, adding an irritable/angry symptom construct to the symptom list, deleting a mandatory duration period for manic/hypomanic episodes, and requiring a greater number of affirmed symptoms for a bipolar diagnosis to manage the risk of overdiagnosis. Granular symptom criteria were identified by analyses and constructed to assist clinician assessment. A potential bipolar screening measure was developed with analyses showing that it could clearly distinguish bipolar versus unipolar status, whether symptom items were assigned as having equal status or weighted by their quantified diagnostic contribution.
Conclusion:
While requiring further validation, we suggest that the revised criteria overcome several current Diagnostic and Statistical Manual of Mental Disorders (5th ed.) limitations to defining and differentiating the two bipolar sub-types, while still respecting and preserving the Diagnostic and Statistical Manual of Mental Disorders template. It will be necessary to determine whether the bipolar screening measure has superiority to currently accepted measures.
Introduction
In diagnosing mental disorders, standardised criteria offered by manuals such as the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) are widely accepted clinically. While any set of diagnostic criteria can always be modified and potentially improved, the DSM-5 definition and differentiation of the bipolar disorders (i.e., bipolar I and II) is worthy of attention. This is a reflection of several issues that we now outline.
The DSM-5 A and B symptom criteria for manic and hypomanic episodes are identical, and thus provide no cleavage between the two states. Criterion C for mania requires ‘marked’ impairment in social or occupational functioning, while Criterion E for hypomania states that the mood state should not be severe enough to ‘cause marked impairment’. There are a few problems with this. First, subjective judgement about impairment criteria (here involving judgement about whether functional impairment is ‘marked’ or not) is problematic, with Goldberg and Harrow (2005) reporting a poor correlation between such subjective judgements and more objective measures of functioning in bipolar patients. Second, the impairment requirement fails to respect the finding that functioning can actually improve in hypomanic and manic patients (Jamison et al., 1980; Judd et al., 2005). Furthermore, while mania is so specified as causing greater impairment than hypomania, Criterion D for hypomania (but not mania) requires that the mood disturbance be observable to others, a somewhat unclear criterion. More importantly, as hypomanic states commonly go unobserved by relatives and clinicians, there is a risk of excluding those with true hypomanic episodes and failing to diagnose a bipolar disorder.
The impairment criteria also specify that an episode is classified as manic if the patient is hospitalised. However, hospitalisation is more a consequence of mania than an integral feature, and its legitimacy (alone and as a differential criterion) is debatable. First, it is context-dependent, with hospitals differing in ease of access and criteria for admission. Second, hospitalisation is not unheard of for those experiencing hypomanic episodes, with an Australian study (Parker and Graham, 2016) quantifying 5391 hospitalisations for diagnosed hypomanic patients (as against 21,857 for manic patients) over a 14-year period. Overall, the impairment criteria for the bipolar disorders have been applied inconsistently (e.g., Angst et al., 2003; Judd et al., 2003), with such criteria, and especially those relating to hospitalisation, having been judged to be ‘extremely arbitrary’ (Joyce, 2008).
Another issue for consideration is the differing minimum periods mandated for the two conditions (i.e., at least four consecutive days for hypomania and 1 week for mania). Such criteria were, to our knowledge, arbitrarily derived, while several empirical studies (Bauer et al., 2011; Benazzi and Akiskal, 2006; Judd et al., 2003; Parker et al., 2014; Tully and Parker, 2007) of those experiencing hypomanic states have demonstrated similar phenotypic patterns in those having briefer episodes than mandated by the DSM duration criteria. More specifically, a study of an outpatient sample (Parker et al., 2006) quantified that 2% of bipolar I and 21% of bipolar II patients had never had a manic/hypomanic episode last more than a day, only 54% of the bipolar I patients had had a manic/hypomanic episode last longer than a week, and that only 31% of the bipolar II patients had had a manic/hypomanic episode last more than 4 days. Thus, if DSM duration criteria are imposed, a distinct percentage of those with a bipolar disorder will be unable to be formally diagnosed. The objective of the current paper is to provide a summary of findings from several studies undertaken by the AREDOC (Assessment, Revision and Evaluation of DSM and Other Operational Criteria) taskforce which aimed to address these concerns. We first describe the AREDOC approach (which sought both the ‘outside-in’ views of taskforce members and the ‘inside-out’ views of those with a bipolar disorder). We then detail the processes involved in generating new diagnostic criteria (which respect the DSM template), and report on the development of a bipolar disorder screening measure derived from study data. Finally, our final criteria set are reported and compared to DSM-5 criteria.
