
Abstract
Background:
Shared decision making (SDM) is recognised as a promising strategy to enhance good collaboration between clinicians and service users, yet it is not practised regularly in mental health.
Aims:
Develop and evaluate a novel training programme to enhance SDM in psychiatric medication management for service users, psychiatrists and care co-ordinators.
Methods:
The training programme design was informed by existing literature and local stakeholders consultations. Parallel group-based training programmes on SDM process were delivered to community mental health service users and providers. Evaluation consisted of quantitative measures at baseline and 12-month follow-up, post-programme participant feedback and qualitative interviews.
Results:
Training was provided to 47 service users, 35 care-coordinators and 12 psychiatrists. Participant feedback was generally positive. Statistically significant changes in service users’ decisional conflict and perceptions of practitioners’ interactional style in promoting SDM occurred at the follow-up. Qualitative data suggested positive impacts on service users’ and care co-ordinators confidence to explore medication experience, and group-based training was valued.
Conclusions:
The programme was generally acceptable to service users and practitioners. This indicates the value of conducting a larger study and exploring application for non-medical decisions.
Keywords
Introduction
Shared decision making (SDM) is a process of exchanging information and preferences concerning an intervention, aimed at reaching an agreed, decision (Charles, Gafni, & Whealan, 1999; Edwards & Elwyn, 2009; O’Connor, 2005).
It was developed in mental health as a response to the well-documented difficulties in ensuring concordance about psychiatric medication and the existing doubts about the efficacy of psychiatric medication (Morrison, Hutton, Shiers, & Turkington, 2012; Nose, Barbui, & Tansella, 2003). Given the dominance of medication as an intervention in the mental health field, the pilot project described below focused on SDM in psychiatric medication management.
