
Abstract
Background:
In recent years it could be shown that psychosocial working conditions and mental health of employees are closely correlated. One well-established instrument to measure psychosocial stress at work is the COPSOQ (Copenhagen Psychosocial Questionnaire, German Standard Version). It is an 84 item self-rating instrument addressing several domains of psychosocial working conditions and is generally used for risk assessments in companies.
Aims:
To examine associations between COPSOQ ratings with clinical features and symptoms of employees who currently suffer from an episode of a mental illness requiring inpatient treatment.
Method:
For 265 inpatients with mental disorders who participated in a cluster randomized trial (RETURN-study) COPSOQ-data were available as part of the baseline data acquisition. These data were compared with the German COPSOQ validation sample of the Freiburg research center for occupational sciences (FFAW; approximately 250,000 participants). For subdomains of the COPSOQ that showed major and significant differences between the two samples regression analyses were done to predict COPSOQ scores within the RETURN-sample.
Results:
Psychiatric inpatients did not assess their working conditions significantly different compared to the population based FFAW sample. However, with regard to the effects of working conditions (general health, burnout, presenteeism, and intention to leave the job) there were major differences between the two samples with the clinical sample expressing more negative views. In the RETURN sample these were predicted by a greater expression of depressive symptoms.
Conclusions:
The linkage between work and mental wellbeing is complex. Mental illness is not necessarily a result of poor working conditions, while good working conditions may not in every case prevent symptoms of bad health, even if such associations exist.
Keywords
Introduction
Mental illnesses are responsible for an increasing part of cases of inability to work and the related economic burden is immense (European Union, 2018; Wittchen et al., 2011). In recent years it has been acknowledged that psychosocial working conditions and mental health of employees are closely correlated (Laaksonen et al., 2006; van Hoffen et al., 2021) and that poorer psychosocial working conditions can also lead to increased sickness absences (Rugulies et al., 2010; Slany et al., 2014). Thus, psychosocial work conditions may also be expected to be closely related to episodes of mental illnesses.
In Europe, the COPSOQ (Copenhagen Psychosocial Questionnaire) has been established as a valid measure to assess psychosocial working conditions (Kristensen et al., 2005; Lincke et al., 2021). The COPSOQ is an 84 item self-rating instrument addressing several domains of psychosocial working conditions including quantitative and emotional demands (Lincke et al., 2021).
Despite its widespread use, employers may sometimes have concerns about the COPSOQ, especially with regard to the validity of employees’ self-ratings of potentially stressful work conditions. Additionally, there is only limited evidence on the use of the COPSOQ by (highly) symptomatic employees, for example, those suffering from acute depressive episodes. Specifically, there is no data on whether psychiatric symptoms considerably influence the COPSOQ ratings of working conditions.
Therefore, the aim of the present analysis was to examine associations between COPSOQ ratings and clinical features or symptoms of employees who currently suffer from an episode of a mental illness requiring inpatient treatment.
Within the analysis we try to answer the following research questions:
How do employees currently being treated as psychiatric inpatients rate psychosocial working conditions at their workplace?
How do these ratings compare to the average data standard scores of German employees as obtained by FFAW (Freiburg research center for occupational sciences)?
Which clinical patterns explain major variations between these two samples?
Methods
The present analysis is a cross-sectional study using baseline data of the RETURN study (Riedl et al., 2020), comparing them with a validation dataset of the COPSOQ (FFAW-dataset (Lincke et al., 2021)) and trying to identify reasons for differences between the datasets and therefore differences between employees currently being treated as psychiatric inpatients and employees in a non-clinical setting.
The RETURN-study was a multi-center, cluster-randomized controlled trial addressing inpatients suffering from psychiatric disorders with current employment (Riedl et al., 2020) and aiming at supporting the return to work process of these patients by implementing a case management intervention. Thus, all patients in the intervention group of the RETURN study were supported in their return to work by case managers (RTW-Experts: Return to work Experts; Brucks et al., 2021). Overall, 268 patients were recruited for the study from January 2019 until February 2020. All participants held employment (as the main inclusion criterion for the study), were aged between 18 and 60 years and were diagnosed with either schizophrenia, an affective disorder, anxiety disorder, obsessive compulsive disorder, or a personality disorder. At study inclusion, all patients were suffering from acute episodes of their disorder requiring psychiatric inpatient treatment.
