
Abstract
Background:
There is a complex relationship between health and religiosity. People may use religion to cope with difficulties and uncertainties in their life – such as induced by the COVID-19 pandemic.
Aims:
The purpose of this study is to investigate the relationship between religious coping, care burden and psychological distress among caregivers during COVID-19 in Pakistan.
Method:
We conducted a cross-sectional survey in Pakistan. We used the Religious Coping Scale (RCOPE), Care Burden Scale (CB), and Depression, Anxiety and Stress Scale (DASS-21) to measure psychological stress from 303 caregivers. Data were analyzed using a hierarchical linear regression model for each of the three outcome variables, which are depression, anxiety, and stress. This analysis allows to investigate whether adding variables significantly improves a model’s ability to predict the criterion variable.
Results:
The findings reveal that emotional care burden, physical care burden, negative religious coping, and social care burden explain a significant amount of the variance of three components of psychological distress among caregivers.
Conclusions:
Health experts, psychologists, and policymakers can make better strategies to combat pandemics like COVID-19 by incorporating religious coping methods.
Background
In some societies, the influence of religion on social life is beyond question (Roof & McKinney, 1987, p. 103). Because of its function, religion has been an important topic of interest and research for sociologists since sociology became a scientific discipline (Durkheim, 1898; Weber, 1993). The way in which people respond to stress through their religion or relationship with religion has been conceptualized as religious coping (Ano & Vasconcelles, 2005; K. Pargament et al., 2011). During the COVID-19 pandemic, religiosity was one important factor to maintain people’s well-being (Koenig, 2020; Rahman et al., 2020). Previous research has demonstrated that religious coping is helpful in order to calm the level of depression (Brelsford et al., 2015; Chong et al., 2019), anxiety (Dolcos et al., 2021), and stress (Pandey & Singh, 2019; Thomas & Barbato, 2020) by enabling people to deal with remorse (Knabb & Grigorian-Routon, 2014), accept the God’s will (K. I. Pargament et al., 1990), perceive illness positively (Phillips & Stein, 2007), and manage their fears (Menzies & Menzies, 2020; Rosmarin & Leidl, 2020; Vishkin et al., 2020). Religious coping acts as a shield, which reduces the negative effects of anxiety on people especially suffering from chronic illness (Tepper et al., 2001) and psychological distress (Trevino et al., 2012). Religious coping increases confidence and hope that, in turn, prevents the fear of death (Park, 2020).
The foundation for positive religious coping is to secure a relationship with the sacred (Bush et al., 1999; O’Brien et al., 2019), a positive point of view regarding the universe (Giordano et al., 2015), and, finally, a sense of spiritual connections with others (Allen & Lo, 2010; Ciarrocchi & Brelsford, 2009). Positive religious coping techniques in the context of life stressors have been associated with improved well-being and individual growth (Counted et al., 2022). However, religious coping is not always positive. Negative religious coping also exists (K. I. Pargament et al., 1998) reflecting a complex relationship with religion, a threatening point of the world’s view regarding religion that negative coping creates major stress issues and increased religious/spiritual struggles of the individuals (Abu-Raiya et al., 2015). Negative religious coping, as opposed to positive religious coping, is associated with those who suffered from mental health issues (Gerber et al., 2011; Vitorino et al., 2019).
Gartner et al. (1991) explained that there is a complex relationship between health and religiosity, often to the extent that many different aspects of religiosity are significant predictors that increase the level of anxiety rather than reduce it (Folkman & Moskowitz, 2004; Seybold & Hill, 2001). People usually look to religion to cope with difficulties and uncertainties in their life (Folkman, 2013; Krause et al., 2002) and they often become more religious when they face challenges in their life, such as a serious illness (Koenig & Koenig, 2008, p. 23), the death of a family member (Chapple et al., 2011), divorce (Beehr et al., 1995), severe accident (Pargament, 2001), and happening of natural calamities (Ano & Vasconcelles, 2005; Bentzen, 2019).