SDM is recognised as a promising strategy for enhancing collaboration between clinicians and service users, due to complementary knowledge brought to the SDM process (Morant, Kaminskiy, & Ramon, 2015). Participation in treatment decision-making is desired by many service users (Joosten et al., 2008), is feasible even during an acute admission (Hamman et al., 2006), improves service users’ satisfaction (Loh, Simon, & Wills, 2007), self-efficacy and self-confidence, likely to empower and to reduce the use of coercion (Stovell, Morrison, Panyiotou, & Hutton, 2016). It is also a core component of person-centred care (Ahmed, Ellins, Krelle, & Lawrie, 2014; Davidson, Tondora, Pavlo, & Stanhope, 2017) and of co-production between service users and providers (Clark, 2015; Coalition for Collaborative Care: Action for Long-Term Condition, 2017).
At present, there is only a small number of known randomised controlled trial (RCT) studies on mental health SDM (Hamann et al., 2011; Loh et al., 2007; Stovell et al., 2016), but there is a growth in researching attitudes to it of service providers and users (Eliacin, Salyers, Kukla, & Matthias, 2015; Puchner et al., 2016) of different age groups (O’Neal et al., 2008; Simmons, Hetrick & Jorm 2010) and in developing decision-making aids (Deegan, 2010).
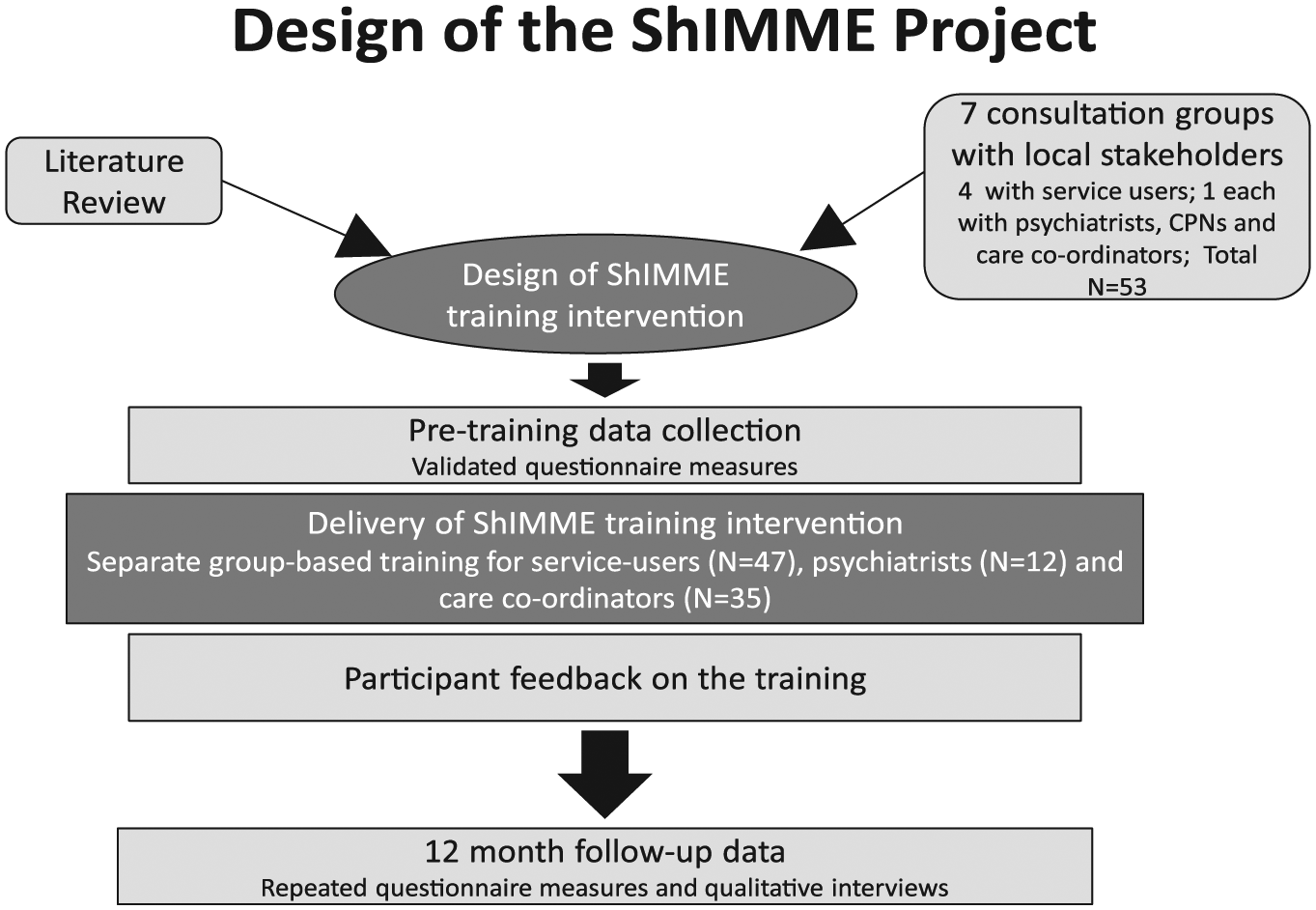
Previous interventions on SDM in psychiatric medication management targeted either prescribers (Priebe et al., 2007) or service users (Deegan, Rapp, Holter, & Riefer, 2008). Yet as change may best be achieved by simultaneously targeting all those involved in this process this project aimed to develop and evaluate the feasibility, acceptability and impact of training for service users, psychiatrists and care co-ordinators (who may come from nursing, occupational therapy or social work) to encourage SDM in the prescription and management of psychiatric medication, focusing on people with long-term mental ill health (see Figure 1).
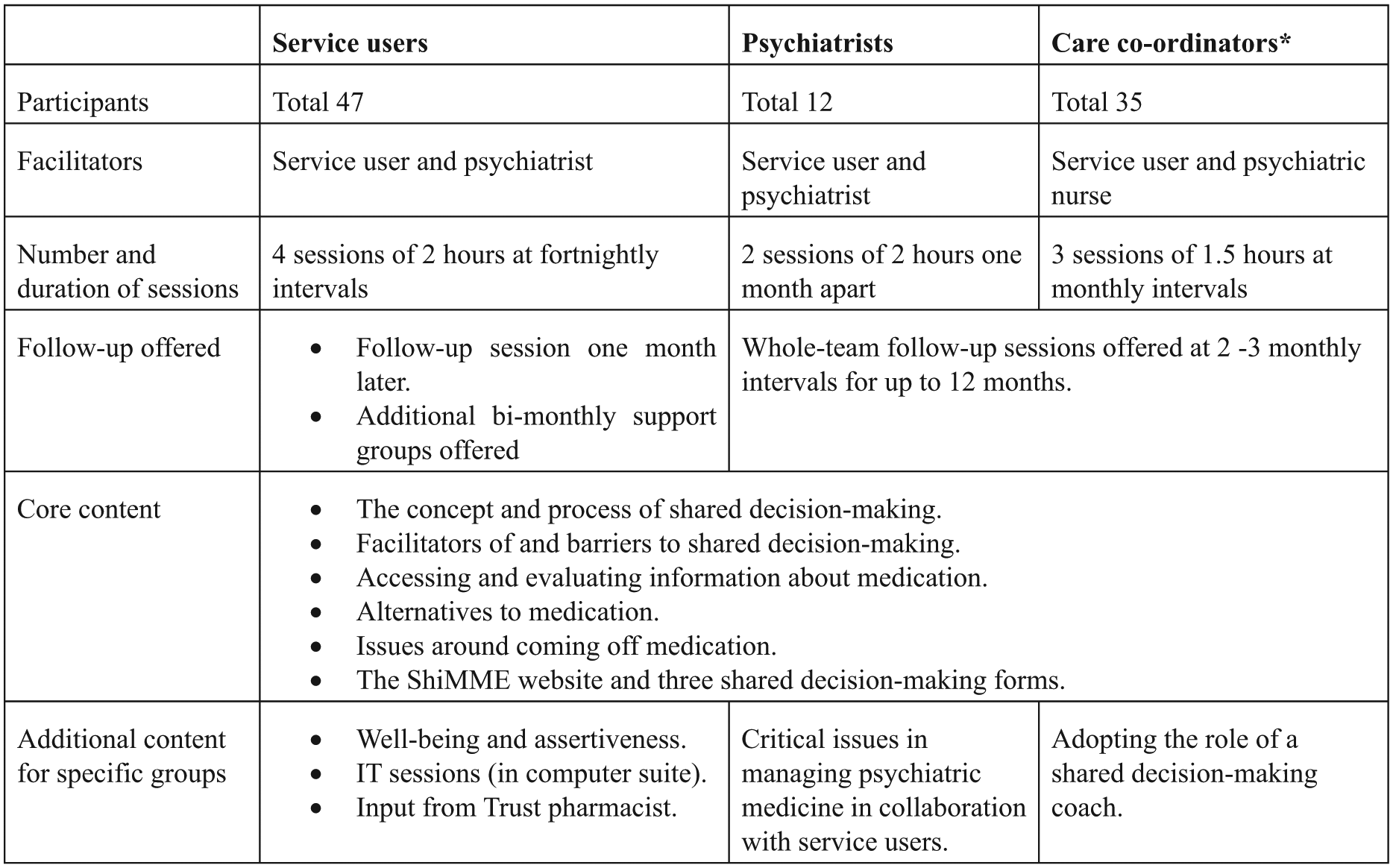
Format and content of ShiMME training programmes.