Data on the main study will be published elsewhere.
Data obtained
For all participating patients the following data were available and used for the analysis:
Sociodemographics: age, gender, education (dichotomized ⩾/<10 years), and marital status (dichotomized: partnership yes/no)
Employment parameters: leading position (yes/no), overtime hours (yes/no), working-hours (full-/part-time), branches (according to Bundesagentur für Arbeit [2011]), intention to return to work (yes/no), and influence of work on mental disorder (rated on a 10-point scale)
Clinical data: diagnosis, duration of disease, number of hospitalizations (and dichotomized in first vs. re-hospitalization), Clinical Global Impression (CGI, overall scale and depressive symptoms scale; 7-point rating scale to assess overall symptom severity; Guy, 1976), Global Assessment of Functioning Scale (GAF, rating from 0 to 100; American Psychiatric Association, 2000), and voluntary hospitalization (yes/no)
Finally, all patients answered the Copenhagen Psychosocial Questionnaire (COPSOQ III [Lincke et al., 2021]), which is the validated German version of the questionnaire. It consists of 84 self-rating items addressing psychosocial work stressors in 31 scales, which are assigned to five sections (four sections regarding working conditions and one section regarding the effects of those working conditions on employees – see Figure 1). The four sections on working conditions include scales on quantitative and emotional demands, influence and possibilities for development, social relations and leadership, and further additional factors, while the section for the effects of those working conditions comprises scales on general health, burnout symptoms, and others (Lincke et al., 2021).
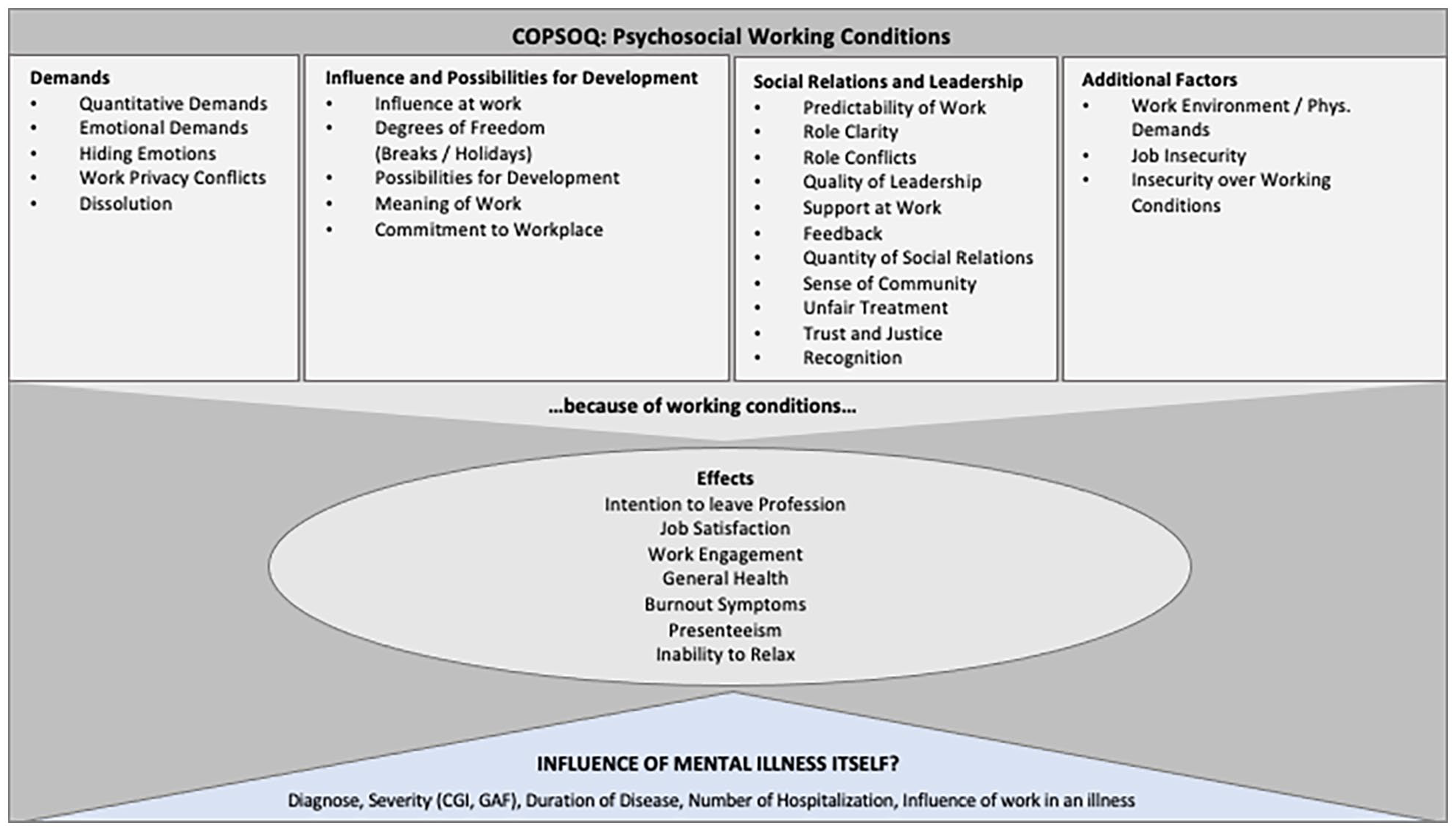
Scales of the German COPSOQ III questionnaire.