Researchers figured out that COVID-19 patients often completely depend on care providers because of their breathing issues (Budnick et al., 2021), weakness (Chowdhury et al., 2020), and other medical confines (Keesara et al., 2020). Caregivers are frequently emotionally drained (Losada et al., 2022) and wish for escapism (Dubey et al., 2021) from the situation because they feel detachment (Anderson & Parmar, 2020), physical (Dhavale et al., 2020) as well as emotional suffering (Sun et al., 2020) due to their frenzied routine of constant care provision (Mohammadi et al., 2021). Care providers also bear social isolation (Pietrabissa et al., 2021), financial problems (Prime et al., 2020), limited social mobility (Binswanger et al., 2021) and lack of communication with other family members, friends and relatives (Mojtahedzadeh et al., 2021). Therefore, this study aims to investigate the relationship between religious coping, care burden and psychological distress among caregivers during COVID-19 in Pakistan, being an example for a traditionally oriented country.
Methods
Study design
We conducted a cross-sectional study in Muzaffarabad City, which is the capital of Azad Jammu and Kashmir State. The area was selected because there are only two state hospitals (Combined Military Hospital and Abbas Institute of Medical Sciences) which have official record of COVID-19 patients and can provide reliable contact information on patients and respondents (caregivers).
Sampling
The sample was selected through systematic sampling method (every ninth respondent from the list provided by the hospitals). The total cases until March 2021 were 3,429, 1 so by using Taro Yamani’s formula (Yamane, 1973) a sample size of 358 was calculated to conduct the current research:


Research instruments
Data was collected from caregivers’ of COVID-19 patients residing in Muzaffarabad by a structured interview schedule. The research tool was divided into four parts:
The instruments were translated into Urdu Language. The Local Health Department and hospital authorities were asked to review the statements to avoid any conflict and be assured that the information collected does not include any confidential data. Furthermore, the respondents of the study were asked to read the items and raise their queries or confusions prior to completing the interview.