Methods
The AREDOC taskforce consisted of an international team of mental health professionals with clinical and/or research expertise in the field of bipolar disorders and was formed with the goal of improving current diagnostic criteria for those disorders (Parker et al., 2018). While International Classification of Diseases, 11th Revision (ICD-11) criteria can also be challenged, given the widespread clinical acceptance of DSM-5 criteria, the taskforce focused on the latter.
The first stage of the project consisted of eliciting a broad set of candidate features of the bipolar disorders from the 63 taskforce professionals (Parker et al., 2018). Subsequent studies conducted a series of empirical analyses on an international sample of patients. Full details of the methodologies in these studies are reported in other publications (Parker et al., 2018, 2020a, 2020b, 2021).
Results
Clinical opinions
Our first report (Parker et al., 2018) considered the diagnostic conundrums outlined previously and generated some provisional definitional options. A new criterion A was provisionally derived for defining manic/hypomanic states, a large set of candidate phenotypic symptoms was generated, a modified impairment criterion was drafted (which allowed for improved functioning in those with hypomania as well as impaired functioning), and the need for duration criteria was considered – with the last issue being the most contentious. While recognising that assigning a minimum duration to mania/hypomania was, as observed by one member, akin to assigning a minimum duration ‘to a hurricane’, most (but not all) members favoured inclusion of such a criterion to guard against false-positive diagnoses, with their modal recommended minimum period for both hypomanic and manic episodes being 2 days.
Empirically investigating potential operational criteria
The second stage of the project involved an empirical study (Parker et al., 2020b). Taskforce members were invited (11 of whom contributed) to recruit clinically diagnosed bipolar I and II patients (with 74 and 104 enlisted, respectively) who had clear memories of their manic/hypomanic episodes. The first author also recruited a comparison sample of 33 unipolar depressed patients. The bipolar I and II respondents did not differ in reporting rates of first-degree and/or second-degree relatives with a bipolar disorder (i.e., 46% vs 43%), had a similar age of onset of initial depressive episodes (i.e., 21 years) and of manic/hypomanic episodes (i.e., 26 vs 24 years), and did not differ in the duration of their longest (136 vs 172 days) or average (i.e., 61 vs 66 days) manic/hypomanic episode. However, the interval between initial episode and formal bipolar diagnosis was briefer in the bipolar I patients (i.e., 2 vs 9 years).
The bipolar patients were provided with a new definition of a bipolar state: A distinct period of an abnormal and persistently elevated, expansive or irritable mood, with the individual feeling energised and ‘wired’ and which is perceived as an ‘overshoot’ and not simply a state of happiness, and generally oscillating with periods of depression.
This was accepted by 95% of the bipolar I and 97% of the bipolar II participants. However, as all psychiatric conditions are ‘abnormal’, we subsequently deleted this descriptor. The term ‘wired’ was also deleted, being judged by some taskforce members as too colloquial. In Table 1, we provide DSM-5’s Criterion A and our modified version of this criterion.
Operational criteria for manic and hypomanic episodes in bipolar disorders derived by the AREDOC taskforce (right), with the DSM-5 criteria on the left for comparison.