Following a Likert-type scale, all items are coded with values of 0, 25, 50, 75, and 100 points. Accordingly, mean values of items range between 0 and 100 points and scale scores are calculated by utilizing the average item score; in case less than half of the affiliated items are missing, no mean value is displayed (Lincke et al., 2021). For the single item on general health a scale from 0 to 10 is used. Overall, higher scale scores indicate a higher expression of the respective topic, irrespective of whether the issue is ‘positive’ or ‘negative’, for example, higher demands, better support.
As patients were recruited before COVID-restrictions were implemented in Germany (lock downs, shift toward more home-office) our data reflect pre-COVID conditions.
Recently data on the use of the COPSOQ in German companies with approximately 250,000 respondents were published by the Freiburger Forschungsstelle für Arbeitswissenschaften GmbH (FFAW; Lincke et al., 2021) and served as a comparator to our data from the RETURN study.
Data analysis
Descriptive statistics (frequencies, means, and standard deviations) were used to display baseline characteristics of the study sample.
We quantified differences in COPSOQ scores between the RETURN and FFAW samples using standardized mean differences (SMDs, expressed as Hedge’s g). SMDs were classified according to the Cohen’s rule of thumb into small (|g| < 0.3), medium (|g| around 0.5), and large (|g| > 0.8).
When we identified substantial differences in COPSOQ ‘effects’ subscales between the two samples (defined as Hedge’s |g| > 0.5), we further conducted multivariable linear regression analyses in order to evaluate which sociodemographic, clinical, or other work-related factors might predict subscale mean values in the RETURN sample. Here, mean values of COPSOQ ‘effects’ subscales were entered as dependent variables whereas sociodemographic data (age, gender), clinical data (diagnosis, CGI depressive symptoms, overall symptoms CGI, GAF, duration of illness, first inpatient stay), first impatient stay, severity of disease, influence of work in mental disorder), and data on the individual work environment (branches: health sector/education vs. other); overtime; intention to return to work) were entered as independent variables.
Data analysis was conducted in SPSS 26 and R statistical software v4.0.3 using metafor v.3.0-2. Alpha was set at two-sided alpha .05.
