
Abstract
Objective
Understanding differences in outpatient care before and after mental health hospitalization for adolescents from diverse backgrounds is critical to ensuring effective and responsive care. The objective of the current study was to examine outpatient mental health care in the two years before and 30 days after a mental health hospitalization for adolescents from immigrant, refugee and non-immigrant backgrounds.
Method
This retrospective, population-based cohort study, conducted in British Columbia (BC), Canada, analyzed linked health service utilization data (practitioner billings, hospitalizations) and migration records to track outpatient care before and after mental health hospitalization. The study included adolescents (ages 10–18) with an unscheduled/urgent mental health hospitalization between January 1, 2008 and December 31, 2016 (n = 5,314) from a cohort of adolescents in 10 of the largest school districts in BC (between 1996 and 2016). The main analyses examined outpatient mental health visits (e.g., general practitioner/psychiatrist) (i) in the two years before hospitalization and (ii) in the 30 days after discharge. Sub-analyses focused on outpatient visits with psychiatrists.
Results
Overall, 30.4% had no outpatient mental health visit in the two years before hospitalization and 45.1% had none in the 30 days following discharge. First-generation immigrants and refugees and second-generation immigrant adolescents were significantly less likely than non-immigrants to have had an outpatient mental health visit in the two years before mental health hospitalization (aOR1st_gen_immg = 0.79, 95% CI, 0.63 to 0.98; aOR2nd_gen_immg = 0.75, 95% CI, 0.61 to 0.93; aOR1st_gen_ref = 0.40, 95% CI, 0.26 to 0.64). Second-generation immigrant adolescents were significantly more likely than non-immigrants to have had any outpatient mental health visit in the 30 days following hospitalization (aOR2nd_gen_immg = 1.34, 95% CI, 1.09 to 1.65).
Conclusions
Results suggest outpatient care before and after mental health hospitalizations is limited for many adolescents in BC and differed by migration background. Implications for meeting standards of care are discussed.
Plain Language Summary Title
Mental health-related care from a doctor/psychiatrist before and after mental health hospitalization for adolescents from immigrant, refugee, and non-immigrant backgrounds in British Columbia
Plain Language Summary
The objective of this study was to examine differences in mental health-related visits to a doctor or a psychiatrist before and after mental health hospitalizations for adolescents from diverse backgrounds in British Columbia, Canada.
Using health insurance and hospital records, the study followed 5,314 adolescents (aged 10-18) who had a mental health-related hospitalization between January 1st, 2008 and December 31st, 2016. For this group of adolescents, the study then tracked whether or not they had received care (i.e., from a doctor or psychiatrist related to their mental health) in the 2 years before their hospitalization and also in the 30 days after their hospitalization.
The study found that 30.4% of those hospitalized for a mental health concern had no mental health visit with a doctor/psychiatrist in the two years before hospitalization and 45.1% had no visits in the 30 days following discharge. A main finding of the study was that newcomers to Canada (immigrants and refugees born outside of Canada) were less likely to have visited a doctor/psychiatrist for a mental health-related reason in the 2 years before their hospitalization than their non-immigrant peers.
Results suggest outpatient care before and after mental health hospitalizations is limited for many adolescents in BC and differed by migration background. Implications for meeting standards of care are discussed.
Mental disorders have profound consequences for the health, and social and economic well-being of young people—and for the societies in which they live.1,2 Recent global prevalence estimates suggest that 1 in 10 children and youth (5–24 years of age) have a diagnosable mental disorder—representing one-fifth of all cause disease-related disability. 3 The majority of mental disorders (75%) have their onset before the age of 25 (50% before age 14 4 ). The importance of child and youth mental health, and optimization of care, is increasingly recognized as a priority in Canada and globally.1,2,4 Yet, inadequate or delayed access to mental health care for young people remains an on-going concern,1,5–7 especially for adolescents from immigrant and refugee backgrounds.6,7
Clinical guidelines recommend that treatment of mental disorders is primarily delivered on an outpatient basis, coupled with supports within the family, school and community, and in-patient care is reserved for treating acute symptoms requiring emergency stabilization and monitoring.8,9 However, evidence suggests a reliance on in-patient, acute mental health services such as emergency room visits and hospitalizations for the treatment and care of mental disorders. 10 Indeed, higher levels of outpatient care have been associated with decreased rates of hospitalizations among youth. 11 The provision of timely follow-up care after child and youth psychiatric hospitalizations has been associated with better treatment outcomes.12–14
Despite the importance of outpatient care before and after hospitalization, there is limited knowledge on variations in outpatient care for different sub-populations of adolescents who are hospitalized with a mental disorder.11,14,15 Children and youth from immigrant and refugee backgrounds may be particularly at risk of not receiving appropriate outpatient care leading up to and following mental health hospitalizations. Immigrant and refugee children and youth have been found to be less likely to access outpatient mental health services16,17 but more likely to utilize the emergency department as a first point of contact for mental health care than their non-immigrant peers.18,19 Understanding differences in outpatient care before and after mental health hospitalization for adolescents is critical to ensuring mental health care is effective and responsive to the needs of the diverse sub-populations of young people.
The Study Objective
The aim of the study was to examine differences in outpatient mental health care before and after a mental health hospitalization for adolescents from immigrant, refugee and non-immigrant backgrounds in British Columbia, Canada, using common mental health service performance metrics.
20
Focusing on individuals’ first hospitalization episodes within the study period (and excluding those with a hospitalization in the two years before study inception), this study examined the likelihood of:
any outpatient mental health visit in the two years before a mental health hospitalization (sub-analysis: any outpatient visits with a psychiatrist in the two years before a mental health hospitalization), any outpatient mental health visit in the 30 days after discharge from hospital (sub-analysis: any outpatient visits with a psychiatrist in the 30 days after discharge from hospital).
