
Abstract
How does informal care affect caregivers’ well-being? Theories and existing research provide conflicting answers to this question, partly because the temporal processes and conditions under which different aspects of well-being are affected are unknown. Here, we used longitudinal data from Dutch, German, and Australian representative panels (281,884 observations, 28,663 caregivers) to examine theoretically derived hypotheses about changes in caregivers’ life satisfaction, affective experiences, depression/anxiety, and loneliness. Overall, results provided evidence for negative well-being effects after the transition into a caregiver role, with more pronounced and longer-lasting well-being losses in women than in men. We further found that well-being losses were larger with more time spent on caregiving, in both men and women. These results were robust across moderators of the caregiving context (care tasks, relationship with care recipient, and full-time employment). Together, the present findings support predictions of stress theory and highlight lingering questions in theoretical frameworks of care-related well-being costs.
Informal care is highly consequential to caregivers’ lives and, potentially, their health and well-being (Pinquart & Sörensen, 2003). With aging populations and strained health-care systems, the proportion of people providing informal care will rise in coming decades (Verbakel et al., 2017). Theory and empirical evidence provide a mixed picture, with some studies indicating negative well-being effects of caregiving (Gerlich & Wolbring, 2021; Hansen & Slagsvold, 2013), others reporting no effects (Hajek & König, 2016, 2018), and others even reporting well-being benefits of informal caregiving (Lakomý, 2020).
In addition, the temporal process by which caregiving may affect different aspects of people’s psychosocial well-being (Willroth, 2023) is largely unknown. It thus remains unclear when, how, and for whom caregiving may have positive or negative well-being effects. To address these questions, we used data from three nationally representative panels (281,884 observations from 28,663 caregivers in the Netherlands, Germany, and Australia) to examine the prospective longitudinal effects on life satisfaction, affective experiences, loneliness, and depression/anxiety of transitioning into the caregiving role. We further examined the effects of caregiving intensity and tested a set of demographic, social, and contextual moderators. Thereby, we aimed to advance our theoretical understanding of the psychological implications of informal caregiving for caregivers’ well-being.
Theories of Informal Care and Well-Being
Theoretical perspectives diverge on how and why well-being may be affected by the provision of informal care, which we define as giving care and support for close others in need (excluding regular childcare). First, perspectives rooted in social-exchange theory (Thibaut & Kelley, 1959) and psychological well-being (Ryff & Keyes, 1995) postulate that informal caregivers commonly experience positive well-being consequences (including life satisfaction and affect; Marino et al., 2017) through the appraisal of role gains (Kramer, 1997) and the experience of purpose and meaning (Quinn & Toms, 2019).
In contrast, stress theory predicts decreases in well-being related to both the primary stressors of caregiving tasks and to secondary stressors, such as family conflict or economic struggles (Pearlin et al., 1990). More involved care may be also related to more concern about the care recipient’s health (Wünsche et al., 2020). Therefore, high time expenditure and more involved types of care tasks (e.g., personal hygiene) should exacerbate well-being losses. Moreover, stress theory emphasizes that both stressor exposure and reactivity are more pronounced in women (Blaise & Dillenseger, 2023; Kramer & Kipnis, 1995).
Role-strain theory (Goode, 1960) also predicts negative well-being effects of caregiving, but places more emphasis on the compatibility of different social roles. The informal-caregiver role should thus lead to particularly strong well-being decreases if it conflicts with preexisting roles. Conflicting role demands (e.g., with formal employment) may thus aggravate decreases in well-being if these demands exceed caregivers’ finite resources.
In summary, existing theories provide conflicting predictions and lack critical details about the process under which positive or negative well-being effects can be expected. More research is needed to address these theoretical gaps and to provide a more nuanced psychological understanding of informal care.
Empirical Evidence
Existing evidence mainly indicated decreases in caregivers’ well-being over time. However, there are several caveats that preclude firm conclusions, as outlined next.
For example, it remains unclear whether decreases in life satisfaction tend to be especially pronounced among, or only present in, female caregivers (Gerlich & Wolbring, 2021; Hajek & König, 2016, 2018), for people who spend more time on caregiving (van den Berg et al., 2014), and who provide care for partners compared to kin (Hansen & Slagsvold, 2013). Notably, for kin caregiving, one study even reported increased life satisfaction (Rafnsson et al., 2017). Fewer studies have investigated the affective experiences of caregivers. One longitudinal study reported a decrease in negative affect only among women caregivers (Marks et al., 2002), yet another found no change (Hajek & König, 2016). Evidence for changes in symptoms of depression and anxiety is also inconclusive, with some studies indicating no effects (Hajek & König, 2018), others reporting effects for women (Lacey et al., 2019) or men only (Zwar et al., 2020), and still others finding heightened depression and anxiety across genders (Oshio, 2014). Similarly, findings for loneliness ranged from no effects (Hajek & König, 2019) to higher loneliness in men only (Zwar et al., 2020), and even beneficial effects on loneliness (Lakomý, 2020). Overall, existing evidence is inconclusive (see Table S1 in the Supplemental Material available online) and does not explain when and how informal caregiving affects different aspects of well-being.
The Present Study
The purpose of this study was to examine the longitudinal effects of informal caregiving on different well-being aspects in three nationally representative samples. Cultural differences may shape informal caregivers’ experiences, including their level of support, financial assistance, and recognition, which may affect links between informal care and well-being. Here, we used data from the Netherlands, Germany, and Australia, three countries with distinct health-care and welfare systems. However, critically, each of these countries has a universal health-care system that supports community-based in-home care, which allowed us to examine the generalizability of results across these countries.
