
Abstract
Objective:
There has been increasing interest in the physical health, mental wellbeing and burnout afflicting medical students over recent years. This paper describes the overall results from phase two of an international study including a further nine countries across the world.
Methods:
We sampled large groups of medical students in nine countries at the same time and with exactly the same method in order to aid direct comparison of demographics, burnout and mental wellbeing through validated instruments.
Results:
A total of 4,942 medical students from these countries participated in this study. Around 68% of respondents screened positive for mild psychiatric illness using the General Health Questionnaire-12. Around 81% and 78% of respondents were found to be disengaged or exhausted respectively using the Oldenburg Burnout Inventory. Around 10% were found to be CAGE positive and 14% reported cannabis use. The main source of stress reported by medical students was their academic studies, followed by relationships, financial difficulties and housing issues.
Conclusion:
Cultural, religious and socioeconomic factors within each country are important and understanding their effects is fundamental in developing successful local, regional and national initiatives. Further quantitative and qualitative research is required to confirm our results, clarify their causes and to develop appropriate preventative strategies.
Introduction
In recent few years there has been a welcome increase in interest in levels of burnout and mental wellbeing of medical students. This is important as not only are they the workforce of the future and essential for the prospective health of our communities, but also are at a vulnerable stage of their lives in terms of developing mental health problems. Hence it is vital that their mental health needs are thoroughly explored and studied.
International comparisons are helpful because they highlight similarities, differences and examples of good practice that can be shared. Throughout the world, medical students face an extremely competitive and stressful admissions process before undertaking a demanding 5- or 6-year academic programme. The medical curriculum applies high levels of pressure to students through frequent and rigorous examinations and assessments. Students also face additional pressures because of the need to conduct research, publish in medical journals, teach, build management and leadership skills and win competitive prizes in order to choose the speciality of their choice. Studies have repeatedly shown that medical students display high levels of stress, ‘mild’ psychiatric illnesses (including anxiety and depressive disorders) and burnout compared to the general population (Dyrbye et al., 2006; Schwenk et al., 2010; Stecker, 2004). Help-seeking is often delayed due to self-stigma and lack of awareness. Limited resources to help may then compound matters further, as can high rates of substance misuse in this age group. It is well-recognised that such difficulties can lead to reduced empathy, reduced academic achievement, increased dropout and potential long-term consequences for patient safety (Ashton & Kamali, 1995; Schwenk et al., 2010; Stewart et al., 1999; Wartolowska et al., 2014; Woloschuk et al., 2004). Inevitably, there are implications for poor patient care and poor patient satisfaction.
Basic medical school teaching programmes and curricula are broadly similar across the world, but substantial cultural, societal and economic differences exist across countries. These wider factors help to determine both the causes of stress and the individual’s response to them.
This study describes these differences and variations in rates of mental wellbeing, stress and burnout and reports on possible causative factors across nine countries. Our previous study using exactly the same methodology involved a sample of over 3,500 medical students participating from across 12 countries (Molodynski et al., 2021). Students in all countries reported very high levels of ‘caseness’ on validated measures of psychiatric illness and burnout (Molodynski et al., 2021). Rates of substance misuse and stressors varied however. These variations were strongly influenced by prevailing cultural, societal and economic factors (Molodynski et al., 2021).
In this paper we report the results from phase two of our global initiative, highlighting the cross-cultural results from a further nine countries.
Methods
Phase one of the study covering 12 countries was completed in late 2020 and published in early 2021 (Molodynski et al., 2021). In view of the gravity of our findings we extended the study to other centres.