Method
Study Design and Setting
We used population-based linked administrative data on hospitalizations and outpatient services in British Columbia (BC), Canada, to conduct a retrospective cohort study of outpatient mental health care in the two years before and 30 days after adolescent mental health hospitalizations. In BC, there are approximately 93 child and youth mental health intake clinics across the province and 7 main hospitals equipped with inpatient child and youth mental health services, servicing different areas of the province. In smaller communities, it is possible that children and youth with mental health concerns may be temporarily admitted to general paediatric beds or to adult psychiatric units until a transfer to a dedicated child and youth mental health inpatient unit is completed. Approval for this project was granted by the University of British Columbia Behavioural Research Ethics Board. The reporting of this study is in keeping with the REporting of studies Conducted using Observational Routinely collected Data (RECORD) guidelines. 21
Data Sources
Health services data were requested from the BC Ministry of Health (including Medical Services Plan (MSP) Registration & Premium Billing (R&PB) 22 and Discharge Abstract Database (DAD) data 23 ). Enrolment in the BC provincial universal health plan is required for virtually all residents. 24 Migration records were requested from Immigration Refugees and Citizenship Canada (IRCC; Permanent Resident Database 25 ). Data sources were linked by Population Data BC using a probabilistic-deterministic approach 24 (linkage rate: 98.4%).
Study Population
The study was based on an approved cohort of adolescents who attended school in the 10 largest districts in BC at some point between 1996 and 2016, which was identified using data from the BC Ministry of Education and Child Care and BC Ministry of Health. All school districts are located in South-Western BC where the majority of the population resides. 26 As outlined in Figure 1, we included adolescents (age 10 to 18) who had an unscheduled (i.e., urgent rather than elective/scheduled admission, as coded on the hospital record) mental health hospitalization between January 1, 2008 and December 31, 2016. Mental health hospitalizations were identified through hospital discharge records with a primary discharge diagnosis indicating an International Classification of Diseases [ICD] 10th Edition (ICD-10-CA) diagnostic code F04 to F99 or a secondary diagnosis indicating an ICD-10-CA code X60 to X84 (for previous use of this coding criteria, see 18 ). Following all exclusions (see Figure 1), this resulted in a cohort of 5,314 for analyses related to outpatient care in the two years before hospitalization. For the analyses predicting outpatient mental health care in the 30 days following hospitalization, we excluded hospitalizations that culminated in death at discharge or transfers with undetermined end dates (e.g., transfers to long-term care facilities, palliative/hospice), resulting in a cohort of 5,162 (see Figure 1). In some cases (9.9%), hospitalization episodes resulted in readmission within 30 days. No significant differences in readmissions within 30 days were found based upon migration background (X2 (4, N = 5,162), P = .882) and follow-up sensitivity analysis revealed no substantive changes in results when readmission records were retained or removed (records were retained for the final analysis).
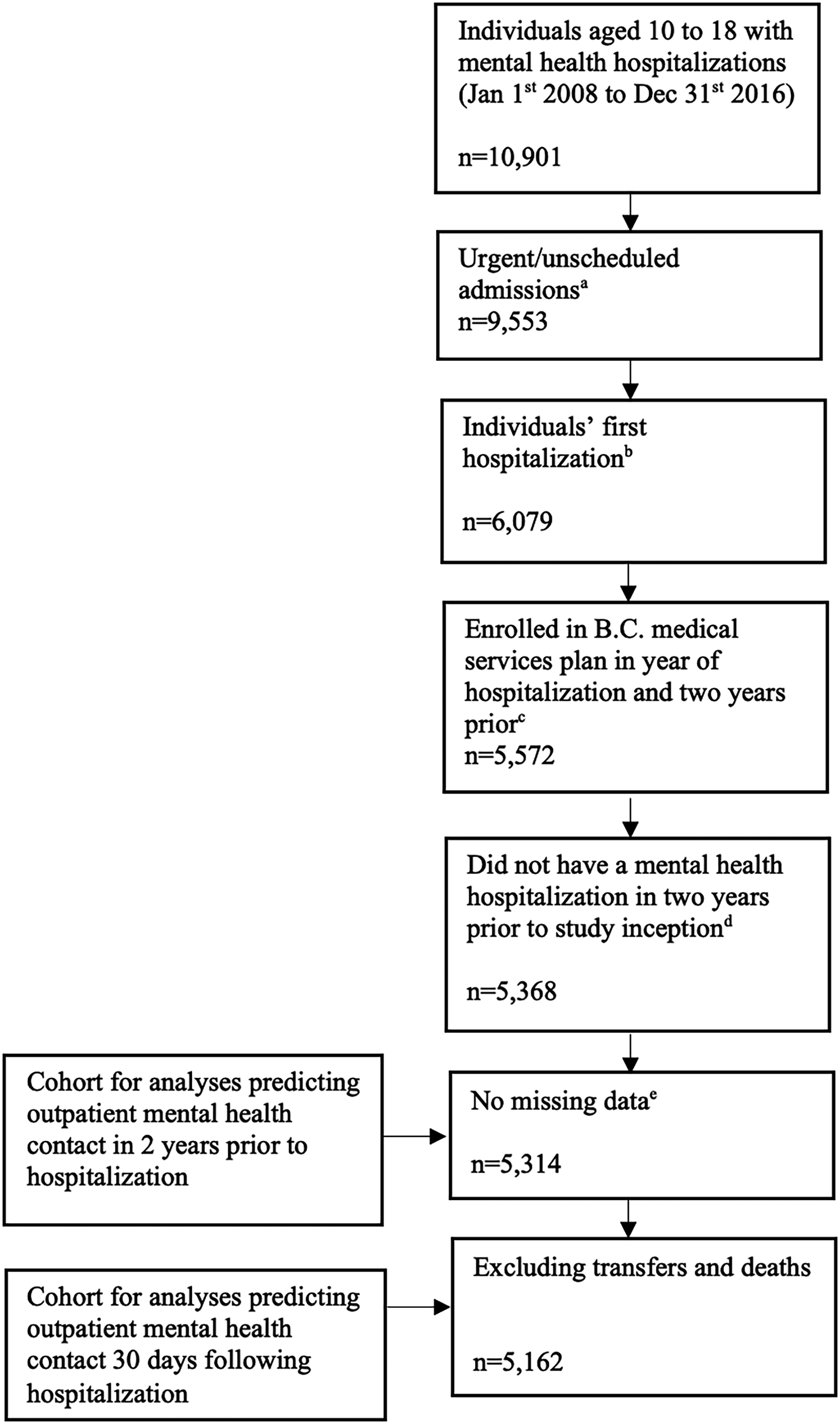
Flow chart of study cohort creation.
