
Abstract
Background:
Depression and anxiety-related disorders are common among adolescents. Research attention to early adolescence and low-income ethnically diverse populations is limited.
Aim:
To conduct screening for depression and anxiety at an early age with attention to gender and socioenvironmental context within a low-income setting.
Method:
Mixed methods included the PHQ-9A and GAD-10 screening instruments and ethnographic interviews.
Results:
75 ethnically diverse middle school students were included. Mean years age was 11.2 (0.74). Females had higher PHQ-9A sum scores than males (p = .002, Mann-Whitney test) and higher GAD-10 sum scores than males (p = .016, Mann-Whitney test). After controlling for multiple comparisons, girls had higher mean responses on three PHQ-9A items (p < .006, two-sided t-test) and only one GAD-10 item (p < .005, two-sided t-test). Ethnographic interviews revealed contexts associated with girls’ experiences of depression and anxiety, including gender-based violence in both school and home environments. Salient for girls and boys alike were worries about consequences of COVID-19 for family with respect to illness, death, job loss, economic hardship. Fears over student perceptions of intensified discrimination and racism in school and community were prominent. These problems were experienced by students as barriers to educational engagement.
Conclusion:
Specific attention to early adolescence is needed to identify emergence of subsyndromal conditions which may benefit from therapeutic attention to reduce symptom severity, identify sociocultural, structural, and gender-specific stressors, and to enhance educational engagement.
Introduction
While the mental health of adolescents has been the subject of investigation for decades now (Cohen et al., 1993; Kazdin, 1993; Rutter & Stevenson, 2008), research is needed to more precisely delineate factors associated with the development of mental disorder. For adolescents, depression and anxiety-related disorders are common, often occurring as comorbid conditions (Garber & Weersing, 2010; Seligman & Ollendick, 1998). While previous research has identified domains of broad risk such as adolescence, gender, and psychological stress (Kuehner, 2017; Nolen-Hoeksema, 1990; Petersen et al., 1991), empirical research is needed to identify specific factors within social context. While the impact of these factors may vary globally, current studies indicate that risk factors are disproportionately greater in low-income settings (GBD 2019 Mental Disorders Collaborators, 2022). A working foundation to approach the goal of greater specificity of our understandings of adolescent mental health is usefully guided by three considerations.
First, is the burgeoning field of global mental health which has expanded focus to include child and adolescent populations (Kessler et al., 2009; Kieling et al., 2011). The World Health Organization (WHO, 2022a) recently reported that 14% of adolescents (based on an age range of 10–19 years) lived with a mental disorder in 2019. While studies of the global burden of disease continue to show mental disorder as a leading cause of disability, childhood and adolescence is the period during which this vulnerability is observed to steadily increase (GBD 2019 Mental Disorders Collaborators, 2022). Second, current reports of the age of onset of mental disorder range from over one-third of cases before age 14 (Solmi et al., 2022) to approximately half of all cases by age 14 (Revet & Kennedy, 2022). Thus, early onset of illness is not uncommon and may call for early intervention as needed and possibly more efficacious (Correll et al., 2018; Fusar-Poli et al., 2017). In parallel fashion, early onset provides the research rationale to focus on a younger age than typically investigated. Third, while still in early stages, studies of COVID-19 and mental health have identified detrimental impacts of the pandemic (Necho et al., 2021; Samji et al., 2022; Torales et al., 2020). Recent estimates from the World Health Organization find an overall increase of 25% in the global prevalence of anxiety and depression, with youth and women among the most affected (GBD 2019 Mental Disorders Collaborators, 2022; WHO, 2022b). Medical and allied professionals have issued declarations of a mental health crisis that has been exacerbated by COVID-19, particularly among children and adolescents living in low-income communities and nation-states. Specific risk factors include higher frequencies of the death of parents, parental job loss, social environments marked by systemic racism, and highly limited mental health services (American Academy of Pediatrics, American Academy of Child and Adolescent Psychiatry, and Children’s Hospital Association, 2021; Huang & Ougrin, 2021; Mansfield et al., 2022; Organization for Economic Development and Cooperation, 2021; United States Department of Health and Human Services, 2021). Taken together, these three sets of interlocking features point to the need to investigate adolescent mental health with attention to younger age, gender, and socio-environmental disadvantage.
Methods
Overview of study design and procedures
This study was designed to investigate lived experience and mental health during adolescence through a mixed method and ethnographic approach. The setting for this non-clinical study was a low-income multi-ethnic school and community in Southern California, USA. The research plan focused on investigation of the everyday routines, mental health status, and educational engagement of middle school students recruited at the sixth-grade level (ages 10–11). Selection from this younger age range is intended as a contribution toward the identification of developmental vulnerabilities that may occur during early adolescence. It should be noted that demarcation of what constitutes the age range of ‘adolescence’ has varied historically and cross-culturally (Ariès, 1996). Data collection procedures included sociodemographic background, a series of semi-structured ethnographic interviews, ethnographic observations, the adolescent modified versions of the Patient Health Questionnaire (PHQ-9A) depression screening scale (Johnson et al., 2002), and the child (age 11-17) version of the Generalized Anxiety Disorder scale (GAD-10) (Craske et al., 2013). Sociodemographic data included age, gender identity, ethnic identity, family composition, and religious affiliation. Our ethnographic interview guide was designed to inquire in an open-ended manner with flexibility for probing questions. Interview themes included family life, experiences at school and with peers, mental health and well-being, perspectives on neighborhood and broader national and global events, as well as future goals. All interviews were conducted in English and were audio-recorded for subsequent transcription and qualitative coding and analysis utilizing NVivo software.
