
Abstract
Aim:
The current research was conducted in the context of an ongoing reform of mental health services in the Republic of Moldova since 2014, where efforts have been devoted to creating community-based mental health services. This article presents a snapshot of the needs of mental health service users in the Republic of Moldova and helps to understand how and with which services their needs can be addressed.
Methods:
This cross-sectional study compared the levels of needs (CANSAS scale), quality of life (EQ-5D 3L), mental health status (MINI for psychotic disorders) and functioning (WHO-DAS) among mental health service users in the psychiatric hospital in Chisinau, Moldova. All service users resided in districts where community mental health services were being developed. Correlations between quality of life, functioning and unmet need were explored.
Results:
Of 83 participants, one third had a psychotic or a mood disorder. On average, participants reported needs in 9.41 domains (SD = 4.41), of which 4.29 were unmet (SD = 3.63). Most unmet needs related to intimacy and relation to others. The level of functioning and quality of life were reported. We found strong, negative associations between the number of unmet needs and level of functioning, as well as the quality of life. We also found that higher functioning levels were positively associated with higher quality of life.
Conclusion:
There were a high number of unmet needs among this inpatient population, particularly social needs and service-related needs. A continuum of inpatient and outpatient care and individual treatment plans can help address the different needs of different patients. Individual treatment plans for patients and the choice of the appropriate treatment for patients could be guided by an assessment of service users’ (unmet) needs of care and level of functioning.
Keywords
In 2007, the first Lancet series on global mental health highlighted the importance of addressing mental health globally and demonstrated the sizable mental health treatment gap and its associated costs for both individuals and society at large (Jacob et al., 2007; Patel, Araya, Chatterjee, & Chisholm, 2007; Prince, Patel, Saxena, & Maj, 2007; Saraceno et al., 2007; Saxena, Thornicroft, Knapp, & Whiteford, 2007). More than a decade after the publication of this global call for action, more progress needs to be made to narrow the care gap (Alonso et al., 2018; Thornicroft et al., 2017). Key barriers in the progress of improving the access to effective care include, for example, the concentration of most mental health resources in urban areas within countries, stig-matization of people suffering from mental ill health and those receiving treatment, and limited provision of evidence-based, cost-effective care (Saraceno et al., 2007; Thornicroft, Deb, & Henderson, 2016). There is general consensus that community-based mental health services are essential in facilitating early detection, decreasing rates of hospital-based psychiatric care and providing evidence-based care in close proximity to the service users’ homes (Abdulmalik & Thornicroft, 2016). For severe mental illness, community-based care often involves multidisciplinary teams consisting of a diverse range of practitioners and disciplines for treatment, based on well-designed care pathways for more intensive care when necessary (e.g. during times of crisis). It aims to treat and enable people to live in a way that maintains their connection with their families, friends, work and community. It also fosters self-determination and a desire for greater involvement in decisions related to their treatment (Bond, Drake, Mueser, & Latimer, 2001; Thornicroft et al., 2010). Community mental health care has been shown to have a positive impact on treatment outcomes in both high as well as in low- and middle-income countries (Thornicroft & Tansella, 2013; Wiley-Exley, 2007), including on measures of community integration, autonomy and quality of life (Taylor et al., 2009). In Central and Eastern European (CEE) countries, recent research indicates that early detection and early intervention as well as community-based services for psychosis could help reduce the burden of disease and even lead to cost savings (Winkler, Broulíková, et al., 2018). Many efficient mental health systems therefore provide the majority of services within the community and reserve hospital-based, inpatient care for severe cases that cannot be resolved in community settings (Abdulmalik & Thornicroft, 2016; Patel et al., 2018; Thornicroft et al., 2010; Thornicroft et al., 2016; Thornicroft & Tansella, 2003; Thornicroft & Tansella, 2013).