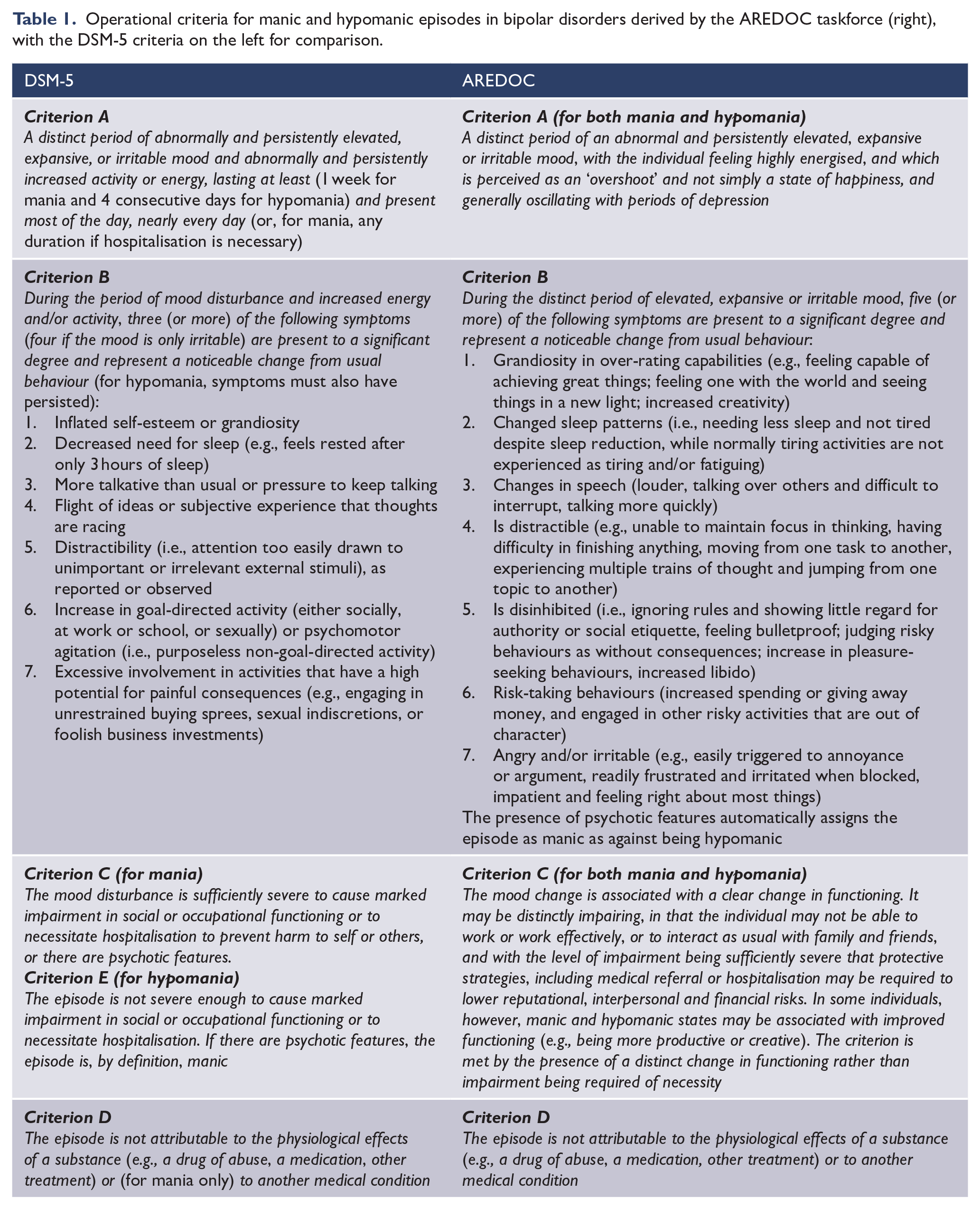
The patients were also provided with two statements addressing ‘impairment’ and were asked if they had experienced any ‘improvement’ in functioning during ‘highs’ and, if so, across what domains. The majority of the bipolar I (76%) and II (86%) group members reported improved functioning, leading to a new criterion addressing functioning (see Table 1). It differs from the existing DSM criterion, in that, it does not vary across manic or hypomanic states, and it allows for both impaired and/or improved functioning. It also positions hospitalisation as simply one of several exemplars of protective strategies that might be required to address illness-related risks to functioning, rather than being a single differentiating diagnostic criterion. Thus, it is positioned as neither necessary nor sufficient to assign a manic state as against a hypomanic one.
The patients were provided with a set of 96 candidate manic/hypomanic symptoms – see Parker et al. (2021) for a full list of the symptoms – and asked to rate the extent to which each typified their manic/hypomanic states (‘very true’, ‘rather true’ and ‘not true at all’). The same item set was provided to the unipolar depressed patients, who were invited to judge whether they experienced each symptom when they felt ‘very happy’ (exemplars of ‘happy’ occasions were provided). Items showing poor differentiation between the bipolar and unipolar patients were deleted. Bipolar I patients were distinctly more likely than the bipolar II patients to report delusions, hallucinations and several potential psychotic or over-valued ideas, and also more often endorsed items weighted to anger or entitlement, such as showing little regard for authority, being uncharacteristically angry or not seeing the point of views of others.