Our mixed method approach to utilize depression and anxiety screening scales, combined with ethnographic tools, was formulated in light of previous studies that demonstrate complementarity of various types of research evidence that shed reciprocal light on domains of inquiry (Csordas et al., 2010; Jenkins, 2015; Jenkins & Csordas, 2020). For example, while students may deny the presence of symptoms when assessed in scalar form, they may narrate their experience of these in an open-ended interview format. Conversely, some research participants may endorse items in a scalar assessment that they may not wish to speak about in a narrative interview format. We focused specifically on depression and anxiety as these are among the most common mental health conditions among youth, including sizeable Mexican-descent populations that reside within the study locale (Flores, 2013; Garber & Weersing, 2010). Our review of the literature shows that the PHQ-9 and GAD-7 adult scales are often used inaptly with child and adolescent populations (Anand et al., 2021; Mossman et al., 2017; Richardson et al., 2010; Tiirikainen et al., 2019; Tsai et al., 2014; Walter et al., 2020). Furthermore, studies which administer the PHQ-9A often rely upon adolescent age cohorts beginning at age 12, possibly on the basis of recommendations to commence clinical depression screenings at age 12 by the American Academy of Pediatrics, the U.S. Preventative Task Force, and the National Committee for Quality Assurance. This guideline also appears to folow the United States Preventative Task Force’s (2022) determination that there is insufficient evidence to warrant depression screenings at a younger age. In terms of assessments, one study utilizing the PHQ-9A documented no significant differences in completion, mean total scores, or rates of positive screenings that would affect or preclude its use among 11-year-olds (Cortez et al. 2021). That study opted to use the adolescent modified versions of the scales (for use among 11–17-year-olds) in light of their established reliability in cross-cultural settings (Aggarwal et al., 2017; Burdzovic Andreas & Brunborg, 2017; Naveed et al., 2019; Yalın Sapmaz et al., 2018). In the present study, we utilized adolescent versions of the PHQ and GAD scales to gain a basic overview of endorsed depression and anxiety symptoms among middle school students.
Participant recruitment and procedures before and during COVID-19 outbreak
Recruitment for this study was conducted between 2018 and 2021 utilizing a purposive sample of middle school-aged adolescents and their families at a school orientation event. The first wave of recruitment yielded 53 student participants primarily comprising 11-year-old participants (sixth grade level). Two bilingual (English-Spanish) research team members recruited participants, explained research aims, procedures, and addressed questions with interested parents and students. Recruitment also occurred via snowball sampling and through the distribution of flyers at the school. Parents who completed flyers or who were recommended for the study were contacted by a research team member to explain the research aims and procedures. After attaining written informed parent consent and child assent, we began research procedures with participants at the school. We conducted between 1 and 8 semi-structured interviews over the course of 1 year with student participants, lasting between 35 and 45 minutes during school elective periods. Interviews were conducted in offices provided by school administrators to ensure student privacy. The total number of interviews per student was contingent upon the time needed to complete all research procedures. Research protocols were conducted by five research team members who each met with the same students to build rapport and trust. While subject recruitment yielded an N of 83, we could only include 75 for whom procedures were fully completed since eight students had family relocations, class schedule conflicts, or disinterest in continuing with research procedures.
In the wake of the COVID-19 outbreak and school closure, we conducted follow-up questions by telephone or zoom and incorporated additional questions in the ethnographic interviews once in-person school instruction resumed, along with a second wave of participants recruitment. The content of these interviews included open-ended questions on student experiences of general health and wellbeing, experiences with relatives and friends during lockdown, and their experience of distance-learning during COVID-19. Given notably heightened political tensions in the research setting, particularly due to its proximity to the U.S./Mexico border zone, we inquired about student perspectives on contemporary local and global events such as immigration policies, the Black Lives Matter protests, the January 6th Washington D.C. insurrection, and COVID-19 safety practices.
Human subjects protection
Research procedures were carried out in compliance with UCSD Institutional Review Board for Human Subjects project approval #171596, and with permission from school district administrators. Participants received a copy of their signed consent form detailing any potential risks for participation in this study. Researchers moved to different questions if they sensed discomfort from adolescent participants and reminded them that all responses were voluntary. To reduce a potential breach in confidentiality, all identifying information was removed from transcriptions, utilizing only pseudonyms and numbers. All physical data is kept in a locked cabinet accessible only to the research team and digital data is stored in a password protected university server. Per IRB protocol, we connected students with a school counselor if they wished to speak with a mental health professional.