Specific objectives were as follows:
Develop a training programme designed to promote SDM processes in psychiatric medication management, based on existing literature and consultations with relevant stakeholders.
Deliver this training separately to groups of service users, psychiatrists and care co-ordinators in adult community psychiatric settings.
Investigate the impact of the training on enhancing the application of SDM at medication reviews by applying a mixed-method process and outcome (detailed below).
Methods
Setting
The project was guided by participatory principles (Reason & Bradbury, 2008), and conducted in community services for adults with long-term mental health problems of an East of England National Health Services (NHS) Trust. Ethical approval was obtained from the local NHS Research Ethics Committee.
Intervention design
A scoping search of internationally published, grey literature, and Internet material on SDM was conducted. Local stakeholder consultation took place via focus groups with service users, psychiatrists, and care co-ordinators (total N = 53). Discussions centred on current decision-making practices in psychiatric medication, preferences for how this could be improved, perceived facilitators and barriers and suggestions for the content and format of the training intervention. (see Kaminskiy, Ramon & Morant, 2013; Stead, Morant, & Ramon, 2017).
A working group with service users trainers (i.e. people who use mental health services, trained to offer training to providers and service users), practitioners and researchers developed the training programme format, content, materials, and decision aids. This included designing a web-site containing training support materials, links to other relevant resources, four videos of medication-related consultations played by trained actors and forms to support and record SDM processes (preferences, priorities and feedback).
Intervention format, content and delivery
Training was delivered to separate groups of service users, psychiatrists and care co-ordinators, providing a safe environment for open discussion among peers and addressing their specific training needs, by a professional and a service user trainer. Group sizes ranged from 2 to 12; a variety of group-based and participatory learning techniques were employed. The core content was the same for all groups, and focused on the process of SDM. Stakeholders’ groups-specific variations are shown in Figure 1; the most important of which is the focus on assertiveness in the training for service users. Training sessions were delivered at fortnightly or monthly intervals to allow individual self-study using web-site materials, opportunities to implement new skills in practice, and access to additional user-trainer support for service users. Training groups were held throughout 2013 in the Trust’s and University locations.
Participants and recruitment
Service user inclusion criteria were as follows: being in the care of Rehabilitation and Recovery services for at least 6 months; having one or more of the diagnoses of schizophrenia, bi-polar disorder and depression, taking any psychiatric medication (antipsychotics, mood stabilisers, anti-depressants or anxiolytics) currently and for at least 6 months previously, selected for participation by a member of their clinical team, having capacity to consent, able to speak and understand English without an interpreter, and aged 18–65.
Suitable potential participants were sent an initial invitation letter by members of their clinical team, who were available for preliminary discussions. Interested service users were then provided with more information by researchers. Training was offered to all psychiatrists and care coordinators who prescribe, monitor or discuss medication with this group of service users.
Data collection
As the study aimed to design and evaluate a novel intervention, a randomised design was considered premature for this early stage of development (Craig, Dieppe, & Macintyre, 2008). The intervention was evaluated within a multi-method process and outcome-oriented approach within a before and after, uncontrolled design (see Figure 2). This assessed the impact of the training on medication decision-making; feasibility, acceptability and participant experiences of the training programme; and cost effectiveness. At the end of the training programme, participants were asked to anonymously evaluate the value of the training for them. As the training lasted for a short duration, an evaluation of the outcomes at that stage was premature.
Quantitative measures.
Study Design.
In line with recommendations for evaluating SDM (Joosten et al., 2008), multiple relevant outcomes were assessed. Measures were completed at pre-training baseline and again at the 12 months follow-up point.
Service users completed the following measures:
The 16 items Decision Conflict Scale (DCS, O’Connor, 2005) measure of service users’ views their medication decisions, with 5 related subscales assessing: access to information, values clarity, feelings of support, certainty in decision and whether the decision is likely to be implemented. This tool is well validated, sensitive to changes following decision support interventions (O’Connor et al., 2009), and applicable in mental health settings (Bunn & O’Connor, 1996).
The 12-item ‘Scale to assess therapeutic relationships in community mental health care’ (STAR) (McGuire-Snieckus, McCabe, Catty, Hansson, & Pribe, 2007). Participating psychiatrists and care co-ordinators completed the STAR clinicians’ version in relation to two service users whose medication management they regarded as ‘problematic’ and ‘very satisfactory’ at baseline and at 12 months follow-up. For the statistical tests applied, see introduction to the data analysis section.
The 12-item OPTION scale (Elwyn, Edwards, & Wensing, 2003) was adapted to assess service users’ self-report of whether clinicians’ interactive styles promoted SDM.