Seeking to have symptom sets defining bipolar status (irrespective of sub-type), we deleted items seemingly weighted to bipolar I status (detailed in the previous paragraph) and quantified similar total mean item scores in the bipolar I and II patients (i.e., 44 vs 41, respectively). Such congruence indicated that the refined symptom set had (as sought) commonality across the bipolar sub-types, but distinctly differentiated the bipolar from the unipolar patients – with mean scores of 42 vs 12 being quantified. Thus, our item set defined bipolar status independent of bipolar sub-type and differentiated bipolar from unipolar mood states.
We then undertook an exploratory factor analysis of the items to derive more granular constructs common to both bipolar sub-types, with a seven-factor solution providing the best statistical fit. We labelled the factors as capturing ‘sleep’, ‘disinhibition’, ‘distractibility’, ‘grandiosity’, ‘anger/frustration’, ‘speech change’ and ‘risk-taking’ constructs, and assembled contributing items to generate seven symptom sets (see Table 1). While DSM-5 criterion A allows the mood state to be ‘irritable’, none of its seven symptom criteria have an ‘irritable/angry’ construct. By contrast, our set does include such a symptom construct. Other nuances include a DSM-5 ‘increased goal-directed activity’ criterion being alternately labelled as a ‘disinhibited’ one by us, and our expanding of DSM’s grandiosity item to include a heightened senses component.
While psychotic features were almost ubiquitous within our clinically diagnosed bipolar I patients (i.e., 90%), nearly, one-third and one-fifth of the assigned bipolar II patients reported delusions and hallucinations, respectively. However, when we compared taskforce members’ and their patients’ reporting of psychotic features there were distinct inconsistencies. While we anticipated that the presence or absence of psychotic features would be an absolute criterion for differentiating bipolar I and II disorders respectively, our data – while supportive – were clearly not absolute. We interpreted this as reflecting rating discrepancies by the clinicians and the patients (perhaps with the latter being inclined to forget episode nuances) and the difficulties in judging psychotic features categorically (i.e., Is a symptom delusional, a de facto psychotic or a non-psychotic over-valued idea? Is a certain symptom truly a hallucination, or a non-psychotic illusion or supra-sensory phenomenon?).
In our proposed revised criteria, we do not impose a minimum duration for hypomania or mania, respecting earlier-referenced studies showing that the phenotypic profile of bipolar disorder has been shown to be similar in samples of those meeting and those not meeting DSM duration criteria. While we respect the concern that not imposing any duration criterion can risk a false-positive diagnosis of a bipolar disorder, we favour not imposing any duration criteria, and instead suggest raising the symptom number threshold. Thus, for a bipolar diagnosis to be made, the patient must meet Criteria A and B as appended and at least five of our seven symptom criteria (i.e., a higher cut-off than the DSM requirement of three or more symptoms) to reduce the risk of a false-positive diagnosis. Data analyses undertaken in preparing this paper quantified that such a cut-off had the highest overall classification rate and 98.2% sensitivity in assigning bipolar as against unipolar status.
Categorical vs dimensional nosology
There is a long-standing debate as to whether bipolar I and II conditions differ dimensionally or categorically. Seeking clarification, we analysed data from our AREDOC bipolar samples (Parker et al., 2020a). The 15 individual items quantified as more likely to be affirmed by the clinically diagnosed bipolar I patients than the bipolar II patients were submitted to a latent class analysis, in which a two-class fit was demonstrated to be superior to both a one-class fit (which would argue for a dimensional model) and a three-class fit (which would argue for there being more than two bipolar categories). In the two-class analysis, those assigned to Class I (putative bipolar I) were distinctly more likely to report delusions, hallucinations, not being bound by social etiquette, having impaired judgement, experiencing mystical events, feeling more religious and being quite grandiose. Even after excluding the symptoms assessing delusions and hallucinations directly, a two-class model (as against a one- or a three-class model) again provided the best fit, a finding interpreted as indicating that the five remaining over-represented symptoms were capturing psychotic manifestations or correlates, or at least over-valued ideas. Mixture analyses for both the 15- and the 13-item sets showed bimodal patterns, with each having a distinct point of rarity. Thus, both the latent class and mixture analyses argued for a two-class categorical model for the bipolar disorders, and further advanced the proposition that manic and hypomanic states (and thus bipolar I and II disorders) are categorically distinct and best differentiated by the respective presence and absence of psychotic features. However, such features may not always be overt, and can perhaps be experienced at the level of over-valued ideas and/or lack of insight.
