
Abstract
Background:
Many studies show that members of minority groups underutilize mental health services and report more barriers to such utilization than majority groups. However, very little is known about these barriers and their relation to mental health service use among the Palestinian-Arab minority in Israel.
Aims:
This study examined barriers to mental health service use in this population based on the stigma-related, attitudinal, and instrumental barriers dimensions of the Barriers to Care Evaluation scale (BACE v3) and its correlates to mental health service use.
Methods:
The participants were a convenience sample of 231 Palestinian Arabs. They completed measures of BACE v3, mental health service use, and sociodemographic characteristics.
Results:
The findings showed that participants who reported using mental health services had lower levels of barriers in all dimensions compared to those who did not use such services. Attitudinal barriers were found to be the main determinants of mental health service use.
Conclusions:
This study underscored the role of attitudinal barriers to the utilization of mental health services. The findings indicated that interventions addressing such barriers might be helpful in increasing mental health service use among the Palestinian-Arab minority in Israel as well as other minorities in Israel and elsewhere, who might share similar backgrounds and perceptions.
Keywords
Introduction
In recent decades, many studies have highlighted differences across various ethnic groups in mental healthcare, particularly the significantly lower rate of seeking and utilizing services among ethnic minority compared to majority groups, even among severely ill individuals (Abu-Kaf & Braun-Lewensohn, 2015; Alegría et al., 2018; Maura & de Mamani, 2017). Not seeking mental treatment could result in poorer health outcomes such as more mental disorder symptoms, higher risk of chronic illnesses, higher disability rates, and greater loss of productivity (Clement et al., 2012). Therefore, ensuring equality in access to mental healthcare is essential for improving outcomes across individuals from diverse ethnic origins (Alegría et al., 2018).
Studies attempting to explain the mental health service underutilization among minorities worldwide show that minority groups report more barriers than do majority groups, with some of these barriers being unique to their status as minorities and to their socioeconomic and cultural background (Fante-Coleman & Jackson-Best, 2020; Planey et al., 2019; Scheppers et al., 2006). These barriers include self-and social stigma; concerns about confidentiality and trust; cultural beliefs against treatment and preference for informal sources of help; cost and transportation problems; lack of cultural and linguistic adaptation of services; and experiences of group-based discrimination (Cheng et al., 2018; Fante-Coleman & Jackson-Best, 2020; Jorm, 2012; Maura & de Mamani, 2017; Planey et al., 2019; Scheppers et al., 2006; Ugarte Bustamante et al., 2020).
Exploring these barriers to mental health service use among minorities is essential for promoting usage by tailored intervention programs. Clement et al. (2012) developed the Barriers to Care Evaluation (BACE) scale, which classified the potential barriers into stigma-related, attitudinal, and instrumental barriers. Stigma-related barriers refer to the prejudices, discriminations and stereotypes related to mental disorders; attitudinal barriers refer to perceptions about mental health treatments such as perceived ineffectiveness, the tendency to try to solve the problem without help, or assuming the problem would go away; and instrumental barriers refers to technical problems, such as financial or transportation difficulties. Despite the growing interest in barriers to mental health service among ethnic minorities, only few studies have used BACE (Clement et al., 2012), and to the best of our knowledge, no prior study has yet assessed barriers to mental health service use among the Palestinian-Arab minority in Israel (hereafter, also Arabs).
Israel defines itself as a Jewish and democratic country. Most of its 9.3 million citizens are Jews, with a large minority of Arabs representing 21% of its population (Central Bureau of Statistics, 2021). The Arabs in Israel are distinct from the Palestinians in the West Bank and Gaza, formally governed by the Palestinian Authority, as they have Israeli citizenship. Most of the Arabs citizens in Israel live in Arab villages and cities, and only about 8% live in mixed Arab-Jewish cities. They are predominantly Muslim, with relatively smaller Christians and Druze groups (A’li, 2019).
