
Abstract
Background:
Homeless people present high rates of psychopathology, including personality disorders. Given the link between personality disorders and attachment, and the potential importance of these two traits for understanding homeless populations.
Aims:
Our aim was to review all studies focusing on attachment and on the full assessment of personality disorders in the homeless.
Method:
Overall, 213 studies were screened through title and abstract. Of these, 63 articles were chosen for full-text assessment.
Results:
A total of 14 articles met eligibility criteria and were included in the present review. Six studies evaluated personality disorders and eight studies assessed attachment in the homeless. In general, reports suggested that personality disorders are highly common in the homeless, with frequencies ranging between 64% and 79% for any personality disorder. The most common personality diagnoses were paranoid (14%–74%), borderline (6%–62%), avoidant (14%–63%), and antisocial (4%–57%) personality disorders. Attachment reports differed in the methods used and presented diverse results and correlates. Even so, insecure types of attachment dominated in the homeless, accounting for 62% to 100% of the samples.
Conclusions:
The high prevalence of personality disorders and insecure types of attachment in the homeless may impact intervention strategies for these people. The available literature evaluating attachment and the full assessment of personality disorders in the homeless is scarce, which supports the need for more research on these two topics.
Keywords
Public policy relevance statements
Given the link between personality disorders and attachment, and the potential importance of these two traits for understanding homeless populations, our aim was to review all studies focusing on attachment and on the full assessment of personality disorders in the homeless.
The high prevalence of personality disorders and insecure types of attachment in the homeless may impact intervention strategies for these people.
The available literature evaluating attachment and the full assessment of personality disorders in the homeless is scarce, which supports the need for more research on these two topics.
Introduction
Homelessness remains a global health concern in the 21st century. In the United States alone, around 550,000 people experienced homelessness on a single night in 2018 (Hossain et al., 2020). Other reports may present somewhat different values (Kidd & Shahar, 2008; Tsai, 2018), which may be related with the different definitions of homelessness (Monteiro Fernandes et al., 2022) used across studies.
Homeless people are one of the most vulnerable groups in society, and their past is usually not far better than their current situation. Histories of adverse childhood experiences, such as neglect, exposure to violence, divorce, loss, poverty, and physical or emotional abuse are highly common among homeless people (Herman et al., 1997; Koegel et al., 1995).
Early trauma can have lifelong consequences and may help explain the high levels of psychopathology that is usually found in the homeless (Fazel et al., 2008). For example, childhood physical abuse has been linked to the development of antisocial behavior (Afifi et al., 2019). Antisocial personality disorder (ASPD), as well as personality disorders as a whole, have been found to be highly frequent in homeless populations (Caton, 1995; Fazel et al., 2008; North, Pollio, et al., 1997; Rhee & Rosenheck, 2021).
Adverse childhood experiences can also influence an individual’s attachment style. Attachment theory, developed by Bowlby (1969), postulates that the interactions of an infant with his primary caregiver creates a base for personality development and shapes subsequent relationships. Ainsworth et al. (1978), using the Strange Situation (SS) procedure, identified different attachment styles, namely secure, avoidant, and anxious/ambivalent. In this experiment, infants were momentarily separated from their parents and left with a stranger in an unfamiliar setting. Secure infants were those that promptly explored the new environment under the care of the caregiver, were anxious in the presence of the stranger, were distressed with the parent’s brief absence, and rapidly sought contact with the caregiver after reunion, feeling reassured by renewed contact, and continuing exploration. Avoidant infants were those that ignored the caregiver’s return following separation, while anxious/ambivalent infants sought contact with the caregiver, but did not feel soothed by the contact. A fourth attachment style, termed disorganized, was later established (Westen et al., 2006). This style is characterized by an incoherent pattern of reaction toward separation and reunion and by a disorganized behavior.
One important feature of attachment patterns is their relative stability through adolescence and adulthood (Rodríguez-Pellejero & Núñez, 2018). For example, the agreement between childhood and adulthood attachment was shown to be between 68% to 75% in previous studies (Lorenzini & Fonagy, 2013).
Attachment styles in adults can be assessed by different methods, based either on narrative interviews or in self-reports. For this reason, attachment instruments in adults may sometimes measure different qualities (Westen et al., 2006). For example, the Adult Attachment Interview (AAI) is a narrative-based interview in which respondents provide five adjectives describing their relationship to each parent and then justify their choice with specific memories (Riggs et al., 2002). With this method, attachment styles are assessed by examining narrative’s coherence, instead of its content. The four styles of attachment assessed by this method are secure, dismissing, preoccupied, and unresolved. Securely attached individuals are those that can support their descriptions with specific examples, not idealizing nor did remaining preoccupy with early parental figures. Dismissing adults (corresponding to avoidant attachment in children) tend to minimize attachment importance, by idealizing painful relationships, or derogating attachment figures. Preoccupied individuals (corresponding to anxious/ambivalent attachment in children) are vaguer in their descriptions, often presenting interruptions and distractions in their speech, as well as jargon and infantile wording. Unresolved individuals (corresponding to disorganized attachment in children) are those presenting affective disruption of coherence, confusion of time and place, and long silences. These individuals usually have early histories of trauma, separation and loss that have not been properly resolved.
The Relationship Questionnaire (RQ) is another method available to explore adult attachment (Bartholomew & Horowitz, 1991). This is a self-report based questionnaire consisting in the rating of four paragraphs by respondents, each describing different patterns of attachment namely secure, dismissing, preoccupied, and fearful. Participants’ ratings are performed using a 7-point scale, ranging from 1 (‘not at all like me’) to 7 (‘very much like me’). Securely attached individuals are those having high rates on the paragraph corresponding to emotional closeness with others, having comfort in depending on others and with having others depend on oneself. Dismissing individuals avoid and devalue closeness of others, preoccupied attachment corresponds to a need to be accepted and validated by others and fearful attachment corresponds to avoidance of others due to fear of rejection.
Previous studies have related insecure attachment patterns with personality disorders (Westen et al., 2006). For example, Brennan and Shaver (1998) found a significant degree of overlap between attachment styles and personality disorders, and found that insecure individuals had doubled the chance of having a personality disorder when compared to secure individuals (39% vs. 75.0%). Rosenstein and Horowitz (1996) found that dismissing adolescents had greater risk for narcissistic and antisocial personality disorders, while preoccupied adolescents were more likely to have histrionic, borderline, and schizotypal personality disorders. Another study (Nakash-Eisikovits et al., 2002) found that fearful attachment was positively correlated with almost all personality disorders, but particularly with borderline personality disorder (BPD). They also found that avoidant attachment was strongly associated with Cluster A personality disorders (i.e. paranoid, schizoid, and schizotypal), while anxious/ambivalent attachment style was more associated with borderline, histrionic, and dependent personality disorders.