Deriving a new bipolar screening measure
While multiple bipolar screening tests have been developed (Angst et al., 2005; Hirschfeld et al., 2000), we analysed the AREDOC symptom data set to develop a new measure and evaluate its differentiation potential. Here, we compared the responses of our bipolar and unipolar depressive participants on our original set of over 90 manic/hypomanic symptoms (Parker et al., 2021). As we sought to differentiate those with a bipolar disorder (independent of bipolar sub-type) from those with a unipolar disorder, the item set excluded the two symptoms directly assessing delusions and hallucinations. We used the machine learning technique of prediction rule ensembles (PREs) to identify the contributory capacity of each item to discriminate between the two groups. We calculated total scores on the 20 most discriminating items (shown in Table 2) emerging from the PRE analyses and showed that each had significantly higher prevalence rates in the bipolar group. Total scores on the 20 items were higher in the bipolar than in the unipolar group (i.e., 16.7 vs 4.8) and a receiver operating characteristic (ROC) analysis quantified an optimal cut-off score of 12 or more as indicating bipolar status (sensitivity = 90.9%, specificity = 96.6%, and overall classificatory accuracy = 91.8%).
Discriminating symptoms used for the full 20-item and shortened 10-item set generating a bipolar screening measure.
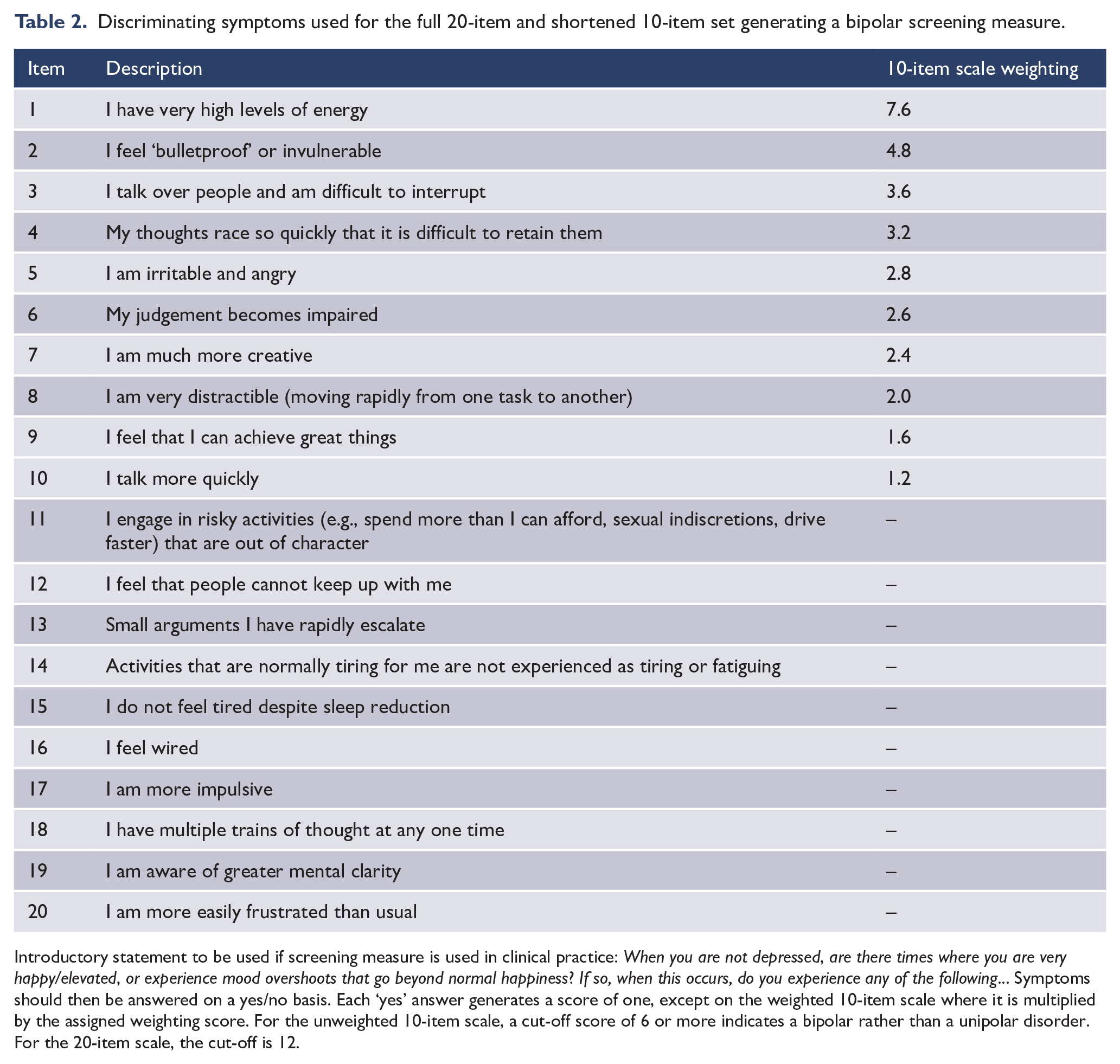
Introductory statement to be used if screening measure is used in clinical practice: When you are not depressed, are there times where you are very happy/elevated, or experience mood overshoots that go beyond normal happiness? If so, when this occurs, do you experience any of the following… Symptoms should then be answered on a yes/no basis. Each ‘yes’ answer generates a score of one, except on the weighted 10-item scale where it is multiplied by the assigned weighting score. For the unweighted 10-item scale, a cut-off score of 6 or more indicates a bipolar rather than a unipolar disorder. For the 20-item scale, the cut-off is 12.