Dependent Variables
We analyzed four dependent variables: In the two years before hospitalization, we assessed whether individuals had (i) any outpatient mental health visit, or (ii) an outpatient psychiatrist visit. In the 30 days after hospital discharge, we examined whether individuals had (iii) any outpatient mental health visit, or (iv) an outpatient psychiatrist visit. The 2-year-before and 30-day-after hospitalization time periods are in line with youth mental health service performance indicators established in a Canadian context. 20 Outpatient mental health visits were identified using billing records covered under the provincial health insurance plan (MSP). Outpatient visits were predominantly physician-based: general practitioners (46.8%), psychiatrists (40.1%), paediatricians (10.6%), neurologists (0.10%) and 2.4% of visits were billed by other types of practitioners (e.g., nurse practitioners). Mental health visits were defined as those for which the primary diagnosis (“most responsible” diagnosis for the visit) was a mental disorder (ICD-9: 290-314) or the practitioner was a psychiatrist. Visits billed over the course of the hospitalization (including on the day of hospital admission/discharge) or by practitioners in hospital (with Emergency Department or inpatient service locations) were not counted as outpatient visits.
Independent Variables
Migration background was identified through IRCC's Permanent Resident Database. 25 First-generation immigrant and refugee (i.e., foreign-born) children were identified by their own IRCC migration record. Second-generation immigrant and refugee children (i.e., children born in Canada to at least one immigrant or refugee parent) were identified based upon parental IRCC migration records. All other children were categorized as part of the non-migrant group (the reference group; ref).
Information on sex at birth (ref: female, male), neighbourhood income quintile (ref: 1, lowest, to 5), and age at hospitalization (ref: 10–12, 13–15, 16–18) was identified through the Consolidation File, which is based upon yearly provincial health registry plan data (MSP Registration & Premium Billing 22 ).