Last September we celebrated the twentieth anniversary of a seminal book dedicated to the plight of the homeless people in Lisboa, Portugal, Europe: ‘Sem-Amor Sem-Abrigo’. Translated to English would be ‘Loveless Homeless’, co-written by António Bento (MD, Psychiatrist) and Elias Barreto (MSc, Psychologist). Since then much has been written regarding homelessness, but to our knowledge, this book still presents an original and unique approach, by connecting homelessness to the concept of lovelessness. While preparing his Master thesis in Psychology, Barreto interviewed a small sample of homeless people, mostly men, and found not a single case of secure attachment style. This zero prevalence of secure attachment style was much lower than expected, when compared to the general population. In other words, this meant that all individuals had an insecure attachment style, that is avoidant, ambivalent, or disorganized (Figure 1), and this was independent of their psychiatric diagnosis (Bento & Barreto, 2002).
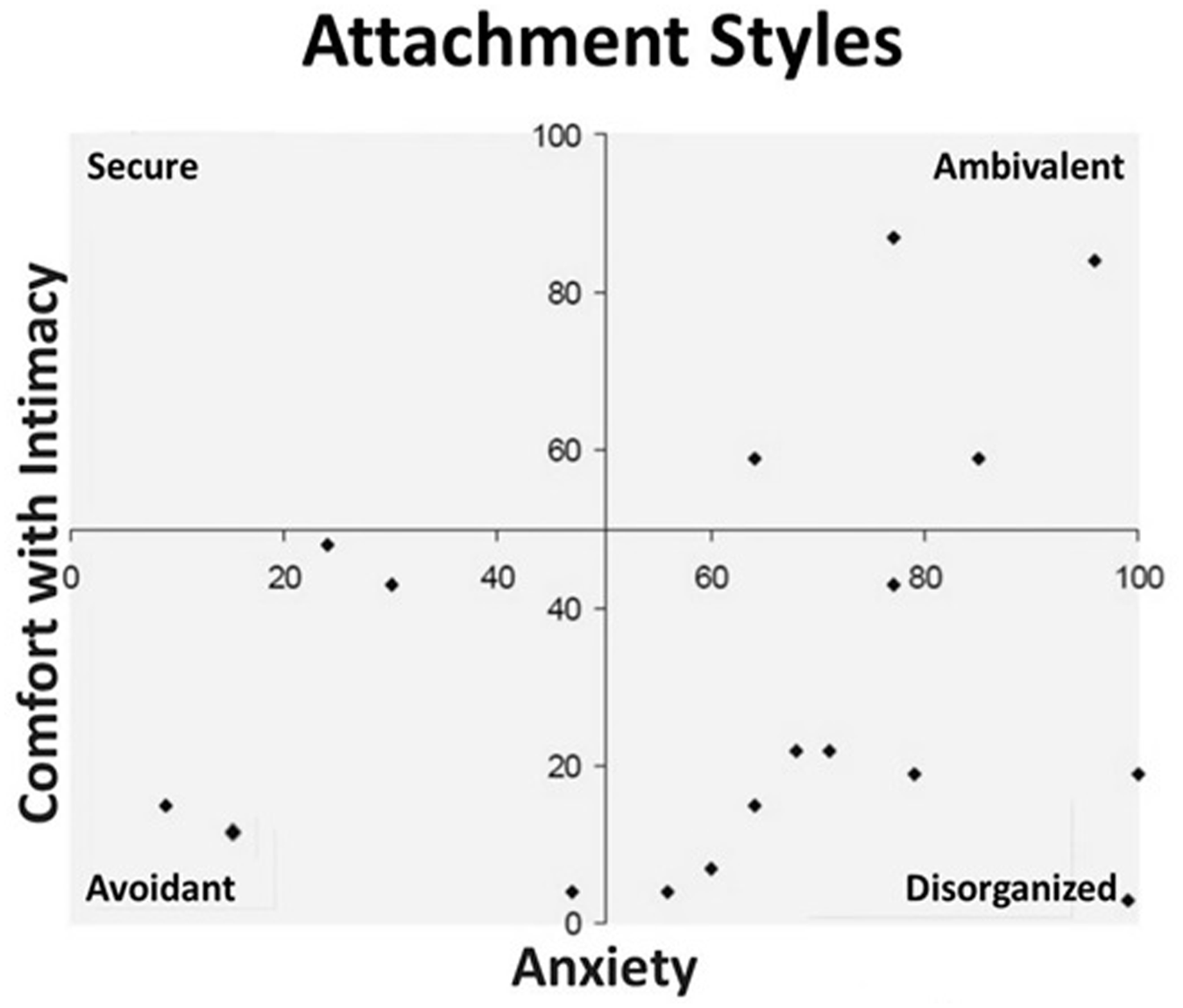
Attachment styles of a small sample of men living homeless in Lisboa.
Given the link between attachment and personality disorders, and the potential importance of both variables in understanding homelessness, the aim of the present study was to review all published literature focusing on attachment and on the comprehensive assessment of personality disorders in the homeless.
Methods
A search was conducted in PubMed database using the truncated terms ‘homeless*’, ‘attach*’, ‘personalit*’, and ‘temperament*’ (search details: (attach*[Title/Abstract] AND homeless*[Title/Abstract]) OR (personalit*[Title/Abstract] AND homeless*[Title/Abstract]) OR (temperament*[Title/Abstract] AND homeless*[Title/Abstract])). The search was last performed on the 5th of December of 2021. Since the available literature on the subject of attachment in the homeless is scarce, we considered any relevant studies published in English, regardless of date of publication, sample size, outcomes, comparators, or length of follow up as potentially eligible for this review. A similar approach was used for the subject of personality in the homeless, but in this case only studies focusing on three or more types of personality disorders in the homeless were included. The search yielded 213 results, which were screened by title and abstract. Off-topic articles were excluded, resulting in 63 articles for full-text assessment. Of these, seven articles concerning attachment in the homeless and six articles concerning personality in the homeless met eligibility criteria and were included in this review. We also searched for additional papers among the references of the articles obtained in the PubMed search, which resulted in an additional article for inclusion regarding attachment in the homeless. Figure 2 shows the flow diagram of the systematic review. General characteristics of the studies included in this review are summarized in Table 1.