Results
Table 1 lists sociodemographic characteristics of the sample, including gender, age, grade level, ethnic background, and household type. Mean years of age was 11.2 with a limited age range among student participants. Within this sample, the majority of students identified as male or female; however, it is salient to note that during the interviews, some students were questioning their gender and sexual identities, revealing the limitations of coding gender or sexuality in a binary fashion. The most frequent ethnic identification was Mexican-descent, followed by combinations of Euro-American background. Additional identifications included African American and Black, Central American, Pacific Islander, South and East Asian, and Native American. Regarding ethnic background, we note that for some students this is a straightforward matter (e.g. ‘I am Mexican’) while others identify with more than one ethnic origin or geographic region. Table 1 thus oversimplifies the complexity of possible combinations. The increasingly common complexity of ethnic diversity has been identified by Hannah (2011) as ‘hyper-diversity’ that exists within the U.S. Overall, there is considerable cultural diversity among students in the sample and within the school setting generally. For household composition, all but one student lived with parents.
Sociodemographic characteristics of student participants. (N = 75).
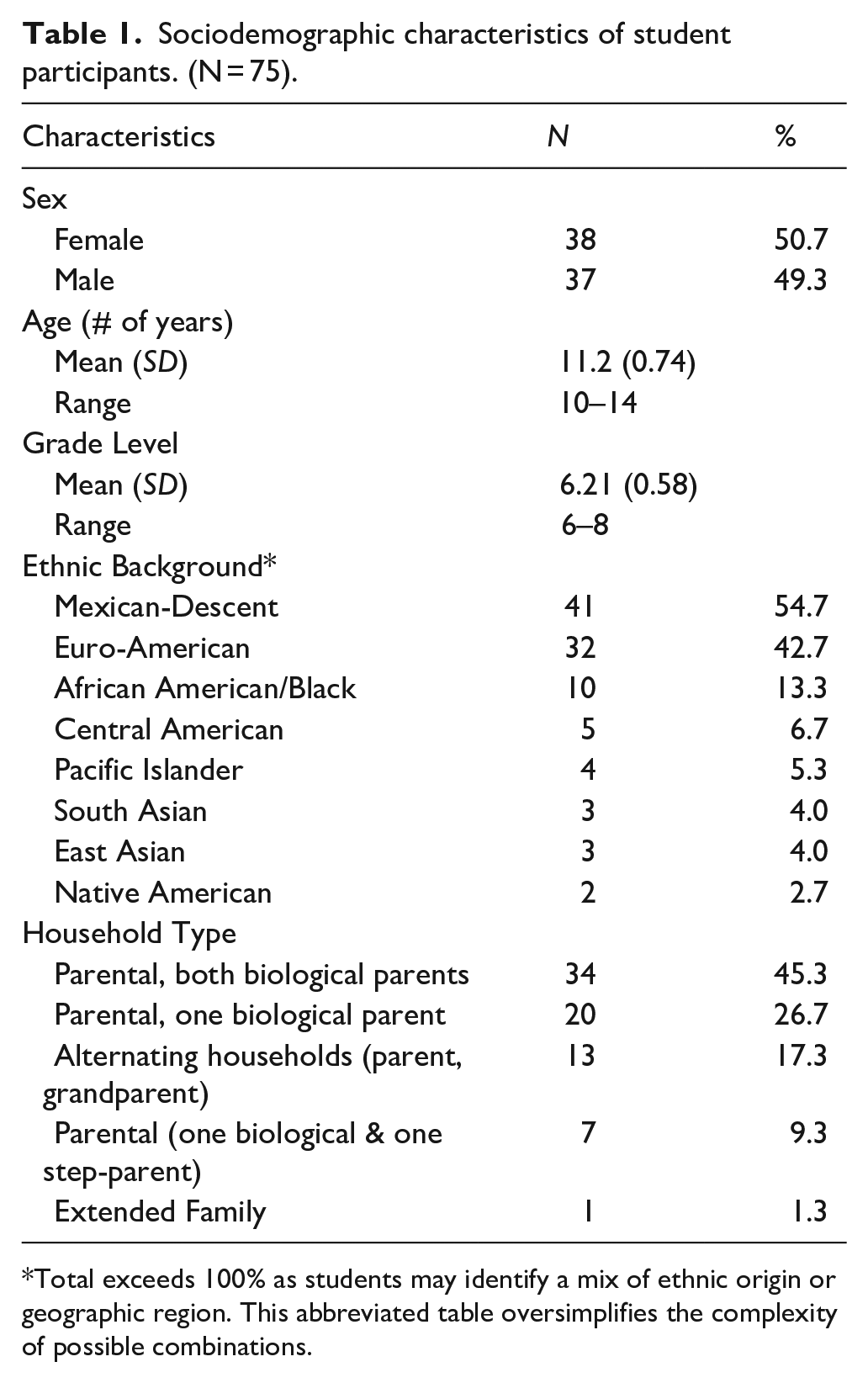
Total exceeds 100% as students may identify a mix of ethnic origin or geographic region. This abbreviated table oversimplifies the complexity of possible combinations.