Year of hospitalization, hospital length of stay and main discharge diagnosis associated with the hospitalization episode were derived from the DAD (via the BC Ministry of Health). 23 Year of hospitalization was grouped into three categories (ref: 2008–2010, 2011–2013, 2014–2016) based on similar odds of outcomes within each category. Length of stay was categorized into quartiles (ref: 0 to 1 days, 2 to 3 days, 4 to 10 days, and more than 10 days). ICD-10-CA diagnostic codes associated with hospitalizations were grouped into seven mental disorder categories: mood/affective disorders (reference), acute stress, anxiety disorders, psychotic disorders, residual self-harm, substance-related disorders and other mental disorders. This diagnostic code categorization was adapted from Ontario's Mental Health and Addictions Scorecard and Evaluation Framework 18 (see Table 1 for more information).
Categorization of Mental Disorders Using ICD-10-CA Codes.
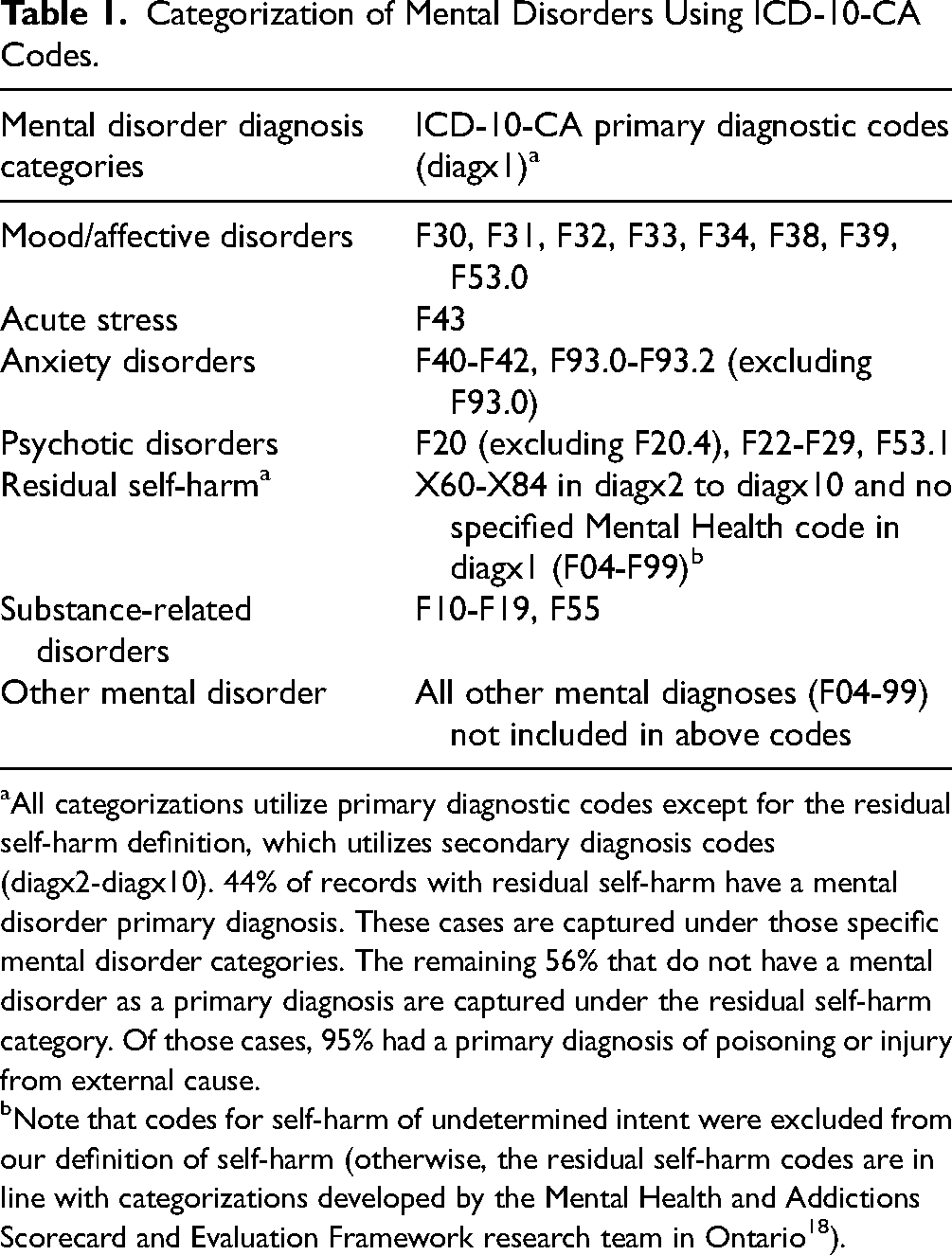
All categorizations utilize primary diagnostic codes except for the residual self-harm definition, which utilizes secondary diagnosis codes (diagx2-diagx10). 44% of records with residual self-harm have a mental disorder primary diagnosis. These cases are captured under those specific mental disorder categories. The remaining 56% that do not have a mental disorder as a primary diagnosis are captured under the residual self-harm category. Of those cases, 95% had a primary diagnosis of poisoning or injury from external cause.
Note that codes for self-harm of undetermined intent were excluded from our definition of self-harm (otherwise, the residual self-harm codes are in line with categorizations developed by the Mental Health and Addictions Scorecard and Evaluation Framework research team in Ontario 18 ).
Statistical Analyses
Descriptive statistics were calculated for all study variables for the full study cohort and by migration background. Bivariate and multivariable logistic regression analyses were conducted to examine unadjusted and adjusted associations between explanatory variables and each outcome variable. Estimated odds ratios with 95% confidence intervals (CIs) were reported and 95% CIs that do not cross 1.0 indicate statistical significance. Analyses were conducted using SAS software. 30