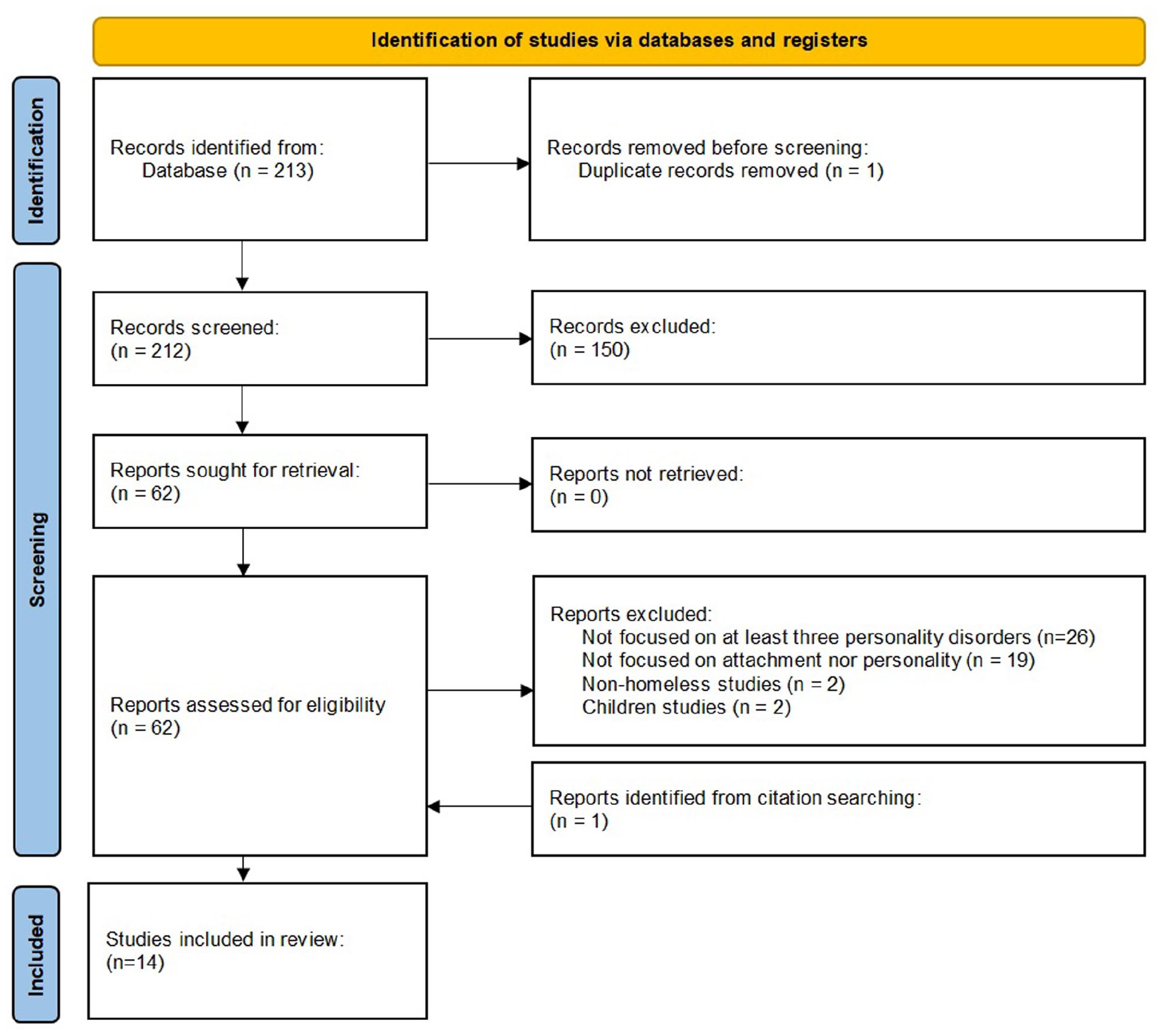
Flow diagram of the systematic review according to PRISMA.
General characteristics of the studies included in the present review.
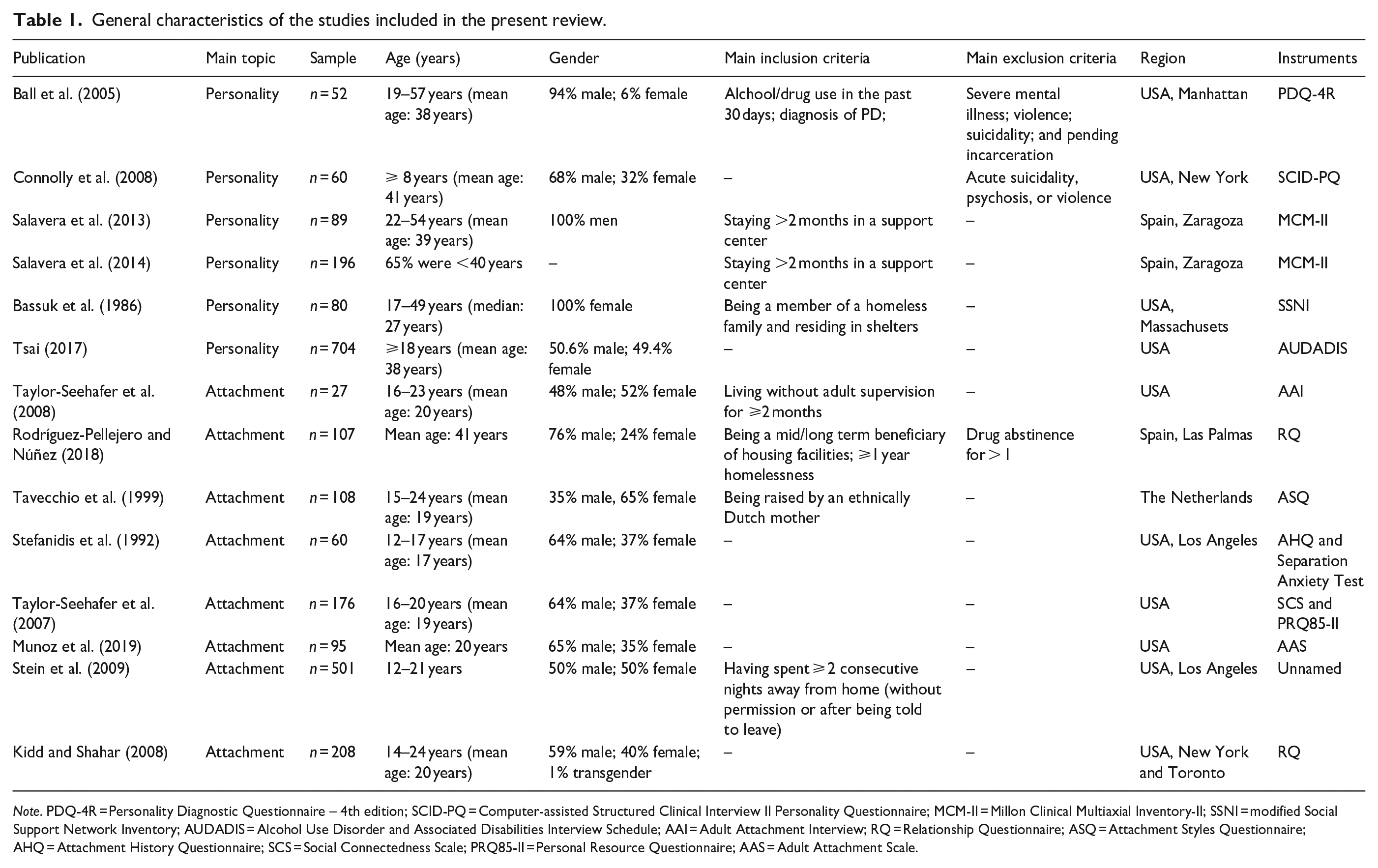
Note. PDQ-4R = Personality Diagnostic Questionnaire – 4th edition; SCID-PQ = Computer-assisted Structured Clinical Interview II Personality Questionnaire; MCM-II = Millon Clinical Multiaxial Inventory-II; SSNI = modified Social Support Network Inventory; AUDADIS = Alcohol Use Disorder and Associated Disabilities Interview Schedule; AAI = Adult Attachment Interview; RQ = Relationship Questionnaire; ASQ = Attachment Styles Questionnaire; AHQ = Attachment History Questionnaire; SCS = Social Connectedness Scale; PRQ85-II = Personal Resource Questionnaire; AAS = Adult Attachment Scale.