The Republic of Moldova has been undergoing a comprehensive national reform of its mental health system since 2014 in an effort to deinstitutionalize mental health care. Up until the reform, mental health care relied heavily on hospital-based mental health care (Turcanu, Domente, Buga, & Richardson, 2012). However, the National Health Policy for 2007–2021 (Republic of Moldova, 2007) and the new National Programme for Mental Health (2017–2021) (Ministry of Health in the Republic of Moldova, 2017) together emphasized the need for community-based services in mental health, encouraged the deinstitutionalization of mental health services and pinpointed a roadmap for the development and implementation of mental health services at the community level. The central aim was to implement a continuum of mental health care provided through family doctors, community mental health care teams and mental health care specialists in acute psychiatric wards and general regional hospitals. In four pilot districts, this implementation is led by a national and international consortium through the SDC (Swiss Agency for Development and Cooperation)-funded project Support for the Reform of Mental Services in Moldova (hereafter Moldova reform project). To successfully deinstitutionalize care, continuous evaluation of progress and quality assurance through monitoring should accompany the implementation at every step (Thornicroft et al., 2010; Thornicroft, Tansella, & Law, 2008). Here, care pathways should be evaluated on the basis of symptom reduction, but also on the basis of recovery of psychosocial functioning and improvement of health-related quality of life (HR-QOL; Bengtsson-Tops & Hansson, 1999; Thornicroft et al., 2010; Thornicroft et al., 2008). To achieve a sustainable shift to community-based mental health care, service providers must first understand the current inpatient population and adapt to the needs of the population being transitioned to alternative forms of mental health care (Zitko et al., 2017).
In line with prior research and in the context of the Moldova reform project that seeks to enable access to community-based mental health care in the country, this article seeks to understand the current inpatient population of mental health service users in Moldova through a cross-sectional study assessing mental health status, (un)met needs, level of functioning and quality of life.
Methods
Participants and recruitment
For a service user to be eligible to partake in the study he or she (a) must have been living in one of the pilot districts (raions) of the Moldova reform project, namely Soroca, Orhei, Cimislia and Cahul and (b) must have been hospitalized as an inpatient in one of Moldova’s three psychiatric hospitals at the time of the study. All hospitalized service users who met these criteria during the time of data collection were invited to partake in the study. Service users suffering from addiction were excluded from this study.
Procedure
Ethical approval was obtained from independent institutional review board in Chisinau, Moldova (Comitetul de Etică a Cercetării al USMF ‘N.Testemiţanu’ Number 26.06.2017/98-104) based at the Medical University in Moldova. The assessments were paper based and administered by trained psychologists and psychiatrists who were external to the service over the course of 2 weeks (i.e. not practicing clinicians at any of the hospitals or services being evaluated within the Moldova reform project). Hospital staff were approached to provide a list of current service users admitted to one of the wards who resided in one of the four project districts mentioned above. Evaluators progressed through the list, explaining the purpose of the assessment. All participants were asked for their informed consent. Consenting patients sat in a separate room or hallway with the assessor to complete the assessment. The assessment took approximately 60 minutes to complete, and where assistance in completing the self-report items was needed, the assessor was available to answer any questions.
Tools
To develop a comprehensive assessment with the further purpose of building a service users profile, the survey was an assessment consisting of several validated tools and outcome measures that assessed the following dimensions:
Medical/psychiatric assessment (diagnosis and symptoms),
Functional assessment (psychosocial and cognitive functioning, HR-QOL),
Needs assessment for mental health care
The final tools used in the assessment were selected by the project team during three rounds of email-based reviews, taken from a comprehensive review of tools prepared by a PhD researcher on the project.
Quality of life
We measured HR-QOL using the EQ-5D 3L questionnaire, a validated and widely used tool in economic and clinical studies that is available in several languages (Greiner et al., 2003). This instrument assesses health on five dimensions, specifically mobility, self-care, usual activities, pain and discomfort, and anxiety and depression. Participants indicated on a 3-point Likert-type scale whether they had no problems, some problems or severe problems in a given domain. Based on a formula derived from western European countries, an overall index of the quality of life was calculated (Greiner et al., 2003). In addition, the EQ-5D 3L contained a visual analogue scale (VAS) on which participants could rate their overall quality of life, ranging from 0 (worst imaginable health) to 100 (best imaginable health).