We then elected to determine whether assignment of bipolar or unipolar status was superior if items were differentially weighted as against being weighted equally (Parker et al., 2022). The weightings were obtained from each item’s machine learning-derived relative importance scores from the previous study (Parker et al., 2021), and given the clinical utility of brief measures, we considered only the top 10 items. The analyses placed a stronger emphasis on high energy levels (in which the item’s contribution to the final scale score was increased by a factor of 7.6), feeling bulletproof (4.8), talking over people (3.6) and racing thoughts (3.2), among others. Both the weighted and unweighted versions of the scale were comparable in their classificatory accuracy (96.4% vs 95.9%, respectively). Thus, the analyses did demonstrate strong performance for a shortened 10-item measure (whether with weighted or unweighted items), and it may be more feasible for use in clinical settings that the original 20-item set (Parker et al., 2021). However, the sample’s high classification rates and recruitment of patients with established (bipolar as against unipolar) diagnoses may have made any difference between the weighted and unweighted versions difficult to detect.
Discussion
The AREDOC objective was to determine how DSM-5 criteria for the bipolar disorders (and specifically for hypomanic and manic states) might be best modified to improve diagnostic accuracy while preserving the overall DSM template model. We drew on the views of both mental health professionals with expertise in bipolar disorders and the views of patients with a bipolar disorder, and a literature review and empirical analyses. We undertook salient empirical studies and drew up new criteria sets that respected the DSM template. The objective of this paper was to report on the whole enterprise, provide new summary data for consideration and provide comparative tabulated criteria presented in comparison to DSM-5 criteria.
We now first comment on the differences between DSM-5 criteria and our proposed criteria. Our Criterion A (which is positioned as having equal salience across manic and hypomanic states) seeks to advance distinction between hypo/manic states as ‘overshoots’ as against merely capturing states of normal happiness that might be reported by non-bipolar patients. We suggest that such episodes should ‘generally’ oscillate with depressive episodes, recognising that while unipolar mania/hypomania is rare, it does appear to exist (Goodwin and Jamison, 2007). However, no mandatory minimum duration period was imposed because, if the prototypic syndromal features are met (and we argue for a higher threshold in symptom numbers than in DSM-5), duration requirements should be redundant (as established in several studies noted earlier) and could risk exclusion of those with a true bipolar condition.
Our Criterion B symptom set was derived empirically (as against DSM strategies which weight expert clinical opinion), with a factor analysis of numerous candidate symptoms finding support for a seven-class solution. Our introductory descriptor statement for that symptom set is simpler than the DSM version. As against imposing a duration criterion, and as noted, we favour imposing a higher cut-off number to address concerns about over-diagnosis of a bipolar disorder. Most of our criteria are in accord with DSM-5 constructs (albeit with some variation in naming). However, we also provide an angry/irritable symptom construct which is not in the DSM-5 symptom set, despite DSM-5’s Criterion A allowing that the mood state may be ‘irritable’. The DSM-5 provides illustrative behaviours for only some of its symptoms, whereas we provide multiple exemplars, with each being empirically derived from our factor analyses and thus providing clinicians with illustrative symptom exemplars that allow probe questions germane to each construct to be used in the clinician’s assessment.