We used prospective longitudinal designs to examine changes within caregivers over time while controlling for stable between-person differences that may influence who selects into the caregiving role. We examined how well-being changed over time when people transitioned into caregiving (Research Question 1) and how variations in the time spent on caregiving related to changes in well-being (Research Question 2). Given the diverse reality of caregiving contexts, we investigated whether characteristics of the person and the care situation moderated these effects (Research Question 3). Specifically, we tested as moderators gender, the relationship with the care recipient (Lee et al., 2020), types of care activities (Blaise & Dillenseger, 2023), and conflicting role demands in the form of full-time employment (Bom & Stöckel, 2021).
We preregistered the following hypotheses (https://osf.io/35spn):
Well-being decreases following the transition to become a caregiver (H1).
With more time spent on caregiving, individuals experience more pronounced decreases in well-being (H2).
Caregivers experience more pronounced decreases in well-being if they are female (H3a), perform personal-care activities (e.g., bathing, showering, dressing; H3b), care for someone in their household (H3c), or are employed full time (H3d).
Research Transparency Statement
General disclosures
Study disclosures
Method
We used data from three nationally representative household panel studies: the Dutch Longitudinal Internet Studies for the Social Sciences (LISS), the German Socio-Economic Panel (SOEP), and the Household, Income and Labour Dynamics in Australia Survey (HILDA; see Table 1; for more information, see Research Transparency). These ongoing household panel studies are based on probability samples of the population in private households in each country. All adult members of participating households are invited to yearly interviews.
Caregiver Analysis Samples
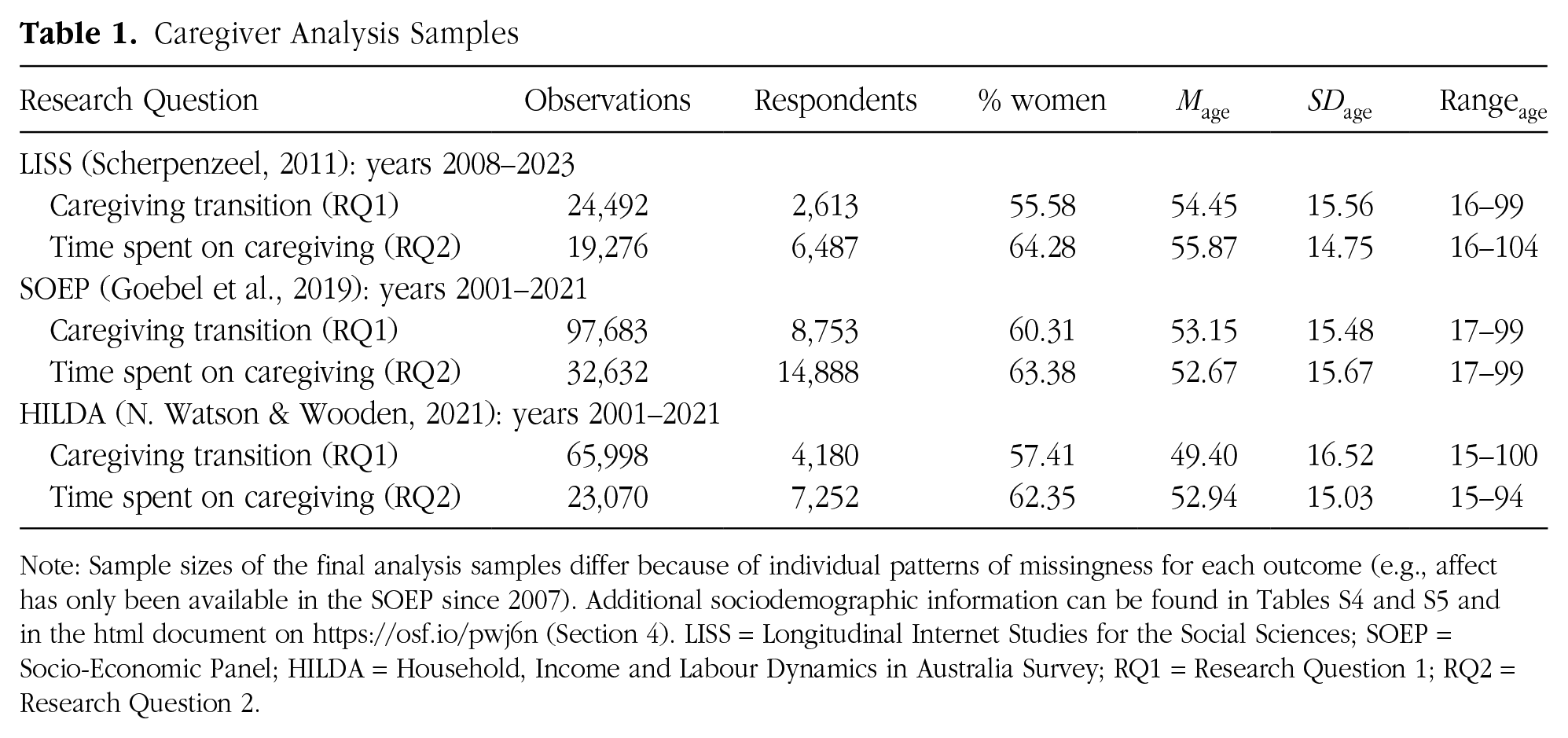
Note: Sample sizes of the final analysis samples differ because of individual patterns of missingness for each outcome (e.g., affect has only been available in the SOEP since 2007). Additional sociodemographic information can be found in Tables S4 and S5 and in the html document on https://osf.io/pwj6n (Section 4). LISS = Longitudinal Internet Studies for the Social Sciences; SOEP = Socio-Economic Panel; HILDA = Household, Income and Labour Dynamics in Australia Survey; RQ1 = Research Question 1; RQ2 = Research Question 2.