Compared to most Jews in Israel, Arab society is relatively traditional and collectivist. Nevertheless, while many within it adhere to patriarchal and authoritarian norms, it has experienced significant sociocultural changes in recent years, such as increase in higher education rates and in the number of women integrated into the labor market (Abu-Asbah et al., 2014; A’li & Da’as, 2016; Haj-Yahia, 2019). Mental health-related issues are also affected by these sociocultural changes, leading to greater community acceptance of formal mental health services (Khatib & Abo-Rass, 2022).
The current rate of Arabs utilizing mental healthcare services in Israel is estimated at 21%, significantly lower than among Jews (39%; Elroy et al., 2017; see also Al-Krenawi & Graham, 2011; Struch et al., 2007). Specifically, Arabs represent only 7% of psychiatric rehabilitation services users (Diab & Sandler-Loeff, 2011). This percentage is a cause for concern because it is much lower than the Arabs’ share in the general population, and because the rates of mental health problems among them are significantly higher than in the Jewish population (Abu-Kaf, 2019; Abu-Kaf & Shahar, 2017; Nakash et al., 2012); for example, depression is 2.5 times more common among Arabs (Kaplan et al., 2010).
In addition, the socioeconomic and political contexts of the Arab society in Israel are considered important and interrelated determinants in mental health issues among them. For example, the political context of the Arabs as a minority and the intractable Palestinian-Israeli conflict, which involves both the Israeli military and the Jewish and Palestinian-Arab populations in Israel and the Occupied Territories, mean that they are subjected to ongoing stress, affecting their physical and mental health, as well as their economic situation (Abu-Kaf, 2019). Relatedly, the Arab minority experiences personal and institutional discrimination, so they have fewer job opportunities in their places of residence (Haj-Yahia, 2019), resulting in lower incomes and higher levels of unemployment (Central Bureau of Statistics, 2022).
Specifically, although mental health services in Israel are free subject to health insurance law for all citizens, they are less available in the Arabs villages and cities, and public transportation services in Arab areas are inadequate. Moreover, mental health services are not culturally adapted and include fewer Arab professionals, and Arab patients are less likely to seek treatment from Jewish therapists because of language, culture, and political differences (Al-Krenawi, 2019).
In terms of cultural and religious preferences, many Arabs worldwide attribute mental illness to supernatural causes or external events, rather than to biomedical factors (Gearing et al., 2013; Zolezzi et al., 2018). As in many other countries, Arabs in Israel, especially Muslims, are mostly religious and conservative (Nydell, 2018), with many perceiving mental disorders as a divine test or punishment and consequently seeking religious and spiritual help for their mental problems, whether exclusively or in addition to medical help (Ciftci et al., 2013; Koenig et al., 2014). Moreover, the Arab world is characterized by enduring stigmas against mental illness, the mentally ill, and non-traditional mental health treatments (Al-Krenawi, 2019; Zolezzi et al., 2018). Nevertheless, at least in Israel, researchers have indicated that despite this unique sociocultural context, traditional beliefs of local Arabs are changing, including in the mental health field (Abo-Rass et al., 2020a). For example, a study conducted recently on Arabs in Israel found that they reported moderate-to-high levels of mental health literacy, whereas specific dimensions of mental health literacy (knowledge of where to seek information and attitudes that promote recognition or appropriate help-seeking behavior) are significant determinants of mental health service use in this population (Abo-Rass & Abu-Kaf, 2023).
The current study
Based on the worrisome findings among the Arab minority in Israel and their unique sociocultural background, the aim of the present study was to examine the prevalence of the different barriers to mental health service use among this group and its correlates to mental health service use, using the BACE scale (Clement et al., 2012).
Method
Participants and procedure
A convenience sample of 231 Arab adults from Israel participated in the study. The inclusion criteria were (a) being over the age of 18 and (b) being an Arab citizen of Israel. The first author interviewed participants who had met the inclusion criteria face-to-face (n = 75), but also sent the questionnaire as an online link to other relevant participants (n = 156). Although a face-to-face meeting was held, the participants filled out the questionnaire on their own; the first author intervened only to clarify questions as required, taking care to be objective and not to bias the participants’ answer. The combined approach to data collection was adopted to ensure that not only internet users would fill out the questionnaire and thus perhaps bias the findings. On the other hand, our goal was to ensure the participation of potential participants who did not feel comfortable participating in a mental health study in the presence of another person, given the aforementioned mental health related-stigma prevalent in Arab society.