Analysis of PHQ-9A depression and GAD-10 anxiety scores
Table 2 lists out the full range of the student scores for the PHQ-9A and GAD-10. As seen therein, 56% of the students fell into the lowest range of ‘none’ for depressive symptoms as did 49.3% for anxiety symptoms.
Student PHQ-9A and GAD-10 responses (N = 75).
Student PHQ 9-A responses
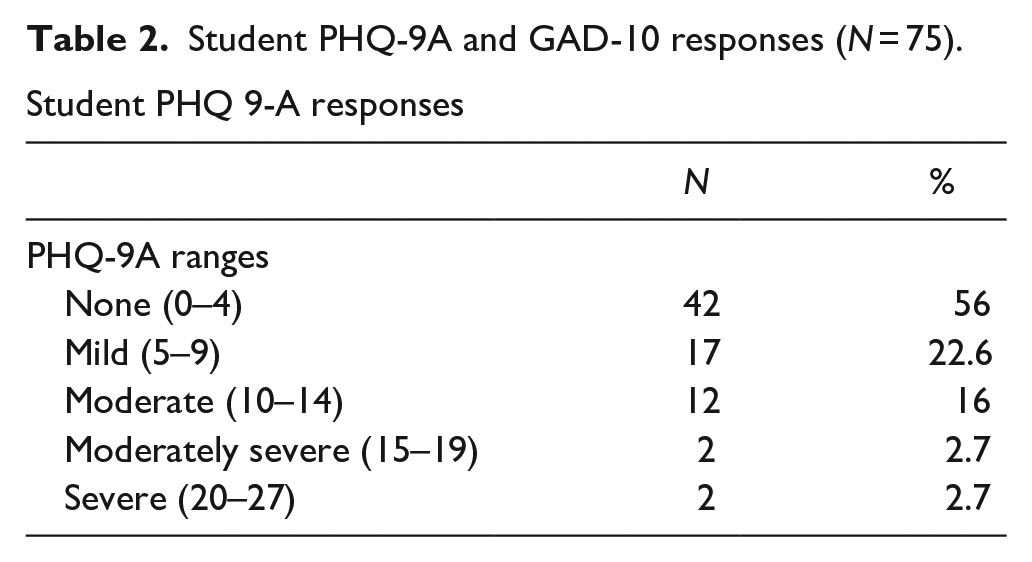
Student GAD-10 responses
Due to rounding, percentage does not equal 100%.
In terms of frequency, what is classified as ‘mild’ is next most common, 22.6% and 32%, respectively. Moderate to extreme levels were less commonly observed. When taken together for any degree of symptoms reported, 44% of adolescents in our study fall in the mild to severe range of the PHQ-9A depression screening scale, while the GAD-10 responses suggest that approximately half (50.6%) of adolescents fall in the mild to extreme anxiety screening range.
The PHQ-9A total scores reflect the frequency of symptoms listed in the nine items for depressive symptomatology. In this study, item 10 of the GAD-10 was modified by omitting the language of ‘superstitious object’ as a matter of cultural validity (further description of this issue is beyond the scope of this article but the subject of a forthcoming publication) and its aggregation of multiple help-seeking behaviors was broken up into seven separate boxes for enhanced identification of specific coping activities. Thus, GAD-10 total scores comprise the sum of items 1 through 9, plus the highest endorsed frequency of the seven expanded items. This calculation was done so as not to overly weigh coping symptoms in the sum scores.
