
Abstract
Background:
Internationally, hospital-based short-stay crisis units have been introduced to provide a safe space for stabilisation and further assessment for those in psychiatric crisis. The units typically aim to reduce inpatient admissions and psychiatric presentations to emergency departments.
Aims:
To assess changes to service use following a service user’s first visit to a unit, characterise the population accessing these units and examine equality of access to the units.
Methods:
A prospective cohort study design (ISCTRN registered; 53431343) compared service use for the 9 months preceding and following a first visit to a short-stay crisis unit at three cities and one rural area in England. Included individuals first visited a unit in the 6 months between 01/September/2020 and 28/February/2021.
Results:
The prospective cohort included 1189 individuals aged 36 years on average, significantly younger (by 5–13 years) than the population of local service users (<.001). Seventy percent were White British and most were without a psychiatric diagnosis (55%–82% across sites). The emergency department provided the largest single source of referrals to the unit (42%), followed by the Crisis and Home Treatment Team (20%). The use of most mental health services, including all types of admission and community mental health services was increased post discharge. Social-distancing measures due to the COVID-19 pandemic were in place for slightly over 50% of the follow-up period. Comparison to a pre-COVID cohort of 934 individuals suggested that the pandemic had no effect on the majority of service use variables.
Conclusions:
Short-stay crisis units are typically accessed by a young population, including those who previously were unknown to mental health services, who proceed to access a broader range of mental health services following discharge.
Keywords
Introduction
Internationally, psychiatric crisis care services are under intense pressure (The Strategy Unit, 2019). An increasing number of visits to emergency departments (ED) for mental health crisis care and decreasing numbers of inpatient beds (Fleury et al., 2019) has result in long waits in ED (Nicks & Manthey, 2012). Concomitantly it is unclear whether short stays on psychiatric wards followed by early discharge are beneficial (Clibbens et al., 2018). Inpatient stays can be unnecessary (Stulz et al., 2015), costly (McCrone et al., 2009) and detrimental (Thibaut et al., 2019). In crisis services, service users’ needs are the most acute, yet their voices can often be ignored (Srebnik & Russo, 2008). For service users, shared decision-making, feeling respected and having basic comforts are priorities when in crisis (Thomas et al., 2018). Within this difficult context, a new type of service is emerging to reduce the pressure on ED and psychiatric wards. Short-stay crisis units, also known as Psychiatric Decision Units (PDU), Mental Health Decision Units, Crisis Stabilisation Units, or Psychiatric Emergency Services have been introduced in Australia (Braitberg et al., 2018), Belgium (Spooren et al., 1997), Canada (Mok & Walker, 1995), The Netherlands (Van Der Sande et al., 1997), the US (Stamy et al., 2021) and England (Trethewey et al., 2019).
In England, psychiatric ward occupancy rates in the publicly funded National Health Service (NHS) have long tended to exceed recommended levels (Crisp et al., 2016), sometimes resulting in long delays for a hospital bed for those in crisis. People presenting with psychological distress at a general hospital ED are over six times more likely than those with physical presentations to breach the 4-hour waiting time target (NHS England et al., 2014), resulting in difficult experiences in noisy environments. PDUs, which are typically designed to alleviate pressure on ED and reduce inpatient admissions can provide an alternative (Goldsmith et al., 2021). A national survey in England identified six units – all were open 24/7 and had maximum stays of 12 to 72 hours. All accepted voluntary (informal) service users only and provided recliner chairs for sleeping rather than beds. Units are staffed by senior mental health nurses and healthcare assistants, with input/oversight from psychiatrists. The staff: patient ratio is high, approximately one member of staff per two service users in daytime hours (Goldsmith et al., 2021). As in other countries, PDUs in England emerged to address pressures on the crisis care pathway, leaving formal evaluation of the units to follow their development, in response to policy initiatives (Department of Health and Concordat Signatories, 2014; NHS England et al., 2014).
A subsequent, comprehensive systematic literature review on hospital-based short-stay crisis units included 12 studies from six countries with a total of 67,505 participants (Anderson et al., 2022). A wide range of comparison groups were used in the included studies including four pre/post studies comparing service use data before and after the unit opened (Braitberg et al., 2018; Browne et al., 2011; Lester et al., 2018; Stamy et al., 2021). A single interrupted time-series compared pre-post data (Parwani et al., 2018). Five studies compared the PDU to other units (Gillig et al., 1989; Kealy-Bateman et al., 2019; Mok & Walker, 1995), one compared referral routes (Trethewey et al., 2019) and one compared to an inpatient service (Schneider & Ross, 1996). Additionally there was a case-control study (Spooren et al., 1997) and a randomised controlled trial (Van Der Sande et al., 1997). Pooled estimates indicated a reduction in ED length of stay by about 2 hours and 40 minutes (−164.24 minutes, 95% CI [−261.24 to −67.23] minutes), and that the odds ratio of an ED presentation for psychiatric crisis leading to an inpatient admission were approximately halved (OR = 0.55, 95% CI [0.43–0.68]) (Anderson et al., 2022). The units were found to have a wide range of effects which seem likely to be connected to staffing levels, how the units are oriented towards their stated aims and the surrounding crisis care services. None of these prior studies examined equality of access to the service, changes to service use following a visit to a unit at an individual patient level, or examined the effects of the COVID-19 pandemic on service use following discharge from a unit. The present study aims to (1) understand who uses PDUs; (2) examine changes to service use following a service user’s first visit to a unit, (3) assess the effects of the COVID-19 pandemic on service use post-discharge and (4) assess equality of access to the units.