Ethics
The trial has been approved by the institutional review board of the ‘Ethikkommission der Technischen Universität München’. All patients had to provide written consent and were informed about the general purpose of the study. The trial had been registered at Deutsches Register Klinischer Studien (DRKS00016037).
Results
A total of n = 268 patients participated in the RETURN study and, depending on the single COPSOQ scales, data on n = 229 to 265 participants were available. Baseline data of the n = 265 patients providing at least some COPSOQ data are given in Table 1. There were more women than men in the sample and the mean age was around 40 years. Most participants were suffering from an affective disorder (67%), followed by 24% of the participants suffering from psychotic illnesses such as schizophrenia. A 38% were in inpatient care for the first time, and 10% had been hospitalized involuntarily. The severity of the illness according to CGI averaged 4.6 (moderately to markedly ill), the CGI depressive symptoms 4.3, and the GAF (global assessment of functioning) 46.2, indicating serious symptoms and impaired functioning.
Baseline data (RETURN study population).
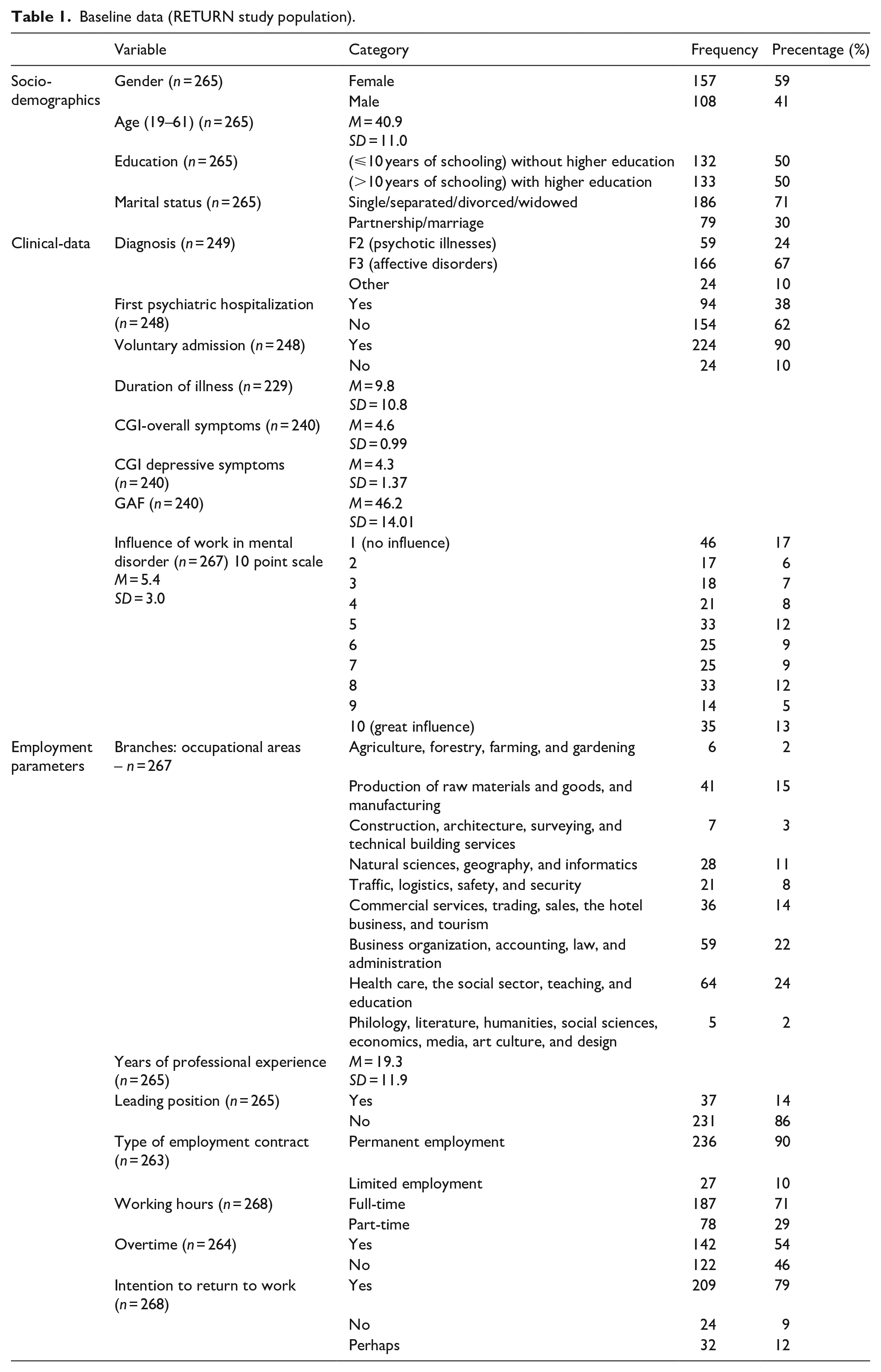