While DSM-5 distinguishes between the level of impairment associated with manic (‘marked’ impairment) and hypomanic (‘not severe enough to cause marked impairment’) states, such subjective judgements about functioning levels are problematic for reasons outlined in the Introduction. While it is reasonable to expect levels of impairment to be more severe in mania than in hypomania, our earlier reference to Australian hospitalisation data indicates that hospitalisation (a potential indicator of severity) is not unheard of for those experiencing hypomania. As such, and as against the DSM-5 criterion, where hospitalisation automatically assigns a manic diagnosis, we simply use hospitalisation as one of several exemplars of functional change, but do not position it or any other specific functional change as establishing manic or bipolar I status.
Furthermore, evidence suggests that the psychosocial disability in manic and hypomanic patients is comparable, and that ‘bipolar II is not merely “the lesser” of the bipolar disorders’ (Judd and Akiskal, 2003).
Furthermore, while the DSM-5 allows only impaired functioning in manic/hypomanic states, our literature review and reports from our subjects indicate that improved functioning is not uncommonly experienced during both manic and hypomanic states, thus warranting our quite differing descriptor. If valid, questions then arise as to whether a bipolar disorder with associated improved functioning constitutes a disorder at all. In response, we argue that an elevated mood state nonetheless represents a ‘disturbance’ in an individual’s cognition, emotion regulation, or behaviour (as required by DSM-5 in defining a mental disorder) in that by definition a hypo/manic episode is an overshoot of a euthymic mood. Furthermore, while bipolar patients may report improved functioning in one life domain (e.g., their career) during hypo/manic episodes, it is possible that their functioning in other domains (e.g., excessive spending, indiscrete behaviour) is likely to evidence a level of impairment and effecting ‘disorder’ status.
DSM-5 automatically assigns manic (and thus bipolar I) status to those who are psychotic during such states, and we support that criterion. Such assignment is straightforward if the patient experiences clear delusions and/or hallucinations. Our analyses positioned several other symptoms not formally capturing psychotic features as weighted to a bipolar I class (i.e., ‘little regard for authority’, ‘being uncharacteristically angry’ and ‘not seeing the point of view of others’). Such symptoms are commonly observed in patients who are extremely aggressive and non-responsive to any management advice when in a manic/hypomanic state, and particularly in inpatients. At times, they may be manifestations or correlates of (denied) psychosis, but clearly, they cannot always be so positioned. Such findings indicate an unresolved grey area complicating our recommendation that psychotic features are necessary and sufficient for assigning manic status in patients meeting other criteria for a bipolar disorder. When delusions and/or hallucinations are present, assignment is straightforward. However, in their absence, but when certain other suggested features are present (e.g., extreme and uncharacteristic anger, absence of insight), the intrinsic disorder may be a bipolar I disorder (and a true manic as against hypomanic state). Eliciting the presence of such features would require close questioning and observation of the patient and, commonly, corroborative witness interviews in addition. Nevertheless, we recommend that manic or hypomanic assignment status is affected by one single categorical variable (i.e., the respective presence or absence of psychotic features).
Such a point of distinction is less clear-cut in relation to deciding whether an individual has an intrinsic bipolar I or II disorder (as opposed to deciding whether a particular episode is manic or hypomanic). Some individuals who have had clear-cut psychotic episodes may also have non-psychotic hypomanic episodes over their lifetime, and for most we would regard having one or more manic episode as establishing a bipolar I disorder. However, clinicians observe some patients having psychotic manic episodes early in their illness course and, even without being in receipt of medication, having only non-psychotic hypomanic episodes subsequently. In such instances, we suggest that a change in disorder status (here from bipolar I to II) should be allowed. The converse pattern can also occur, with patients having non-psychotic hypomanic episodes and then later developing psychotic manic states (and then warranting a bipolar I diagnosis). In individuals who have only had hypomanic episodes, all would clearly be assigned as having a bipolar II disorder. Detailed studies examining the extent to which those with a bipolar disorder change from I to II or the converse are clearly required.