Ethical considerations
The present study was conducted during the COVID-19 pandemic in Pakistan. During data collection, we strictly followed the standard operating procedures defined by the World Health Organization and Government of Pakistan. Written informed consent was taken after participants were briefed about the study. Respondents were authorized to terminate the interview at any stage if they feel uncomfortable with any of the statements. The respondents were ensured that no personal information is required for this study and also that the collected information does not involve any hidden or commercial purpose. The topic and research instruments were approved by the Ethical Review Board of SZABIST-Islamabad and formal permission was taken from the Health Department of Azad Jammu and Kashmir.
Results
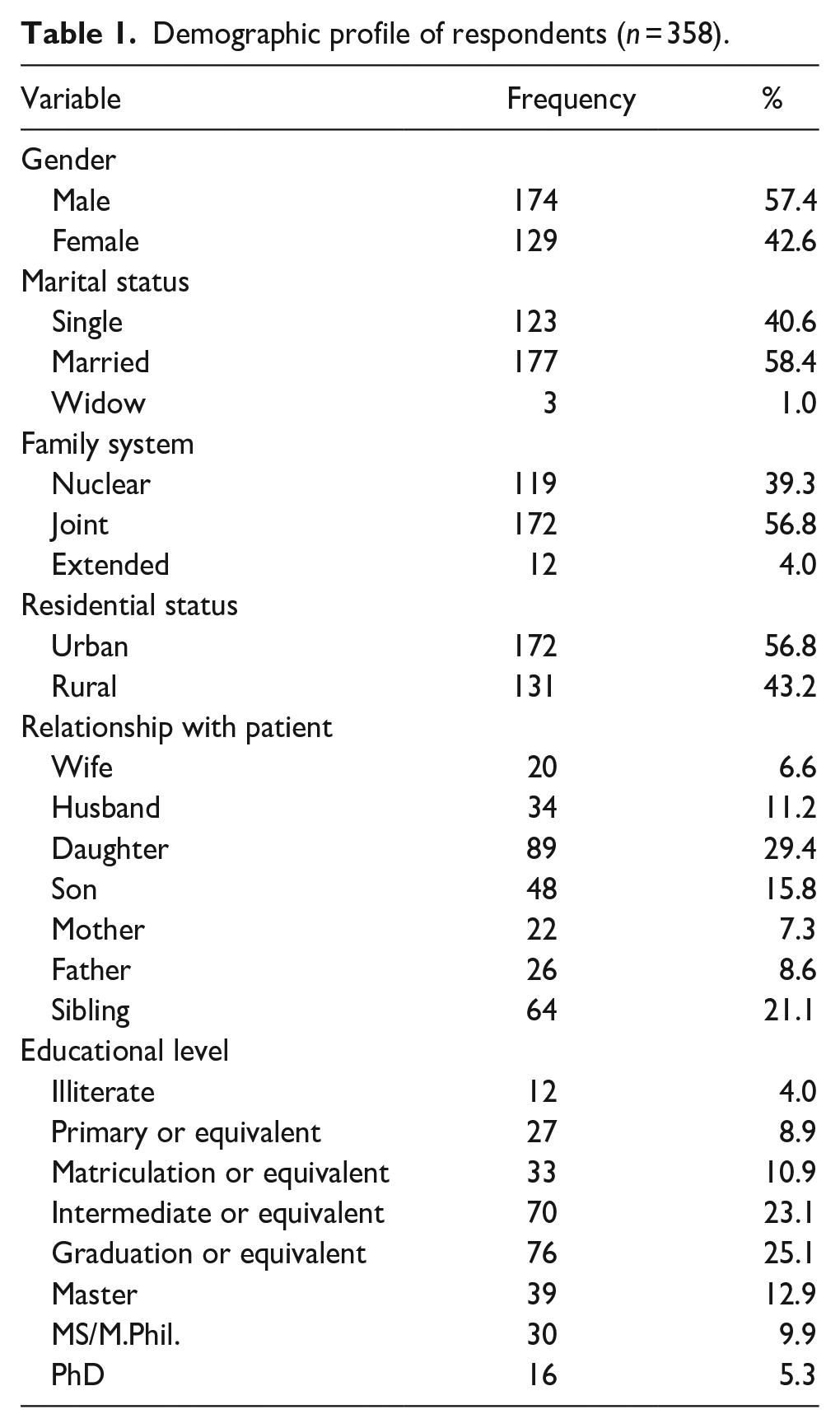
Table 1 shows the demographic profile of respondents. The majority of caregivers (57.4%) was male. The data also reveal that 40.6% were single and 58.4% were married. Most were living in joint family system (56.8%) and in urban areas (56.8%). According to the relationship with patients, our study sample consisted of caregivers who were mainly daughters (29.4%), siblings (21.4%), either husband or wives (17.8%), and sons (15.8%).
Demographic profile of respondents (n = 358).
Depression
The findings presented in Table 2 reveal that emotional care burden, physical care burden, negative religious coping, and social care burden explain a significant amount of the variance of depression among caregivers of COVID-19 patients (F = 30.646, p < .001, R2 = .291). Emotional care burden (β = .263, p < .001), physical care burden (β = .210, p < .001), negative religious coping (β = .191, p < .001), and social care burden (β = .141, p < .05) significantly positively predict depression among caregivers of COVID-19 patients. This mean that caregivers who used negative religious coping were suffering from depression consequently. Caregivers who faced emotional, physical, and social burden also faced depression while taking care of COVID-19 patients.
Predictors explaining the variance of depression among caregivers of COVID-19 patients.