We included all respondents with information on informal caregiving and at least one available well-being measure. Specifically, for analysis samples of the transition to caregiving (Research Question 1), we included as caregivers respondents who reported providing informal care after not having done so in the previous wave, and we included as noncaregivers those who reported never providing care. For analysis samples of time spent on caregiving (Research Question 2), we included any observations with valid information on the hours of care they provided.
Measures
Extensive details about all measures, including their internal consistencies, transformations, and scale references are compiled in Table S2 in the Supplemental Material.
Well-being
Subjective well-being is composed of a cognitive-evaluative component, life satisfaction, and an affective component that includes positive and negative affect. In addition, we considered depression/anxiety (i.e., dimensional severity of psychological distress) and loneliness (i.e., unwanted feelings of social isolation) to capture a broader set of relevant psychosocial well-being aspects (Willroth, 2023). All well-being measures were mean scored, such that higher values represented a higher construct manifestation, and, for better comparability across and within samples, scored as percent of maximum possible (POMP) to be interpretable on a scale from 0 to 100.
Life satisfaction
The LISS used the 5-item Satisfaction with Life Scale (SWLS; Diener et al., 1985), from which we used the first four items (see Table S2), whereas both the SOEP and HILDA relied on a single-item measure of life satisfaction (HILDA: “All things considered, how satisfied are you with your life?”). Such single-item measures have been shown to have high reliability and produce comparable results to longer scales like the SWLS (Cheung & Lucas, 2014).
Affect
In the LISS, affect was measured with the Positive and Negative Affect Schedule (PANAS; D. Watson & Clark, 1999), with 10 items each for positive affect (e.g., “enthusiastic,” “alert”) and negative affect (e.g., “upset,” “afraid”). In the SOEP, the frequency of positive affect (“happy”) and negative affect (“angry,” “worried,” “sad”) was assessed over the last 4 weeks. In HILDA, affect during the last 4 weeks was assessed with four items from the Short-Form Health Survey 36 for positive affect (e.g., “Have you been a happy person?”) and five items for negative affect (e.g., “Have you felt down?”).
Depression/anxiety
The LISS used an adapted version of the Mental Health Inventory short scale to measure depression and anxiety symptoms (e.g., “I felt depressed and gloomy”). The SOEP provides a mental-health-component summary score using the Short-Form-12 Health Survey asking about symptoms during the last 4 weeks (e.g., “feel down and gloomy”). This measure was administered every 2 years from 2002 to 2020 (for some respondents also in 2017 and 2019). We did not form a depression/anxiety score for HILDA because the items overlapped with those we used for affect.
Loneliness
The LISS included a 6-item loneliness scale (e.g., “I often feel deserted”). The SOEP included a 3-item short version of the UCLA Loneliness Scale (e.g., “How often do you feel left out?”), administered every 4 years from 2013 to 2021 (and in some irregular intervals; see Table S2a). In HILDA, we used a 3-item loneliness scale (e.g., “I often feel very lonely”).
Informal caregiving
Informal caregiving was assessed in the LISS with the question “Did you perform any informal care over the past 12 months; that is, did you regularly help someone in your environment requiring help due to a disease or other affliction?”—followed by the question “How many hours of informal care did you provide per week, on average?” In the SOEP, we estimated informal caregiving from the time-use question “What is a typical weekday like for you? How many hours per normal workday do you spend on the following activities? – Care and support for persons in need of care.” In HILDA, we also relied on a time-use question—“How much time would you spend on each of the following activities in a typical week? – Caring for a disabled spouse or disabled adult relative, or caring for elderly parents or parents-in-law”—which was part of an additional self-completion questionnaire, resulting in a somewhat higher initial nonresponse rate in HILDA.
Moderators
Gender
Gender was assessed as a binary variable in all three panels and dummy-coded (0 = men, 1 = women).
Personal-care activities
In the LISS, caregivers provided information about the kinds of care tasks they engaged in. In the SOEP, we used the care recipient’s insurance-relevant care level and linked it to the caregiver in the same household to derive an indicator of care intensity. Consequently, this specific SOEP analysis was based on a smaller subset of informal caregivers who reported providing care within the household. In both samples, we dummy-coded the time-varying moderator “personal care” (e.g., washing, dressing; 0 = no, 1 = yes). In HILDA, there was no consistent information on care activities.
Relationship with care recipient
We dummy-coded the moderator “care in household” (0 = no, 1 = yes) in all three studies. In HILDA, the underlying information was available only since 2005 (see Table S2c in the Supplemental Material for more details). In the LISS, respondents reported specifically on the relationship with care recipients. For exploratory follow-up analyses, this allowed us to distinguish between romantic partners, close relatives (parent, sibling, or child), and others.
Full-time employment
In the LISS, we used a threshold of 36 weekly work hours or more to infer full-time employment (0 = no, 1 = yes) because this is considered a full-time job in the Netherlands. For SOEP and HILDA, we relied on labor-force-status variables.
Analyses
To investigate how informal caregiving affects well-being, we used fixed-effects models (McNeish & Kelley, 2019). Fixed-effects models exclusively analyze within-person variance in longitudinal data by including a cluster-affiliation dummy variable for each person. Conceptually, this is similar to person-mean centering of all variables in multilevel models. The main advantage of this strategy is that fixed-effects models are not biased by omitted time-invariant confounders. These models provide automatic control for time-invariant background characteristics—observed and unobserved—such as prior education, intelligence, or stable personality traits. 1
Transition to informal caregiving
We first estimated the effects of transitioning into the informal caregiver role on well-being (Research Question 1). To do this, we considered only respondents who were not caregivers in their first assessment and became caregivers at a later assessment. Because the SOEP only assessed whole hours per day, we harmonized the procedure of coding the transition to caregiving by considering only caregiving of at least 1 hr per day following no caregiving in the previous wave as a transition in the LISS and HILDA (for more details, see Table S2 and deviations_prereg.pdf on https://osf.io/86akr).