Two ratings of decision-making in preferred and current medication management practice were obtained using the single item Control Preferences Scale (CPS; Degner et al., 1997), asking respondents to endorse 1 of 5 statements ranging from decision-making entirely by the doctor to decision-making entirely by the service user.
Attitudes to taking medication were assessed using the Drug Attitude Inventory (DAI short version; Hogan, Awad, & Eastwood, 1983).
2. Qualitative measures.
Training intervention feasibility, acceptability and participant experiences
Participants’ anonymous written feedback on the training programme via fixed-format, and open questions were completed after each session, and immediately after programme completion. These asked what participants hoped to learn from the programme, views on its content, impact, practical aspects, teaching methods and support materials.
To gain greater understanding of participants’ experiences and the perceived impacts of the training programme, we also conducted semi-structured interviews with sub-samples of service users (n = 12), psychiatrists (n = 6) and care co-ordinators (n = 11) at 12 months follow-up. Service users were interviewed by service users trained in interviewing, while professionals were interviewed by academic researchers. Questions focused on professional-client discussions about medication following the intervention, changes to medication and impacts on well-being, evaluation of the intervention and suggestions for improvements.
3. Cost effectiveness.
Socio-demographics and service use information were obtained at baseline and 12 month follow-up using the Client Sociodemographic Service Receipt Inventory (CSSRI) (Chisholm et al., 1999), analysed by an experienced health economists team, alongside unit cost information.
Data analysis
Quantitative outcome data were analysed using paired t tests or non-parametric within-subject tests where appropriate, to compare pre-training and follow-up scores (DCS, OPTION, STAR, and DAI measures). CPS data were analysed using Pearson’s exact chi squared test. For all tests, p values of < 0.05 were considered significant. Written feedback data were collated for descriptive analysis. Qualitative data from semi- structured interviews were transcribed verbatim, and analysed using thematic analysis (Braun & Clark, 2006). To assess health economic impacts, total costs of the intervention per person were estimated. Service use costs (health/social services and medication) in the year before and following the intervention were obtained by combining CSSRI data with unit cost information (Curtis, 2009).
Results
Participant characteristics
In all, 47 service users, 35 care co-ordinators and 12 psychiatrists participated in our training programme. Attendance, demographic, clinical and professional characteristics of service user and practitioner participants are shown in Tables 1 and 2. Attendance at training sessions was generally high across all groups. Service users had a high level of formal education, very few were in work; the majority were in receipt of state benefits, had long histories of service contact (17.2 years on average) and were high users of medication (5 medications on average, of which 3 were for mental health problems). Twenty service users (43%) took mood stabilisers, 21 (45%) took antidepressants and 32 (68%) were on antipsychotic medication.
Demographic characteristics and attendance of the service user group (N = 47).
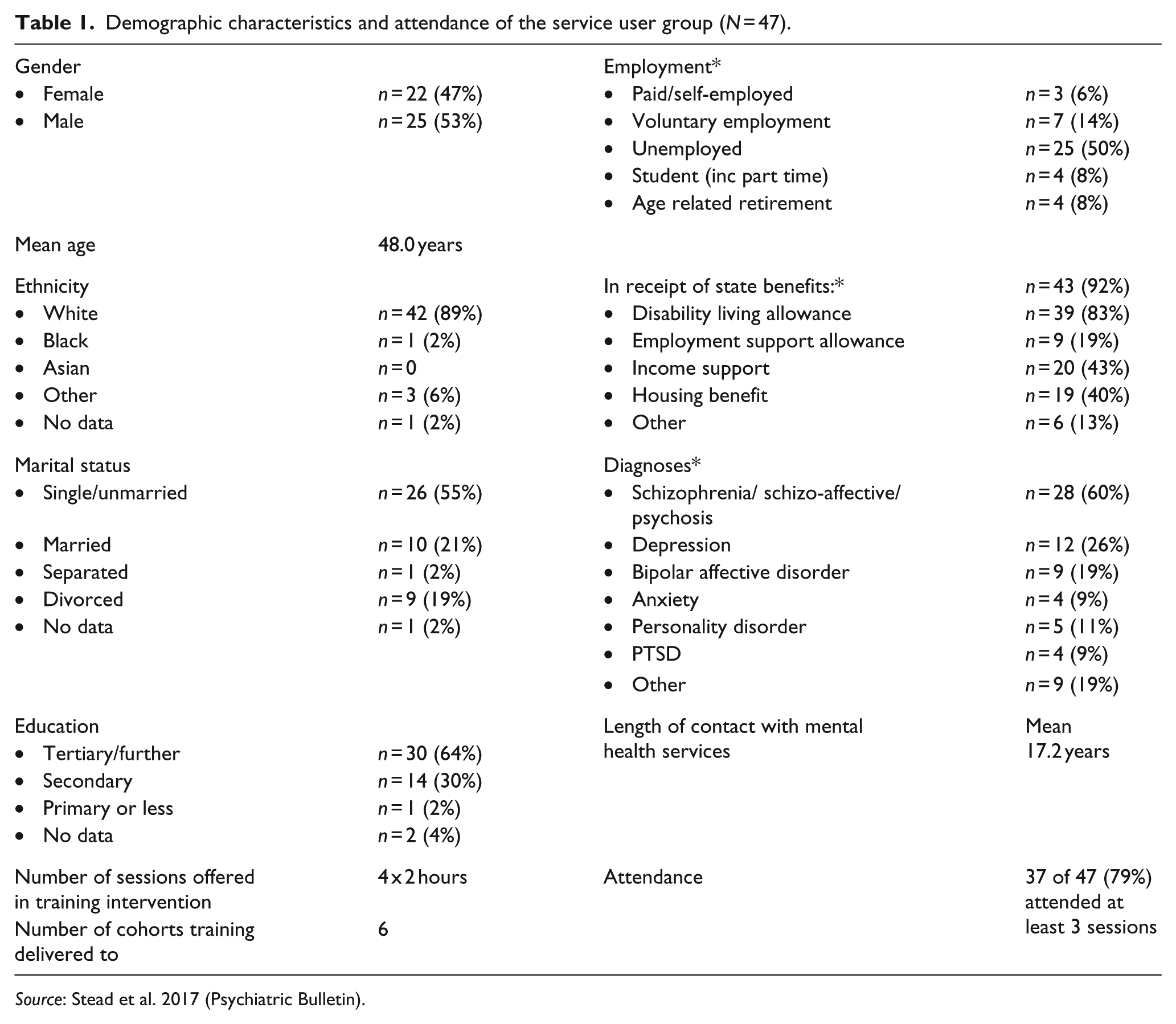
Source: Stead et al. 2017 (Psychiatric Bulletin).