The first author initially interviewed participants who had met the inclusion criteria and who varied in terms of age, gender, education, marital status, and area of residence, and then asked them to refer her to other potential participants (snowball technique). Similarly, a questionnaire link was initially sent to several participants, who were asked to forward it to others. Prior to participating in the study, candidates were briefly interviewed to ensure that the snowball did not ‘roll down’ to the same population category.
Both types of interviews used a structured survey form that had been piloted with 15 participants for clarity. The first page in both the online and hardcopy version included a description of the study, an informed consent form, and the researchers’ contact details. Only participants who had signed the form or checked a box to indicate their agreement to participate could then complete the full survey. Because of the study’s online component, we could not determine the response rate. The research was approved by the Ethics Committee of the University of Ben-Gurion University.
Measures
Barriers to mental health service use
Barriers to mental health service use were assessed using BACE v3 (Clement et al., 2012). The scale consists of 30 items, which examine three dimensions of potential barriers: (1) Stigma-related barriers (12 items, e.g. ‘Concern that I might be seen as crazy’); (2) Attitudinal barriers (10 items; e.g., ‘Wanting to solve the problem on my own’); and (3) Instrumental barriers (8 items; e.g. ‘Problems with transport or traveling to appointments’). Each item refers to a specific barrier reported to have stopped, delayed, or discouraged an individual from receiving professional mental healthcare. All items were rated on a four-point Likert scale ranging from 0 = ‘not at all’ to 3 = ‘a lot’. Six items offered an additional option: ‘not applicable’. The scale has high validity, reliability, and acceptability for the total score (Clement et al., 2012).
Similar to previous studies (Ugarte Bustamante et al., 2020; Negash et al., 2020; Salaheddin & Mason, 2016), three overall indices were generated, for stigma-related, attitudinal and instrumental barriers, by averaging the relevant items of each dimension, with higher scores indicating a greater barrier (a mean score of 0 indicated that it was not rated as a barrier; 0–1 indicated a low barrier; 1–2 indicated a medium barrier; and 2–3 indicated a high barrier). In addition, a mean score was calculated for each item separately, as for the likelihood of rating each item as a barrier (the number and percentage of participants who answered 1, 2, or 3 for each item). The items considered normally distributed for social science and 4-Likert scale (skewness ranges: 0.23–4.79; Leung, 2011).
The scale was translated from English into Arabic using the back-and-forth method (Beaton et al., 2007; Guillemin et al., 1993). It showed high internal consistency for all dimensions (Cronbach’s alpha = .90, .80, and .81 for stigma-related, attitudinal, and instrumental-related barriers, respectively).
Sociodemographic characteristics
The participants’ sociodemographic characteristics were examined using a questionnaire that collected details about their gender, age, marital status, education, and income (above average, average, or below average in Israel). Respondents also reported whether they used mental healthcare services.
Data analysis
All data were coded and analyzed using SPSS Statistics 25. Descriptive statistics were used to describe the participants' characteristics and main variables. To assess sociodemographic differences between participants who reported using as opposed to not using mental health services, t and χ2 tests were performed. In addition, t-tests were employed to examine differences in BACE dimensions between the two groups.
A binary logistic regression analysis was conducted to examine the determinants of mental health service use. In the first step, sociodemographic variables found to be significantly related to mental health service use at the bivariate level were included as control variables. These variables were gender, marital status, and education. The second step included all barriers dimensions, since all were found significantly related to mental health service use. To assess for multicollinearity, we examined the variance inflation factor between all covariates and found values ranging from 1.45 to 2.36, reflecting the fact that there was no multicollinearity problem in the regression models.