Variance in PHQ-9A and GAD-10
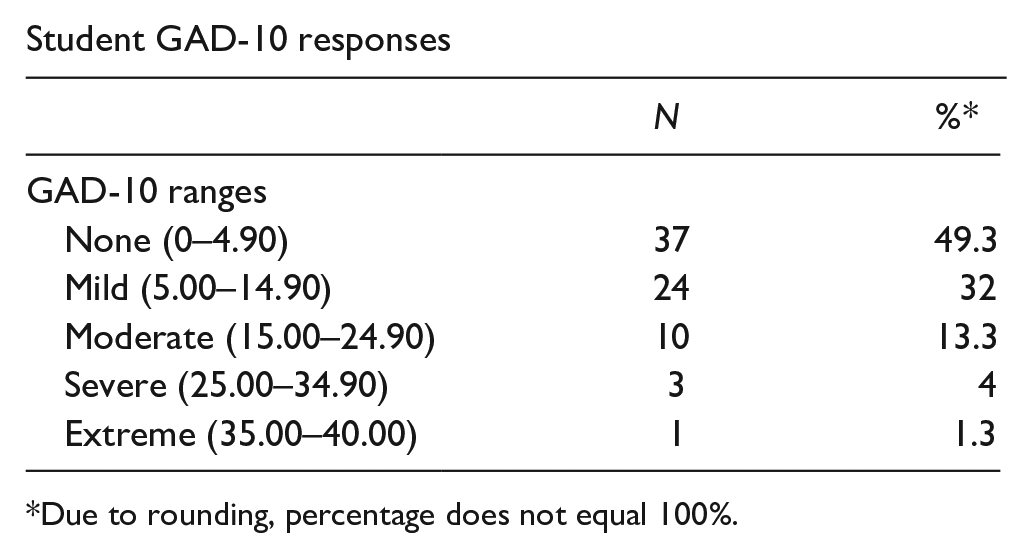
Previous studies have found that PHQ-9 scores are not normally distributed among adults and older adolescents (Burdzovic Andreas & Brunborg, 2017; Tomitaka et al., 2018), and that GAD-7 item responses are similarly skewed (Tomitaka & Furukawa, 2021). We confirmed these findings among our cohort of early adolescents. Neither the PHQ-9 (p < 10−5, Shapiro-Wilk test) nor the GAD (p < 10−6, Shapiro-Wilk test) sum scores were consistent with a Gaussian distribution (Figure 1a). PHQ-9A sum scores ranged from 0 to 23, with median 3.4 (IQR 6.5); GAD-10 sum scores ranged from 0 to 36, with median 5.0 (IQR 9.5) Prior studies have also shown strong correlations between the PHQ-9 and GAD-7 among adults (Kroenke et al., 2016) and adolescents (Leung et al., 2020). We confirmed that PHQ-9A and GAD-10 scores were highly correlated among our cohort (Figure 1b, Pearson’s r2 = .76). This indicates that over three quarters of the variation in PHQ-9A scores can be explained by variation in GAD-10 scores. The correlations remained strong for male and female participants analyzed separately (Figure 1b, r2 = .76 for females, r2 = .74 for males).
PHQ-9A and GAD-10 response distributions: (a) histograms of sum scores for the PHQ-9A and GAD-10 across all participants and (b) scatter plot of PHQ-9A versus GAD-10 sum scores for all male (purple) and female (green) participants.
Gender differences in PHQ-9 and GAD scores
Females consistently report higher levels of depression than males (Salk et al., 2017). In fact, gender disparities in depression have widened among adolescents in the United States in the past decade (Daly, 2022). We confirmed in this cohort of early adolescents that PHQ-9A scores were higher for females than males (p = .002, Mann Whitney test), with a difference in medians of 4 points (Figure 2). Similarly, GAD-10 scores were higher for females than males (p = .016, Mann Whitney test), with a difference in medians of 3 points (Figure 2).
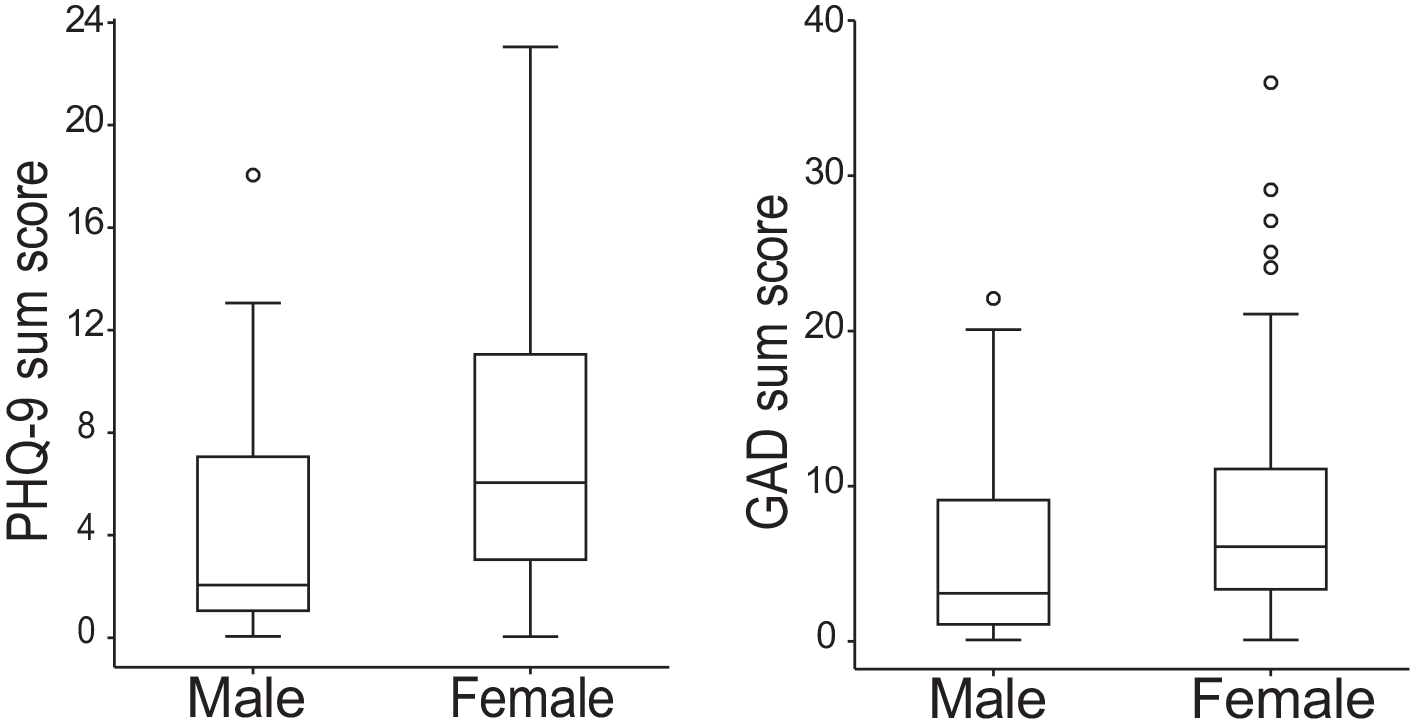
Female adolescents have higher PHQ-9A and GAD-10 sum scores than males: (a) box plots of PHQ-9A sum scores for male and female participants and (b) box plots of the GAD-10 sum scores for male and female participants. For a & b, boxes show median and interquartile range (IQR); whiskers extend to extend to the last datum within 1.5 IQR outside the first and third quartiles; points outside of this range are represented as outliers.