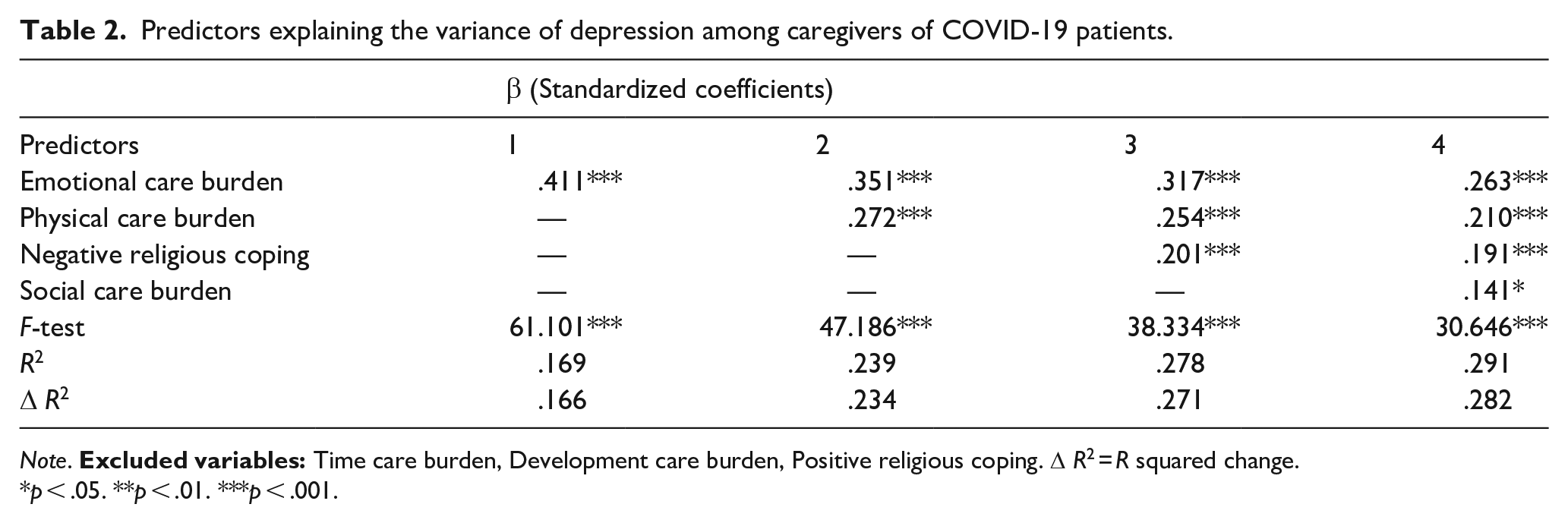
Note.
p < .05. **p < .01. ***p < .001.
Anxiety
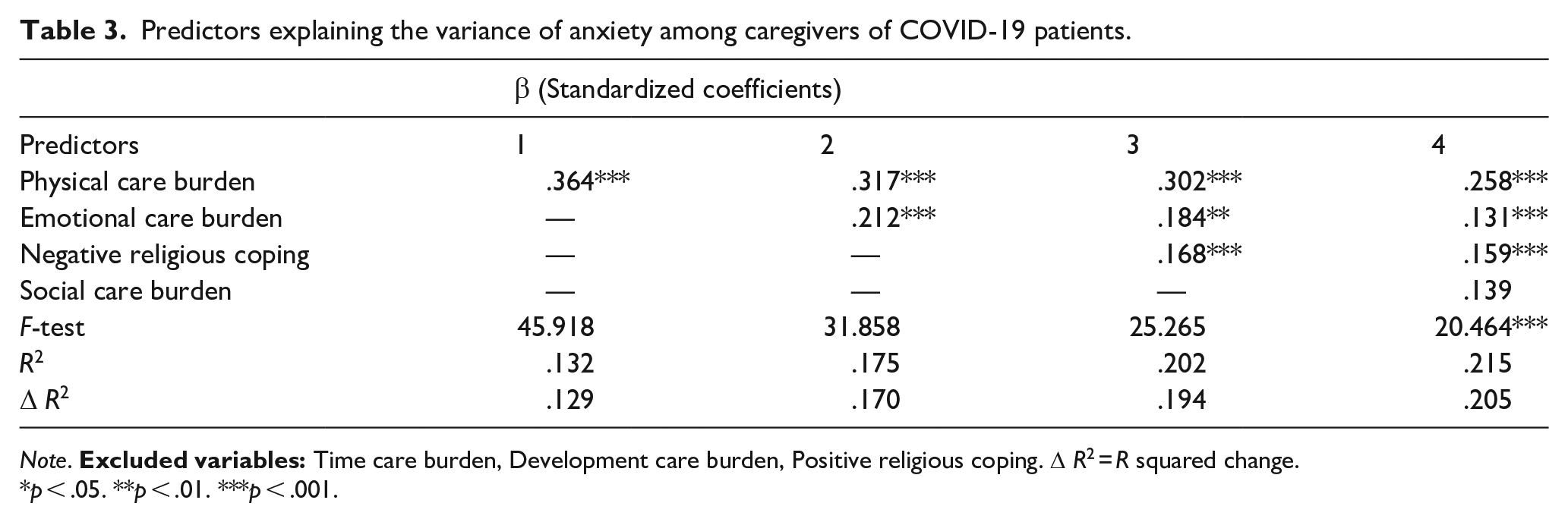
Emotional care burden, physical care burden, negative religious coping, and social care burden explain a significant amount of the variance of anxiety among caregivers of COVID-9 patients (F = 20.464, p < .001, R2 = .215). The analysis shows that physical care burden (β = .258, p < .001), emotional care burden (β = .131, p < .001), and negative religious coping (β = .159, p < .001) are positively predicting anxiety among caregivers of COVID-19 patients. This implies that the caregivers who used negative religious coping were suffering from anxiety. The caregivers who were having emotional and physical burden also faced anxiety while taking care of COVID-19 patients in the pandemic (Table 3).