Results
Wide variability in the measurement of attachment and personality was found across studies. No study simultaneously reported on attachment and personality in the homeless.
Main results of the personality studies
The main results concerning personality in the homeless from the six personality studies included in this review are summarized in Table 2.
Main results of the studies concerning personality in the present review.
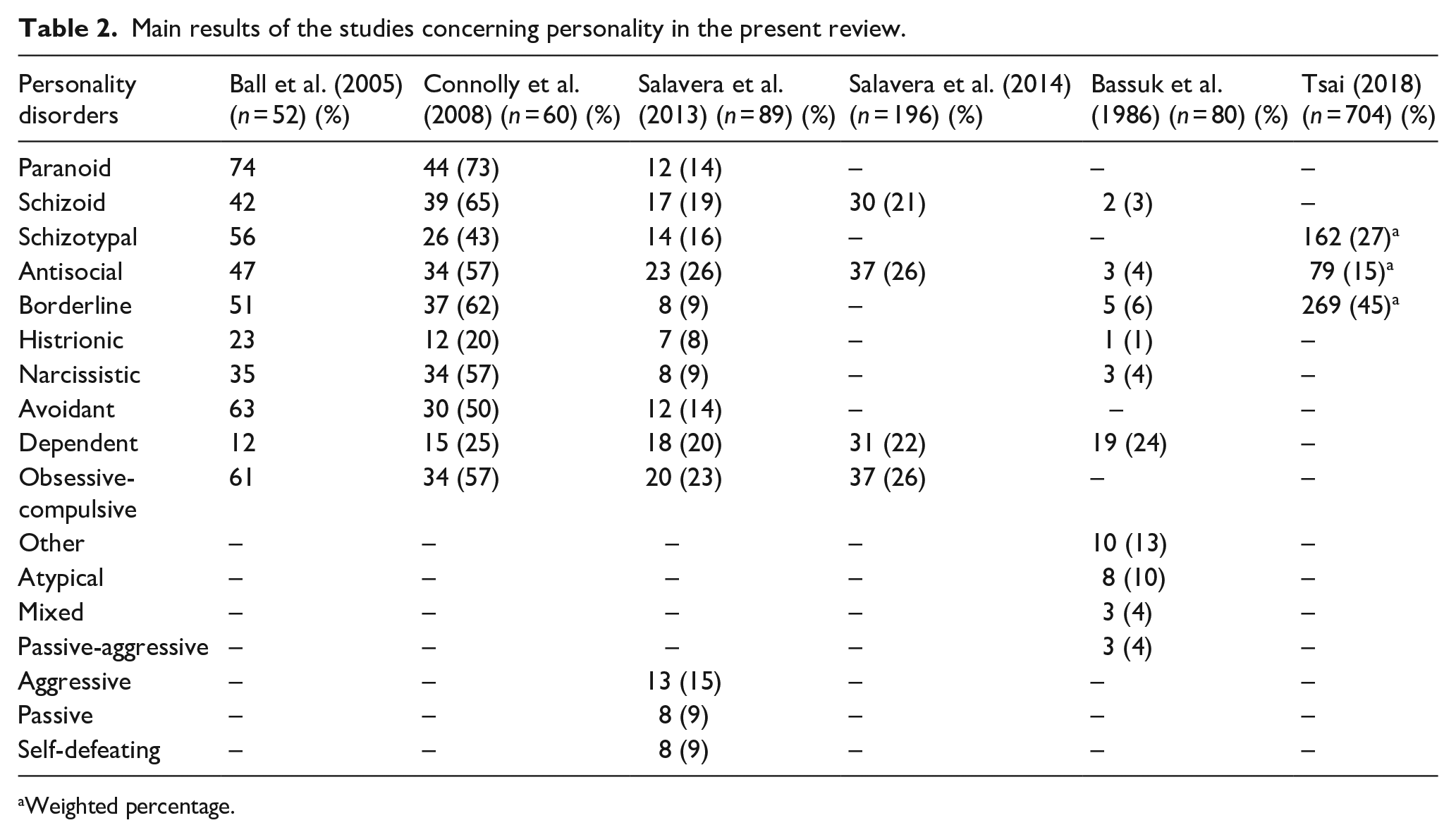
Weighted percentage.
The study from Ball et al. (2005), evaluated the psychiatric symptoms, psychosocial problems, and treatment response of 52 homeless individuals receiving services in a drop-in center in Manhattan. Alcohol or drug use in the past 30 days and a diagnosis of personality disorder were amongst the inclusion criteria. Participants were assessed in respect to personality disorders, substance use disorders, addiction severity, severity of psychiatric symptoms, interpersonal problems and early maladaptive schemas. Personality disorders were primarily assessed using the Personality Diagnostic Questionnaire – 4th edition (PDQ-4R; Koegel, 1988). Participants presenting a sufficient number of symptoms in the PDQ-4R were further evaluated regarding chronicity, pervasive maladaptivity, independence from other disorders and distress.
Cluster A disorders were found in 88% of the sample, with paranoid personality disorder being the most common (74%), followed by schizotypal (56%) and schizoid (42%) personality disorders. Cluster B disorders were found in 74% of the sample, with BPD (51%) and ASPD (47%) being the most frequent personality disorders. Cluster C disorders were detected in 85% of the sample, with avoidant (63%) and obsessive-compulsive (61%) being the most common diagnosis.
Additionally, using the family/social section of the Addiction Severity Index (ASI; McLellan et al., 1992), 54% of the participants reported not living with family, friends, or significant others over most of the previous 3 years. Most of the respondents reported periods of serious problems with their nuclear family (50%) or with a partner/spouse (63%) over their lifetime. History of physical abuse and sexual abuse was reported by 42% and 21% of the respondents, respectively.
In this study, after primary assessment, participants were randomly assigned to receive either individual psychotherapy (focused on personality disorder and substance abuse relapse prevention) or standard group substance abuse counseling. Follow-up assessments were however compromised by the inability to locate participants. Most of their sample failed to appear in treatment appointments and in drop-in center services, with 60% of participants abandoning treatment by the end of the first month.
A later study from the same team (Connolly et al., 2008), evaluated the prevalence of Axis I and II diagnoses, according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR), in a sample of 60 homeless adults receiving services at two drop-in centers in New York. They used Computer-assisted structured clinical interview to assess DSM-IV Axis I psychiatric disorders, while personality disorders were primarily assessed using the Computer-assisted Structured Clinical Interview II Personality Questionnaire (SCID-PQ; First & Gibbon, 2004). Each SCID-PQ endorsed item was then further evaluated regarding chronicity, pervasive maladaptivity, independence from Axis I disorders and distress.