In addition to deriving new criteria for wider consideration, the generation of a very large set of manic/hypomanic symptoms by taskforce members allowed us to develop a potential screening tool for those with a bipolar disorder. Both the 20-item and 10-item derived versions showed very high discrimination (as we quantified using a machine learning approach) while weighting each item by their contribution as against regarding each as having equal value (the latter being the DSM strategy) made no difference to the classificatory accuracy. As our subjects were seemingly ‘clear-cut’ cases of those with a bipolar or unipolar disorder (having received such a diagnosis) and were aware of their diagnosis, the measure needs to be evaluated in those who have never received a formal mood disorder diagnosis to establish its intrinsic capacity to differentiate bipolar from unipolar status and to assess (in comparative studies) whether it is superior to currently accepted screening measures.
Limitations
We note a number of limitations raised in the previous AREDOC papers. Only 11 out of the 64 initial taskforce members proceeded to recruit patients for the empirical study, most commonly reflecting the difficulty of obtaining international and inter-institutional ethics approval. The resulting members recruited an international sample of patients, but this sample was not necessarily internationally representative and could have been influenced by a number of biases (e.g., cooperativeness, allegiance to their taskforce clinician, language, memory issues). In addition, the bipolar I/II diagnoses of each patient were provided by their clinician (as against being generated from a structured interview) and were not validated against any standardised measure.
For the patients themselves, their symptoms were self-reported rather than objectively measured. Patient data obtained on the presence or absence of psychotic features also occasionally contradicted the judgements of the taskforce members. This could reflect the reality that patients often have limited memory of psychotic manic episodes, thus hindering their capacity to report on them. Other unknowns include the patient’s English proficiency, the extent to which any current mood state of participants might have impacted on their reports, and their medication histories; the latter of which may play a relevant role in their symptom profile, functional impairment and diagnosis.
The sample of unipolar depressed patients was quite small and were only recruited from one private outpatient clinic, with diagnosis (confirming clinical depression and excluding any bipolar status) being undertaken clinically as against use of a structured interview. Furthermore, the overall sample size was modest compared to the ‘big data’ traditionally used in machine learning models. These two issues could very well have impacted upon the strength of the model and the generalisability of findings, and potentially explain the comparatively low accuracy for the unipolar group.
Because of such issues, the results of the AREDOC studies should be considered preliminary at this stage, with further evaluation of the revised criteria and new screening measure required. Such studies should seek to validate the AREDOC criteria in larger clinical samples and should include comparison against diagnoses made using other bipolar screening measures and by clinicians outside of the taskforce. To address the epistemological challenges in comparing one diagnostic system against another, we suggest that comparing diagnostic models in terms of their sensitivity and specificity with regards to certain properties of the condition (e.g., family history prevalence, or response to one or more accepted mood stabiliser) may be useful.
Conclusion
The AREDOC project was designed to re-evaluate and revise current DSM-5 criteria for the bipolar disorders based on the clinical expertise of international bipolar experts and an empirical investigation of their patients. The studies indicated that revision of several criteria may be beneficial, including recognising that impairment is not a necessary criterion, removing hospitalisation as indicating bipolar I status, and adding an irritable/angry construct to the symptom list, among others. While the revised criteria require future validation, we suggest that the AREDOC project contributes to the multi-faceted discussion in the literature surrounding how elevated mood states, and consequently the bipolar disorders, are to be best defined and diagnosed. Diagnostic criteria for any psychiatric condition can always be critiqued and best regarded as ‘works in progress’ rather than cemented in perpetuity, as recognised by there being iterations over time in DSM and other diagnostic manuals. We hope that the study findings reviewed in this paper may advance the next DSM iteration in defining the bipolar disorders and their component manic and hypomanic states.
Footnotes
Acknowledgements
The authors would like to thank Martin Alda, Tomas Hajek, David Dunner, Claire O’Donovan, Janusz Rybakowski, Joseph Goldberg, Adam Bayes, Verinder Sharma, Philip Boyce and Vijaya Manicavasagar for their contributions to recruitment, data collection and their editorial contributions to the AREDOC manuscripts. The authors would also like to thank Amy Hickey for assisting with recruitment.
Author Contributions
G.P. was the primary author of the manuscript. G.P. also designed the AREDOC studies discussed in this manuscript and contributed to the data collection. M.J.S. and G.T. co-authored the manuscript and contributed to the analyses of the previously mentioned reviewed studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The studies reported here were funded by grants (#1037196 and #1176689) awarded to G.P. from the Australian National Health and Research Council (NHMRC). The contents of the published material are solely the responsibility of the individual authors and do not reflect the views of the NHMRC.