
Abstract
Objective:
This study sought to investigate the impact of a service user-led anti-stigma and discrimination education programme, encompassing numerous interventions focused on facilitating multiple forms of social contact, the promotion of recovery, and respect for human rights, on medical student attitudes.
Method:
A comparison cohort study was used to compare the attitudes of two cohorts of medical students who received this programme as part of their fifth (the fifth-year cohort) or sixth (the sixth-year cohort) year psychological medical education attachment (programme cohorts) with two cohorts of equivalent students who received a standard psychological medical attachment (control cohorts). Attitudes to recovery (using the Recovery Attitudes Questionnaire) and stigma (using the Opening Minds Scale for Healthcare Providers) were measured at the beginning and end of the attachments for each year and compared both within and between the cohorts using Wilcoxon signed-rank or Wilcoxon rank-sum tests.
Results:
With sample sizes ranging from 46 to 70 across all cohorts, after their psychological medicine attachment both the programme and control cohorts showed more positive attitudes towards recovery and less stigmatising attitudes towards people with lived experience of mental distress. Significant differences between the programme cohorts and the control cohorts were found for recovery attitudes (median difference of 2, p < 0.05 in both fifth and sixth year), with particularly large differences being found for the ‘recovery is possible and needs faith’ subdomain of the Recovery Attitudes Questionnaire. There were no significant between cohort differences in terms of stigmatising attitudes as measured by the Opening Minds Scale for Healthcare Providers.
Conclusion:
The introduction of a comprehensive service user-led anti-stigma and education programme resulted in significant improvements in recovery attitudes compared to a control cohort. However, it was not found to be similarly superior in facilitating less stigmatising attitudes. Various possible reasons for this are discussed.
Introduction
The Report of the United Nations High Commissioner for Human Rights identifies discrimination and denial of human rights as serious challenges faced by People with experience of Mental Distress (PwMD) and calls for mental health services to be recovery-focused (United Nations High Commissioner for Human Rights, 2017). The active involvement of PwMD in training healthcare providers is identified as a particular action that can support this call. This is echoed in the World Health Organization’s (WHO) Mental Health Action Plan (World Health Organization, 2013). The Convention on the Rights of Persons with Disabilities (CRPD) exists to promote, protect and ensure human rights for persons with disabilities (including PwMD), with principles which include non-discrimination and social inclusion (United Nations, 2007). The WHO have developed the Quality Rights training package, which provides guidance on implementing a recovery and human rights approach in mental health, in accordance with the CRPD (see www.who.int/publications/i/item/who-qualityrights-guidance-and-training-tools).
Australia’s Fifth National Mental Health and Suicide Prevention Plan requires state governments to make the WHO Quality Rights package available to healthcare providers (Department of Health, 2017). This is intended to support its aims of promoting recovery, reducing stigma and ensuring the rights and social participation of PwMD. The Plan also notes the important role that PwMD play in addressing stigma and discrimination, by providing social contact and positive role modelling. New Zealand’s He Ara Oranga, the Report of the Government Inquiry into Mental Health and Addiction, also identifies the need for improved training for healthcare professionals to support them to provide effective, non-pharmaceutical responses to mental health and addiction issues (New Zealand Government, 2018). New Zealand’s Mental Health and Addiction Workforce Action Plan 2017–2021 specifically identifies that PwMD should have a role in training and development for the mental health and addiction workforce (Ministry of Health, 2018).
The Royal Australian and New Zealand College of Psychiatrists (RANZCP) has identified recovery, social inclusion, avoiding stigma and discrimination, and disability rights as a paramount focus of mental health services (RANZCP, 2013, 2016). RANZCP has recommended that the expertise of PwMD is incorporated into training (RANZCP, 2014).