We coded five discrete time dummy variables to model time in relation to the role transition to informal caregiver, from “year 2 before the transition” to “3 or more years after the transition.” This coding scheme (Table 2) had the advantage that it imposed no functional form on the change trajectories, thus allowing for nonlinear, discontinuous change to be modeled. The discrete time dummy variables were interacted with gender to arrive at separate estimates for the trajectories of men and women. We ran separate models for each of the five well-being outcomes and each country. The formula for an exemplary model predicting life satisfaction (LS) for a person
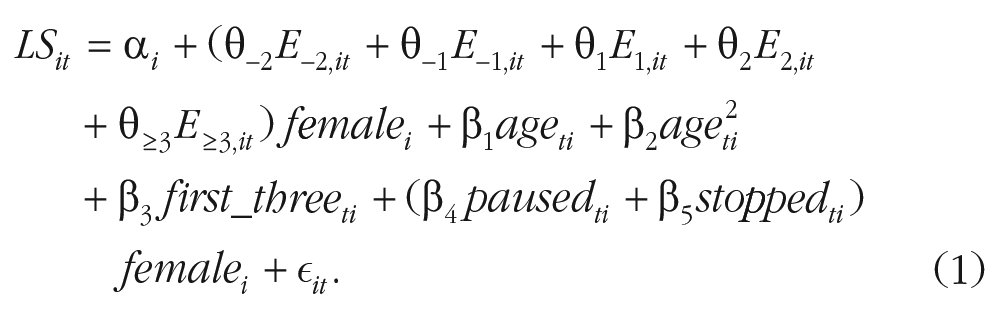
Here,
Exemplary Coding Scheme to Model the Transition to Informal Caregiving
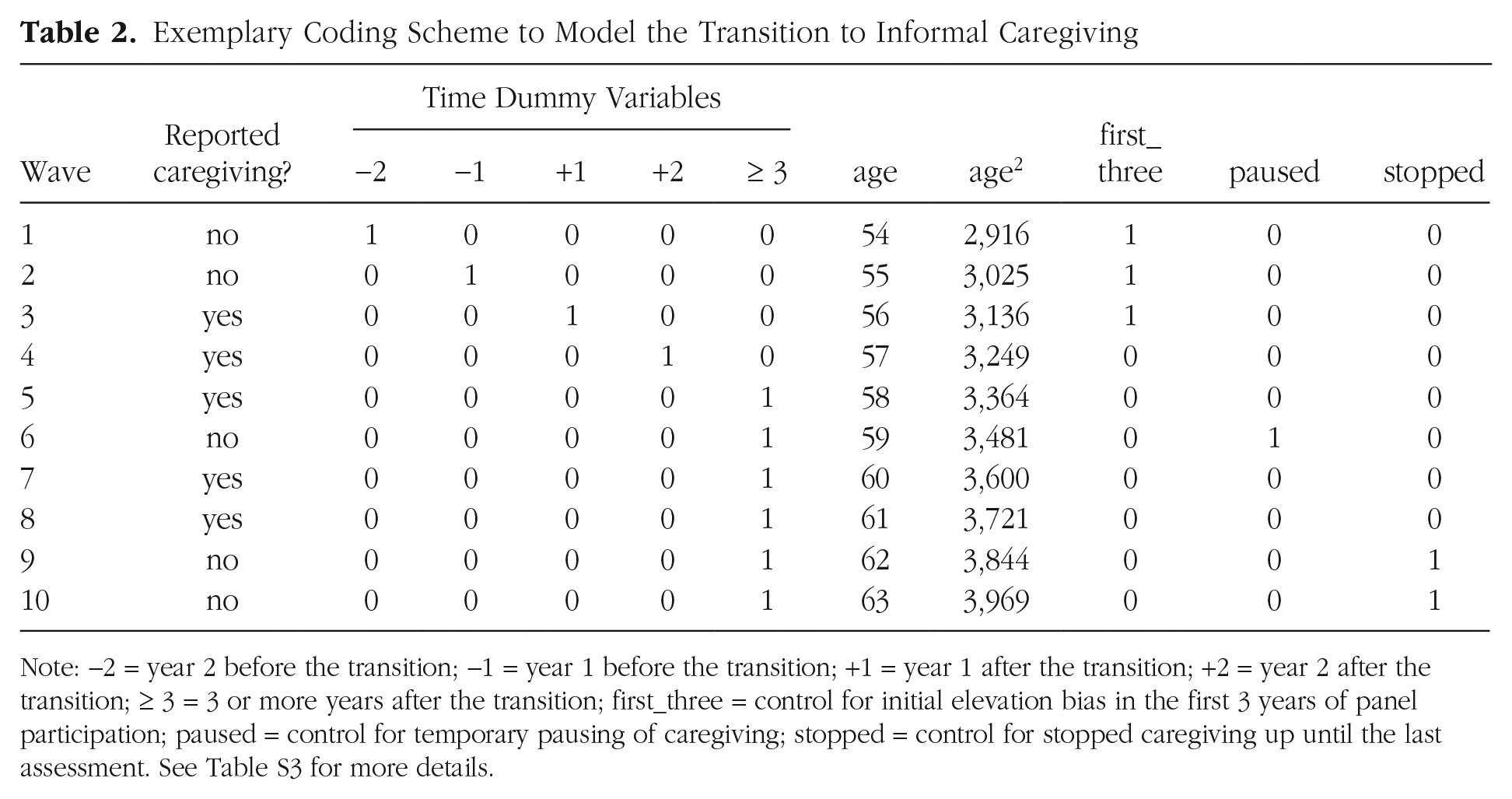
Note: −2 = year 2 before the transition; −1 = year 1 before the transition; +1 = year 1 after the transition; +2 = year 2 after the transition; ≥ 3 = 3 or more years after the transition; first_three = control for initial elevation bias in the first 3 years of panel participation; paused = control for temporary pausing of caregiving; stopped = control for stopped caregiving up until the last assessment. See Table S3 for more details.