Demographic characteristics and attendance of clinicians.
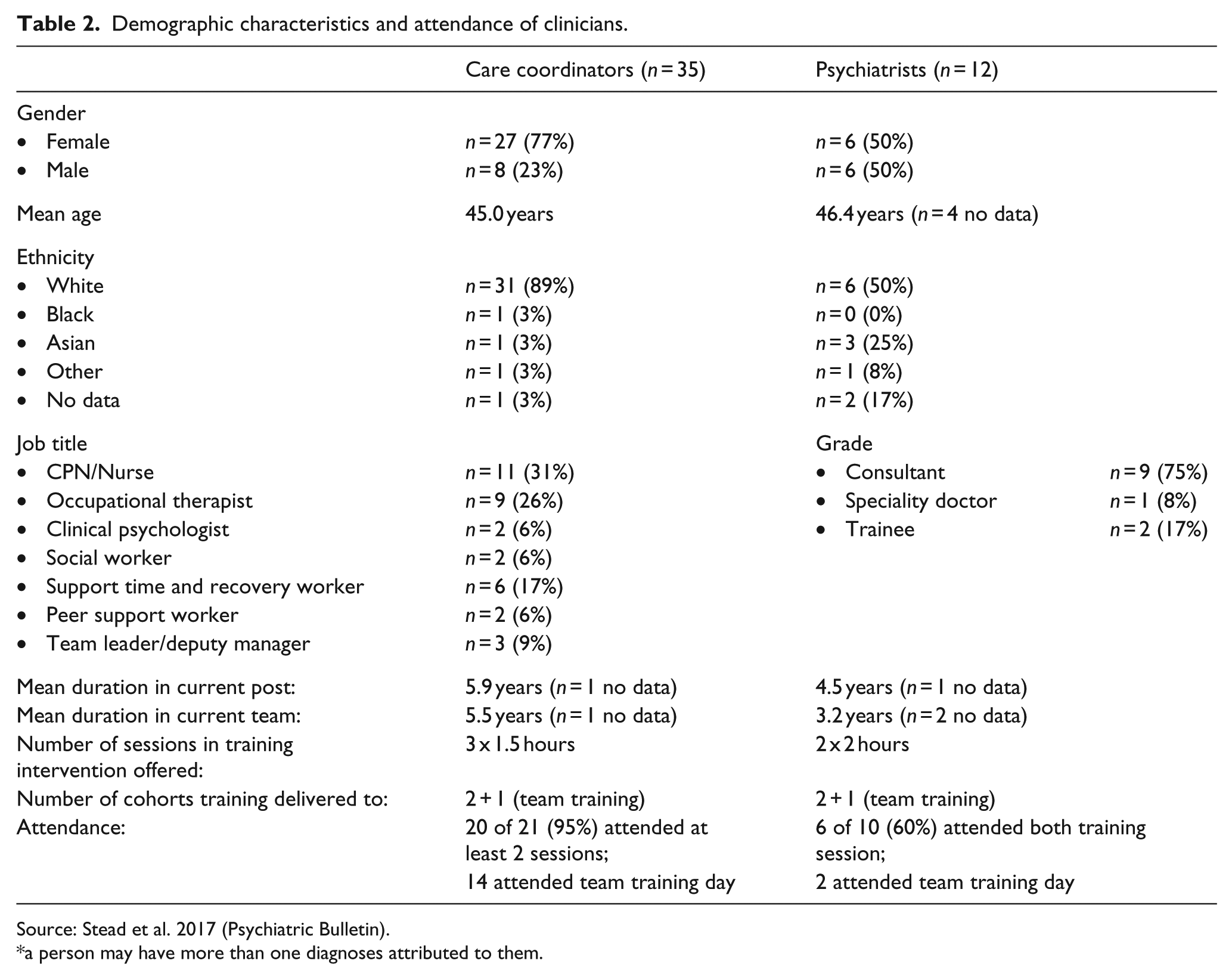
Source: Stead et al. 2017 (Psychiatric Bulletin).
a person may have more than one diagnoses attributed to them.