The rates of specific Axis II disorders exceeded the rates of specific Axis I disorders, with over half of the personality disorders assessed having rates exceeding 50%. Almost all participants (92%) met criteria for at least one diagnosis of cluster A personality disorder (i.e. paranoid, schizoid, or schizotypal). Most of the participants (83%) met criteria for one of Cluster B personality disorders (i.e. antisocial, borderline, histrionic, or narcissistic) and around two thirds of the sample had at least one of Cluster C personality disorders (i.e. avoidant, dependent, or obsessive-compulsive). Multiple diagnoses were therefore the norm (average of 5.8, SD = 3.2).
Salavera et al. (2013, 2014) published two studies concerning personality disorders in the homeless. The study published in 2013 comprised 89 adult participants of a reintegration center in the Spanish city of Zaragoza (Salavera et al., 2013). To assess personality of the individuals they used the Millon Clinical Multiaxial Inventory-II (MCMI-II; Millon, 1997). This is a questionnaire consisting of 175 true or false questions ranking several personality diagnoses (i.e. schizoid, avoidant/phobic, dependent, histrionic, narcissistic, antisocial, aggressive/sadistic, compulsive, passive/aggressive, self-defeating, schizotypal, borderline, and paranoid personality disorders) as well as other clinical syndromes.
The most frequent diagnoses were antisocial (26%), compulsive (23%), dependent (20%), and schizoid (19%) personality disorders. Most of the participants (64%) had at least one personality disorder, while participants with two, three and four personality disorders accounted for 12%, 10%, and 19% of the sample, respectively.
The second study of Salavera et al. (2014) was published in 2014 and included 196 participants of a psychosocial insertion center in Zaragoza, Spain. In this case, the goal was to analyze the comorbidity of attention deficit hyperactivity disorder and personality disorders in the homeless. Personality of homeless individuals was again assessed using the MCMI-II (Millon, 1997).
Concerning personality disorders, antisocial (26%), dependent (22%), compulsive (26%), and schizoid (21%) personality disorders were the most frequent diagnoses. Overall, 79% of the sample showed one or more personality disorders and almost half of the individuals (49%) received three or more personality diagnoses.
A study from Bassuk et al. (1986) provided Axis-II diagnoses of 80 homeless mothers living in family shelters in Massachusetts. The personality diagnoses were obtained using a structured questionnaire, the modified Social Support Network Inventory (SSNI; Flaherty et al., 1983). Additionally, using a semi-structured clinical interview of about 260 items, further data was gathered from their sample, including developmental background, family disruptions, and patterns of violence (Bassuk et al., 1986).
Regarding personality, 71% of the homeless mothers presented a personality disorder, with the most frequent being dependent (24%) and atypical (10%) personality disorders. One-third of the participants reported being physically or sexually abused during their childhood and two-thirds of the sample reported experiencing a major family disruption (e.g. separation or divorce of the parents, death of a parent, mental illness and alcoholism of the parent, and state placement). Additionally, a third of the participants had never known their fathers. At the time of the interview, 26% of the respondents reported lacking a supportive relationship, 18% reported having one supportive relationship, and 20% reported having two supportive relationships.
Lastly, a study by Tsai (2018) used a representative sample of 36,299 US adults (⩾18 years) to determine the life-time and 1-year prevalence of homelessness in the United States of America (USA), while also evaluating its demographic and psychosocial characteristics, including the prevalence of three personality disorders (i.e. borderline, schizotypal, and antisocial). They used the Alcohol Use Disorder and Associated Disabilities Interview Schedule (AUDADIS), a structured diagnostic tool, to assess substance use disorder as well as selected personality and other psychiatric disorders, according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria (Grant et al., 2015).
A total of 1,683 individuals reported not having a place to live for more than 1 month sometime in their lifetime, while 704 respondents reported being homeless sometime during the previous year. Compared with the remaining sample (n = 35,595), past-year homelessness respondents presented a higher prevalence of all the three personality disorders evaluated. BPD was the most common personality disorder, occurring in 45% of the past-year homelessness participants and in 11% of the non-past year homelessness participants. Schizotypal and antisocial personality disorders were also more prevalent in the group of past-year homelessness individuals (27% and 15%, respectively) than in the remaining non-past year homelessness individuals (6% and 2%, respectively).
Main results of the attachment studies
Taylor-Seehafer et al. (2008) examined homeless youths’ perspectives on attachment, trauma, and substance use. The sample consisted of 25 homeless individuals, reaching for health or social services, and living without adult supervision for 2 months or more. Attachment was assessed using the AAI (Riggs et al., 2002). Participants were classified as secure – autonomous, insecure – dismissing, insecure – preoccupied, insecure – cannot classify or unresolved. The ‘cannot classify’ group included adolescents that did not present a consistent strategy, showing instead a mix of secure – autonomous, dismissing, and preoccupied strategies. Participants placed in the ‘unresolved’ category were also assigned to one of the other groups (i.e. secure, dismissing, preoccupied, or cannot classify).
Authors found the sample to be highly traumatized, with 74% of the participants reporting emotional abuse, 70% reporting physical abuse, and 55% reporting sexual abuse. None of the participants presented a secure attachment style. Instead, participants were distributed as follows: 4 were classified as dismissing, 1 was classified as preoccupied, 15 were classified as unresolved, and 5 were assigned the ‘cannot classify’ as a primary attachment pattern. Most of the sample (78%) scored low to average social connectedness and 82% reported moderate to high alcohol or other drug abuse. No statistically significant correlations were found for attachment pattern, social connectedness, and alcohol or other drug use/abuse, probably due to the small sample size, as authors stated.
A study by Rodríguez-Pellejero and Núñez (2018) determined the prevalence of adult attachment styles and executive dysfunction in a sample of homeless individuals, and analyzed the relationship between type of attachment and executive dysfunction, to determine if different types of attachment could predict executive functioning. The sample consisted of 107 Spanish homeless individuals assisted in housing facilities between 2013 and 2015. Attachment was evaluated using the Spanish adaptation of the RQ (Yárnoz-Yaben & Comino, 2011). Attachment styles were secure, dismissive – avoidant, preoccupied, and fearful – avoidant. Executive functioning was assessed with the Spanish version of the Dysexecutive Questionnaire (DQ; Llanero-Luque et al., 2008), which consists of five dimensions: inhibition, intentionality, executive memory, and two factors related to emotional and personality changes.