Results
Sample description
Most (67.5%) of the participants were females, with a mean age of 35.94 years (SD = 10.82, range = 18–72), and their years of formal education averaged at 14.36 (SD = 4.40). Sixty-five (38.52%) of the participants reported mental health service use (see Table 1 for their service usage data). As can be observed, the majority of both service users and non-users were females. However, significant gender differences were found between users and non-users. Significant differences were also found in education and marital status, with better-educated participants reporting higher and married participants reporting lower use of mental health services.
Participants’ sociodemographic characteristics by mental health service utilization (N = 231).
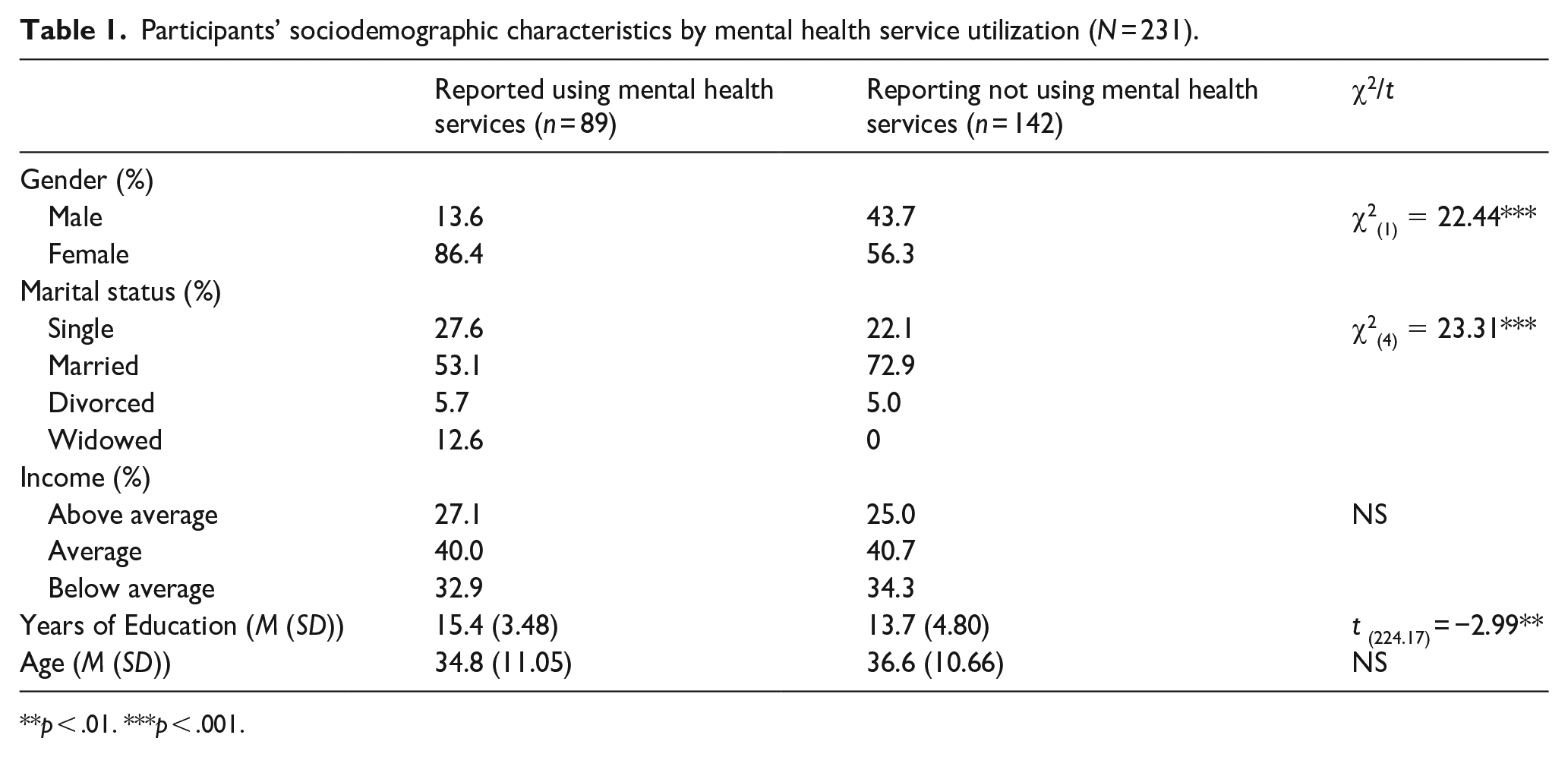
p < .01. ***p < .001.