Time spent on caregiving and moderators
To examine how changes in the time spent on informal caregiving affect well-being (Research Question 2), we included all observations with information on the time spent caregiving and used fixed-effects models with hours of caregiving as a linear predictor. Again, fixed-effects models analyzed within-person variance and, thus, gave an estimate of how a within-person change in the hours of caregiving related to changes in well-being. The formula for an exemplary model predicting life satisfaction (LS) reads:

Here,
Lastly, for moderation analyses (Research Question 3), an interaction term with the respective moderator was added to the model. For example,
Software
For fixed-effects modeling in R (Version 4.3.1; R Core Team, 2023), we used the plm package (Version 2.6-3; Croissant & Millo, 2008) with panel-robust (clustered) standard errors to account for nested data. Our main inference criterion was
Results
Effects of interest and their confidence intervals are shown in Figures 1, 2, and 3. The supplementary html document available on the Open Science Framework (https://osf.io/pwj6n) presents further information on variable distributions (Section 4.7) and complete model results (Sections 5.2–5.4).
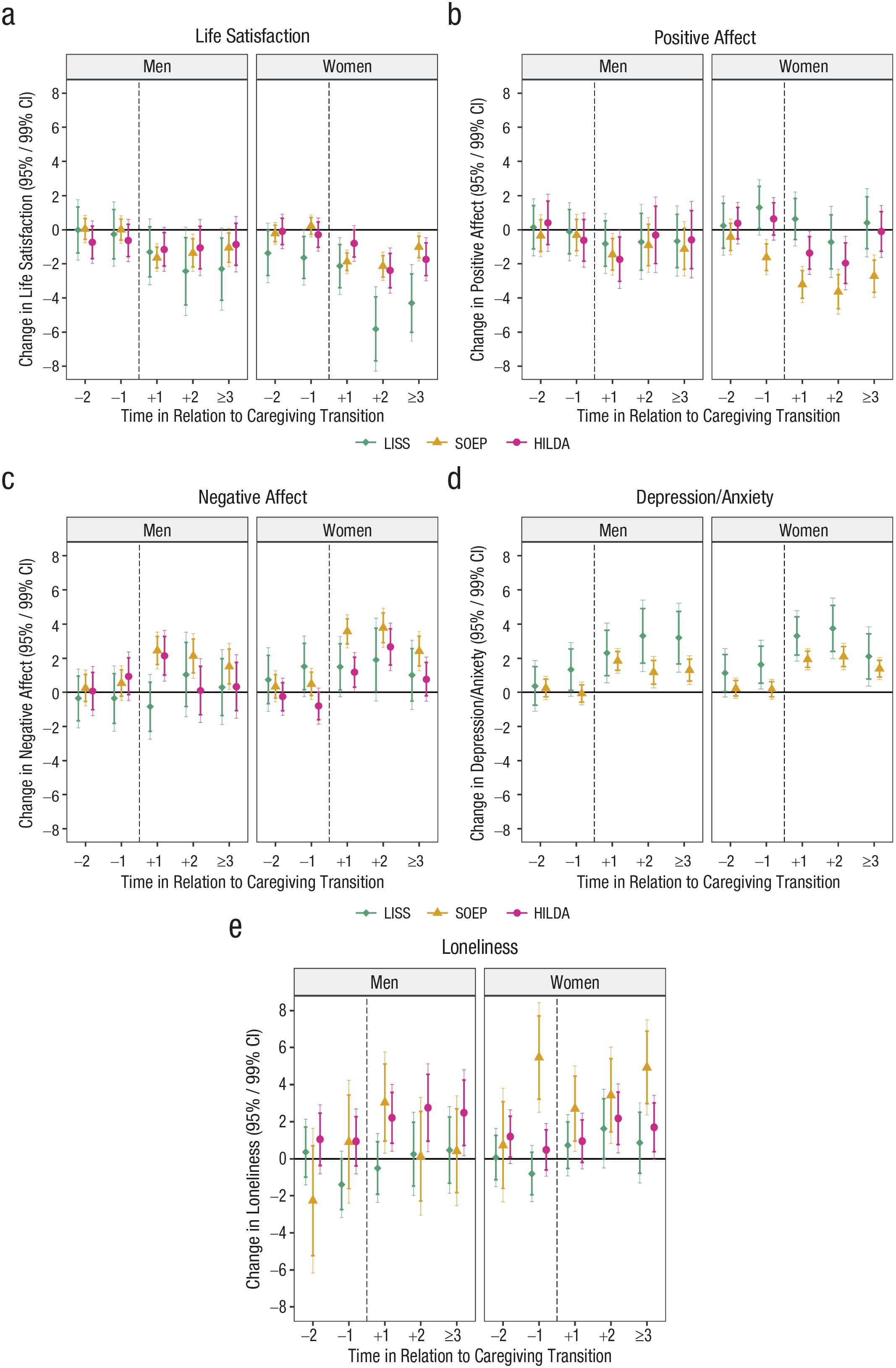
Well-being change trajectories over the transition to informal caregiving. Effects reflect changes in the well-being outcomes on the POMP scale from 0 to 100 (see Table S4). Confidence intervals (CIs; both 95% and 99%) reflect the precision of the estimated effects. The horizontal line indicates no within-person changes. The vertical dashed line indicates the approximate timing of the transition to informal caregiving. LISS = Longitudinal Internet Studies for the Social Sciences; SOEP = Socio-Economic Panel; HILDA = Household, Income and Labour Dynamics in Australia Survey.