Methods
Setting
This prospective cohort study was conducted in four participating mental health service providers (NHS mental health trusts) in England – London, Birmingham, Sheffield (city sites) and Lincolnshire (a rural site), each with an operational PDU before the study commenced. Key characteristics of study sites, including configuration of the units and other local crisis care services, are in Table 1. Changes to the unit or other crisis care provision during the timeframe of the research, including those resulting from the COVID-19 pandemic are indicated in parentheses.
Key characteristics of study sites.
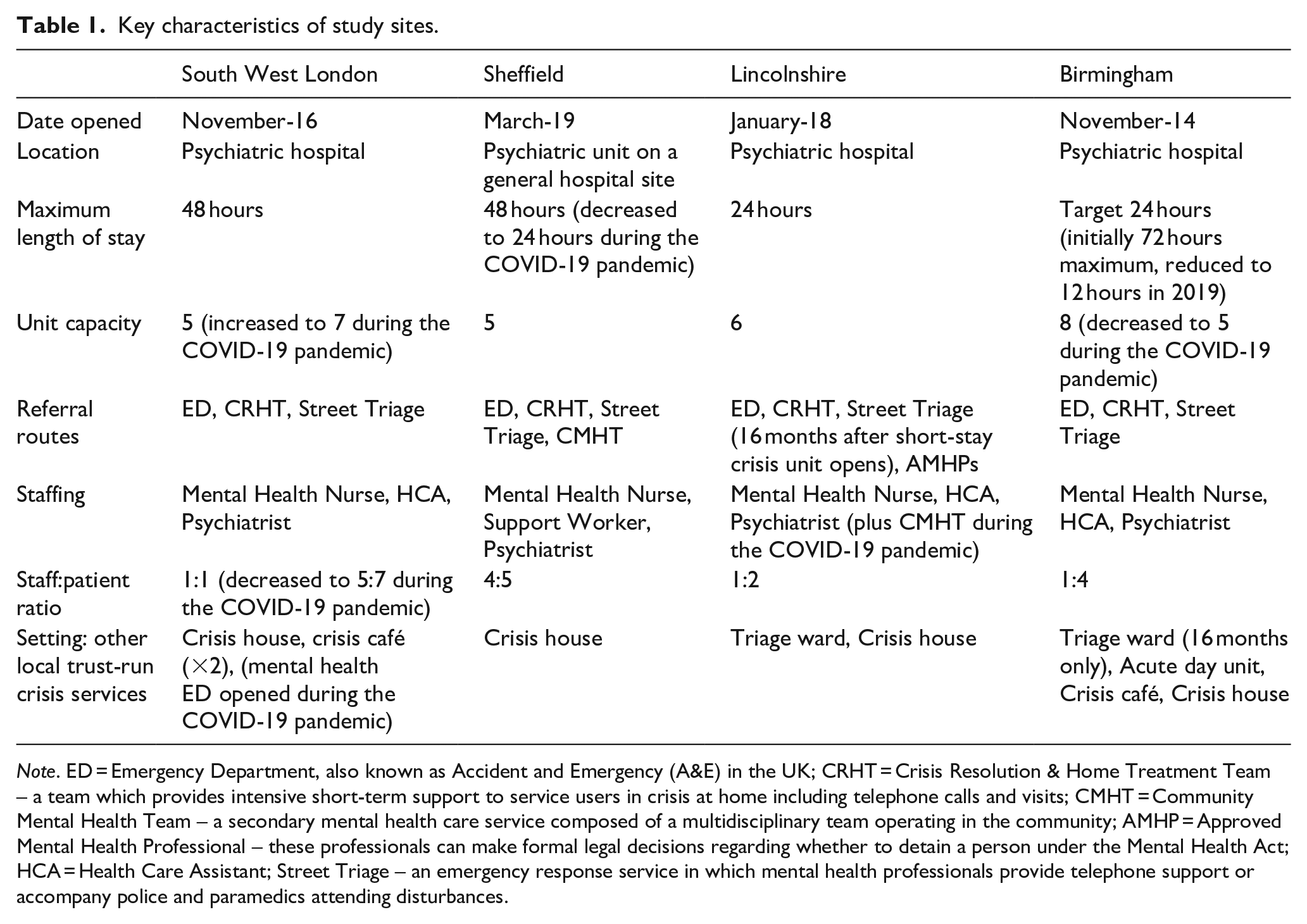
Note. ED = Emergency Department, also known as Accident and Emergency (A&E) in the UK; CRHT = Crisis Resolution & Home Treatment Team – a team which provides intensive short-term support to service users in crisis at home including telephone calls and visits; CMHT = Community Mental Health Team – a secondary mental health care service composed of a multidisciplinary team operating in the community; AMHP = Approved Mental Health Professional – these professionals can make formal legal decisions regarding whether to detain a person under the Mental Health Act; HCA = Health Care Assistant; Street Triage – an emergency response service in which mental health professionals provide telephone support or accompany police and paramedics attending disturbances.