The core study team based in the United Kingdom (AM, SF, MK, TL and DB), approached health leaders in nine countries: Canada, Denmark, India, Indonesia, Iran, Nepal, Nigeria, Russia and Sri Lanka. Canada and India had already participated in the previous data collection although different medical schools had participated in the two surveys. Each country set up a local steering group and then approached medical students in one or more medical schools through an email invitation. This invitation was similar across all countries and emphasised the confidential nature of the survey and included links for available student support in case of distress. A confidential and secure platform (‘Typeform’) was utilised to collect student responses. No identifying personal information was collected. All responses were anonymous. Multiple responses from the same individual were prevented due to Typeform’s encrypted IP software. Ethical approvals were sought and granted as needed, as outlined in each individual paper. Data was collected between February 2020 and 2021, with some delays occurring due to the COVID-19 pandemic.
The survey consisted of a covering letter, basic demographic information and several valid and reliable assessment tools. The covering letter highlighted the importance of the survey and its secure, anonymous and voluntary nature. Details of support services were provided to students. Demographic information included the country of the respondent, medical school, year of study, gender, educational level of parents and previously diagnosed mental ill health. Assessment tools included the General Health Questionnaire-12 (GHQ-12) (Goldberg & Blackwell, 1970) to identify mild psychiatric illness, the Oldenburg Burnout Inventory (OLBI) (Reis et al., 2015) to assess burnout and the CAGE questionnaire to identify problematic alcohol abuse. These instruments have previously been shown to be reliable, valid and accurate (Masur & Monteiro, 1983; Peterson et al., 2008). It must be emphasised that these instruments were used for screening only and not for making formal diagnoses.
Data from each included country was extracted from the Typeform database into an Excel spreadsheet. Incomplete responses were excluded. Demographics and assessment tool data were analysed individually before performing pooled analyses. All analysis was performed using SPSS version 25 (IBM, Armonk, NY, USA). Continuous data were compared with one-way ANOVA while categorical data were compared with chi-square test or Fisher’s exact test depending on the number of events. A p-value of less than .05 was considered significant and all tests were two-sided.
Results
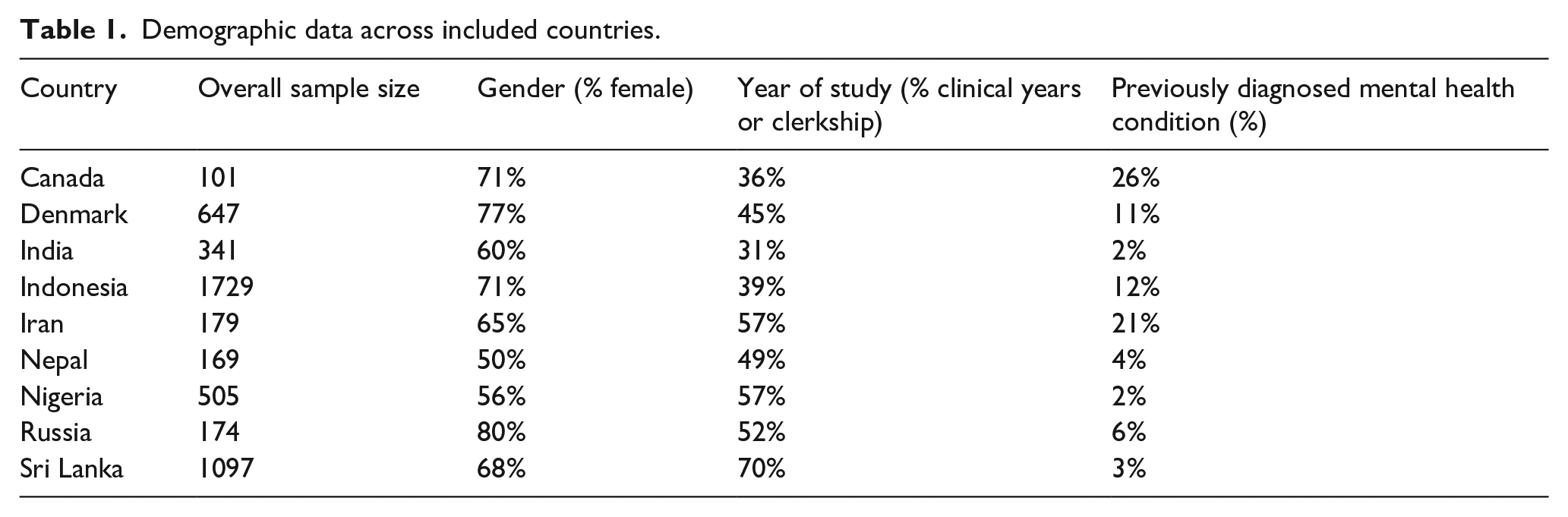
Around 4,942 medical students from nine countries participated in this study. The number of participants varied from 101 (Canada) to 1,729 (Indonesia). On average, females represented 66% of the medical student respondents (ranging from 50% to 80%). Around 45% were in their clinical or clerkship years of study. One in seven (13% with a range of 2%–37%) students had been formally diagnosed with a psychiatric illness prior to starting medical school. Table 1 summarises these results. No statistically significant differences were noted between countries.