Nine of the psychiatrist participants were consultants. Community psychiatric nurses and occupational therapists were the most common professional groups among care co-ordinator participants, with a few non-medical and non-professional groups also represented (clinical psychologists, social workers, support workers and peer support workers).
Impact of the training: quantitative measures
Pre-training quantitative data were provided by 100% of participants. At 12-month follow-up data were obtained from 33 service users (70%), 11 care co-ordinators (31%) and 6 psychiatrists (50%). Sensitivity analyses conducted on the main measures did not suggest biases due to missing data at follow-up (see findings in Table 3).
Primary service user outcomes: DCS, OPTION and DAI measures.
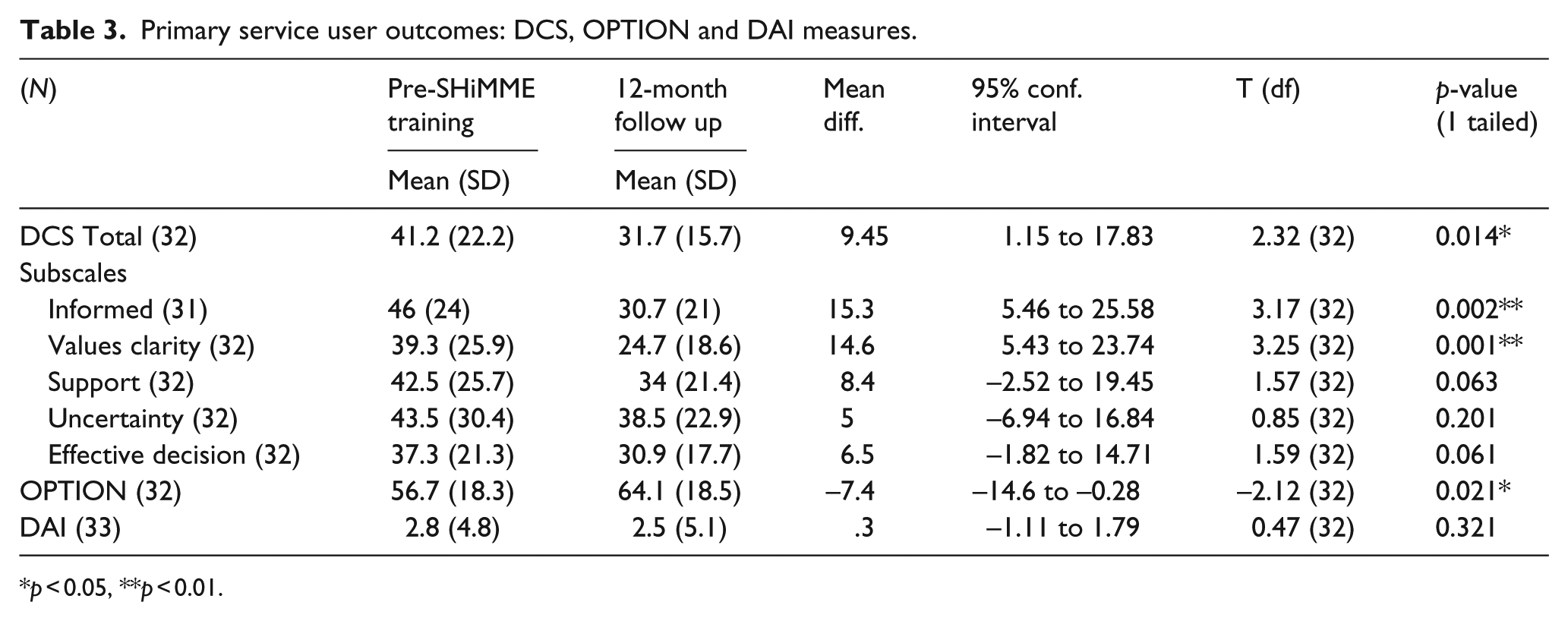
p < 0.05, **p < 0.01.
Service users
Changes between pre-training and 12-month follow-up scores for service users on the DCS total score and sub-scales indicated decrease of decisional conflict. These changes reached statistical significance for the subscales for feeling informed (p = 0.002) and clarity of values (p = 0.001). Changes on the total score (p = 0.014) and 2 of the other 3 sub-scales on this measure approached statistical significance (feeling supported p = 0.063, and feeling an effective decision has been made p = 0.061). There was also a statistically significant change on the OPTION scale (p = 0.021), representing an increase in practitioners’ interactional style in promoting SDM as perceived by service users. Scores on the DAI did not show significant changes, remaining constant at a neutral to positive position on average between baseline and follow-up (p = 0.321). Service users’ ratings of the quality of their therapeutic relationships were in the neutral to positive range, but significantly lower for their psychiatrist than for the other mental health practitioner involved at both baseline and follow-up (p < 0.001). Ratings of both these relationships showed no changes between baseline and follow-up in both total scores and sub-scales.
On the single item CPS ratings of medication decision-making with psychiatrists, the modal preferred style was consistently ‘the doctor and I make the decision together’ (indicated by 69% of the respondents at baseline and 56% at follow-up). No respondents indicated a preferred style which did not involve them in decision-making to some extent.