Design
Primary cohort study
The prospective, primary cohort study included all individuals at the four study sites experiencing their first visit to a PDU over a 6-month period between 01/September/2020 and 28/February/2021. The study compared routine service use data for the 9 months preceding this visit (the ‘pre’ period) to the 9 months following (the ‘post’ period). The follow-up period for the study closed on 30/November/2021, allowing complete follow-up for service users who joined the study at the end of the ‘pre’ period. The study is prospective, and was registered with the ISCTRN (53431343) (Goldsmith, 2020) on 11/February/2020.
To characterise the population accessing PDUs, we summarised socio-demographic data including age, ethnicity, gender, diagnosis, marital and employment status, housing, sexual orientation and referral source. The English indices of deprivation 2019 (McLennan et al., 2019) is a measure of relative deprivation, based on seven different, weighted, domains of deprivation: income, employment, crime, living environment, barriers to housing and services, education, skills and development deprivation and health deprivation and disability. We conducted the equalities impact assessment by comparing the demographic characteristics of people in the primary cohort accessing the crisis unit to the general population of service users (calculated over a recent 1-year period) at the corresponding NHS mental health trust.
To address the third aim, to identify whether there were changes to service use following a visit to a unit, we examined two primary outcomes as PDUs are designed to reduce the pressure on both general hospital ED and inpatient wards. First, we examined whether there is a change in informal (voluntary) admissions for the cohort between the pre- and post- periods. Second, we examined whether there were changes to the number of ED presentations, measured as liaison psychiatry episodes (referral to the services providing psychiatry support to ED). We also checked for changes in inpatient admissions, short-stay (0–5 days inpatient admissions), average length of inpatient stays, compulsory admissions, use of community mental health team (CMHT) and other mental health trust specialist services to identify the wider effects of a PDU visit.
Adaptation due to COVID-19: an additional retrospective cohort
Widespread restrictions of movement and social interaction were introduced in England in response to the COVID-19 pandemic on 23/03/2020, during the follow-up period for the primary cohort. The effects of the pandemic on access to care and help-seeking behaviours could affect the generalisability of the results to other periods. Hence the study was adapted to include a retrospective cohort of people who visited a unit 1 year prior to the prospectively designed cohort (eligible first visits to the units were between 01/September/2019 and 28/February/2020). Choosing dates exactly 1 year prior controls for any effect of seasonality on the results. The retrospective cohort includes three of the sites as the fourth site opened their unit during the ‘pre’ period, meaning that complete data for the retrospective cohort could not be obtained from this site.
Coproduction
The present study is part of a larger project, ‘Evaluating mental health decision units on acute crisis care pathways’ (National Institute for Health Research Funding and Awards, Award ID 17/49/70, 2019). The project was coproduced with a national expert panel of people with lived experience of mental health crisis services, a local service user research advisory group and researchers who also have lived experience of psychological distress. This lived experience informed decisions about which outcomes we would collect, which data we included in our equalities impact assessment, and interpretation of results in a data synthesis workshop.
Data extraction and statistical analysis
Data were extracted from electronic patient records by Business Intelligence teams at each site, pseudonymised, securely transferred to the study team, cleaned and analysed. Each cohort population was summarised using descriptive statistics. We tested for differences in service use in the pre- and post-periods using McNemar’s χ2 tests (Fagerland et al., 2013) for binary paired data and paired t-tests bootstrapped with 2,000 replications for continuous data (Efron & Tibshirani, 1994). Unpaired t-tests were used for the average length of inpatient stay – many in the cohort were not admitted to a ward in both the pre- and post-periods – an unpaired test enabled all data to be included in the analysis. The additional, retrospective cohort facilitated examination of whether there were changes in service use due to the COVID-19 pandemic. The number of service users in each cohort was used as a denominator and tests for significant differences in service use across the two post-periods at each site were conducted using odds ratios and unpaired t-tests.
For the equalities impact assessment, summary statistics describing the demographics of those using mental health services in the catchment area of each unit during a recent 1-year period were compared to the demographics of the primary cohort. Z-tests were used to compare the proportions of each demographic (where numbers were sufficient) – this is a valid way of comparing a subgroup drawn from a population to a wider population. Correction for the overlap was not needed as each subgroup represented less than 10% of the whole population (Hayes & Berry, 2006).
Results
Population accessing hospital-based short-stay crisis units
In total, 1,176 people were included in the primary cohort, 277 (23.55%) in South West London, 308 (26.19%) in Lincolnshire, 387 (32.91%) in Birmingham and 204 (17.35%) in Sheffield, as shown in Table 2. Six hundred and nine participants (51.79%) were female, with an average age of 36 years. The predominant ethnicity was White British, which describes 821 (69.81%) of the cohort. Between 55% and 82% of service users at each site had no primary diagnosis. Most people were living in mainstream housing, but not with a partner, and had an occupation. There were no data recorded about sexuality for the majority of the cohort (842 people; 71.60% of participants). A sizeable portion of people were relatively new to mental health services; 372 (38.27%) had their first contact with mental health services in the 9 months preceding their first crisis unit visit (based on data from 3 sites; 972 participants). The English indices of deprivation 2019 (McLennan et al., 2019) mean scores ranged from 3.45 (2.58) to 5.78 (2.34) at each site (lower scores indicate higher deprivation). The large standard deviations indicate substantial variation within sites in the disadvantage of the people in the relatively small local areas accessing the unit. Comprehensive data on participant characteristics by site are provided in Table 2.