Assessment of met and unmet needs
To assess needs for care, we used the Camberwell Assessment of Need Short Appraisal Schedule (CANSAS; Slade, Thornicroft, Loftus, Phenan, & Wykes, 1999), which covers 22 domains of an individuals’ life such as accommodation, food, self-care, daytime activities, psychotic symptoms, child care, money, distress, physical health and relationships. Participants indicated in each of the 22 domains whether they have no needs, met needs or unmet needs.
Psychiatric assessment
We used the Romanian paper-based version of the Mini International Neuropsychiatric Interview (MINI), version 7.0.2, for psychotic disorders (Sheehan et al., 1998), a staff-administered structured diagnostic interview that assesses the diagnosis of psychiatric patients according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) or International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10) criteria. It is an internationally recognized tool in clinical practice and has shown to have well-defined psychometric properties (Van Vliet & De Beurs, 2007). In Moldova, ICD-10 is used as the diagnostic coding study, and therefore we report in this article mental disorders falling between ICD-10 categories F00–F09 (organic disorders, for example, dementia or delirium), F10–F19 (disorders due to psychoactive substance use), F20–F29 (psychotic disorders), F30–F39 (mood (affective) disorders), F40–F48 (neurotic, stress-related and somatoform disorders), F50–F59 (behavioural syndromes), F60–F69 (disorders of adult personality and behaviour), or having comorbid disorders or another disorder. Participants fell into the category comorbid disorder if they had a diagnosis in more than one of the ICD-10 categories according to the MINI. If a service user’s diagnosis did not fall into a category that was included in the MINI, the participant was assigned to the group of other disorders. These other diagnoses included, for example, organic disorders such as dementia or mental retardation, as well as other non-psychotic disorders.
Level of functioning
The WHO Disability Assessment Schedule 2.0 (WHO-DAS) is a 36-item measure of (dis)ability designed to measure six domains of social-cognitive functioning, specifically understanding and communication, getting around, self-care, getting along with others, life activity and participating in society (World Health Organization, 2010), that allows for cross-cultural standardized measurement of the level of functioning. On each of the 36 items, participants rated statements on a 5-point Likert-type scale ranging from 0 ‘None’ to 4 ‘Extreme or cannot do’ such as ‘In the past 30 days, how much difficulty did you have in maintaining a friendship?’ (getting along with others). For ease of interpretation, we inverted the scores of the WHO DAS understanding in the current study, so that a higher score would indicate more ability rather than more disability.
Statistical analysis
Statistical analysis was performed using R Version 3.4.1 (R Core Team, 2016). Demographic information for some participants was missing. Approximately 30% of participants (n = 27) did not respond to half of items in the domain Life Activity of the WHO DAS. On all other dimensions of the WHO DAS, maximally two responses were missing. Two responses were missing for items of the EQ-5D. One response was missing for eight CANSAS items. For the CANSAS items benefits, intimate relationships, child care, and sexual expression, two, four, five and eleven responses were missing respectively. To avoid a loss in power and biased estimates, we imputed missing values with multiple imputation by chained equation using the MICE package (van Buuren & Groothuis-Oudshoorn, 2011) with 10 rounds of multiple imputations and a maximum of 20 iterations. Descriptive statistics in this report are based on the non-imputed data to represent the current sample accurately. All parameter estimates for inferential statistics are pooled estimates based on the imputed data, to make these results more generalizable and avoid a loss in power.
Results
The study included 83 service users with an average age of 48 years (SD = 12.5; range = 21–77). Among the disorders explicitly recorded by the MINI, the largest group among service users overall (n = 19; Table 1) and among men (n = 14) were those affected by psychotic disorders. Mood and affective disorders were the type of disorder most commonly found among women (n = 7). Several service users had at least two diagnoses, that is, comorbidities (n = 17). A large group of service users (n = 25) had a diagnosis that was no available category on the MINI for psychotic disorders, for example, dementia.