Ratings of how medication decisions are usually made showed that both at baseline and follow-up the majority of responses were split between ‘the doctor and I make the decision together’ and ‘the doctor makes the decision after seriously considering my opinion’ (66% of the respondents at baseline and 78% at follow-up gave one of these responses). At baseline, 10 service users (31%) selected ‘the doctor makes the decision’ to describe usual medication decision-making, compared to only 3 (9%) at follow-up.
Practitioners
As numbers at the follow-up were small, analysis was conducted on both practitioner groups together. This provided a baseline sample of 47 and a follow-up sample of 17. Analysis carried out on each group separately produced very similar results to those of the combined sample. At both baseline and follow-up, practitioners rated their relationship with a service user whose medication management was ‘very satisfactory’ as significantly better than for someone for whom this was ‘problematic’ (p = 0.002 at baseline, p < 0.000 at follow-up). No significant changes in these ratings were found between baseline and follow-up.
Service use and costs
Service use information shows decreases in hospitalisation and increases in community activities for all but two service users at follow-up. For 39.7% of service users reduced decisional conflict following the intervention was associated with lower service use costs, while for 57.5% this was associated with slightly increased costs. Long periods of hospitalisation for 2 individuals contributed substantially to increased costs. These findings indicate the potential of lowering costs in a larger sample.
Experiences of the training: feedback questionnaires
Immediate post programme feedback data were obtained from 33 (70%) service users, 22 (63%) care coordinators and 6 (50%) psychiatrists. The training programme mostly met respondents’ expectations, and high levels of satisfaction with its content and pitch of teaching were reported by the majority of service users and care coordinators. Comments included ‘I feel more able to influence my treatment rather than taking a passive role’ (service user); ‘Overall I found it very informative and I feel it’s given me more confidence in this area’ (care-coordinator).
Psychiatrists’ evaluations of the content and level of teaching were more mixed:
Well, it would be good to set realistic expectations, because some people, especially people with schizophrenia they sometimes have a lack of insight… so on one hand it may make their relationship much closer and better on the other hand that might also lead to some confrontation about … now I have read a few side effects about the medication I want to stop my medication. (PSY06) the approach to the topic occasionally felt stereotypical towards psychiatrists and how they liaise with patients. Psychiatrists were portrayed in a negative light; at some points the approach underestimated psychiatrists’ knowledge or interest in collaborative work. (PSY01)
All stakeholder groups particularly valued opportunities for discussion, exchange of ideas and experiences with peers. Practitioners appreciated suggestions for information and SDM support tools. Use of the project website was variable, with most psychiatrists, about half of service users, but less than a third of care coordinators having accessed the website.
Both groups of practitioners considered the programme relevant to their clinical practice, but were less certain that it would shape their future practice. Service users too were cautious about the future impact of the programme on practice (see further discussion in Stead et al. (2017).
Experienced impact of the training: semi-structured interviews at 12-month follow-up
Interviews with service users reflected the generally positive views seen in post-training feedback. High levels of satisfaction were explained in terms of feeling empowered, increased understanding of their experiences by practitioners, and an improved sense of wellbeing. They valued also the group-based nature of the training that enabled peer support and social connections. Areas earmarked for improvement in the training programme were information technology (IT) arrangements, request for more sessions and managing group dynamics:
It definitely makes me ask questions about what’s being offered, you know, wanting to be really clear what the side effects are as well as the helpfulness of the drug. I think to speak up and not be so kind of placid always and just accepting what people say, but questioning what it is that I am being offered. Yeah, I think I feel more confident about going to see the psychiatrist than I did initially, yeah. (Service user)
Interviewed care co-ordinators’ and psychiatrists’ views at the immediate post-programme feedback were similar to their views at 12-month follow-up. Care co-ordinators valued the training more than psychiatrists, citing the value of time and space to reflect on SDM, the usefulness of the informal yet challenging approach to training, and the opportunity to develop their practice:
I’ve worked with a few clients where they’ve never thought about opening up about medication, and they’ve had the belief that actually it is already decided and that they don’t have a choice. So the project has been really good for opening that up… and it sort of broadened my awareness of that importance of sharing, and if I hadn’t have done the project I don’t know whether that awareness would have been as prominent as it is now. (Care co-ordinator)
Some practitioners felt they had gained confidence to open dialogues about medication with service users, and had become more aware of the importance of helping service users in having a choice:
I think I am definitely much more open and … I don’t feel so scared of having those medication conversations, because obviously there’s always that fear, as soon as you start talking about medication, what’s going to happen, there’s always that fear of what’s the next step. And I think having done the project I don’t feel that fear, I feel quite comfortable, with service user, about what they would like, what they see would be the best for them and having that open discussion … and being able to come up with a mutual decision. (Care co-ordinator) Yes. I think it has had impact in different ways; in my meetings with the patients, in my care plan reviews or medication reviews, I have been more focused in sharing more information, proposing different options, granting to the patient the final choice about medication. (Psychiatrist)
One psychiatrists spoke about experiencing tensions between his medical responsibility and the risks associated with reducing medication, stating ‘that’s why I am pulling my hair with this shared decision’. Improvements were called for in reducing the focus on decision-aid forms, their length and format. Asked about using SDM in the future, more service users and care co-ordinators than psychiatrists said they would like SDM to be an integral part of everyday practice.