Demographic data across included countries.
The GHQ-12 is a well validated and commonly used screening instrument that we used to assess so- called ‘minor psychiatric illness’. ‘Caseness’, indicated by a score of two or greater, was noted to range between 50% in Nepal and 85% in Russia, with an average of 68% across all nine included countries (Table 2). The OLBI questionnaire was used to measure burnout and rated two key parameters – disengagement and exhaustion. Disengagement ranged from 61% in Canada to 93% in Indonesia, with an average of 81% across these countries (Table 2). Reported Exhaustion ranged from 65% in Nepal to 95% in Indonesia, with an average of 78% across all nine countries (Table 2).
Results for the GHQ-12, OLBI and CAGE questionnaires.
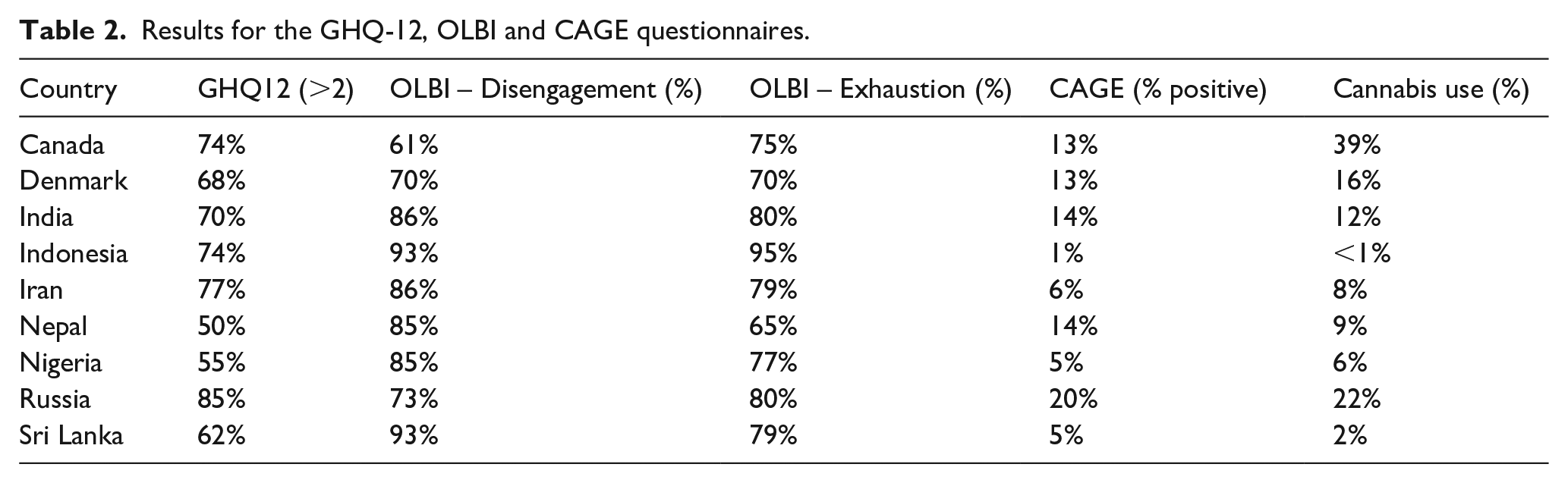
The CAGE questionnaire was used to identify and quantify problematic alcohol consumption. Around 10% of students overall screened positive, but this disguised substantial variability from 1% in Indonesia to 20% in Russia (Table 2). Students were also surveyed about any potential drug use. Cannabis was found to be the most used recreational drug amongst medical students, with reported rates of up to 39% in Canadian students (Table 2).