Gender differences in specific PHQ-9 and GAD items
Items were sorted in decreasing order of normalized mean difference (Figure 3), and two-sided t-tests were computed to evaluate group difference. To control for multiple comparisons, Bonferroni correction was applied with an alpha of 0.05, which sets the significance level to 0.05 divided by the number of comparisons. Of note, the total number of comparisons was 10 for the GAD-10, as we only compared the maximum response to the seven coping questions in accordance with existing GAD-10 research studies that utilize a composite item #10. Thus, significance was defined as p < .006 for PHQ-9A items and p < .005 for GAD-10 items. Females had higher mean responses on three items of the PHQ-9A after controlling for multiple comparisons (p < .006, two-sided t-test). This included the item concerning depressed mood (DEPRSD), one of two core symptoms required for a diagnosis of depression according to the DSM and ICD criteria. The other two significant question items concern feeling tired or having low energy (TIRED), and feeling bad about yourself or like a failure (FAILUR). The normalized differences for the TIRED, FAILUR, and DEPRSD items were 5.18, 4.35, and 4.33, respectively. This indicates that the mean responses on these items were 4 to 5 standard errors higher for females than males. The item concerning poor sleep (SLEEP) showed strong trend level differences (p = .018, two-sided t-test) with normalized difference of 3.4, but this item failed to reach significance after Bonferroni correction.
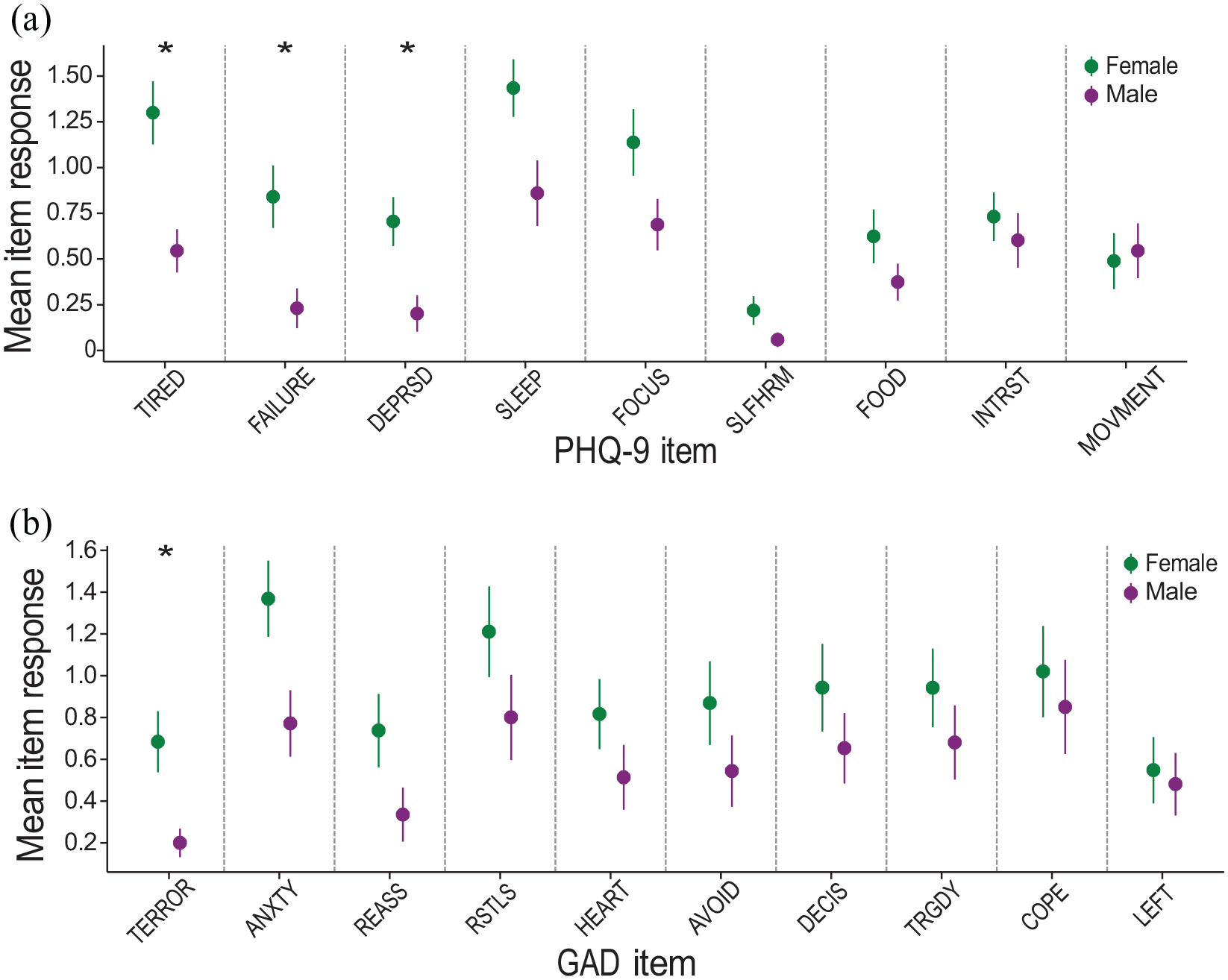
Gender difference in specific PHQ-9A and GAD-10 items: (a) mean item responses and standard errors for all nine items of the PHQ-9A for female (green) and male (purple) participants and (b) mean item responses and standard errors for all 10 items of the GAD for female (green) and male (purple) participants. For (a) and (b) items are sorted on x-axis in decreasing order of normalized mean difference between males and females, defined as the difference in means divided by the average standard error.
Females had higher mean responses on only one question item in the GAD-10 after controlling for multiple comparisons (p < .005, two-sided t-test). This question concerns feeling moments of sudden terror or fright (TERROR), which had a normalized mean difference of 4.5, indicating mean responses 4.5 standard errors higher for females than males. The core diagnostic item concerning feeling anxious, worried, or nervous (ANXTY) showed a strong trend level differences (p = .017, two-sided t-test) with a normalized mean difference of 3.5, though this item was not significant after Bonferroni correction. Trend level differences were higher for females on all 10 items of the GAD-10, and for 8 of 9 items of the PHQ-9A.