On a range from 1 (no influence) to 10 (very strong influence), 17.2% of respondents declare that work had no impact on their illness, whilst 13.1% sensed a very strong influence. A 49.4% of the participants indicated a value higher than five.
In terms of occupational areas (Bundesagentur für Arbeit, 2011), 23.9% of respondents worked in health care, the social sector, teaching and education, 22.1% in business, accounting, law, and administration, and 15.3% worked in production of raw materials and goods, and manufacturing. These were also the major occupational areas in the FFAW sample.
Whilst 11.9% of participants were unsure if they wanted to return to work, 9.0% indicated that they could not imagine returning. As such, 79.1% were envisaging a return to their workplace.
Table 2 compares the COPSOQ mean values between the RETURN and FFAW samples. For the subscale scores of psycho-social factors, there were no differences (e.g. in influences and possibilities for developments) or small to medium differences (|g| ⩽ 0.34). Participants of the RETURN sample in some dimensions exhibited better scores (g > 0), in the sense that they felt less exposed to stressful working conditions (e.g. predictability of work, trust, and justice), and worse scores (i.e. g < 0) in other dimensions (e.g. quantitative and emotional demands, dissolution).
Comparison of COPSOQ data from RETURN and FFAW.
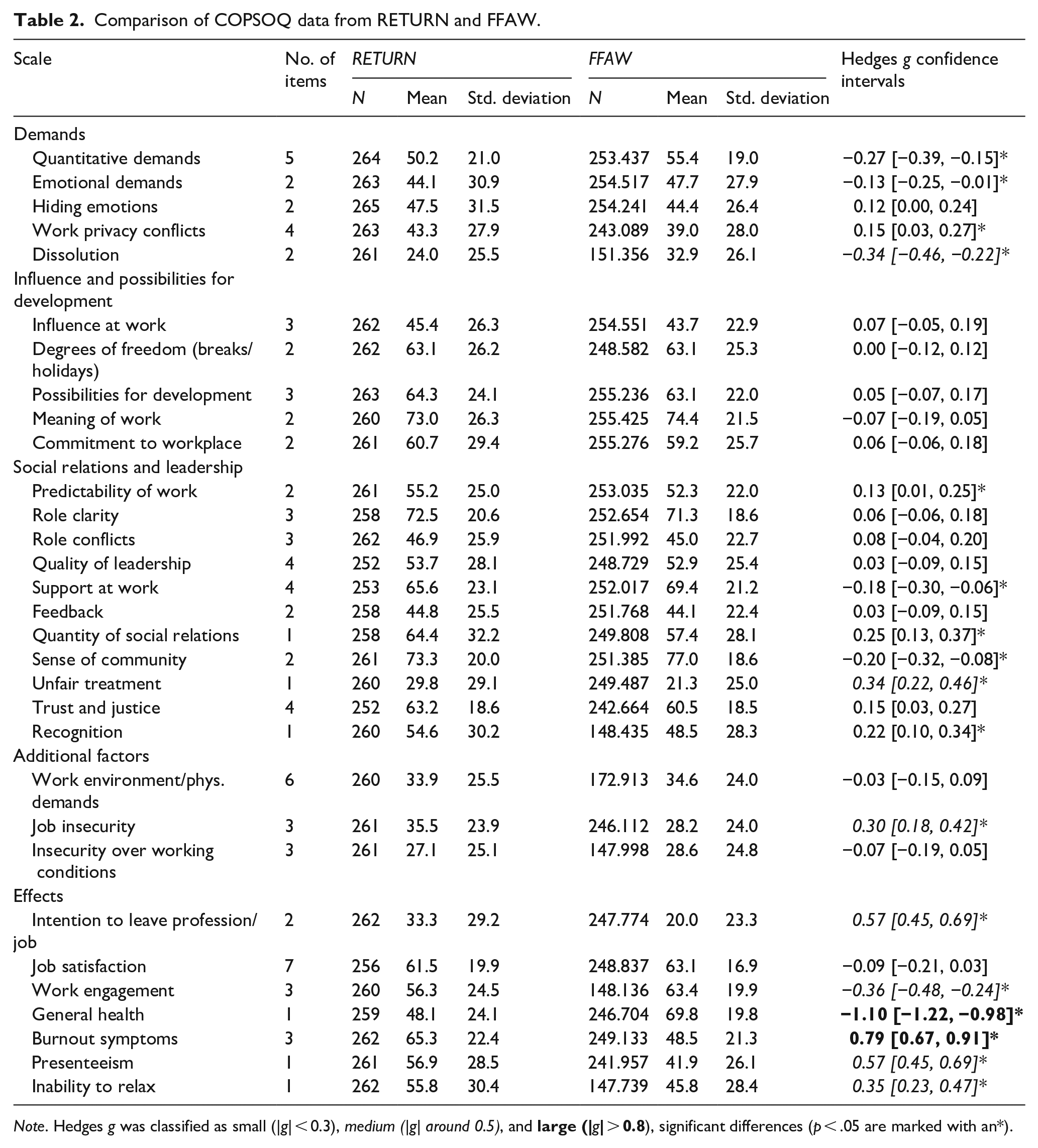
Note. Hedges g was classified as small (|g| < 0.3), medium (|g| around 0.5), and
In contrast, there were considerable (medium to large) differences (|g|>0.5) between the two samples with regard to four of the ‘effects’ scales of the COPSOQ, that is intention to leave the job, burnout symptoms, presenteeism, and general health, with participants of the RETURN-sample exhibiting more unfavorable ratings.
Prediction of COPSOQ effects subscales by clinical factors
The COPSOQ subscales on general health, burnout, presenteeism, and intention to leave the job could be predicted to some extent by independent variables (Table 3). Thus, general health was better for patients with schizophrenia (compared to depressed patients) and poorer for patients with more depressive symptoms. Higher burnout scores were predicted by female gender, a diagnosis of depression (compared to schizophrenia) and by first inpatient stay (compared to more than one inpatient stay). In addition, burnout was higher in patients who attributed more influence of work on their mental illness, who did not plan to return to their workplace, patients with more depressive and less overall symptoms.
Clinical predictors of COPSOQ ‘effects’-scales.