Frequency of ICD-10 diagnoses among service users by gender (N = 83).
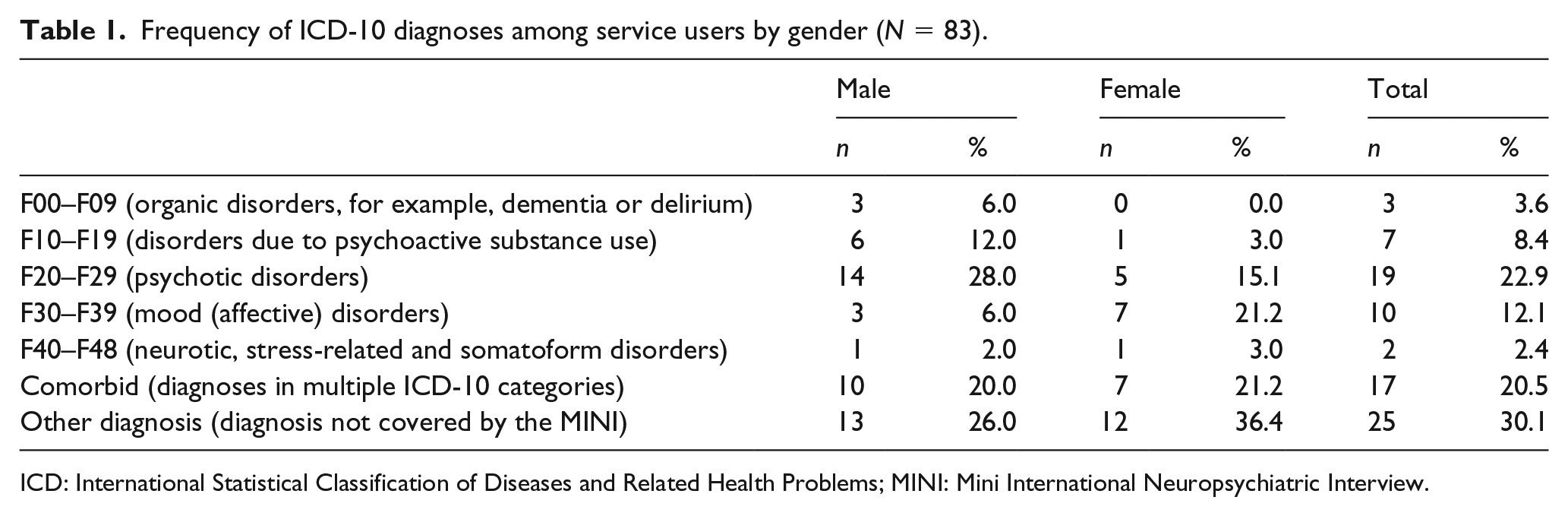
ICD: International Statistical Classification of Diseases and Related Health Problems; MINI: Mini International Neuropsychiatric Interview.
On average, service users reported 9.41 total needs, of which 4.29 were unmet, out of the 22 domains measured. Of the 83 service users, n = 39
Descriptive statistics and pooled correlation coefficients between the needs for care, the level of functioning, the quality of life and the service users’ age and gender.