Results
Table 2 provides descriptive information for the overall study cohort (n = 5,314) and subgroups including first-generation immigrants (n = 406), second-generation immigrants (n = 461), first-generation refugees (n = 82) and second-generation refugees (n = 102). Overall, about 70% (69.6%) had at least one mental health visit in the two years before their hospitalization episode, with 52% of these visits specifically to a psychiatrist. Following hospital discharge, just over half (54.9%) of the cohort had a mental health visit within 30 days, and 60% of those visits were to a psychiatrist. Among those who had a mental health visit in the 30 days following discharge, 77.4% had a mental health visit in the two years before admission. Additionally, 53.8% of those who saw a psychiatrist within 30 days of discharge had a psychiatrist visit in the two years leading up to hospitalization. Finally, 9.9% of individuals were readmitted to hospital within 30 days following hospital discharge, with a median time to readmission of 11 days (mean = 12.68 days; range = 1–29 days). Among those readmitted, 85.9% had a primary discharge diagnosis of a mental disorder.
Descriptive Statistics by Migration Background.
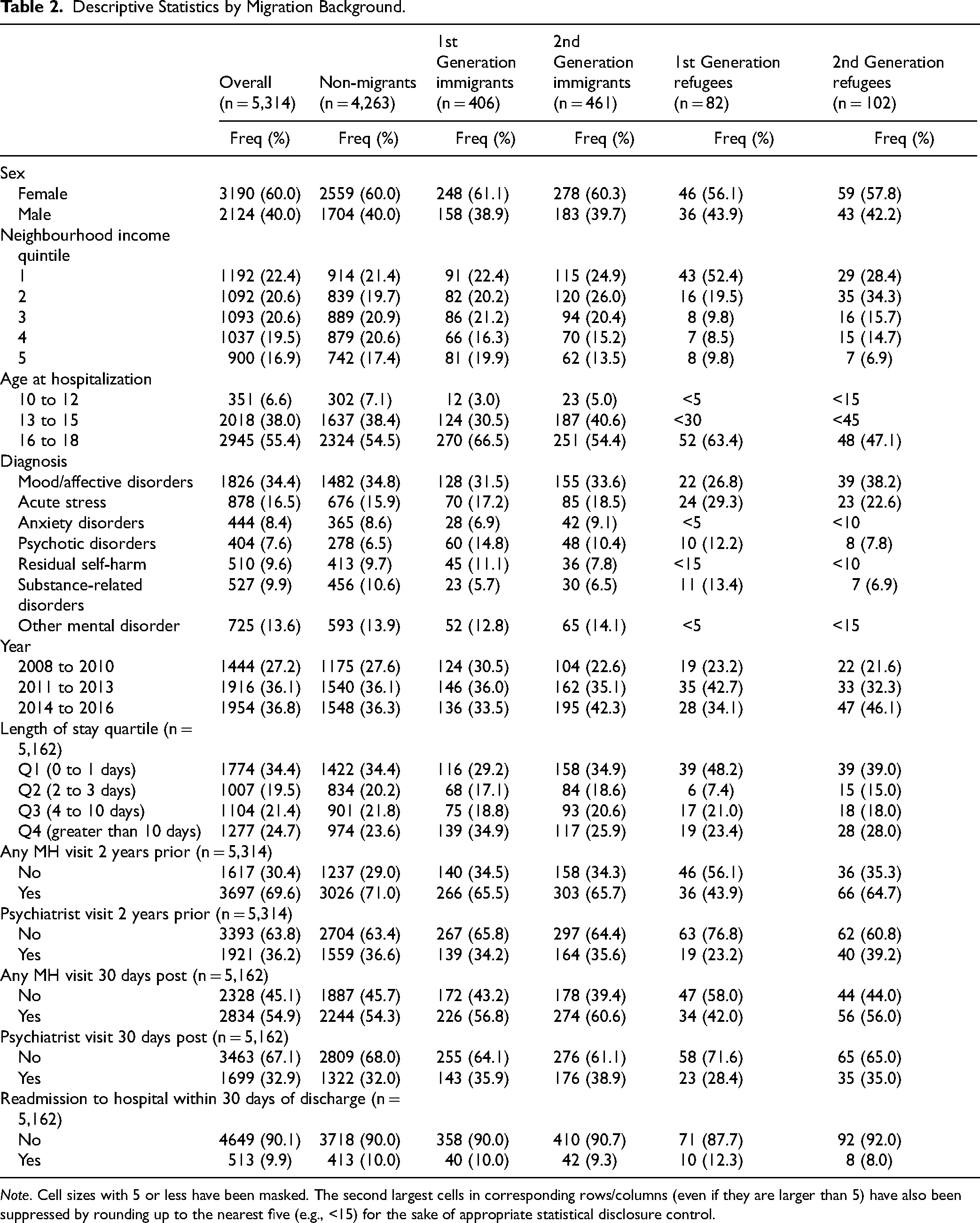
Note. Cell sizes with 5 or less have been masked. The second largest cells in corresponding rows/columns (even if they are larger than 5) have also been suppressed by rounding up to the nearest five (e.g., <15) for the sake of appropriate statistical disclosure control.
Mental Health Outpatient Care in the Two Years Before Hospitalization
All results presented here are for the adjusted models reported in Table 3, unless otherwise noted.
Relative Odds of Mental Health Contact in the Two Years Before Hospitalization by Socio-Demographic and Diagnostic Groups (n = 5,314).
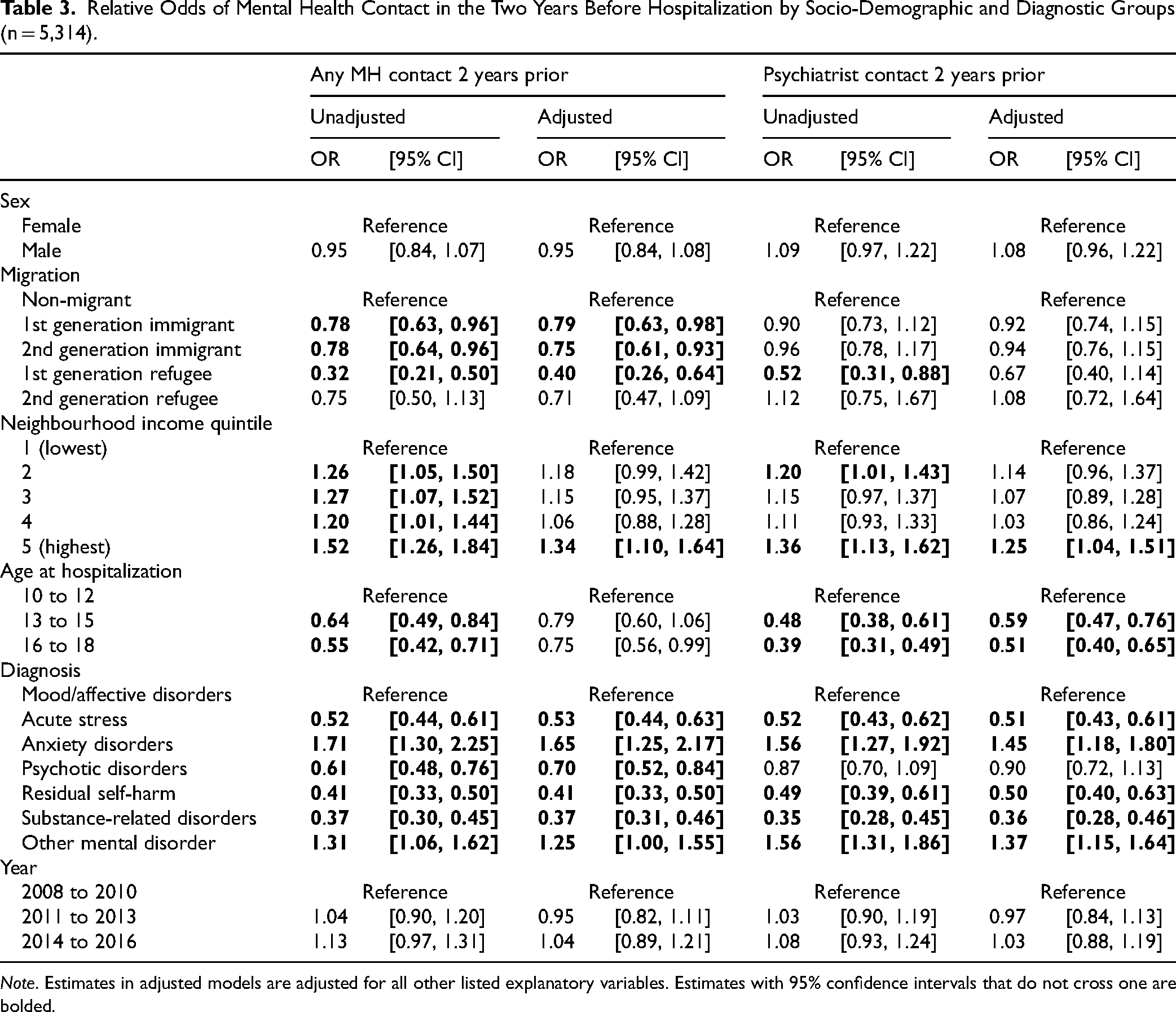
Note. Estimates in adjusted models are adjusted for all other listed explanatory variables. Estimates with 95% confidence intervals that do not cross one are bolded.