Primary cohort – participant characteristics by site.
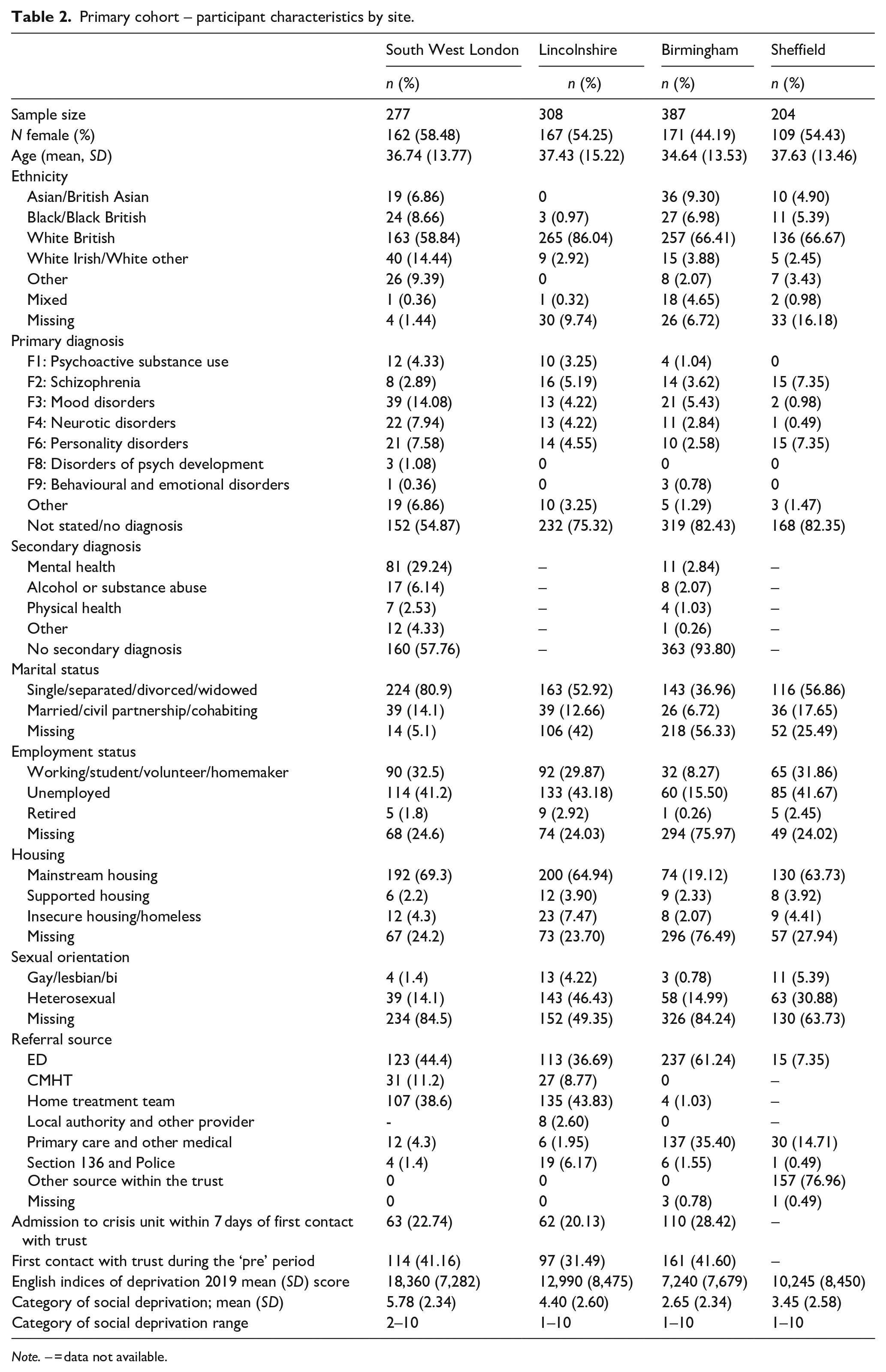
Note. – = data not available.
The ED was the largest single source of referrals (488; 41.50%), followed by the Crisis Resolution and Home Treatment Team, who provide intensive home-based therapies as an alternative to inpatient admission (246; 20.92%). At one site, the majority of participants (157; 76.96%) accessed the crisis unit via single point of access – a single route into all crisis services at that Trust.
Changes to service use following the first visit to a short-stay crisis unit
Typically, there was a marked increase in the use of mental health services following a first visit to a PDU. There were more informal (voluntary) admissions in the ‘post’ period, a difference which reached significance at all but one site (see Table 3). ED presentations were significantly reduced at two sites and unchanged at a further two sites. There were significant increases in both compulsory admissions and inpatient admissions at all sites. At three of the four sites the number of individuals experiencing a short (0–5 days) admission increased, this was significant at two sites. At all four sites there was a very substantial increase of at least 8 days in the average length of an inpatient stay. Due to relatively small numbers admitted to wards combined with a huge variation in the length of these stays (indicated by the very large SD), this increase was significant at only one site – where the mean increase in duration was over 30 days.