Insecure types of attachment were the most prevalent in this sample, with 63% of the subjects self-identifying with one of the three insecure attachment styles. The distribution of the sample by attachment style was the following: 22% were classified as dismissive-avoidant; 18% were classified as preoccupied, 22% were classified as fearful – avoidant and 37% were classified as secure. Executive dysfunction was also common in this sample (44%). There was a negative and significant correlation between secure attachment style and all dimensions of executive dysfunction, namely inhibition (r = −.31, p < .01), intentionality (r = −.28, p < .01), executive memory (r = −.22, p < .05), positive affect (r = −.20, p < .05), and negative affect (r = −.45, p < .01). There was a positive and significant correlation between some insecure attachment styles (i.e. preoccupied and fearful) and the dimensions of intentionality (r = .28, p < .01 and r = .20, p < .05, respectively), executive memory (r = .26, p < .01 and r = .37, p < .01, respectively), and expression of negative affect (r = .29, p < .01 and r = .38, p < .01, respectively). Only dismissive-avoidant attachment style had no significant correlations with any of the executive dysfunction dimensions.
Tavecchio et al. (1999) published a study comparing homeless youths (n = 108) with residential youths (n = 85) and youths from the standard population (n = 1,228) in terms of family background, parenting style, experiences of separation and loss, and quality of the attachment relationship. The age of the participants in the three groups was between 15 and 24 years. The responsiveness of the parents was measured with the Parental Bonding Instrument, consisting of 25 questions about parents’ care and control in the first 16 years of the participant’s life (Parker et al., 1979). Using the Attachment Styles Questionnaire (ASQ; Hazan & Shaver, 1987) authors measured the opinions of the participants about themselves and their social environment. Four attachment styles were distinguished, namely secure, avoidant, ambivalent, and disoriented attachment.
Over half of the residential and homeless youths experienced their first separation before age 10. Homeless youths experienced the least care and the most control from both father and mother (p < .001, for the difference of the three groups by analysis of variance). Only 13% of the homeless youths described themselves as securely attached. The percentage was higher for the general population group (33%) and the residential group (23%). The securely attached youths perceived both parents as more caring and as less controlling than the insecurely attached participants (p < .001, by analysis of variance).
In this study the social network of the three groups was also evaluated using the Personal Network (PN, representing the degree to which the participant reports being supported in relationship problems by 10 explicitly-named family and friends network members; Tavecchio et al., 1999) and the Social Support Questionnaire-6 (SSQ-6), measuring the perceived social support by the number of people available in six specified problem situations, and the satisfaction felt with that support; Sarason et al., 1983). They found that the homeless youths scored lower than the residential and standard population groups in terms of social network, for both family and friends factors. According to SSQ-6 results, homeless youths reported a smaller number of supportive people available to them when compared with residential youths.
A study from Stefanidis et al. (1992) explored homeless youths behavior using a sample of 60 homeless youths. Of these, 40 were Los Angeles Youth Network (LAYN) shelter residents and 20 were former LAYN shelter residents. Participants were distributed in three groups: a Stabilization-Responsive (SR) group, composed of shelter residents who actively pursued a stabilization goal, followed rules, voluntarily participated in activities, and were respectful and helpful to others; a Stabilization Non-Responsive (SNR) group, composed by residential youths who left the program prematurely, did not follow rules, missed appointments, and did not respect staff and peers; and a stabilized group, a control group of former runaways. Participants were evaluated by the Attachment History Questionnaire (AHQ) and the Separation Anxiety Test. The AQH was designed to assess basic areas of family life and the family interactions reflecting attachment between children and caregivers. The second test uses 12 pen-and-ink drawings depicting several situations that occur frequently in childhood and adolescence, and participants are asked to select applicable responses to specific situations, to generate patterns of response. Attachment, individuation, and self-love-loss were the patterns of response evaluated (Stefanidis et al., 1992).
Stabilization Non-Responsive youths had less positive attachment histories and were less able to reintegrate into society. The stabilized group and the SR group were similar in their attachment histories and were significantly different from the SNR group. Differences were also found in all patterns of the Separation Anxiety Test, with the SNR group scoring below normal range for attachment but showing scores consistent with self-love-loss and individuation. Stabilized and SR youths showed greater need for care and attention from caregivers than did the SNR group. SNR youths were less engaged with caregivers than were SR youths, and more frequently adopted an uninvolved attitude toward their homelessness and helping staff.
Another study from Taylor-Seehafer et al. (2007) evaluated attachment and sexual health behaviors in homeless youths using a sample of 176 individuals. The Social Connectedness Scale (SCS) and the Personal Resource Questionnaire (PRQ85-II; Weinert, 1987) were the relevant instruments in terms of attachment assessment. The PRQ85-II is a global measure of perceived social support based conceptually on a multidimensional model of relational functions, namely attachment/intimacy, social integration, opportunity for nurturance, reassurance of worth, and availability of assistance from others (Taylor-Seehafer et al., 2007).
Social connectedness and social support were highly correlated with each other (r = .44, p < .01), but correlated differently with the remaining variables in the study. For instance, social connectedness was significantly correlated with time being homeless (r = .28, p < .01), while social support significantly correlated with sexual self-concept (r = .18, p < .05), intention to use condoms (r = .22, p < .01), and self-efficacy to use condoms (r = 0.42, p < .01).
Munoz et al. (2019) searched for a dose-response relationship between exposure to Adverse Childhood Experiences (ACEs) and lower trust in the medical profession, in a sample of young adults. The sample was composed of 107 participants (95 completed all items on the survey), self-reporting as homeless and receiving services from an outreach program for young adults. ACEs were measured by the Adverse Childhood Experiences Scale (Felitti et al., 1998), which is a 10-item measure capturing the total number of ACEs experienced per respondent. Trust in the Medical Profession Scale (MPS; Hall et al., 2002) based on 11-items, was used to capture the respondent’s overall trust in the medical profession. Attachment was measured with the Adult Attachment Scale (AAS; Collins & Read, 1990), an 18-item measure that captures a person’s general comfort with closeness and dependency on others. The AAS contains three subscales, namely close, depend, and anxiety, with each subscale containing six items. Higher scores on the close and depend subscales indicate more comfort with being close to and depending on others, while higher scores on the anxiety subscale indicate more worry about being abandoned or unloved by others.
Respondents reported a high level of adult-perpetrated childhood trauma, with up to 90% of the homeless individuals reporting at least one ACE, and 73% reporting four or more ACEs. This contrasts with a general population sample (n = 17,337) where 64% of respondents reported one or more ACEs and 13% of respondents reported four or more ACEs. Hierarchical regression analysis using the covariates age, gender, ethnicity, and all three AAS subscales showed that only comfort in depending on others and attachment anxiety significantly predicted trust in the medical profession, with comfort in depending on others having a positive relationship, and anxiety toward others having a negative relationship. When also entering ACE scores as a block (one ACE, two ACEs, three ACEs, and four or more ACEs) all three AAS subscales were significant predictors of trust in the medical profession, with comfort in depending on and being close to others having a positive relationship, and anxiety demonstrating a negative relationship. All ACEs groups were significant predictors of lower trust in the medical profession.