Predictors explaining the variance of anxiety among caregivers of COVID-19 patients.
Note.
p < .05. **p < .01. ***p < .001.
Stress
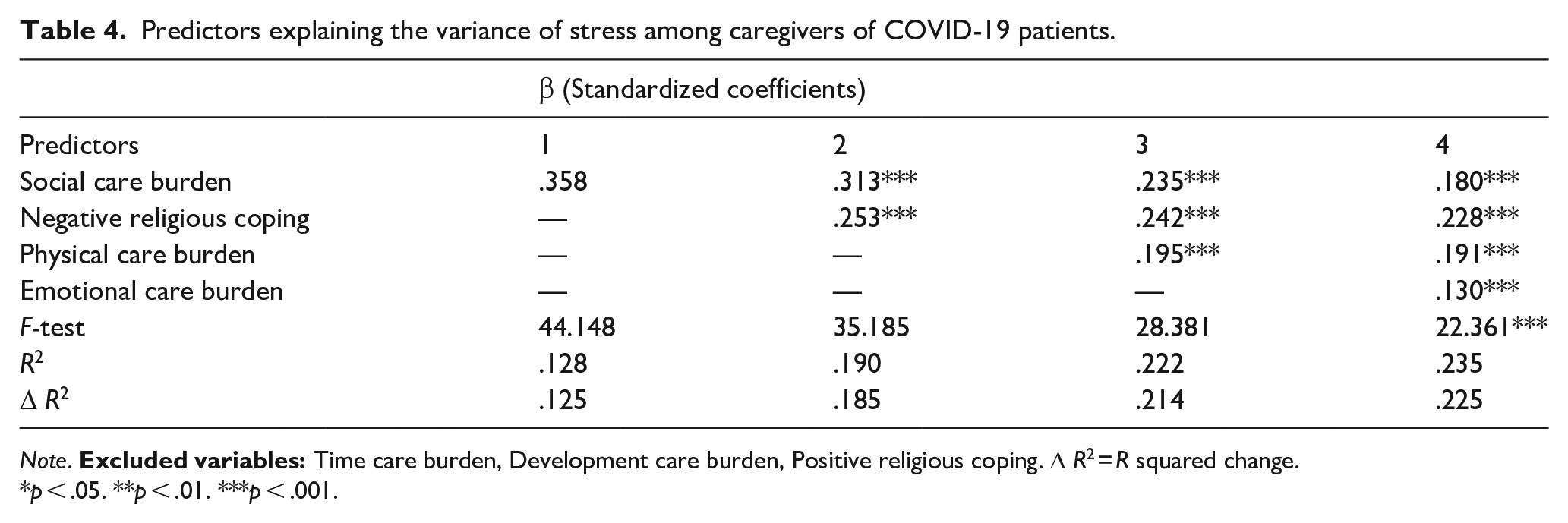
The findings of Table 4 reveal that emotional care burden, physical care burden, negative religious coping, and social care burden explained a significant amount of the variance of stress among caregivers of COVID-19 patients (F = 22.861, p < .001, R2 = .235). The analysis shows that social care burden (β = .180, p < .001), negative religious coping (β = .228, p < .001), physical care burden (β = .191, p < .001), and emotional care burden (β = .130, p < .001) are significantly positively predicting stress among caregivers of COVID-19 patients. This mean that the caregivers who used negative religious coping were suffering from stress resultantly. The caregivers who were having emotional, physical, and social burden also faced stress while taking care of COVID-19 patients.