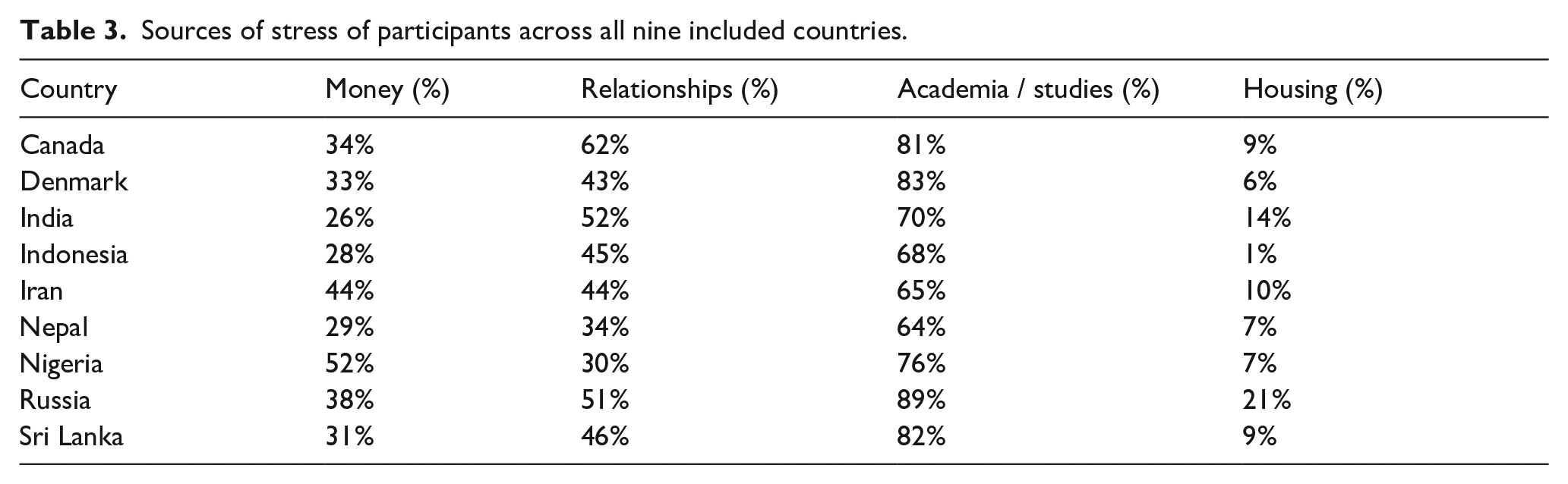
Psychiatric illnesses, burnout and substance abuse are often linked to stressors. This study identified sources of stress in four broad categories: financial, relationships, studies and/ or housing. Academic studies were highlighted as the key source of stress in 75% of students, ranging from 64% in Nepal to 89% in Russia. Around 45% of students highlighted that relationships were also a major stressor. These included parental as well as relationship difficulties. Just over one third of students (35%) reported financial difficulties and only 9% noted housing or accommodation factors (Table 3).
Sources of stress of participants across all nine included countries.
Discussion
Our results indicate a pervasive pattern of high levels of psychiatric symptoms, disengagement and exhaustion in medical students across these nine countries as with our previous sample. This is concerning for a number of reasons, particularly given the current global difficulties due to the COVID-19 pandemic. With these effects continuing and many predicting further economic, environmental, geopolitical and societal turmoil, it is more important than ever that we identify and safeguard society’s future doctors.