Barriers to mental health service use
Table 2 lists the stigma-related, attitudinal, and instrumental barriers’ means, standard deviations, and differences between participants who reported using versus not using mental health services. As can be observed, relatively low levels of attitudinal, instrumental, and stigma-related barriers were reported by participants in both groups, as both rated them as low barriers. Participants also provided low ratings for all BACE scale items, meaning that more of them rated the barriers as low than as medium or high. However, statistically significant differences between the two groups were found in all three barriers dimensions. compared to participants who reported mental health service use, those who did not had higher levels of barriers in all dimensions (stigma-related, attitudinal, and instrumental barriers).
Barriers to mental health service utilization among Arab participants (N = 231).
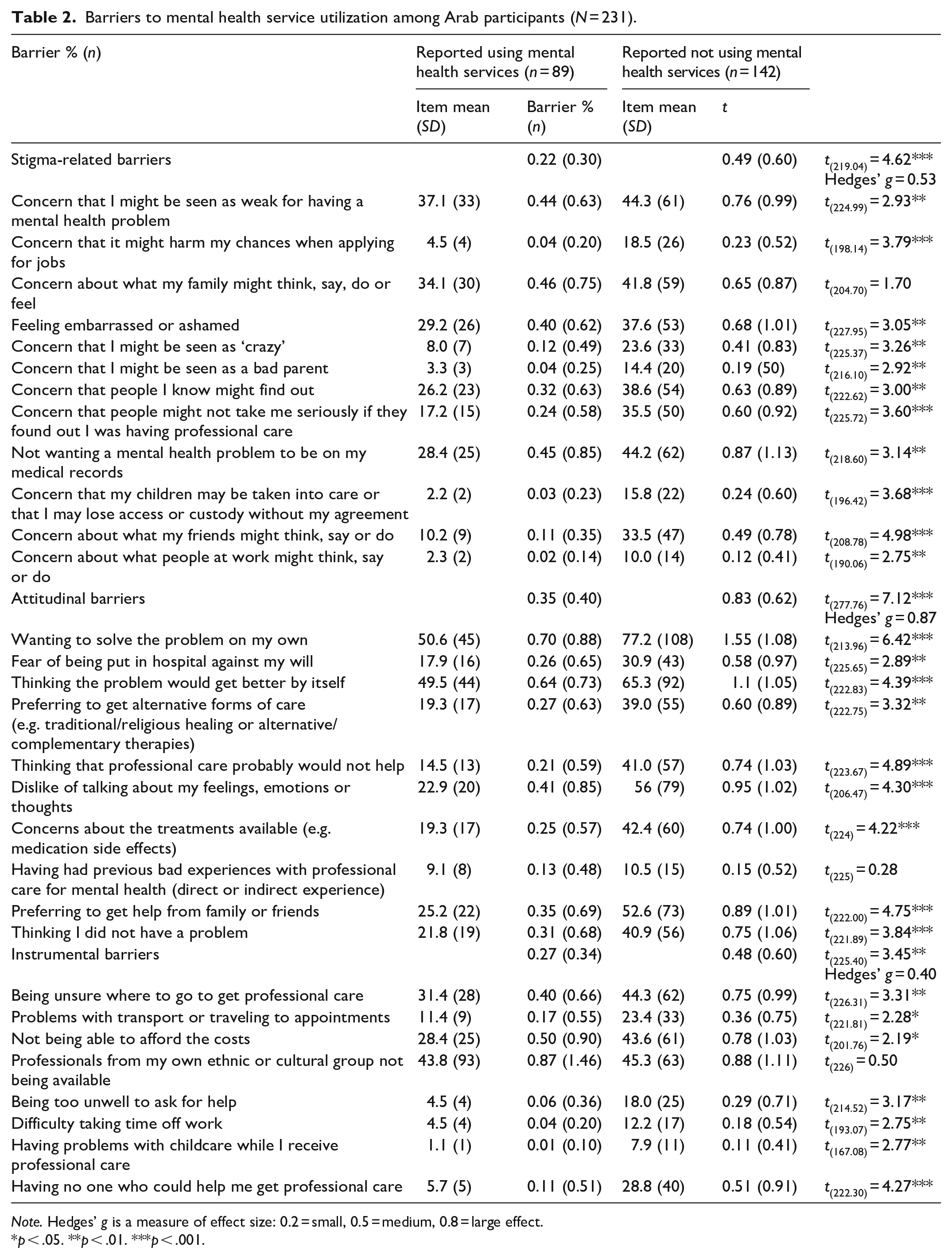
Note. Hedges’ g is a measure of effect size: 0.2 = small, 0.5 = medium, 0.8 = large effect.