Migration Background
First- and second-generation immigrant adolescents and, to a greater degree, first-generation refugee adolescents, were significantly less likely than non-immigrants to have had any mental health visit in the two years before mental health hospitalization.
Sex
No significant sex differences in mental health outpatient care in the two years before hospitalization emerged.
Neighbourhood Income Quintile
Adolescents in the highest income quintile were more likely to have had any mental health visit or psychiatrist visit in the two years before hospitalization in comparison to those in the lowest income quintile.
Age
Compared to younger (10–12) adolescents, older adolescents (13–15, 16–18) were less likely to have had a psychiatrist visit in the two years before hospitalization. This age pattern was also observed for any mental health visits in the two years before hospitalization, although the significant association did not hold after adjusting for other predictors.
Diagnosis
Compared to adolescents hospitalized for mood/affective disorders (ref), adolescents hospitalized for acute stress, psychotic disorders, residual self-harm and substance-related disorders were significantly less likely to have had any outpatient mental health visits in the two years before hospitalization and (except for psychotic disorders) significantly less likely to have had a psychiatrist visit in the two years prior. Adolescents hospitalized for anxiety disorders and “other” mental disorders were significantly more likely than those with mood/affective disorders to have had any mental health outpatient visit or psychiatrist visit in the two years before hospitalization.
Year
Time period of hospitalization was not significantly associated with mental health outpatient contact in the two years before hospitalization.
Mental Health Outpatient Care in the 30 Days Following Hospitalization
All results reported here are based on the adjusted models presented in Table 4, unless otherwise noted.
Relative Odds of Mental Health Contact 30 Days Following Hospitalization by Sociodemographic and Diagnostic Groups (n = 5,162).
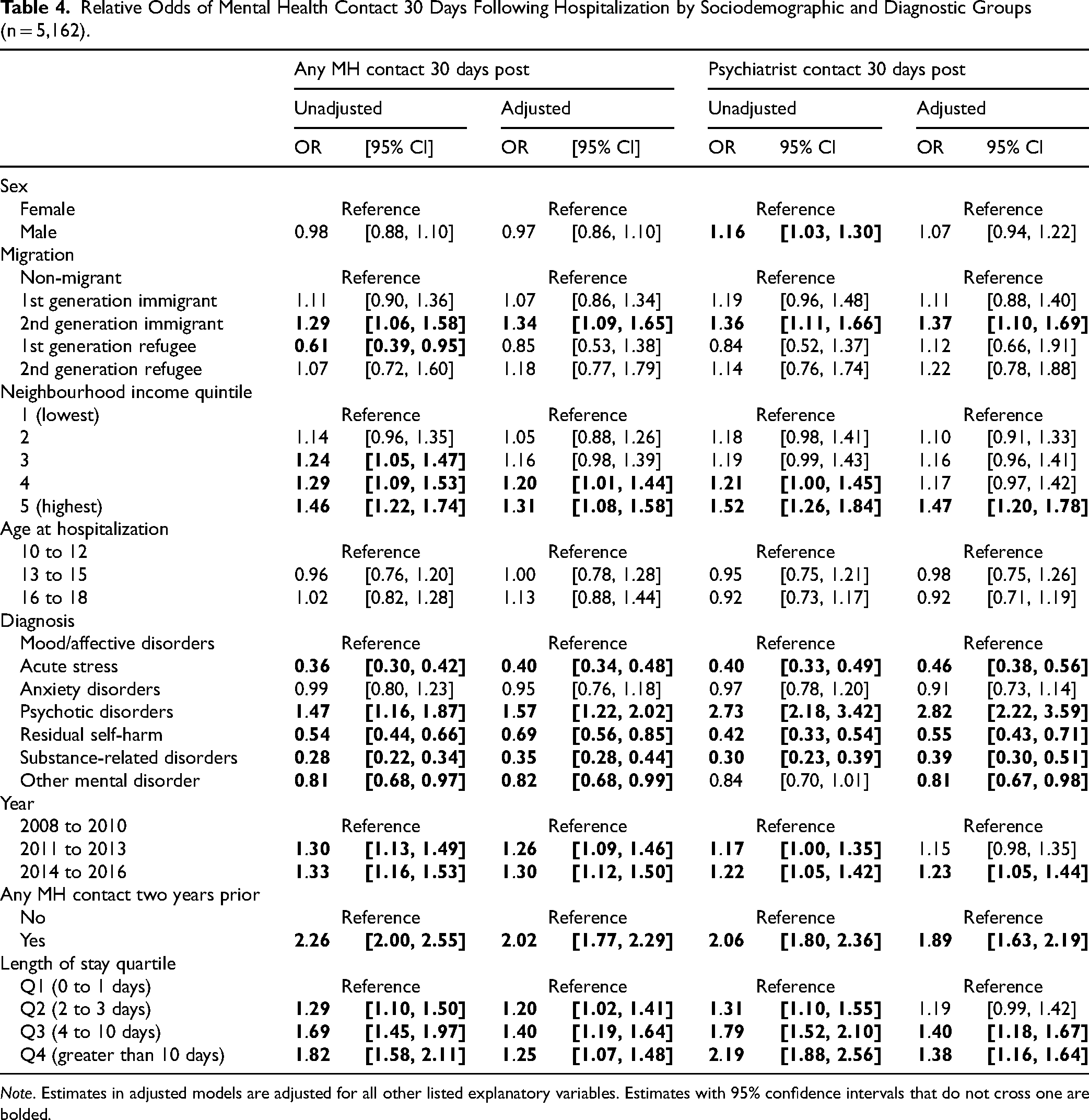
Note. Estimates in adjusted models are adjusted for all other listed explanatory variables. Estimates with 95% confidence intervals that do not cross one are bolded.