Pre-post comparisons (primary cohort).
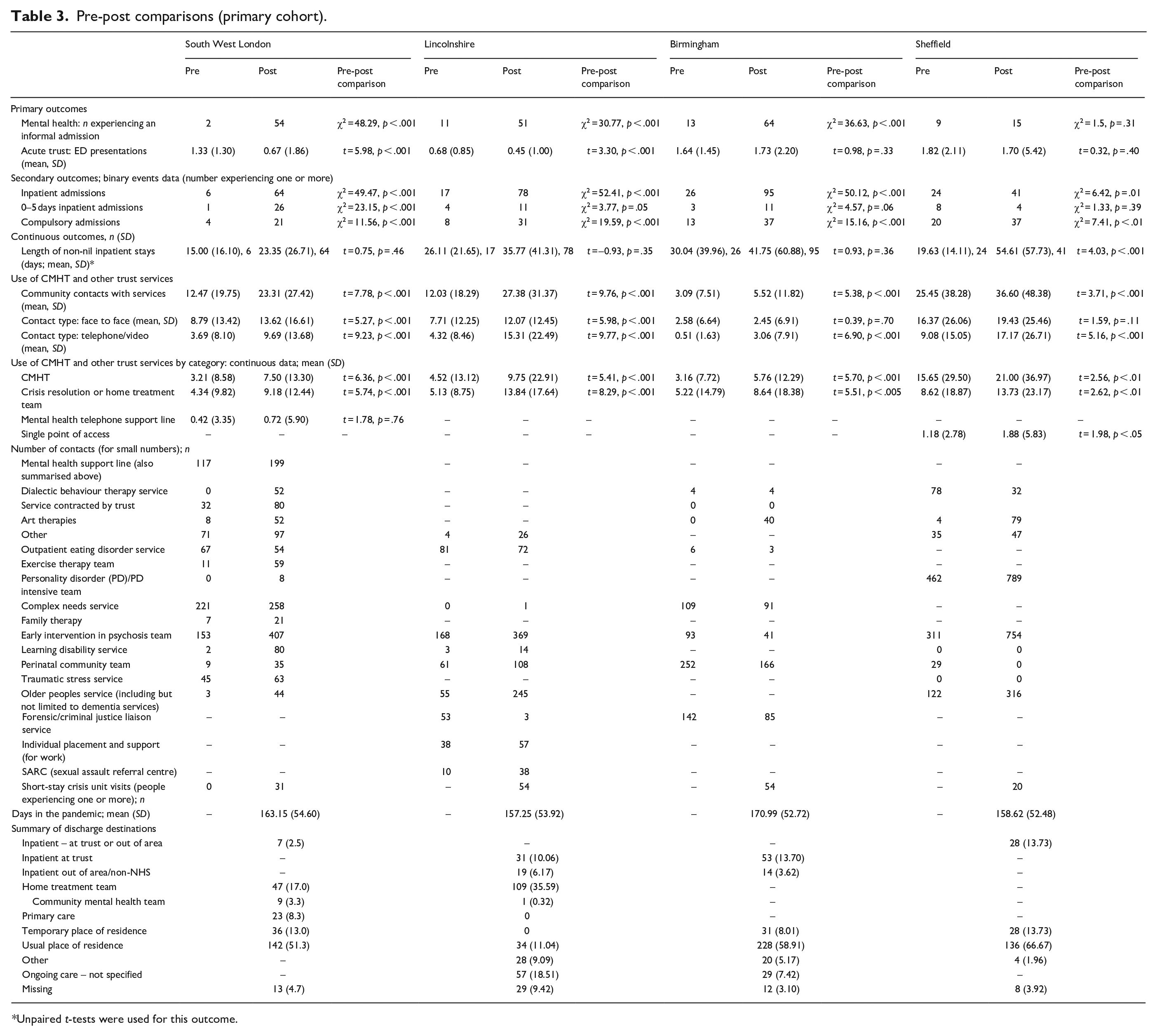
Unpaired t-tests were used for this outcome.
At every site the number of contacts the cohort had with community services was significantly increased in the ‘post’ period. Broken down into face-to-face and remote (telephone/video) appointments, the number of remote appointments significantly increased at all sites – and despite the ‘post’ period overlapping with the COVID-19 pandemic, the number of face-to-face appointments also significantly increased at two sites. Contacts with the community mental health team (CMHT) approximately doubled at three sites, and significantly increased at all sites. Contact with the crisis resolution/home treatment team was similarly increased. Use of the single point of access operating at a single trust also significantly increased. Use of specialised services, which typically increased, is summarised towards the lower part of Table 3. Tests for significance were not used on these data due to the relatively low counts. Following their visit to the unit, participants were typically discharged to their usual place of residence (540; 45.92% participants). A smaller proportion were discharged into the care of the Crisis and Home Treatment Team (156; 16.05%), and 12.76% (124 participants) were discharged to a psychiatric inpatient ward. Across all four sites, social-distancing measures as a result of the COVID-19 pandemic were in place for just over 50% of the follow-up period.