Research on psychiatric medical school attachments’ impact on reducing stigmatising attitudes is conflicting with positive (e.g. Bingham and O’Brien, 2018; Economou et al., 2017; Petkari et al., 2018; Shen et al., 2014), mixed (e.g. Ay et al., 2006; Da Rocha Neto et al., 2017; Reddy et al., 2005), no improvement (Hofmann et al., 2013; Zhu et al., 2018) and more stigmatisation (Omori et al., 2012; Totic et al., 2012) being found. A review by Luigi et al. (2020) concluded, ‘[t]rainee psychiatrists’ and medical students’ traditional rotations contribute to developing sceptical or negative expectations for recovery and towards the expert status of service users’ (p. 8) and that ‘clinical experience in hospitals seems to reinforce the beliefs of chronicity and incurability of mental illnesses such as schizophrenia’ (p. 6). Best practice for countering healthcare provider stigma and discrimination includes multiple forms of favourable social contact, the promotion of recovery, and respect for human rights (Ashton et al., 2018; Knaak and Patten, 2016; Knaak et al., 2014; United Nations High Commissioner for Human Rights, 2017). The lack of the use of comparison or control groups has been identified as a limitation of studies examining the impact of medical student anti-stigma and discrimination education programmes (Fernandez et al., 2016; Galletly and Burton, 2011; O’Connor et al., 2013). The studies which have utilised comparison or control groups to assess the impact of medical student anti-stigma and discrimination education in medical training have typically involved one-off interventions, which appear to have none or only a short-term impact on the improvement of attitudes (Friedrich et al., 2013; Kassam et al., 2011; Wechsler et al., 2020), as has been identified as an issue with anti-discrimination work more generally (Ashton et al., 2018).
In 2011, the Department of Psychological Medicine at University of Otago, Wellington, developed a service user-led, recovery-focused and contact-based education programme as part of their overall psychological medicine attachment, with the primary aim being to counter stigma and discrimination. Initial minimalist interventions were shown to have little impact (Gordon et al., 2014). In 2017, the programme (now referred to as the World of Difference) was significantly extended to encompass various interventions that facilitate multiple forms of favourable social contact, the promotion of recovery and respect for human rights. The present comparison cohorts study assesses the impact of this more extensive anti-stigma and discrimination programme.
Methodology
Participants and medical training programme
The participants were fifth- and sixth-year medical students undertaking their psychiatric attachments with the University of Otago (UO), New Zealand, medical programme in two centres: Christchurch and Wellington. UO delivers a comprehensive medical programme that spans 6 years. The final 3 years, advanced learning in medicine, are largely patient-facing with an increasing emphasis on an apprenticeship style of learning supported by didactic and small group teaching. Both centres provide psychiatric attachments that involve 5 weeks at fifth year and 4 weeks at sixth year, with approximately 100 students undertaking the attachments at each year. Attachments in both Wellington and Christchurch include a didactic teaching course with the majority of time spent seeing patients although the Senior Medical Officer supervisors and clinical experiences depend on individual placement. The major medical exam occurs at the end of fifth year, enabling a genuine apprenticeship style of learning to occur in the final ‘trainee intern’ or sixth year.
The programme
All students at the Wellington campus received the World of Difference programme (programme cohorts). The programme involves students at each year receiving a 6-hour workshop, a 1-day placement with a service user-led recovery-focused service, recommended readings, an optional tutorial, and a reflective assessment over the course of their psychiatric attachments. Woven throughout all aspects of the programme is a focus on Māori and Pacific worldviews and models of health (Newton-Howes et al., 2020). Details of each of the components of the programme are provided in Table 1. All aspects of the programme were mandatory apart from the tutorials, which were poorly attended.
Components of the World of Difference programmes at fifth and sixth years.