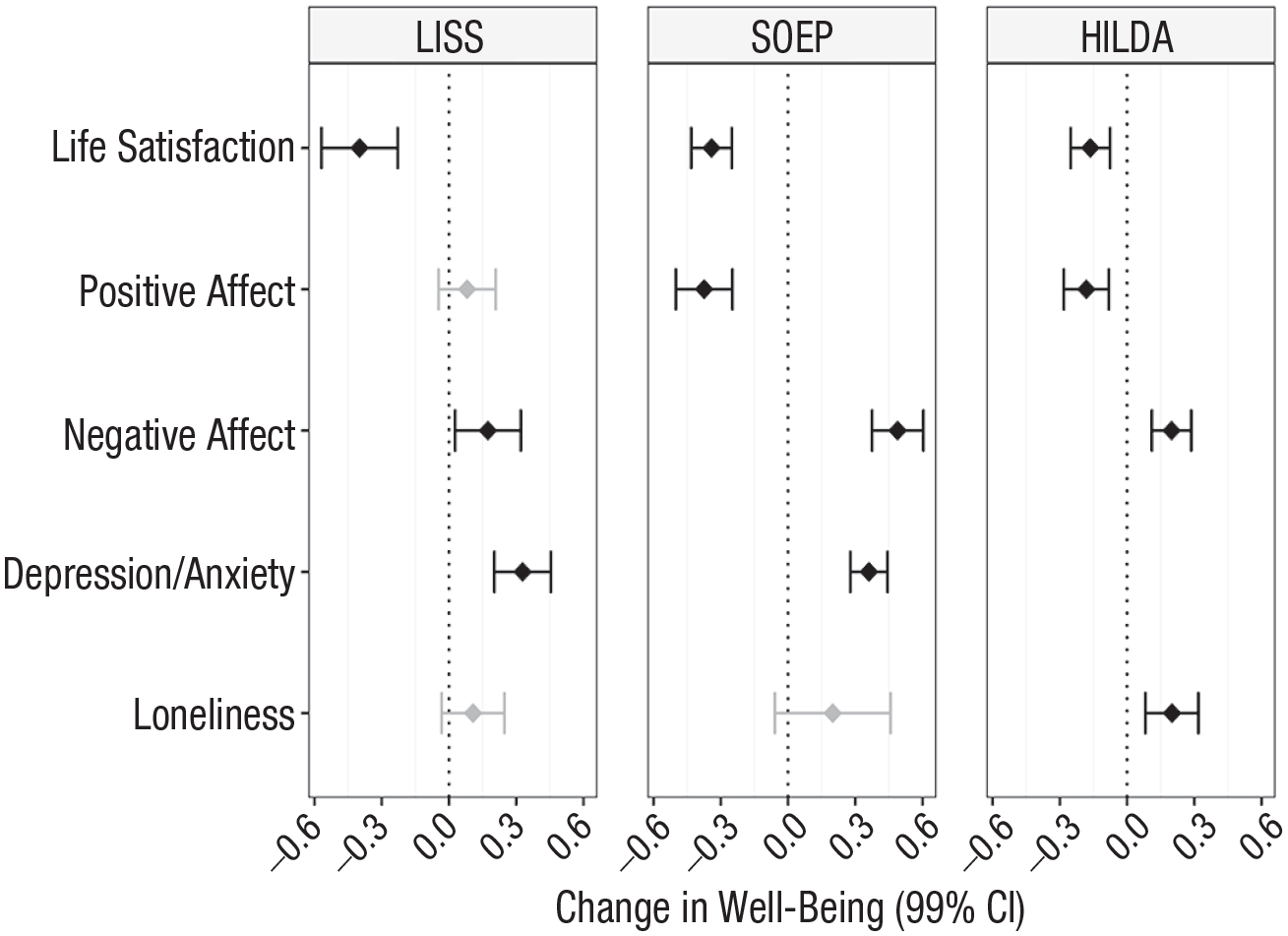
Effects of time spent on informal caregiving on well-being. Effects reflect a within-person increase of 1 hr per day and are reported on a POMP scale from 0 to 100 (see Table S5). CI = confidence interval (reflecting the precision of the estimated effect); LISS = Longitudinal Internet Studies for the Social Sciences; SOEP = Socio-Economic Panel; HILDA = Household, Income and Labour Dynamics in Australia Survey.

Moderators of the effect of time spent on informal caregiving on well-being. Anx. = anxiety. CI = confidence interval (reflecting the precision of the estimated effect); LISS = Longitudinal Internet Studies for the Social Sciences; SOEP = Socio-Economic Panel; HILDA = Household, Income and Labour Dynamics in Australia Survey.
Transition to informal caregiving
Descriptively, informal caregivers were more likely to be female, older, and slightly lower in well-being compared to respondents who never provided informal care (see Table S4).
Across the three samples, life satisfaction decreased in women when they started providing informal care (LISS: b = −2.13, 99% CI [−3.80, −0.46], p = .001) and did, on average, not recover when they continued caregiving (LISS: b = −4.30, 99% CI [−6.55, −2.05], p < .001; see Fig. 1a). In men, a life satisfaction decrease was significant in the SOEP only during the 2 years following the transition, b = −1.35, 99% CI [−2.45, −0.25], p = .002.