Effect of the COVID-19 pandemic on service use
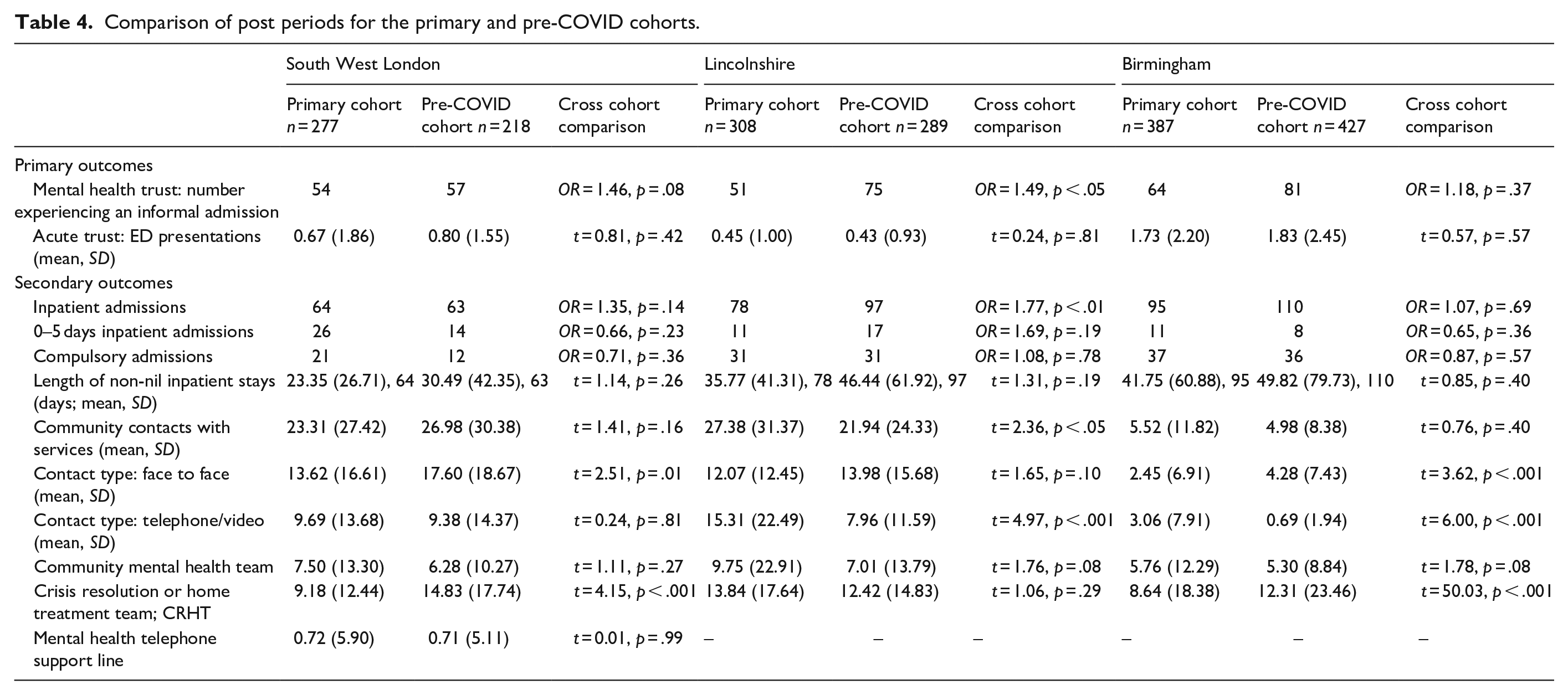
Data describing the post-period of the primary and pre-COVID cohorts were compared to examine whether the COVID-19 pandemic had an effect on service use (see Table 4 for comparisons). The pre-COVID cohort is summarised in the Supplemental Materials. In general, service use was unchanged during the pandemic, with a few exceptions. In Lincolnshire a significantly higher proportion of people experienced an involuntary inpatient admission in the pre-COVID cohort (OR = 1.49, p < .05); this is also reflected as a higher proportion of people experiencing any type of admission in the pre-COVID cohort at this site (OR = 1.77, p < .01). The proportion of face-to-face appointments at two sites (London and Birmingham) were significantly reduced in the primary cohort (t = 2.51, p = .01 and t = 3.62, p < 0.001 at each site, respectively). Similarly, appointments with the CRHT decreased significantly in both London (t = 4.15, p < .001) and Birmingham (t = 50.03, p < .001). There was no evidence of difference for any of the other outcomes.
Comparison of post periods for the primary and pre-COVID cohorts.