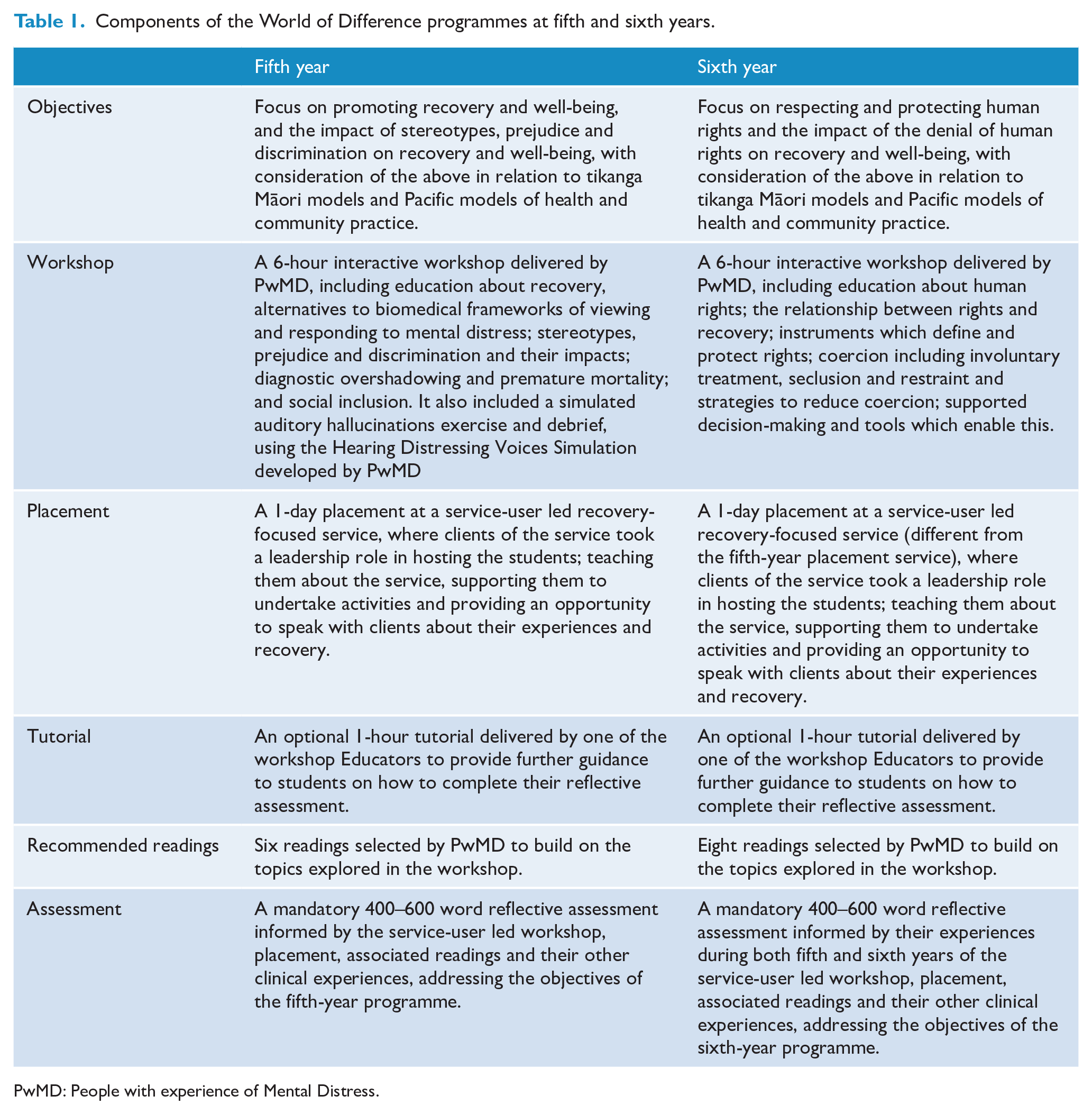
PwMD: People with experience of Mental Distress.
These two groups (fifth- and sixth-year programme cohorts) were compared to the equivalent groups of students who received the standard psychological medicine attachment, without the addition of the World of Difference programme, in Christchurch (control cohorts).
Measures
Two measures were used to examine attitudes. Both tools were initially developed to measure stigmatising/negative perspectives and therefore higher scores on both tools and in all domains indicate a more stigmatising/anti-recovery attitude.
The first measure used was the Recovery Attitudes Questionnaire (RAQ; Borkin et al., 2000), a 16-item validated self-report measure. Two domains, described as ‘recovery is possible and needs faith’ (factor 1) and ‘recovery is difficult and differs among people’ (factor 2), have been identified (Borkin et al., 2000). All items are measured using a 5-point Likert-type scale, with lower scores indicating a more positive attitude towards recovery.