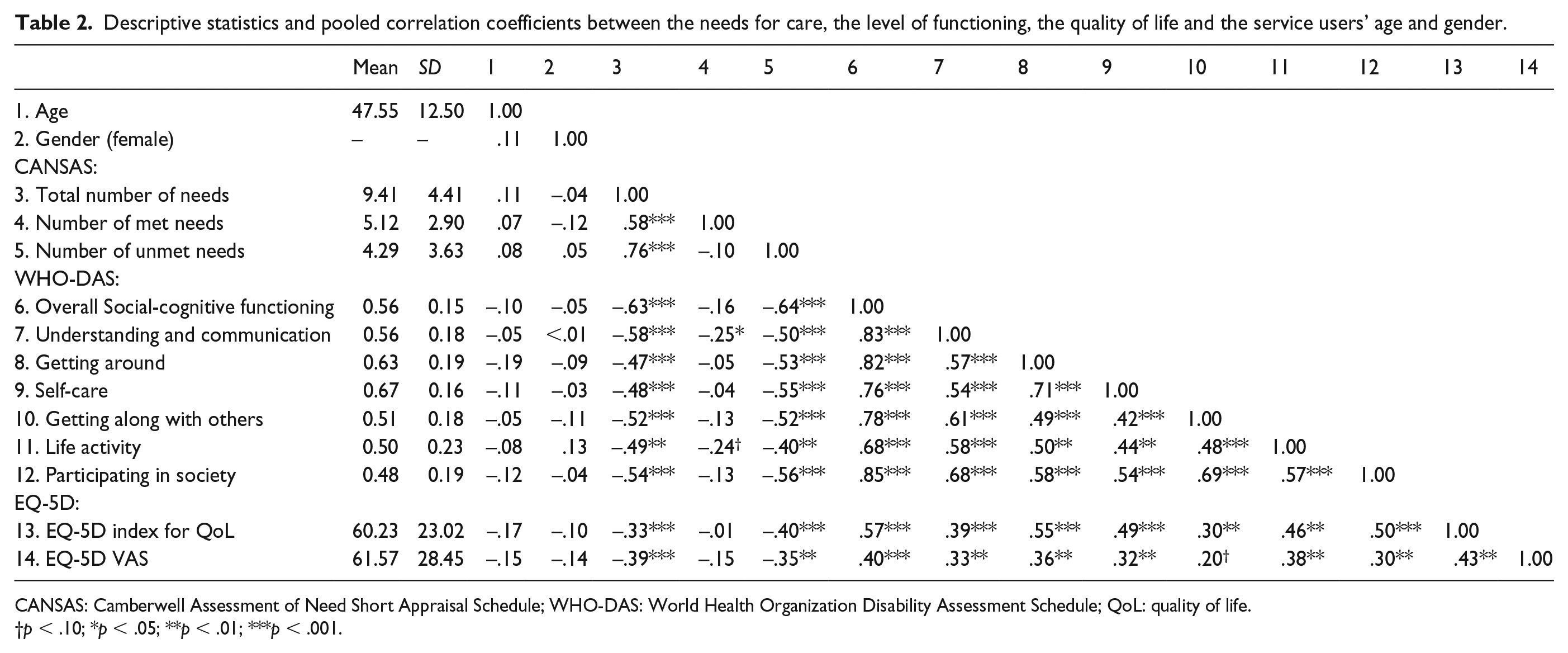
CANSAS: Camberwell Assessment of Need Short Appraisal Schedule; WHO-DAS: World Health Organization Disability Assessment Schedule; QoL: quality of life.
†p < .10; *p < .05; **p < .01; ***p < .001.
The pooled correlation coefficients between and among the needs for care, (domain specific) level of functioning and EQ-5D quality of life index are given in Table 2. Participants’ age or gender was not significantly correlated to the number of needs (total, met or unmet), the social-cognitive functioning (overall and domain specific) or the EQ-5D index for quality of life (compare Table 2; p values are provided in Supplemental Appendix A). Higher levels of social and cognitive functioning were positively, strongly correlated to quality of life (r = .57, p < .001). That is, the better someone is able to master day-to-day-tasks and maintain social ties, the higher they would report their overall quality of life. On average, lower levels of social-cognitive functioning were associated with more needs for care (r = –.63, p < .001). Only the number of unmet needs were strongly and significantly related to the level of functioning (r = –.64, p < .001), but not the number of met needs (r = –.16, p = .161). This pattern was also reflected in the association between needs for care and the quality of life. Having more needs overall, and furthermore, having more unmet needs, showed a moderate, negative correlation with lower quality of life (r = –.33, p = .001; r = –.40, p < .001).