p < .05. **p < .01. ***p < .001.
Regarding stigma-related barriers, there was a difference between the two groups in all 12 items, except for the item related to what the family might think, say, do or feel. Among participants who reported using mental health services, compared to the ones reported not using them (in brackets) the leading stigma-related barrier was concern with being seen as weak, reported by 37.1% (compared to 44.3%) at any barrier level. Regarding attitudinal barriers, significant differences were found between the two groups in all 10 items, except for the item of previous bad experiences with professional mental healthcare. The leading attitudinal barrier related to the desire to solve the problem on one’s own – reported by 50.6% (77.2%) at any barrier level. Finally, regarding instrumental barriers, significant differences were found between the two groups in all eight items except the item related to unavailability of professionals from one’s own ethnic or cultural group – the leading instrumental barrier in both groups, reported by 43.8% (45.3%).
Determinants of mental health service use
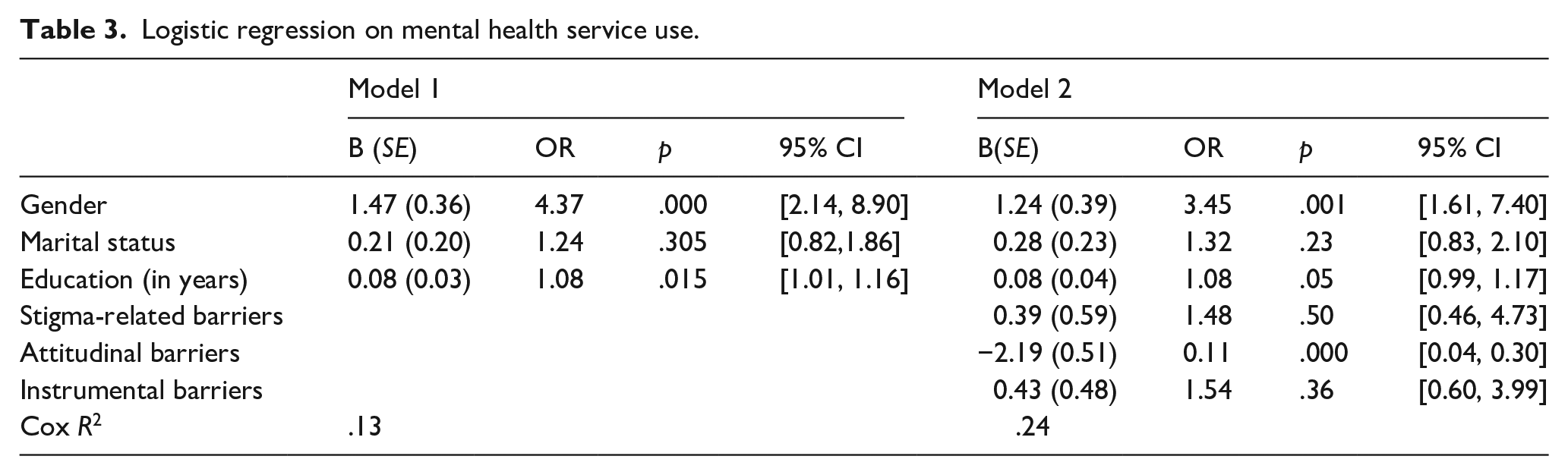
The results of binary logistic regression models predicting mental health service use are shown in Table 3. As can be observed, sociodemographic characteristics explained 13% of the variance in mental health service use. With the addition of the three barriers dimensions, Cox R2 was .24, indicating that 24% of the variation in mental health service use was explained by the estimated model. However, only the attitudinal barriers were significant correlates of mental health service use. Being female, having higher education and lower attitudinal barriers were the most important determinants of mental health service use.