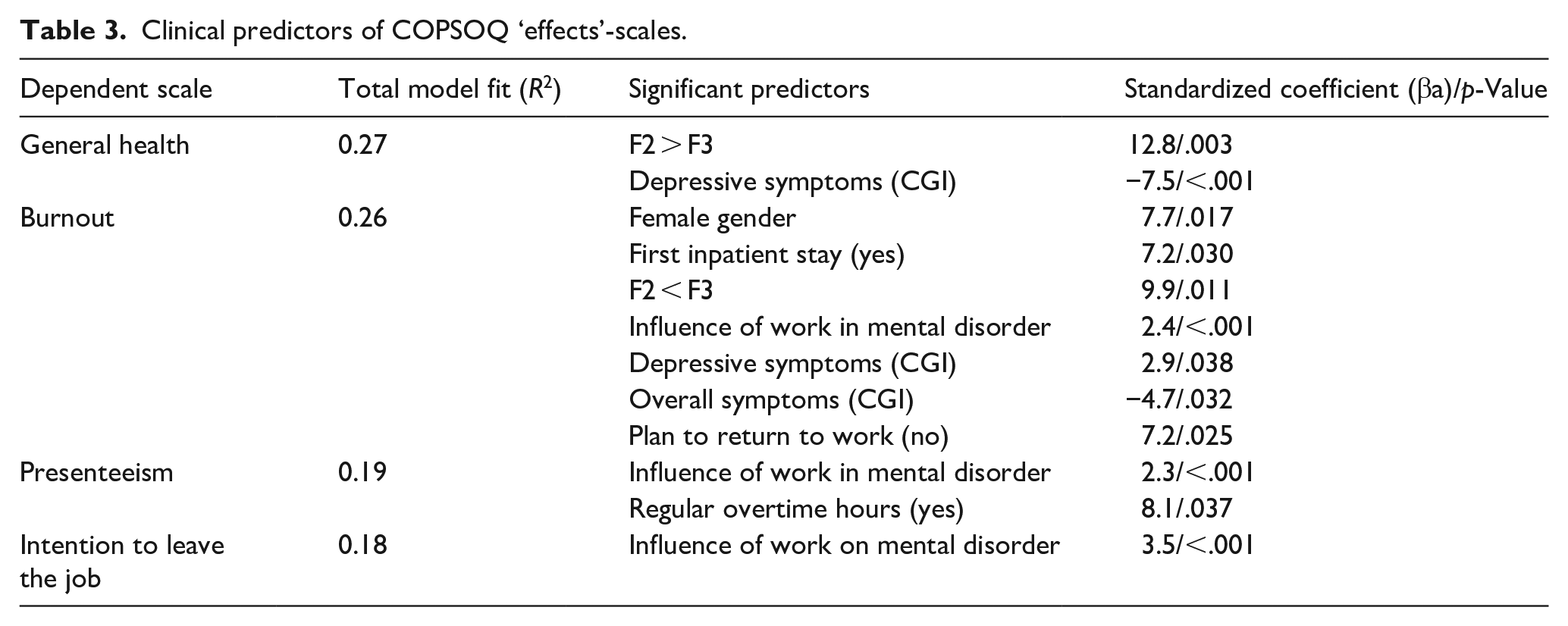
Presenteeism was higher in patients who attributed more influence of work on their mental illness and in patients who reported regular overtime hours.
Conclusions
Our results show that employees in episodes of acute mental illnesses do not generally rate psychosocial working conditions differently compared to participants from a large, non-clinical, population-based dataset. However, ‘effects’ (e.g. burnout and general health) were rated considerably more unfavorable. These effects scales could, to some extent, be predicted by clinical variables such as depressive symptoms and the self-rated influence of job conditions on the course of the illness.
Interpretation of the results
We see two results as especially important. First, patients with a severe episode of a mental illness do not necessarily rate their working conditions poorer than the general population. Second, the major differences in the effects-scales (e.g. burnout) are to a relevant extent explainable by depressive symptoms.
Regarding clinical interpretation, one could argue that it is not poor working conditions that play a major role of these persons becoming ill. In this sense, the patients studied might be suffering from rather clinical disorders for which, for example biological, biographical, and non-work-related psychosocial risk factors may play a bigger role than working conditions. On the other hand, referring to the vulnerability stress model, even smaller amounts of work-related stress might have illness specific consequences in persons suffering from more severe mental illnesses. Thus, the minor differences between the RETURN and the FFAW sample might be sufficient to have contributed to relapse and inpatient admission. The major differences in the ‘effects’ section (e.g. for burnout) do in our view reflect the symptomatology of patients, that is with burnout items mapping mostly depressive symptoms.