Equalities impact assessment
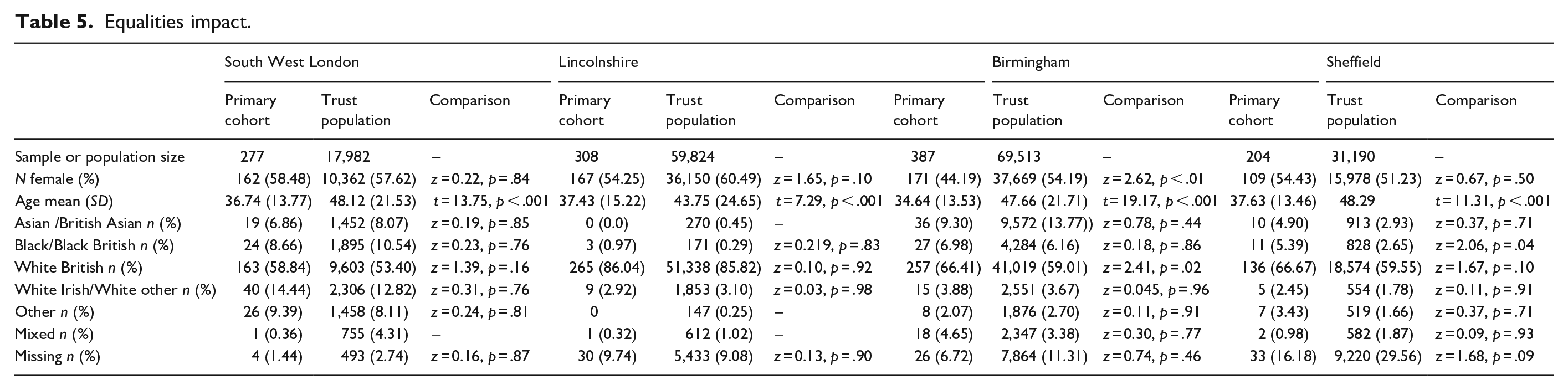
To assess equality of access to the units, demographic characteristics of the primary cohort and a recent sample of all people using mental health services at the local mental health Trust were compared (Table 5). Across all sites there is a consistent trend that the population accessing the units was significantly younger (by, on average, 5–13 years) than the population of service users at the Trust. At one city site, first-time visitors to the PDU were significantly less likely to be female compared to the Trust-wide population (171/387 [44.19%] compared to 37,669/69,513 [54.19%]; z = 2.62, p < .01) and significantly more likely to be White British (257 [66.41%] compared to the Trust population 41,019 [59.01%], z = 2.41, p = .02). At the rural site the population was predominately White British, both at the Trust and cohort levels. At a second city site, service users accessing the crisis unit were more likely to be Black than the Trust population (11/204 [5.39%] compared to 828/31,190 [2.65%]; z = 2.06, p = .04), although the small number of Black individuals in the cohort (11) make it difficult to draw statistically reliable conclusions.
Equalities impact.
Discussion
This study aimed to understand who uses short-stay psychiatric units, assess equality of access to the units and examine change in service use following a service user’s first visit to a crisis unit (termed PDU in the UK). We also aimed to assess the effects of the COVID-19 pandemic on service use post-discharge from a PDU. The population accessing PDUs was consistently younger across all sites than a recent sample of all people using mental health services at each site. In one site, there were significantly fewer female and White British first-time visitors to the unit than one would expect compared to the wider Trust population. In another site, more service users using the unit for the first time were Black compared to the Trust population, although this result was based on small numbers.
Inpatient admissions increased in the period following first visit to a PDU (compared to a similar period pre-first visit) at all sites, including increases in voluntary and compulsory admissions. At three of four sites the number of individuals experiencing a short (0–5 days) admission increased. At all four sites there was an increase in length of inpatient stay. There was a substantial increase in use of community mental health services at all sites, including community-based crisis teams. A wider range of specialist mental health services were accessed by service users in the ‘post’ period compared to the ‘pre’ period. A reduction in ED presentations in the period post-first visit to PDU was observed at two sites, but was unchanged at the other sites.
Overall, the effect of the pandemic on service use post-first visit to a PDU was minimal, especially in terms of inpatient admissions. There was some effect on types of contacts, with fewer face-to-face community appointments and fewer appointments with crisis resolution and home treatment teams in two sites during the pandemic, while in two sites there were increases in remote contacts (face-to-face contacts also increased in two sites).
Comparison with the literature
People accessing crisis services in mental health Trusts in England are typically younger than the mean age of all people using mental health services we observed in our study (Lloyd-Evans et al., 2020), but our cohort of first time PDU visitors was younger still. We note that a relatively high proportion of our participants had only recently accessed any mental health care. As such it is possible that PDUs offer a first access point to mental health care for some people, and as such units may benefit from being oriented towards working with a younger demographic. An established literature is indicative of inequalities in care pathways in mental health services for people from some racialised communities (Bhui et al., 2003), including among young people accessing mental health care (Chui et al., 2021). There were indications at some sites that people visiting a PDU for the first time were either less likely to be White British, or more likely to be Black, but this was not consistent across sites and based on a small amount of data. Further research is needed to establish whether PDUs might improve access to mental health care for people who otherwise experience inequalities of access.