Similarly, in women, positive affect decreased during the transition to the caregiving role, but only in the SOEP and HILDA (SOEP: b = −3.21, 99% CI [−4.27, −2.15], p < .001; see Fig. 1b). In the SOEP, this decline was even present in the year before the transition, b = −1.61, 99% CI [−2.65, −0.57], p < .001. Men’s positive affect was slightly affected immediately after the transition in the SOEP and HILDA (SOEP: b = −1.44, 99% CI [−2.67, −0.21], p = .003).
Negative affect, on the other hand, increased in both men and women in the SOEP following the transition (women: b = 3.58, 99% CI [2.61, 4.54], p < .001; see Fig. 1c). Results from HILDA partly supported this finding; men increased in their negative affect in the year after becoming a caregiver, b = 2.15, 99% CI [0.67, 3.63], p < .001, and women in the 2 years after (“+2”: b = 2.67, 99% CI [1.29, 4.06], p < .001). In the LISS, both positive and negative affect did not change significantly.
Depression/anxiety increased in both the LISS and the SOEP once respondents became informal caregivers (women in LISS: b = 3.31, 99% CI [1.84, 4.78], p < .001) and remained high in later years when respondents remained involved in care (women in LISS: b = 2.11, 99% CI [0.38, 3.84], p = .002; see Fig. 1d). These effects did not differ by gender.
For loneliness, the LISS indicated no changes across the transition to informal caregiving (see Fig. 1e). SOEP respondents, however, and especially women, increased in loneliness when they became caregivers, b = 2.71, 99% CI [0.41, 5.01], p = .002; men only in the first year, b = 3.03, 99% CI [0.31, 5.76], p = .004, but women continually from the year before the transition to three or more years following the transition, b = 4.92, 99% CI [2.36, 7.48], p < .001. In HILDA, men and women increased in loneliness to a similar extent.
Taken together, we found relatively consistent well-being losses in women after they became informal caregivers and temporally specific well-being losses for men that partly did not extend beyond the first year of the transition to the caregiver role.
Time spent on caregiving
Next, we examined the well-being effects of changes in the time spent on caregiving. The majority of caregivers provided relatively low levels of care (Mdn = 0.57 hrs in the LISS, 2 hrs in the SOEP, with only whole hours reported, and 0.86 hrs in HILDA; see Table S5). Overall, with more time spent on caregiving, people reported slightly lower well-being (see Fig. S1).
Models of within-person change showed that well-being declined when people increased the time they spent on informal caregiving (see Fig. 2). Across the three samples, respondents consistently experienced lower life satisfaction when they increased the amount of time spent on caregiving (LISS: b = −0.40, 99% CI [−0.57, −0.23], p < .001). This effect was somewhat more pronounced in the LISS and SOEP compared to HILDA, b = −0.16, 99% CI [−0.25, −0.08], p < .001. In the SOEP and HILDA, respondents decreased in positive affect (SOEP: b = −0.37, 99% CI [−0.50, −0.25], p < .001) and increased in negative affect with increasing hours of informal caregiving (SOEP: b = 0.49, 99% CI [0.37, 0.60], p < .001). In LISS, there was also a similar, albeit smaller increase in negative affect, b = 0.17, 99% CI [0.03, 0.32], p = .002, whereas positive affect did not change. As respondents intensified the amount of informal care, their depression/anxiety worsened in the LISS and SOEP (LISS: b = 0.33, 99% CI [0.20, 0.45], p < .001). Finally, we only saw evidence for a significant rise in loneliness in HILDA as respondents increased the time spent on caregiving, b = 0.20, 99% CI [0.08, 0.32], p < .001. In the SOEP, the effect was of similar size but estimated with lower precision and therefore nonsignificant, b = 0.20, 99% CI [−0.06, 0.46], p = .047.
Follow-up analyses showed that quadratic effects of caregiving time were significant for all well-being outcomes except for loneliness and, in the LISS, positive and negative affect (see the html document Section 5.3.7.3 on https://osf.io/pwj6n). Initial increments in the time spent on caregiving (e.g., from 0 to 2 hrs) had a larger impact on well-being than increments in the middle range. However, quadratic effects were small overall and data points sparse in the upper range of hours (see the html document Sections 5.3.7.1-2, on https://osf.io/pwj6n).
Moderators of the effects of time spent on caregiving
Finally, we tested whether four theoretically derived moderators influenced how the time spent on caregiving affected well-being (see Fig. 3). First, we found inconsistent evidence for gender differences: In the SOEP and HILDA, but not the LISS, women experienced slightly more pronounced increases in negative affect with higher caregiving time (SOEP: b = 0.22, 99% CI [−0.04, 0.47], p = .029; HILDA: b = 0.14, 99% CI [−0.04, 0.33], p = .042). Second, in the SOEP only, caregivers experienced less severe increases in negative affect when they were involved in personal-care tasks (b = −0.25, 99% CI [−0.50, −0.0002], p = .00994; see Fig. S2a). There were no effects of type of care in the LISS and HILDA. Third, in the SOEP and HILDA, increases in negative affect were less pronounced when care was provided within the household (SOEP: b = −0.28, 99% CI [−0.48, −0.08], p < .001; see Figs. S2b and S2c). Fourth, effects did not differ between caregivers who were employed full-time or not.