Discussion
Age-specific findings in depression and anxiety
We find that 44% of adolescents in our study fall in the mild to severe range of the PHQ-9A depression screening scale, while the GAD-10 responses suggest that approximately half (50.6%) of adolescents fall in the mild to extreme anxiety screening range. Given that this is a non-clinical, school-based study, our results indicate that screening for these common mental health-related items could be important for the early identification of distress that may continue or become exacerbated beyond age 11. Our study is one of the few we could identify that specifically target this earlier adolescence age group. In comparing our results with existing studies that utilize the PHQ-9A, and which report scores within lower and narrower age ranges, our findings are lower than those reported among school-based Pakistani children (at 66.8%) (Naveed et al., 2019), yet higher than the 13.2% depression scores among 10 to 12 years-old students in South West Nigeria (Oderinde et al., 2018). Although the GAD-7 is used in clinical and research settings for screening of anxiety symptoms, the GAD-10 modified for use with adolescents to date has not been widely applied in screenings for research on adolescent prevalence of anxiety symptoms.
Gender, depression/anxiety, and mental health care
In light of studies of adult and older adolescent populations that find higher levels of depression and anxiety among women and girls (Beesdo-Baum & Knappe, 2012; Jenkins & Csordas, 2020; Nolen-Hoeksema, 1990; Seedat et al., 2009), we hypothesized that girls in this study would score higher on these assessments even at the lower range (mean age 11 years) of what is typically classified as ‘adolescence’. Thus far, empirical study of age-specific rather than a broad age-range for adolescence has yet to be undertaken. While screening instruments such as those used here for depression and anxiety in no way constitute a clinical diagnosis of a syndrome, the presence of symptoms even at subsyndromal levels suggests that the observable onset of depression and anxiety may occur earlier than previously thought. Risk of major depressive disorder is considered low in childhood, and when it does occur, this has been in the absence of gender differences (Kazdin, 1993; Lewinsohn et al., 1994). Longitudinal studies show that subsyndromal symptoms of depression in early life may predict the future development of major depressive disorders (Uchida et al., 2021).