Discussion
In the current study, we undertook a cross-sectional survey to assess the needs of care, level of social and cognitive functioning and quality of life among a consecutive sample of service users with mental health problems in the Republic of Moldova. Our findings show that participants with mostly severe mental disorders reported needs in 9.41 out of the 22 probed categories, which covered several domains of the social-, domestic-, economic-, and day-to-day life. Of these, on average 4.29 were unmet. In other words, of the 22 measured domains, participants reported needs among almost halve of them (42.77%) and had unmet needs in a fifth (19.50%). The typical service user was male, had received general secondary education, was single, unemployed and hospitalized at least once in the past year. The number of unmet needs is comparable to those found in a study in Vellore, India, where on average of 5.16 unmet needs were reported among service users with schizophrenia (Ernest, Nagarajan, & Jacob, 2013). In Europe, service users with severe mental illness in countries such as Great Britain, the Netherlands, Germany and Spain report four to eight needs on the CANSAS scale, with a two-to-one ratio of met-to-unmet needs (Wiersma, 2006). This indicates that patients from the current sample in Moldova have greater care needs compared service users with severe mental illness in studies from other parts of Europe. This may underscore the current challenges in existing mental health services in Moldova and highlight the need for a reform of services that caters more closely to service users’ needs. The majority of participants in this study had unmet needs concerning relationships with others, making it the most prominent category within unmet needs. This parallels our findings on level of functioning, in that service users reported few deficits in functioning domains related to ‘getting around’ and ‘self-care’ but reported difficulty on functioning domains related to social interaction, general participation in society and communicating with and understanding others. One factor contributing to reported problems and the high number of unmet needs in the social domain could be the prevailing discrimination and stigmatization associated to mental ill health in CEE countries (Petrea, 2012; Winkler et al., 2017), leaving service users feeling isolated. Moreover, while poverty has declined in recent years, Moldova remains one of the poorest countries in Europe (World Bank Group, 2016). Mutually reinforcing with high unemployment rates and vast emigration, this constitutes a hostile environment for the prevention, detection and treatment for mental health problems. While the high emigration rate has significantly contributed to the country’s economic growth through remittances, the flip side of the coin is a loss of social cohesion and support networks, for example, through the break-down of family ties (Pantiru, Black, & Sabates-Wheeler, 2007). Taken together, this social, economic and cultural environment is likely contributing to the high number of unmet needs. Finally, the inpatient, clinical-based care that service users in the sample were receiving may not afford sufficient opportunity for building meaningful social relationships, explaining the high number of unmet social needs.
Finding ways to address these specific needs is pivotal, given the close link between the number of unmet needs – in particular social needs – and the quality of life among mental health care service users. Previous research found this link consistently (Hansson et al., 2003; Ruggeri et al., 2004; Slade et al., 2004), and we corroborated this finding in our study. Addressing those unmet needs could therefore help to improve the quality of life of the service users. Overall, the participants in the current study reported a mean EQ-5D index for the quality of life of 60.23 (SD = 23.02) on scale ranging from 0 to 100. This is markedly lower in comparison to mental health service users in other countries. A Swedish study, for example, reported a mean quality of life of 69 among patients with major depressive disorder (Sobocki et al., 2007). Moreover, from the Central and Eastern European context, Winkler and colleagues report an EQ-5D index for quality of life between 77 and 80 among Czech mental health care service users suffering from a psychosis (Winkler, Koeser, et al., 2018). In South Africa, service users with severe mental disorders reported a quality of life (EQ-5D VAS) of 84 (out of 100), which is higher than service users in the current sample (Sibeko et al., 2017). In sum, service users in other studies using the same tool to assess quality of life and with similar mental health systems in transition to that of Moldova report a higher quality of life than in our sample, indicating that services can make steps towards further improvements in quality of life of service users.