Discussion
Psychological consequences of informal caregiving have been the topic of theoretical debate and empirical inquiry, although often in fields outside psychology and with mixed conclusions. We found that the adoption of an informal caregiver role has negative effects on mental health and on hedonic and interpersonal aspects of psychosocial well-being—across the Netherlands, Germany, and Australia. These negative effects were more marked in female than male caregivers—they were stronger and longer-lasting, and they affected more aspects of well-being. Spending more time on caregiving exacerbated well-being losses relatively evenly across genders, with suggestive evidence for more pronounced effects on women’s negative affect. Other social and contextual factors did not consistently moderate decreases in well-being. Overall, these results provide broad support for the propositions of stress theory (Pearlin et al., 1990), limited support for role-strain theory (Goode, 1960), and no support for well-being gains through caregiving (Kramer, 1997). These findings offer novel insights into the temporal process of well-being losses during caregiving, and the role of moderators.
Examining when informal caregiving affects well-being, we found that decreases in well-being during the first 2 years after adopting a caregiving role were the most pronounced and generalizable across samples and aspects of well-being. In contrast, well-being losses before the transition were less consistent and were mostly limited to female caregivers. Also, although adaptation effects set in for men, women continued to decrease in well-being with ongoing caregiving, especially in life satisfaction (Gerlich & Wolbring, 2021). Symptoms of depression and anxiety increased similarly in both male and female caregivers and remained elevated in later years (Oshio, 2014; Zwar et al., 2020). These findings contrast the idea of transient changes after life events as articulated in set-point theories of well-being (Diener et al., 2006).
Examining how informal caregiving affects well-being, we found robust evidence that decreases in well-being intensified as caregivers spent more time on caregiving tasks. This negative dose-response relationship is consistent with role-strain theory. Both primary caregiving stressors and secondary stressors might become more detrimental for well-being, for example, as satisfaction with leisure time decreases (Gerlich & Wolbring, 2021). An increase in caregiving hours may also reflect increasing health problems of the care recipient, which may amplify caregivers’ well-being losses.
Last, moderation analyses showed that both men and women experienced well-being losses with more time spent on informal caregiving, suggesting that women’s more pronounced long-term effects may be explained by their higher time investment (Hirst, 2005). Contrary to our expectations, neither care within the household nor personal-care tasks, both of which might involve higher daily stress (Lee et al., 2020), were associated with stronger decreases in well-being (Blaise & Dillenseger, 2023). Potential role conflicts from full-time employment also did not translate into differential well-being effects of caregiving time, refuting the hypothesis of role conflict from role-strain theory.
Implications
The present findings have theoretical and practical implications. First, the longitudinal results serve as an important stepping stone to more precise theories and rigorous research on the mechanisms through which informal caregiving affects changes in different aspects of psychosocial well-being. Still, future studies should comprehensively examine changes in caregivers’ psychological or eudaimonic well-being (Ryff & Keyes, 1995; Willroth, 2023). Second, a better understanding of the timeline at which negative well-being effects unfold can inform targeted interventions designed to reduce stress during the first two posttransition years. Third, targeted interventions may focus on female caregivers who tend to be more broadly affected than men, and for longer. Finally, considering the generally negative well-being effects of informal caregiving, policies designed to reduce the need for informal care through easier access to formal long-term care or combined forms of care may alleviate the detrimental effects of informal care (Verbakel, 2014).
Limitations
The current study had several limitations. First, a causal interpretation of the within-person effects rests on the assumption that there are no important time-varying confounds. For example, if changes in income affected both life satisfaction and the likelihood of providing informal care, estimates of caregiving on life satisfaction might have been biased (cf. Gerlich & Wolbring, 2021, where effects were robust to multiple such covariates). More advanced causal inference techniques that model confounding in the allocation to treatment in a time-varying manner may build on the current study (Chatton & Rohrer, 2024).
Second, we estimated average well-being effects using yearly panel data but did not model person-to-person heterogeneity beyond the tested moderators. Intensive longitudinal data would be needed to study the heterogeneity of daily-life processes by which caregivers’ well-being is affected, potentially through the accumulation of momentary stress (Gérain et al., 2023). Such data might also reveal certain circumstances under which caregiving is experienced as rewarding.
Third, we had limited information about additional moderators proposed by theory, such as the specific care situation (e.g., the perceived burden), the relationship with the care recipient (or multiple recipients), and their health status. The demands of conflicting roles, such as childcare, may exacerbate well-being losses. A more detailed longitudinal assessment of the care situation may help identify further moderators that shape informal care effects on well-being.
Last, results indicate similar well-being effects across the Netherlands, Germany, and Australia, although we did not formally test country-level differences. The current study primarily pertains to the socioeconomic and cultural contexts of Western, democratic countries. However, even within Europe, there are significant differences in the access to formal care that may affect caregiver health and well-being (Wagner & Brandt, 2018). Further, informal caregiving within the family might be seen as more normative in more collectivist contexts (Kalenkoski et al., 2022), raising questions about cross-cultural generalizability.
Conclusion
The current study demonstrates that informal caregiving on average affected caregivers’ well-being negatively. Across three nationally representative panel studies, informal caregivers, and especially women, decreased in their well-being after taking on this responsibility. Well-being further decreased in both men and women when they spent more time on caregiving tasks. Overall, these findings are most compatible with stress theory, but they also highlight a need for more explicit and precise theoretical groundwork in caregiving research to conceptualize the temporal processes and mechanisms underlying these effects.
Supplemental Material
sj-pdf-1-pss-10.1177_09567976241279203 – Supplemental material for The Well-Being Costs of Informal Caregiving
Supplemental material, sj-pdf-1-pss-10.1177_09567976241279203 for The Well-Being Costs of Informal Caregiving by Michael D. Krämer and Wiebke Bleidorn in Psychological Science
Footnotes
Acknowledgements
We thank everyone at the German Institute for Economic Research (DIW Berlin), Centerdata/Tilburg University, and the Melbourne Institute involved in making the data available to the research community.
Transparency
Action Editor: Amy Orben
Editor: Simine Vazire
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.