Psychiatric, epidemiologic, and anthropological studies suggest multiple factors as possible explanations for higher rates of depression, including developmental, psychological, biological, and sociocultural processes (Jenkins & Csordas, 2020; Kuehner, 2017; Riecher-Rössler, 2017). Sex variation in depression may commence with morphological and endocrinological changes in early adolescence (Cyranowski et al., 2000; Nolen-Hoeksema, 1990; Petersen et al., 1991; Piccinelli & Wilkinson, 2000). The onset of symptoms of anxiety may begin earlier in the life course, frequently preceding or co-occurring with depressive symptoms (Beesdo et al., 2010; Strawn et al., 2021). A frequently cited factor utilized to explain the emergence of depressive and anxiety-related symptoms entails bodily development that may be perceived negatively in comparison to peers, particularly among adolescent girls (Blakemore, 2019). Genetics have also been explored, though specific markers for depression and anxiety risk have yet to be identified (Li & Graham, 2017).
Another critical concern is the impact of widespread sociocultural gender inequity and gender-based violence since girls and women are more frequently exposed to childhood sexual abuse and assault (Oram et al., 2017; Stoltenborgh et al., 2015). Based upon our ethnographic interviews and observations, we consider several factors as of likely relevance for adolescent girls’ experiences of depression and anxiety. Gender-based violence, particularly in a school and community setting, involving extant insecurity is a prominent feature of the socio-structural environment of the research participants. Girls in our study report having experienced or witnessed sexual assault at home, and/or school settings, hearing or receiving sexually based or derogatory remarks on girls’ bodies online via social media and at school, and/or recount instances of being attacked by peers resulting in school fights. The heighted risk of gender-based violence in both school and home environments extends also to adolescents who may be questioning their sexual and gender identities. Within familial settings, psychosocial features of the home atmosphere are also of key relevance. Within our study, we observed that a notable feature within home environments for girls who endorsed depression and anxiety (to any degree, mild to severe), was criticism by family members (parents, siblings, grandparents) directed toward girls’ bodily appearance (e.g. weight), academic performance, along with cultural attributions of laziness or lack of motivation in accomplishing tasks. Additionally, girls often worry about the possibility of being abandoned by friends, loved ones, or significant others based upon their experiences of loss and grief in the context of the COVID-19 pandemic. Among the large proportion of our sample who maintain cross-border ties with Mexico, the dread of deportation of relatives, border closures, and heightened discrimination and racism in their school and community settings creates additional sources of fear and uncertainty in their everyday milieu.
With respect to seeking mental healthcare, some students in the study had sought services with or without a referral from a school counselor. Generally, there was limited available care and significant social stigma attached to the use of mental healthcare services by students and parents alike. Also important to note for the United States, often imagined as a wealthy country with multiple resources, is the reality of severely limited or unavailable mental healthcare services for many. Ever-increasing social inequity within the country most affects low-income communities, such as described in this study. This structural problem points to the recent observation (WHO, 2022b) that: ‘Even before the COVID-19 pandemic, just a small fraction of people in need had access to effective, affordable, and quality mental health care. . . For depression, the gaps in service coverage are wide across all countries: even in high-income countries, only one third of people with depression receive formal mental health care and minimally-adequate treatment for depression is estimated to range from 23% in high-income countries to 3% in low- and lower-middle-income countries’.
Indeed, recent rankings by the Global Burden of Disease group (GBD 2019 Mental Disorders Collaborators, 2022) for ‘disability-adjusted life years’ show the highest health impacts across three geographic regions: Australasia, Tropical Latin America, and North America. Some of the impacts of structural features affecting these students was mediated by supportive relationships with family and friends, thereby offering a buffer zone from which to fend off or struggle with depressive or anxiety-related feelings, thoughts, and behaviors. Having such support has been associated with academic success or engagement (Benner, 2011; Gonzales et al., 2013; Stanton-Salazar, 2001). Moreover, anthropological research documents how unstable social environments throughout adolescence can exacerbate the ways that individuals develop self-protective strategies associated with preoccupation or dissociation from multiple forms of familial abuse (Jenkins, 2015).
Conclusion
Our data, showing the presence of mild to severe levels of symptoms of depression and anxiety within a non-clinical sample of young middle school students, suggests that research attention is warranted at an earlier age for basic screening procedures. These findings for 11-year-old students are of potential clinical relevance for identification of subsyndromal conditions during early adolescence. Significant gender differences, previously found for older adolescents and adults, were observable in this study. In a middle school setting such as that of the present study, the need to address mental health difficulties, whether mild or severe, is vital to facilitate educational engagement.
Footnotes
Author contributions
JHJ is Principal Investigator for the study, responsible for study design and supervision of all aspects of the research. She is the primary author of the article. GS is Research Coordinator and lead researcher for data collection and management; she is also a primary author for this article. EAM completed all computational analyses for this study and is a primary author for write-up of statistical results. NS is a senior ethnographic researcher and assisted with data collection. GU assisted with data collection and management. AJP assisted with data collection and management. All authors have reviewed the manuscript and provided their consent for the publication.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received support through grants awarded as PI through the UCSD Frontiers of Innovation Scholar Award # C6009, UCSD Faculty Senate grants 2020-2022.