Migration Background
Second-generation immigrant adolescents were significantly more likely than non-immigrants to have had any mental health visit or psychiatrist visit within 30 days following hospitalization. First-generation refugees were significantly less likely than non-immigrants to have had any mental health outpatient contact in the 30 days following hospitalization although this association was not significant after adjusting for the other explanatory variables.
Sex
No significant sex differences were found in mental health contact in the 30 days following hospitalization in the adjusted models.
Neighbourhood Income Quintile
Adolescents from the highest neighbourhood income quintile were significantly more likely to have had a mental health visit and a psychiatrist visit in the 30 days following hospitalization compared to those from neighbourhoods with the lowest income quintiles.
Age
Age at hospitalization was not significantly associated with any mental health outpatient or psychiatrist visits in the 30 days following hospitalization.
Diagnosis
Adolescents hospitalized for acute stress, self-harm, substance-related and “other” mental disorders were less likely than those hospitalized for mood/affective disorders to have had any mental health visit or psychiatrist visit within 30 days of hospitalization. Those hospitalized with a psychotic disorder were significantly more likely than those hospitalized for a mood/affective disorder to have had any mental health visit or psychiatrist visit within 30 days following hospitalization.
Year
Adolescents hospitalized in later years (2014–2016) were more likely than those in earlier years (2008–2010) to have had any mental health visit or psychiatrist visit within 30 days following hospitalization.
Mental Health Contact Two Years Prior
Adolescents who had had mental health contact in the two years before hospitalization were significantly more likely to have a mental health outpatient visit or psychiatrist visit in the 30 days following hospitalization.
Length of Stay
Finally, those with longer lengths of stay were significantly more likely to have a mental health visit or psychiatrist visit within 30 days of hospitalization.
Discussion
The study found that among adolescents in BC hospitalized for a mental health condition, nearly one-third (30.4%) did not have a documented outpatient mental health visit in the two years preceding hospitalization. This indicates that a high proportion of adolescents did not receive any physician-based outpatient mental health care before reaching a level of severity that necessitated hospitalization—and this was disproportionately so for adolescents from immigrant and refugee backgrounds. From an early intervention perspective, these findings highlight the need for alignment with clinical guidelines that advocate for the treatment of mental disorders primarily through outpatient services.
In the 30 days after hospitalization, 45.1% of adolescents had no documented physician-based outpatient mental health care (67.1% did not see a psychiatrist). The likelihood of receiving outpatient care during the follow-up period differed by diagnosis type. In comparison to mood/affective disorders, adolescents hospitalized for psychotic disorders were more likely to receive follow-up care, while those hospitalized for substance-related disorders, residual self-harm, and acute stress were less likely to have received outpatient follow up care within 30 days. The greater likelihood of follow-up outpatient care in the case of psychotic disorders may be due to the severity of the disorder and the greater need for acute medication management. There are also a number of services and supports available for the management of psychotic disorders in the province (e.g., through the BC Psychosis Program or the Early Psychosis Intervention Programs). Understanding the reasons for variations in outpatient care following hospitalization, and their potential impact on treatment outcomes is an important area for future research, especially given that timely follow-up care has been associated with better treatment outcomes.12–14 Notably, nearly 1 in 10 (9.9%) adolescents with a mental health-related hospitalization were readmitted to hospital within 30 days of discharge. This is an outcome that warrants further examination from a safety and effectiveness lens.
We found that first-generation refugee and first- and second-generation immigrant youth were less likely than non-immigrant adolescents to have received outpatient mental health care in the two years prior to hospitalization. This pattern suggests that hospitalizations are more likely to be the first point of physician-based mental health contact for newcomers to Canada, particularly for first-generation refugees. This is consistent with an Ontario study, which found that emergency department visits were more likely to be the first point of contact for refugees and recent immigrants. 18 High rates of hospitalization as the first mental health contact are potentially indicative of poor access to outpatient mental health care—and is used as a mental health system performance indicator. 31 Adolescents from immigrant and refugee backgrounds were over-represented in the lowest income quintiles (particularly those from refugee backgrounds)—further widening treatment disparities before hospitalization between immigrant, refugee and non-immigrant groups. First-generation refugee adolescents were the least likely to have received outpatient mental health care in the two years before their mental health hospitalization, compared to non-immigrant adolescents. This is particularly notable, as young refugees may have experienced persecution and trauma, making them vulnerable to mental health issues. 32
These are concerning patterns given the importance of having a regular, trusted primary care provider as an entry point to the health care system. A regular outpatient care entry point is not only associated with higher patient satisfaction and trust, but with higher overall quality of care and outcomes, including less reliance on emergency services, reduced need for hospitalizations and a greater uptake of preventative care. 33 Access to primary health care is considered foundational to a well-functioning health care system as it promotes health and wellbeing and helps prevent diseases, including mental health conditions, and related hospitalizations. 33 In many cases, hospitalizations and potentially more acute mental illness, may be preventable if preceded by appropriate outpatient mental health care. 11
The disproportionate lack of outpatient care in the lead-up to hospitalization for first-generation immigrant and refugee youth underscores a critical health inequity. Several factors may explain why immigrant and refugee adolescents are less likely to access outpatient mental health services. A recent review identified key barriers faced by immigrant populations in Canada, including cultural discrepancies and discomforts (e.g., culturally prominent social stigmas, differing expectations of healthcare providers), communication challenges, socio-economic obstacles (e.g., transport, childcare) and health system structural barriers (e.g., concerns about invasive technology). 34 Yet, access to health care is not only a function of individual characteristics and abilities (e.g., one's ability to perceive need, seek, reach or pay for services), but also the capacity of the health care system to respond to the needs of individuals in a way that makes health care more approachable, acceptable, available, affordable and appropriate. 35 A promising approach in BC is an integrated youth health and wellness service model (e.g., Foundry 36 ), which incorporates elements that are designed to reduce barriers to accessing mental health services (e.g., integrated services, walk-in and virtual services for youth). More research is needed to understand whether this approach is effective at reducing barriers specifically for adolescents from immigrant and refugee backgrounds with specific social, cultural and linguistic needs.