Logistic regression on mental health service use.
Discussion
To the best of our knowledge, this study was the first to examine barriers to mental health service use among the Arab minority in Israel and its other correlates. Overall, we found significant differences between the two groups – users and non-users – in all three dimensions of the Barriers to Care Evaluation scale (BACE, v3; Clement et al., 2012), with those who did not use mental health services reporting higher levels of barriers. However, participants in both groups reported relatively low levels of stigma-related, attitudinal and instrumental barriers. In general, studies show that minorities report high barriers to the use of mental health services (Clement et al., 2012; Fante-Coleman & Jackson-Best, 2020; Planey et al., 2019; Scheppers et al., 2006). While we could not compare our results to previous studies because of our use of different barrier measures, several explanations may account for our findings. First, most of our participants were female, with an education level higher than average in Arab society in Israel (Central Bureau of Statistics, 2017). According to the literature, gender and education are significantly associated with mental health service use, with female and better-educated individuals both reporting higher utilization of mental health services (Abo-Rass & Abu-Kaf, 2023; Campo-Arias et al., 2020). Second, the process of sociocultural change in Arab society in Israel has been shown to positively affect mental health literacy, prevailing attitudes to mental illness, treatment, and stigma (Al-Krenawi, 2019), and this may therefore have also positively affected the perceptions of barriers to mental health services. Third, it is possible that the sample's clinical characteristics such as psychological symptoms and perceived need, which we did not examine, influenced the findings, especially given the positive association between these characteristics and perceived barriers to mental health service use (Ugarte Bustamante et al., 2020).
However, the BACE results identified significant differences between those who reported using versus not using mental health services, not only in the three general barrier dimensions but also in all individual BACE items except three, with two of them rated as major barriers among the two participant groups. The first was ‘Concern about what my family might think, say, do or feel’; over a third of each group reported this item as a barrier at any level. The family is very important to individuals from the Arab minority in Israel, it is their main support system and the relationships between the Arab family members are very close (Abu-Kaf, 2019; Haj-Yahia, 2019). This may explain why both groups, even those reporting having used mental health services, perceived the stigma that may be experienced by the family as a major barrier.
The second item in which there was no difference between those using and not using mental health services was ‘Professionals from my own ethnic or cultural group not being available’; almost half of each group reported this item as a barrier at any level. This finding is not surprising and is also consistent with previous studies showing that the unavailability of professionals from the same background is a barrier to mental health service use among minorities (Fante-Coleman & Jackson-Best, 2020; Ugarte Bustamante et al., 2020). In Arab society in Israel in particular, this finding is also an adequate reflection of structural realities: the mental health services provided to this minority are inferior compared to Jewish society (Al-Krenawi, 2019). The shortage of Arab mental health professionals is well documented and moreover, available services are rarely culturally adapted, not even to the extent of using Arabic (Al-Krenawi, 2019). A recent qualitative study examining mental health literacy among Arab students in Israel has shown that they protest against the low availability of mental health services in Arab areas in Israel, the low availability of Arabic-language services, as well as the relative lack of Arab mental health professionals (Khatib & Abo-Rass, 2022).