We note that many short-stay crisis units internationally are established with the intention of reducing psychiatric inpatient admissions, with evaluations indicating an overall drop in admissions at a service level following opening of the units (Gillig et al., 1989; Lester et al., 2018; Stamy et al., 2021). However, at the individual patient level, our study indicated a general increase in admissions post-first visit to a PDU. Again, we note that for many of our participants this was an early contact with mental health services and so units might function for some as an entry to appropriate care. Some of the units we evaluated also had an explicit assessment and signposting function (Goldsmith et al., 2021; Trethewey et al., 2019), and so onward referral to either community or inpatient care might be appropriate in some cases. The fact that inpatient stays were longer post-first visit to PDU may be indicative of a higher proportion of planned admissions, rather than very brief admissions than can be typical of crisis and for which evidence of beneficial effect is limited (Clibbens et al., 2018). Increased access to community mental health services post-first visit to a PDU was also a potentially positive outcome as lack of engagement with community care has been shown to be a risk factor for admission (Karasch et al., 2020; Walker et al., 2019), while crisis and home treatment teams have had some success in reducing admissions (Stulz et al., 2020), especially where quality of care is high (Lloyd-Evans et al., 2020). Furthermore, in England as elsewhere, some people experience multiple, repeat mental health presentations to ED (Care Quality Commission, 2014; Okorie et al., 2011). More research is needed to establish whether the increase in mental health service use post-first visit to ED we observed is evidence that that group of people are successfully being signposted, from ED, via a short stay crisis unit to appropriate mental health care. We did see some evidence of a reduction in ED presentations in our cohort after the first PDU visit. This appears promising, although this result is not replicated in findings elsewhere (Anderson et al., 2022), and it is worth noting that a large proportion of our participants were referred to the PDU from ED and so this might be an artefact of the research.
Short stay crisis units and the COVID-19 pandemic
The psychological challenges of the COVID-19 pandemic and social distancing measures were widely considered to present huge psychological challenges (Gruber et al., 2021) and population-level mental health in the UK deteriorated during the first wave of the pandemic (Jia et al., 2020; Pierce et al., 2020). In the early phase of the pandemic, immediate service challenges related to controlling infection in inpatient settings and establishing remote working in the community (Johnson et al., 2021). Pooled data pertaining to the European COVID-19 first wave peak (April 2020) found psychiatrists treated half as many patients in outpatient settings compared to usual (Rojnic Kuzman et al., 2021). As such our finding that there was little overall change in both inpatient and community service use between our primary and pre-pandemic cohorts is interesting (the switch from face-to-face to remote contacts in some sites not withstanding), suggesting perhaps that crisis care was prioritised and suffered less from the pandemic than routine care (Johnson et al., 2021). Other research has indicated that some people with pre-existing mental health conditions were able to adapt to challenges posed by the pandemic in part by seeking alternative sources of help (Shah et al., 2022). It is possible that PDUs were able to signpost people to a range of helpful community-based support, as suggested by our data.
Strengths and limitations
We note this is the only historically controlled study examining the impact of visiting a short-stay crisis unit on individual service use. Other evaluations typically compare organisational-level outcomes between those who access a crisis unit and those who access other forms of crisis and acute care (Gillig et al., 1989; Kealy-Bateman et al., 2019; Mok & Walker, 1995; Schneider & Ross, 1996; Trethewey et al., 2019). As such, the present paper makes a valuable contribution to understanding the potential impact on individual crisis care pathways, although it may be that studies which take this historical approach compare a period of crisis with a period of relative stability, and are therefore not identifying a true casual effect of the PDU. A strength of the study is that all eligible service users are included in the sample, reducing any potential selection bias and enhancing generalisability and applicability. Use of routinely collected data (e.g. number of appointments and hospital admissions) is another strength where these are comprehensively recorded, although substantial missing data for some important demographic variables including ethnicity and sexual orientation was a limitation. Our analysis of the effect of the COVID-19 pandemic using a pre-post design controls for differences between cohorts as a result of seasonality. However, we cannot be certain that any differences in outcomes between the primary and pre-COVID cohorts are solely related to the pandemic.
Conclusions
Our study suggests that short-stay crisis units might help people in mental health crisis, visiting a crisis unit for the first time, to access a wide range of inpatient and community mental health care. This may especially be the case for people who are new to mental health services and for younger people using mental health services. As such, short-stay crisis units may make a useful contribution to mental health crisis care pathways.
Supplemental Material
sj-docx-1-isp-10.1177_00207640221142530 – Supplemental material for Service use preceding and following first referral for psychiatric emergency care at a short-stay crisis unit: A cohort study across three cities and one rural area in England
Supplemental material, sj-docx-1-isp-10.1177_00207640221142530 for Service use preceding and following first referral for psychiatric emergency care at a short-stay crisis unit: A cohort study across three cities and one rural area in England by Lucy Pollyanna Goldsmith, Katie Anderson, Geraldine Clarke, Chloe Crowe, Heather Jarman, Sonia Johnson, Jo Lomani, David McDaid, A-La Park, Jared G Smith and Steven Gillard in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We would like to thank the St George’s, University of London Peer Expertise in Education & Research (PEER) group for their contribution to the design of this project and the DECISION lived experience group for coproducing with us.
Conflicts of interest
None.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute of Health Research (NIHR) Health Services and Delivery Research (Grant Number 17/49/70); ![]() . The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethics approval and consent to participate
The project was given favourable opinion from the East Midlands Leicester South Research Ethics Committee (19/EM/0226) on 12th August 2019; subsequent amendments were approved and the study was run in accordance with Good Clinical Practice guidelines.
Data availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.