Predictors explaining the variance of stress among caregivers of COVID-19 patients.
Note.
p < .05. **p < .01. ***p < .001.
Discussion
COVID-19 patients, their families and caregivers bear significant levels of psychological distress due to abnormal physical and mental states. This study aimed to figure out the effect of religious coping and care burden on psychological distress of the caregivers of COVID-19 patient. It found that religion plays a significant role as a coping strategy, particularly in terms of negative dimensions (i.e. negative religious coping increased psychological distress among respondents).
During the COVID-19 pandemic, people adopted various measures to cope with their mental health challenges (Fullana et al., 2020). In this regard, religious coping remained a ubiquitous practice, particularly among traditional societies to seek protection (Meza, 2020), prevention (Ede & ZuokeKalu, 2021), and healing (Yoosefi Lebni et al., 2021) to overcome the psychological (Yıldırım et al., 2022), social (Fitri & Nashori, 2021) and behavioral problems (Cassell, 2020) among patients, caregivers and the general population.
COVID-19 has a negative impact on the psychological well-being of caregivers (Christner et al., 2021; Davidson et al., 2021), namely causing more psychological distress (J. Zhang et al., 2020). Within our study, for three components of psychological distress (i.e. depression, anxiety, and stress) the significant predictors were emotional care burden, physical care burden, and negative religion coping. These results imply that increasing emotional and psychical care burden on caregivers of COVID-19 patients increases depression, anxiety, and stress. Similarly, the increase in negative religious coping also creates psychological distress.
This may create a social gap between caregivers and the society, because caregivers face financial, emotional, and psychological problems to handle and respond in such a way that the patient and further family members remain comfortable. Caregivers of COVID-19 patients face severe levels of psychological distress because of the bad health of patients (Zhao et al., 2020) and also because of their own lives (Park, 2021) which remain in danger throughout the caring period (L. Zhang et al., 2021).
Religion is considered as strong agent of socialization, social support, and a process of healing, especially in traditional societies. Financial, psychological, emotional and social problems are often tackled by religious practices. During COVID-19, people observed religious practices as source of healing and meditation. It is not surprising that people have turned to religion for their comfort during the time of outbreak and people follow religion to overcome their fears (Wilson et al., 2020). The COVID-19 pandemic poses a very severe amount of burden, particularly in terms of care of the patients with regards to the issues related to time management and limitations due to care of patients, development, physical movement, social and emotional involvement and activities.
When interpreting the results, one needs to keep in mind that all data is based on self-reports. It may be biased due to a selective sample and social desirability to answer the questions. Furthermore, it is cross-sectional data which does not allow to draw causal conclusions.
Conclusion
This study found high levels of depression, anxiety, and stress due to the burden of care and use of negative religious coping mechanisms. During the COVID-19 pandemic, care burden has significantly impacted on the lives of caregivers. Caregivers faced care burden of patients in terms of social, emotional, and physical burden. Being members of a religiously oriented society, the respondents of this study were inclined toward the confirmation of positive religious coping and the increase in psychological distress was found due to negative religious coping. The pandemic encouraged people to connect with religion and adopt the religious methods for healing and handling strategies especially for emotional, social and psychological problems.
Footnotes
Acknowledgements
None
Authors contributions
MAHR, SAM, MMM and FF contributed to the study conception and design. Material preparation and data collection was performed by SAM. Data analysis was performed by MMM and MAHR. The first draft of the manuscript was prepared by MAHR. FF critically revised the manuscript for important intellectual content. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethical Review Board of SZABIST-Islamabad (Ref. No.: IERB(7)/SZABIST-ISL(SS)/1890103/200176).
Informed consent from participants
Written informed consent was taken from participants.
Data availability
Data is available from corresponding author upon reasonable request.