Out of all three BACE barrier dimensions evaluated, the one found to be a statistically significant determinant of mental health service use was the attitudinal dimension. On one hand, following the literature, we expected the instrumental dimension to be a significant determinant in a minority of low socioeconomic status such as the Arab minority in Israel, especially in light of the abovementioned low availability of mental health services in minority areas. We also expected to find the stigma-related barrier dimension to be a significant determinant of service use, given the aforementioned highly stigmatizing approach to mental health treatment in the Arab world, including Arab society in Israel (Al-Krenawi, 2019; Zolezzi et al., 2018). We assume that our results might be due to having used a convenience sample partly based on snowball sampling, so the questionnaire was administered among relatively similar participants reporting low levels of stigma-related and instrumental barriers. However, our findings are in line with previous studies that showed that attitudes and perceptions are related to health outcomes including help-seeking and treatment adherence (Abo-Rass et al., 2020b; Andrade et al., 2014; Baines & Wittkowski, 2013; Mojtabai et al., 2016; Ten Have et al., 2010). They are also consistent with a recent study conducted in the Arab minority in Israel, which found that attitudes that promote mental help-seeking behavior are positively related to the utilization of mental health services (Abo-Rass & Abu-Kaf, 2023).
Finally, our findings highlight the relationship between attitudes and behaviors (Ajzen et al., 2018) in the area of mental health, also among minorities with low socioeconomic status, as they indicate that this relationship also exists between the Arab minority’s attitudes and their mental health service use. However, since our model provides an only partial explanation for the use of mental health services, we suggest conducting further research regarding the factors that might better predict minorities' mental health service use. Based on our findings, we recommend that intervention programs work on improving attitudes that constitute barriers to the use of mental health services, but on the other hand, given the findings, also work to remove the barriers associated with the minority’ disadvantaged socioeconomic status. In other words, the fact that certain cultural perceptions lead individuals to avoid mental health services does not free those services from the responsibility of addressing the structural barriers that also contribute to that avoidance.
Limitations and implications
The current study has several limitations. Firstly, its use of a convenience sample that is culturally homogeneous limits the generalizability of our findings and conclusions. Specifically, the sample was dominated by female participants, a fact that might bias the results. Future studies should also include more males. Secondly, our cross-sectional design prevents us from inferring causal relationships, so we cannot answer essential questions such as did those who use mental health services experience fewer barriers to service use, or did they experience the same barriers as non-users but considered them as less of a hindrance? Thirdly, our data are based mostly on self-report measures administered online that have several limitations, including preselection of frequent internet users, and potentially inaccurate interpretations of specific questions that cannot be corrected due to the absence of a researcher. Fourthly, the face-to-face interviews in which some of our data were collected might have involved social desirability bias. And it is also possible that there is a bias in the findings because of the online component in the data collection because there are groups of people who do not use the Internet, and thus the snowball did not reach them. Fifthly, Clement et al. (2012) BACE scale does not include an examination of barriers that may be unique to the specific sociopolitical context of the Arab minority in Israel, such as religiosity, faith-based healing, or political barriers. Future studies must examine these barriers to complete the picture about the utilization of mental health services in this unique population. Based on the literature reviewed and the barriers found, it seems particularly important to gain in-depth understanding of the barriers related to the specific socioeconomic and political status of the Arab minority in Israel. Finally, the study did not distinguish between subgroups in Arab society, such as different religious groups, Muslims, Christians, and Druze. Therefore, there is a need for further research that will examine whether barriers to mental health services differ across subgroups.
These limitations notwithstanding, this study has several strengths make an important contribution to emerging efforts to understand mental health service use among minority groups with unique cultural characteristics. Devoting special attention to these groups is essential, as they are at higher risk of facing barriers related to their minority status. In addition, the present study has important theoretical and practical implications. Our findings expand on the results of available studies, most of which are descriptive and non-empirical, regarding barriers to mental health service use among the Arab minority in Israel. Our study also adds to the literature by linking barriers directly to actual service use, rather than to help-seeking behaviors or intentions. Our findings can serve as a theoretical basis for understanding and examining other mental health service use barriers among Arabs in Israel. In addition, they inform professionals and policymakers about these barriers, drawing their attention specifically to the fact that the attitudinal barrier dimension was the most significant determinant of mental health service use. Hence, our findings stress the need to develop multidimensional interventions, with emphasis on attitudes, in order to improve mental health service use by Arabs in Israel.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.