These findings from our study together provide valuable insights for policymakers and service planners to guide the ongoing realization of community-based care in Moldova. Developing and implementing sustainable community-based mental health care services in Moldova, like in other country contexts, requires a thorough understanding of the care needs of the current service user population. An understanding of unmet needs provides valuable insights to stakeholders regarding which aspects of care can be improved, whereas an assessment of mental health status and functioning can help to direct and guide which mental health services might be most appropriate for service users currently receiving inpatient mental health care. Interventions addressing service users’ social skills may be helpful in improving service users’ level of functioning and quality of life. Compared to hospital-based, inpatient care, community mental health care aims to treat service users close to their own communities, therefore enabling them to partake in society and might address unmet social needs. Moving people to community-based care gradually could represent a helpful shift towards engaging more with community life and developing in social domains. However, decisions on the best treatment approach for a specific service user, including about the choice between community-based care or inpatient care, should always be made on an individual basis. Particular caution is needed for patients with severe mental health disease who also lack a social network or stable shelter, and where deinstitutionalization may not be a feasible option at the moment. We consider the best approach to be the development of individual treatment plans for each patient that rely on a thorough understanding of the personal needs, strengths and recovery goals. Such a treatment plan should be drafted in close collaboration with the patient and be built on shared or supported decision-making models (Pathare & Shields, 2012). This would also help address service users’ unmet needs with respect to information about their treatment. The present study may be able to shed light on the state of mental health care in Central and Eastern Europe, an area that continues to be a blind spot in international literature on mental health (Winkler et al., 2017). Our findings can also inform other national mental health reform processes and needs assessments, particularly in the context of middle-income countries with mental health systems in transition.
Limitations
Findings from this study should be interpreted in light of its limitations. Service users’ diagnoses were recorded with the MINI, version 7.0.2, for psychotic disorders, which only included a limited range of ICD-10 diagnoses as eligible categories, and not all disorders present among service users in the sample. With respect to EQ-5D index for quality of life, values for the current study were calculated on the basis of population norms derived from the populations from Western European, high-income countries and the correlation between the EQ-5D index and the self-reported quality of life on the VAS was moderate. This may indicate that the EQ-5D index calculated for the current study may deviate to some extent from actual value that people in the socio-economic and cultural setting would attach to a given health state. Finally, a particular high number of responses were missing for the WHO-DAS variable life activity (approximately a third). Conclusions regarding this domain should therefore be drawn with caution.
Conclusion
This study shows that assessing the needs for care and current level of functioning among service users is important to consider before further developing mental health services, to make more informed decisions about what types of interventions should be offered. Addressing unmet needs for care and areas in which service users experience disability could contribute to improve treatment effectiveness. Considering that service users report most problems with respect to their social life, interventions that enable service users to foster social ties are likely to help in this regard and can be provided by specialized care teams based in the community, which are now available in Moldova as a result of the ongoing mental health reform. An individualized treatment plan for mental health service users is needed to determine what balance of inpatient and outpatient care is most appropriate. Measures such as assessments of the needs for care and level of functioning can be drawn upon to make these decisions. Such a comprehensive patient assessment should become routine and emerge as a fixed part of the annual treatment cycle. These assessments should be carried out in close collaboration between patients and providers and should form the basis for the drafting and adjustment of treatment plans. Simultaneously, these assessments should help identify strengths and weaknesses of the health care system overall and guide its continuous evolution.
Supplemental Material
Appendix_A – Supplemental material for Taking steps towards deinstitutionalizing mental health care within a low and middle-income country: A cross-sectional study of service user needs in the Republic of Moldova
Supplemental material, Appendix_A for Taking steps towards deinstitutionalizing mental health care within a low and middle-income country: A cross-sectional study of service user needs in the Republic of Moldova by Jona J Frasch, Ionela Petrea, Jana Chihai, Filip Smit, Matthijs Oud and Laura Shields-Zeeman in International Journal of Social Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge Marjonneke de Vetten for her work in the formative phase of this project, Dr Raluca Nica for her work in designing and implementing this assessment and the Moldova reform project team for making this research possible. We gratefully acknowledge the project mandate and funding for the Moldova reform project from the Swiss Agency for Development and Cooperation (SDC), project number 7F08711.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted in the context of the Moldova reform project, a project funded by the Swiss Agency for Development and Cooperation (SDC, project number 7F08711) and implemented by the Trimbos Institute in the Netherlands. The views expressed in this publication are those of the authors and do not necessarily reflect the views of the SDC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.