Based on a sample of 501 homeless and runaway youths, Stein et al. (2009) searched for a differential protective effect of attachment to mothers and fathers in terms of youths’ recent problem behaviors. They hypothesized that positive attachments and relations with both mothers and fathers are important in mitigating adverse behaviors. Attachment theory was operationalized with one latent variable representing the quality of youths’ relationship with their mother and one representing the quality of youths’ relationship with their father. Each latent variable was constructed with six items: ‘I fight with her/him all the time’, ‘I do not respect my mother/father’, ‘She/he does not respect me’, ‘My mother/father loves me’, ‘My mother/father does not care for me’, and ‘I love my mother/father’. Possible responses varied between ‘strongly agree’ and ‘strongly disagree’. Reason for living home, substance use, criminal behaviors, survival sex, and psychological distress were also evaluated.
Positive attachments to parents had protective influences on problem behaviors and emotional distress. A good relationship with the father was significantly associated with a good relationship with the mother (r = .25, p < .001), decreased probability of leaving home due to abuse and violence (r = −.023, p < .001), less substance use (r = −.25, p < .001), less criminal behavior (r = −.24, p < .001), and less psychological distress (r = −.12, p < .05). A good relationship with the mother was associated with decreased probability of leaving home due to abuse and violence (r = −.28, p < .001), less psychological distress (r = −.18, p < .001), and less survival sex (r = .16, p < .01). A better relationship with the mother was associated with male gender (r = .19, p < .001), but no association between relationship with the father and gender of the participants was found.
A study from Kidd and Shahar (2008) examined the interactions between risk and resilience factors among homeless youths. The sample consisted of 208 youths, who either had no fixed address or were living in a shelter at the time of the survey. Attachment style was assessed using the RQ (Yárnoz-Yaben & Comino, 2011). Other variables included in their study were maltreatment, neglect, social involvement, self-esteem, and loneliness.
Secure attachment was positively associated with social involvement (r = .33, p < .001), self-esteem (r = .20, p < .01), and subjective health status (r = .23, p < .01) and was negatively associated with loneliness (r = −.17, p < .05), childhood sexual abuse (r = −.24, p < .001), childhood neglect (r = −.24, p < .001), and suicidal ideation (r = −.15, p < .05). Fearful attachment was positively associated with physical abuse (r = .16, p < .05), sexual abuse (r = .16, p < .05), neglect (r = .16, p < .05), sexual orientation (r = .18, p < .01), being bullied (r = .19, p < .01), sex trade involvement (r = .16, p < .05), loneliness (r = .23, p < .01), feeling trapped (r = .23, p < .01), and suicidal ideation (r = .23, p < .01), and negatively associated with social involvement (r = −.16, p < .05), self-esteem (r = −.19, p < .01), and subjective health status (r = −.16, p < .05). Preoccupied attachment was positively associated with sexual orientation (r = .15, p < .05), loneliness (r = .30, p < .01), feeling trapped (r = .23, p < .01), and suicidal ideation (r = .16, p < .05), and was negatively associated with social involvement (r = −.16, p < .05).
Discussion
As the authors did not conduct a meta-analysis, it is impossible to state which personality disorder is the most common type among the homeless. But, in general, the studies included in this review suggest that personality disorders are highly frequent in the homeless. Three out of six personality studies presented the overall proportion of personality disorders in the homeless (Bassuk et al., 1986; Salavera et al., 2013, 2014) and according to these studies, 64% to 79% of the participants presented a personality disorder. Another study, despite not reporting the overall proportion of personality disorders, found that 92% of the participants presented one of the DSM-IV-TR’s Cluster A diagnoses (Connolly et al., 2008). When comparing the overall prevalence of personality disorders in the homeless reported by the studies included in the present review with results from other studies not included in the present review due to the lack of assessment of at least three personality disorders, more modest results can be found in the excluded articles. For example, two previous reviews reported rates of personality disorders to be between 23% and 29% (Fazel et al., 2008; Schreiter et al., 2017). The discrepancy between the studies included in this review and the remaining literature is probably multifactorial and may be associated with the contrasting inclusion criteria of the individual studies, the different size of the samples, the particular methods used to evaluate personality disorders (Connolly et al., 2008) and the limited number of studies of the present review.
The frequency of the individual personality disorders varied between the studies. For example, schizoid personality disorder ranged from 3% to 65% (Ball et al., 2005; Bassuk et al., 1986; Connolly et al., 2008; Salavera et al., 2013, 2014), ASPD ranged from 4% to 57% (Ball et al., 2005; Bassuk et al., 1986; Connolly et al., 2008; Salavera et al., 2013, 2014; Tsai, 2018), BPD was between 6% and 62% (Ball et al., 2005; Bassuk et al., 1986; Connolly et al., 2008; Salavera et al., 2013; Tsai, 2018) and dependent personality disorder fluctuated between 12% and 25% (Ball et al., 2005; Bassuk et al., 1986; Connolly et al., 2008; Salavera et al., 2013, 2014). Of all personality studies included in this review, Salavera et al (2013) was the one presenting more middle ranged values. When comparing the prevalence of personality disorders in their sample of homeless individuals with data from the general population and from clinical samples, they still found a higher prevalence of personality disorders among their sample of homeless people.
Two articles, both from Salavera et al. (2013, 2014), found ASPD to be among the most frequent personality disorders. Given our inclusion criteria, several articles reporting solely on ASPD in the homeless were excluded from the present review (e.g. Caton et al., 1994; Crawford et al., 2011; Ferguson et al., 2015; Fletcher & Reback, 2017; Fond et al., 2019; Jainchill et al., 2000; McQuistion et al., 2014; North et al., 1993; North, Thompson, et al., 1997; Nower et al., 2015; Quimby et al., 2012; Reback et al., 2007). When evaluating the frequency of ASPD in the homeless reported by these additional studies, a high variation can be found between studies, with values ranging from 10% to 66%. In spite of this diversity, most of the excluded studies reported values between 20% and 40%, which is in agreement with the values reported in the two studies of Salavera et al. (2013, 2014).
ASPD is not only a frequent diagnosis in the homeless, but also an important one. This personality disorder was found to be related with an earlier onset of homelessness, chronicity of homelessness, poorer utilization of homeless services and less positive outcomes after discharge (Caton, 1995; North et al., 1998; North, Pollio, et al., 1997; Pollio et al., 1997). However, the fact that ASPD was not the most frequently identified personality disorder in all the personality studies included in the present review highlights the importance of carefully evaluating the full range of DSM-IV-TR’s Axis II disorders in the homeless. Nevertheless, caution should be taken, whenever interpreting these results. ASPD may include people with primary anti-social behavior (psychopaths), with a more genetic influenced personality disorder, but also people with secondary anti-social behavior (sociopaths) with a more environment influenced personality disorder. Anyway, both ways will help surviving in the streets, for sure.
The other most frequent personality disorders in the homeless according to the personality research reports included in this review were paranoid personality disorder, which accounted for ⩾ 73% of the participants in two studies (Ball et al., 2005; Connolly et al., 2008), avoidant and obsessive-compulsive personality disorders, each accounting for > 50% of the participants in two studies (Ball et al., 2005; Connolly et al., 2008) and BPD, which occurred in > 45% of the participants in three studies (Ball et al., 2005; Connolly et al., 2008; Tsai, 2018). Again, we cannot be sure if paranoid, avoidant, or even obsessive compulsive personality disorders are cause or consequence of being homeless. All this three personality disorders may be mimicked by survival street behavior. For example, a person experiencing homelessness can perfectly assume an avoidant and/or paranoid to avoid conflicts with other people. On the other hand, obsessive compulsive personality disorder can be mimicked by a hoarding behavior, especially with food or other essential items, in order to increase the chances of survival.