With respect to outpatient mental health or psychiatrist care within 30 days following their hospitalization, second-generation immigrant adolescents were more likely than non-immigrants to receive care. However, worth noting is the lack of significant differences in outpatient follow-up care between youth with other immigrant and refugee backgrounds and non-immigrant youth after adjusting for other factors. Altogether, these findings may indicate that hospitalization could have served as a connection point to the outpatient mental health care system for those previously unconnected, but needs to be explored further in future research.
Limitations
This study has some important limitations. The study only captures fee-for-service outpatient practitioner visits captured through BC's universal health insurance (MSP) program. This is important to note because adolescents may have accessed allied, non-physician-based mental health services not covered by MSP or physician services provided under alternative payment plans and therefore would not be captured in the MSP billing data (including mental health services offered for newcomers to BC). Recent evidence in a Canadian context suggests that non-physician based mental health contacts are common amongst children and adolescents. 37 Having the ability to capture non-physician-based mental health services outside of the MSP program (e.g., through private practice, in schools, by social workers, the provincial Child and Youth Mental Health Teams, or Foundry—Integrated Youth Services) would provide a more complete picture of differential access and barriers to mental health services. Past research suggests that immigrant and refugee children and youth are less likely than their counterparts to access mental health services in general38,39 but research that includes diverse forms of mental health care access would provide a better indication of the different type of services each group may be accessing. Further to this, we note that undocumented migrants are not captured in the present study. Although there are currently no known accurate estimates of the number of undocumented migrants in Canada, this is a sub-population that requires further attention. 40
We note that the findings apply to the specific study time period, migration wave and provincial context. The study time period does not capture the health care system impacts experienced over the past several years, namely changes in mental health service use during the COVID-19 pandemic and in its aftermath. Overall, child and youth mental health hospitalizations declined and physician visits went up from the pre-pandemic to post-pandemic period, 41 but it remains to be seen whether these patterns are consistent for immigrant and refugee youth and this is an important area for future research. Note that the study does not capture the most recently arrived immigrants and refugees. This includes recent refugee claimants or others who were not yet covered under MSP or were covered under a federal health insurance program, or those recent immigrants/refugees who were not in the province/country long enough to meet the 2-year presence criterion. The study captures the BC context only. Given that healthcare is mainly a provincial jurisdiction, it remains an important question as to whether the study findings would be consistent across other provinces.
Finally, this study was unable to account for the severity of mental disorders. Some adolescents may require more outpatient care before and after hospitalization depending on the severity of the mental disorder or incident that led to their hospitalization. Severity/acuity likely influences the likelihood of receiving outpatient care and this may differ by migration background, which represent key areas for future research.
Conclusion
First- and second-generation immigrants and refugees comprise a significant, and growing, proportion of the Canadian population. 42 As noted by the World Health Organization, “the ability of the health-care system to deal with growing linguistic and cultural diversity in equitable and effective ways are no longer marginal issues” (WHO report, page 8 33 ). The findings of this study enhance our understanding of the variations in care before and after hospitalization among adolescents from diverse backgrounds. This knowledge is crucial for identifying those who may not be receiving the outpatient care they need, informing health services planning, and addressing disparities in the healthcare system. 14 Future research would benefit from employing both quantitative and qualitative methods to deepen our understanding of care dynamics before and after hospitalization. Future research should also include a focus on other under-represented subpopulations, the most recent migrants and health service use changes during and post-pandemic to develop a more nuanced understanding of the intersecting factors influencing mental health outpatient care and hospitalizations for young people in Canada.
Footnotes
Acknowledgments
The authors gratefully acknowledge funding from the Canadian Institutes of Health Research (CIHR) for facilitating this research. AG also gratefully acknowledges funding from the Canada Research Chairs Program. Data for this study was obtained (via Population Data BC) from the Data Stewardship Committee, the BC Ministry of Health, BC Ministry of Education and Child Care, and Immigration, Refugees, & Citizenship Canada, who approved and provided access to the data for this study. Further information on the data sets used for this project is at: ![]() . Access to data provided by the Data Steward(s) is subject to approval but can be requested for research projects through the Data Steward(s) or their designated service providers. All inferences, opinions and conclusions drawn in this material are those of the author(s), and do not reflect the opinions or policies of the Data Steward(s).
. Access to data provided by the Data Steward(s) is subject to approval but can be requested for research projects through the Data Steward(s) or their designated service providers. All inferences, opinions and conclusions drawn in this material are those of the author(s), and do not reflect the opinions or policies of the Data Steward(s).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Research Chairs, Canadian Institutes of Health Research.