Discussion
This is the first UK based study to develop and evaluate a training intervention to promote SDM for psychiatric medication that targets both service users and practitioners. The generally high level of attendance at training sessions suggests good acceptability and engagement. This was confirmed by service users’ end of training feedback and 12-month follow-up interviews. Feedback from practitioners at these two points was also positive, although less so among psychiatrists.
Quantitative measures showed encouraging changes among service users. They reported significantly reduced decisional conflict scores. Statistically significant changes were found on DCS sub-scales measuring feeling informed and clarity about personal values underpinning decisions, both of which may contribute to service users feeling more empowered and developing greater confidence in decisional involvement and self-management (Stovell et al., 2016). They indicated clear and consistent preferences for equal roles with psychiatrists in medication decision-making. Their ratings of usual practice suggested that doctors tended to have greater decision-making roles, especially at baseline when a third of respondent endorsed the most extreme statement (‘the doctor makes the decision’) suggesting little or no involvement. No changes in service users’ attitudes to medication were found following training. Similarly, neither service users nor practitioners reported changes in therapeutic relationship quality, with service users consistently rating relationships with prescribing psychiatrists as less strong than for other practitioners involved in medication management.
Most existing SDM research in mental health focuses on attitudes of service users and practitioners, with fewer studies developing decision making aids or evaluating their application. Compared to a decade ago, there is currently more interest in promoting SDM across stakeholder groups and countries. However, it is still rare to find an articulation of the conceptual aspects of SDM, and the differential power relations related to it (Kaminskiy, 2015; Morant et al., 2015).
The connection of SDM to the strengths approach and the new meaning of recovery, and its role in enhancing therapeutic alliances is beginning to be reflected in the literature (e.g. Deegan et al., 2008). For some, SDM is a potential route to increasing service users’ agency and self-management (The King’s Fund, 2011), while for others it is a tool to enhance treatment adherence (Nice, 2009).
Strengths and limitations
The project had a strong co-production ethos between researchers, service users and practitioners. This ensured that the agendas and concerns of both service users and practitioners were reflected in the design and delivery of the intervention (Stayley, 2014). Training content recognised the significance of power, and the need to acknowledge and challenge power inequalities among partners to the SDM process. Thus, assertiveness training was included for service users, while practitioners heard direct service user experiences, and were exposed to being trained by both professionals and service user trainers as equals.
Although the study had broad inclusion criteria, these depended on clinicians’ interpretations. Training for practitioners did not provide sufficient opportunities for post training support. While the decision aids forms were subject to three developmental cycles, practitioners remained unconvinced of their practical utility, and their uptake was low.
There are several methodological limitations of the training evaluation. Response rates at 12-month follow-up were poor among practitioners – due primarily to demoralisation resulting from service reorganisation – sample sizes were small, and there were no comparison group. These limit the strength and generalisability of the conclusions we are able to draw from the quantitative data. However, triangulating with other data sources – training feedback and semi-structured interviews at 12-month follow-up – allows us to build up a rich, if tentative, picture of the strengths, weaknesses and impact of the training programme.
Practice implications and further developments
The training intervention developed in this study provided a largely feasible and acceptable way of enhancing SDM relating to psychiatric medication. This suggests it is possible to move towards more equal and collaborative discussion and decision processes between people who take medication and their key providers in medication management. The project also highlights the value of including a wide range of mental health practitioners in SDM training. Compared to psychiatrists, care co-ordinators have more regular contact with service users, including in service users’ home environment. Although most of them do not make medication decisions, they can discuss both positive and negative impacts of medication, and may have greater awareness than psychiatrists of how it impacts on service users’ social functioning. Hence, this group is well-placed to implement components of SDM such as supporting service users to access appropriate medication information or raise concerns with psychiatrists.
The frequency and nature of repeat or ‘top-up’ training for practitioners required to ensure sustainability of these principles over time to become embedded in clinical practice remains unexplored in this article. The training programme is relatively simple, short and inexpensive, and could be easily adapted for implementation in many mental health settings. Given that service user participants in this study had long-term experiences of primarily severe mental health problems, similar training interventions may be as, or more, effective for those experiencing shorter or milder forms of mental ill-health. There is also potential for broadening the scope of this training to cover non-medical aspects of mental health interventions.
The less positive response to the programme of psychiatrists than care-coordinators warrants further exploration. Existing research highlights psychiatrists’ focus on an assumed lack of insight by service users of their mental ill-health as a key barrier to engaging in SDM (Shepherd, Shorthouse, & Gask, 2014). Engaging trainee psychiatrists early on in their career in the training of SDM, alongside service users, would be a useful move in this direction. The NHS Trust within which this work was conducted has taken on SDM as a preferred policy across all pathways, and now provides training on SDM processes to additional groups of practitioners (e.g. non-medical prescribers), and service users. The impact and organisational processes of embedding this type of innovation in standard mental health practice is worthy of research attention. The results indicate the value of conducting a larger research study that incorporates a randomised design with more representative samples across multiple settings.
Footnotes
Acknowledgements
We wish to thank all participants in this study. In particular, we wish to thank Fiona Blake, Judy Dean, Furhan Iqbal, Sheena Mooney, Carole Morgan, Mary Jane O’Sullivan and Sarah Rae.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Institute for Health Research under its Research for Patient Benefit (RfPB) programme (PG-BG- 0909-20054), for which we are grateful. Views expressed are those of the authors and do not necessarily represent those of the NHS, the NIHR or the Department of Health.