Personality disorders can have an impact on treatment programs for the homeless. For example, in one study (Salavera et al., 2013) all patients presenting BPD or personality limit and passive disorder abandoned treatment, while patients with dependent personality disorder or self-destructive disorder had rates of abandonment of around 40%. Another study (Bassuk et al., 1986), in which the most frequent diagnosis was dependent personality disorder, found that several homeless mothers struggled to become autonomous. These mothers presented difficulties in holding jobs and in maintaining relationships with other adults and institutions.
Regarding attachment, the approaches varied between studies, with only two out of eight studies (Kidd & Shahar, 2008; Rodríguez-Pellejero & Núñez, 2018) using the same method namely, the RQ. This translated into different qualities being coded in some studies, as was expected (Westen et al., 2006).
Two studies showed the distribution of the different types of attachment in the homeless (Rodríguez-Pellejero & Núñez, 2018; Taylor-Seehafer et al., 2008). In one of these studies (Taylor-Seehafer et al., 2008) none of the 25 participants presented a secure attachment style, while in the other study (Rodríguez-Pellejero & Núñez, 2018), only 38% of the 107 participants presented a secure type of attachment. Despite not showing the distribution of attachment styles, an additional report (Tavecchio et al., 1999) found that only 13% of their homeless sample was securely attached. Additionally, when comparing their homeless sample with a general population sample and a sample of residential youths, they found higher values for secure attachment in the comparison groups (33% and 23%, respectively). Higher prevalence of secure attachment was also found in other studies evaluating attachment in non-homeless adults (Ainsworth et al., 2014; Bakermans-Kranenburg & van IJzendoorn, 2009). The lower values for secure attachment in the homeless found in the studies included in the present review may be related with higher rates of childhood trauma, childhood abuse, and unresolved childhood situations, which are more frequent in the homeless than in the general population, and which was found to be high in some studies of the present review.
In the studies showing the distribution of the different types of attachment in the homeless (Rodríguez-Pellejero & Núñez, 2018; Taylor-Seehafer et al., 2008), insecure attachment styles were differently distributed. While in the study of Taylor-Seehafer et al. (2008) the most common attachment style was unresolved attachment (60%), in the study of Rodríguez-Pellejero and Núñez (2018), both dismissive-avoidant (22%) and fearful-avoidant (22%) were the most common types of attachment. All these insecure attachment styles may represent an obstacle to psychosocial rehabilitation, favoring homelessness chronicity (Rodríguez-Pellejero & Núñez, 2018).
Homeless people have impaired capacity to trust other people, authority figures, and institutions, probably due to their early trauma experiences. For example, Munoz et al. (2019) found that even a single ACE can lower trust in the medical profession. Stefanidis et al. (1992) reported that their subgroup of stabilization non-responsive homeless youths were mistrustful of close relationships and afraid of allowing themselves to rely on others. They also stated that this subgroup often rejected help from others in order to avoid being rejected. The provision of specific and timely supportive social networks to homeless youth can, however, prevent the generalization of the lack of trust created by past experiences, as stated in Tavecchio et al. (1999). Additionally, homeless people can establish important relations with other homeless counterparts. For example, the study of Taylor-Seehafer et al. (2007) found a direct relationship of time being homeless and social connectedness. They related this finding with the fact that the street family or peer subgroup may provide important attachment experiences for homeless youth.
Some studies evaluated the factors leading to homelessness. Salavera et al. (2013) listed the following factors, in decreasing order of importance: additions, problems with family of origin, divorce, labor problems, and psychological problems. Parents’ divorce and the lack of perceived parental responsiveness and emotional support were pointed as particularly important for the development of homelessness in the article of Tavecchio et al. (1999). The study of Bassuk et al. (1986), which evaluated personality disorders in homeless mothers, found that besides external factors (e.g. poverty), psychosocial factors, especially family breakdown, play an important role in family homelessness.
The seminal work by Bento and Barreto (2002) suggested that attachment disorder may have a role in the psychopathology of homeless people living with mental illness, probably in a transverse mode, independently of diagnose or comorbidity. As insecure attachment has been correlated with oxytocin disorders (Caicedo Mera et al., 2021), there might be a promising opportunity for this hormone as a new type of psychopharmacological treatment in psychiatry (Buchheim et al., 2009; Marazziti et al., 2006; Martins et al., 2016). Bento and Barreto (2002) have been working with homeless people with mental illness, with different organizations, for a large number of years that altogether surpass the fifty years mark. To this day, they provide scientific literature regarding mental illness of homeless people, contributing to Portuguese studies (Monteiro Fernandes et al., 2022) and European guidelines (Barreto et al., 2019). Bento and Barreto (2002) could easily be considered our charismatic leaders who could bring people together and who held on to a vision, two of a kind of that homelessness needed champion especially in non-housing agencies such as the health authority (Pannel & Parry, 1999). Homeless patients living with severe psychiatric disorders in Portugal, like any part of the world, are usually super difficult patients (Gama Marques, 2021), with high somatic comorbidity (Gama Marques & Bento, 2020b), living in the streets, many times anonymous (Gama Marques & Bento, 2020a).
The present review presents some limitations. First, it was impossible to register the protocol of this systematic review. On the other hand, there were no resources to conduct a proper meta-analysis. Nevertheless this article may catch the attention of other authors, opening an opportunity for future collaborations among clinicians and academics, giving birth to better protocols and studies regarding this issue.
For instance, the research reports included in this review do not allow generalization. The samples were relatively small in some studies, and the variables were diverse in the attachment studies. We also noted that the age groups of the participants differed between attachment and personality studies. While most of the attachment studies were performed in adolescent and young adults, the majority of personality studies were based in more middle-aged adults. An important limitation is that among the studies evaluating personality in the homeless, two teams contributed with two articles each. To avoid overrepresentations, ideally all studies should have been performed by different research groups.
The present review revealed there is scarce literature evaluating attachment and personality disorders in the homeless and supports the need for more research focusing on these two topics in homeless populations. Despite the few available studies published in English, we noticed references were made to articles published in other languages. Perhaps, more effort could be made to make such studies widely accessible.
Overall, the studies presented in this review suggest that homeless people suffer from high rates of several personality disorders and are mostly characterized by insecure types of attachment. These traits represent an obstacle for treatment intervention strategies and should be considered in advance when planning strategies are built to assist the homeless.
Footnotes
Acknowledgements
The authors would like to thank the Psychologist Elias Barreto, from Hospital Júlio de Matos, Centro Hospitalar Psiquiátrico de Lisboa, Lisboa, Portugal, for his insight to the research that underlies the present study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.