In any case our data do not support the assumption that poor working conditions are strongly linked with psychiatric illness, but rather that working conditions and episodes of mental illness are either only weakly linked (‘mediated’ by vulnerability) or not linked. This finding fits well with the fact, that ‘effects’ like general health and burnout symptoms could be explained to a relatively low extent by work factors in statistical regressions. Additionally, general salutogenetic aspects of work have been well established and may counteract work-stress (Modini et al., 2016).
As depressive symptoms occur episodically in the majority of the clinical case, one must be aware that such illness episodes may have more disruptive effects than, for example, psychotic disorders which often have a more chronic course. Thus, the effect of a person losing one’s sense of self-coherence and looking for an explanatory model for the acute illness, may explain, why depressive symptoms had the greatest impact on the COPSOQ effects – and certainly this may lead to (potentially unnecessary) ideas of leaving the job.
Regarding methodological interpretation, our results support the validity of the COPSOQ, at least with regard to the sections of psychosocial working conditions. Thus, ‘work’ seems to be a different and in a way independent sphere from, for example general aspects of (mental) health.
Limitations
There are no data on psychiatric morbidity in the FFAW sample. The two samples (RETURN/FFAW) were not comparable regarding sociodemographics. While the FFAW sample is weighted by occupational groups to represent German workforce, this was not possible for the RETURN sample due to its limited size.
The COPSOQ questionnaire is not intended and not validated to measure individual burden. Its main focus is to describe working conditions on group levels and mean values or statistical results are of rather general significance. Working conditions and bad health effects may, of course, be associated with mental illness on the individual level.
Finally, we would like to comment on the issue of pre-COVID and COVID-working conditions. Patients in the study were recruited shortly before COVID restrictions were implemented in Germany. Thus, our data represent pre-COVID conditions. During the follow up period of the study (these data are not presented in this paper) and also in our work as clinical psychiatrists we experienced significant stress of patients who were sent to home-office during COVID-lockdowns and afterwards. Therefore, patients’ ratings of their working conditions in 2021/2022 might differ considerably from the results we presented here, as potentially salutogenetic effects of work (e.g. personal contact with colleagues, clear day structure) ceased to exist when patients were sent for home-office. One implication suggested by data from our main trial could be, that some patients are better reintegrated into their workplace when being offered office-based work compared to home-office.
Conclusion
The study highlights, that the linkage between work and mental wellbeing is complex. Mental illness must not necessarily be a result of poor working conditions, while good working conditions may not in every case prevent symptoms of bad health, even if such associations exist. Rather our results support a complex interplay of work-stress, salutogenetic effects of work, and the potentially disruptive effects of depressive illness symptoms.
Footnotes
Acknowledgements
The authors would like to thank the following persons who supported recruitment within the RETURN study: Prof. Dr. Michael Landgrebe (kbo Klinikum Agatharied), Prof. Dr. Stephan Heres (kbo Klinikum München Nord), Dr. Pierre Beitinger & Prof. Dr. Martin Keck (Max-Planck-Institut für Psychiatrie), Prof. Dr. Alkomiet Hasan/Prof. Dr. Peter Falkai (Klinik für Psychiatrie und Psychotherapie der LMU München), and Dr. Nikolai Marstrander (kbo Klinik Fürstenfeldbruck).
Availability of data and materials
Original data can be made available upon reasonable request.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.H. received lecture honoraria from JnJ, Lilly, ROVI, and Otsuka and research grants from JnJ. HJ L. is affiliated with Freiburger Forschungsstelle für Arbeitswissenschaften GmbH (FFAW), Freiburg, Germany. For all other authors: none.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by Gemeinsamer Bundesausschuss, Innovationsfonds, Förderkennzeichen 01VSF17012.
Ethical approval
The trial has been approved by the local review board (Ethikkommission der Technischen Universität München) and has been registered at Deutsches Register Klinischer Studien (DRKS00016037). All participating patients had to give written informed consent.