This study formed phase two of a global study. Phase one was conducted in 2019 to 2020 and investigated 12 countries spanning five continents (Molodynski et al., 2021). Phase one succeeded in recruiting 3,766 students, and highlighted variable but high levels of psychiatric illness, burnout and substance use. The sources of distress reported by medical students varied across the different cultural, societal and economic country profiles. This study (phase 2) has successfully recruited a further 4,942 medical students across nine other countries, making a total of 8,708 across two studies. The number of respondents and relatively similar results across a total of 19 countries lends support to the growing concern of many healthcare professionals and health care leaders regarding the welfare of medical students.
This study has limitations. Although a high number of respondents was achieved, the overall response rate could not be calculated due to the study’s convenience sampling approach. This could lead to selection bias, with those suffering most being more inclined to respond. Secondly, the study was based on a cross-sectional observational methodology, and therefore cannot infer causality.
In this study, GHQ-12 positivity was seen in 68% of medical students. This screening tool is helpful in identifying mild psychiatric disorders. The OLBI questionnaire revealed average disengagement of 81% and exhaustion of 78% amongst our respondents. This index has been validated as a reliable tool to assess burnout. CAGE positivity was observed in 10% of students and cannabis use in 14%. Variability likely reflects national cultural factors. For example, Indonesia has only 1% positivity on CAGE and that may reflect the fact that it is an overwhelmingly Muslim country. Our results demonstrate a clear need for more rigorous local, national and global initiatives. Although the COVID-19 pandemic has caused much suffering globally, it has also triggered significant support mechanisms and initiatives such as national mindfulness programmes, confidential support schemes and advice services (Kadhum et al., 2020). It has created a window of opportunity for change.
Our results have identified key stressors, with many students indicating that academic studies were their biggest worry, followed by relationships, financial difficulties and then housing issues. These stressors are to be expected considering rapidly changing developments in medicine and technical challenges but should be of interest to teachers, policymakers, health leaders and healthcare professionals and encourage us to tailor our current and prospective support mechanisms for medical students in a similar way that we aim for patient-centred care (Kramer et al., 2014). This necessarily involves an understanding of the cultural, religious and socio-economic circumstances that surround medical students within specific regions. For example, in Indonesia, our results reveal extremely high levels of burnout (>90%) and psychiatric illness (>70%), but extremely low alcohol and drug abuse (<1%) reflecting cultural factors and relative difficulty and risk in obtaining alcohol and drugs. In particular, alcohol and drugs are not part of the common consumption for the general public in Indonesia, with further research required to identify whether Indonesian medical students resort to other more readily available ‘compensations’, such as tobacco or pornography. In contrast, 40% of Canadian medical students use cannabis, likely reflecting the decriminalisation of cannabis in Canada (Government of Canada, n.d.).
There are major challenges for medical schools, policymakers and individuals. Medical students must be trained to look after their own mental health and wellbeing. In the same vein, medical schools must offer services which are non-stigmatising, available and easily accessible. These need to be funded properly for which policymakers must be held responsible. Crucially the over emphasis on individual factors needs to be challenged and replaced by systemic and preventative approaches.
Conclusion
Our results highlight relatively uniform high rates of poor mental wellbeing, burnout and substance misuse in many countries. The main sources of stress for medical students included academic studies, followed by relationships, financial and accommodation difficulties. Cultural, religious and socioeconomic factors within each country are important and their understanding is fundamental in developing successful local, regional and national initiatives. With the disastrous effects of the COVID19 pandemic and associated healthcare burden, it is imperative that we identify the needs of our medical students and prevent psychiatric illness. One of our most important findings is that students in wealthy countries were no better off than their colleagues elsewhere. In fact in many cases levels of distress and problematic substance use were greater. Thus, nowhere can say they do not have a problem or that they do not urgently need to address it by sharing examples of good practice and learning from each other.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval declaration
Individual countries did seek out ethical approval as required, and this is outlined in the individual country-specific publications.