The second measure used was the Opening Minds Stigma Scale for Health Care Providers (OMS-HC-20) (Kassam et al., 2012; Modgill et al., 2014). This peer-reviewed and validated measure aims to assess the degree of stigma in health care providers, including medical students. It contains 20 self-report items measured on a 5-point Likert-type scale covering three domains: attitudes of health care providers towards people with mental illness, disclosure/help-seeking and social distance. Lower scores indicate less stigmatising attitudes. It is sensitive to change, particularly in its attitudinal subscale, although overall changes are typically relatively small (Modgill et al., 2014). While the 20-item version is an acceptable measure for capturing health care provider stigma, additional examination of psychometric properties suggests that the 15-item version of the scale is superior to the full 20-item, particularly in terms of responsiveness to change (Modgill et al., 2014). For the purposes of comparing and contrasting previous studies that utilised only the OMS-20 (as will be reported elsewhere), the current study data collection and analysis was undertaken using both the 15- and 20-item versions.
Data collection
The study was approved by the University of Otago Human Ethics committee (D17, 386). Students were invited verbally to participate in the study by a member of the team and provided an information sheet on the project. Those willing to participate completed a written consent form. This occurred using the same system in both Christchurch and Wellington. Hard copy or electronic versions of the self-report measures were administered in person in a group format (e.g. during classes) twice for each group of students, at the beginning of the psychological medicine attachment (T1) and at the end of the attachment (T2) for each year. The students were asked to supply a code for anonymous matching of pre- and post-measures. This process was facilitated independently from the teaching, learning and assessment process to avoid any conflation of the two.
Statistical analysis
The primary null hypothesis examined in this study was that the addition of the World of Difference programme would not lead to any change in students’ attitudes towards PwMD. Changes between T1 and T2 within each of the cohorts for both fifth and sixth year were compared with Wilcoxon signed-rank tests. The changes between T1 and T2 of the programme and control cohorts were compared with Wilcoxon rank-sum tests for both fifth and sixth year. After assessing the overall scores, the factors of the two measures were also examined. Since the data was not consistent with a normal distribution, non-parametric analyses were most appropriate. The analysis was undertaken using the statistical package SAS v9.4 (SAS Institute Inc., 2013).
Results
All respondents who agreed and completed part or all of the questionnaires were entered into the analysis. This led to responses varying between 65 and 70 respondents for the fifth-year programme cohort (equating to 55–59% of the total cohort) and 50 and 55 respondents for the sixth-year programme cohort (equating to 43–47% of the total cohort). For the control cohorts, there were between 59 and 67 respondents for fifth year (equating to 56–63% of the total cohort) and between 46 and 51 respondents for sixth year (equating to 46–51% of the total cohort).
See Table 2 for all results. Both the fifth-year programme and control cohorts had similar median RAQ and OMS scores initially. Significant improvements towards recovery were found for both fifth- and sixth-year programme and control cohorts by the end of their psychological medicine attachments. For the programme cohorts, significant reductions in stigma were also found as measured by both the OMS-20 and the OMS-15. For the control cohorts, significant decreases in stigma were found as measured by the OMS-15 but not as measured by the OMS-HC-20 in fifth year; however, there were statistically significant improvements reflected in both by sixth year. Subdomain analysis provided a more nuanced picture. The fifth-year programme cohort showed significant changes in both the RAQ subdomains. There was also significant change for the OMS subdomain of ‘disclosure/help-seeking’, but no significant change in the OMS subdomains of ‘social distancing’ and the ‘stigmatising attitudes of health care providers’. The sixth-year programme cohort showed significant change for the RAQ subdomain of ‘recovery is possible and needs faith’, but no significant change in the subdomain of ‘recovery is difficult and differs among people’. For the OMS, significant changes were found for the subdomains of ‘attitudes of health care providers towards people with mental illness’ and ‘disclosure/help-seeking’ but not for the ‘social distancing’ subdomain of the OMS.
Pre-programme (T1) and post-programme (T2) attitude scores for fifth- and sixth-year programme and control cohorts and comparison between the two.
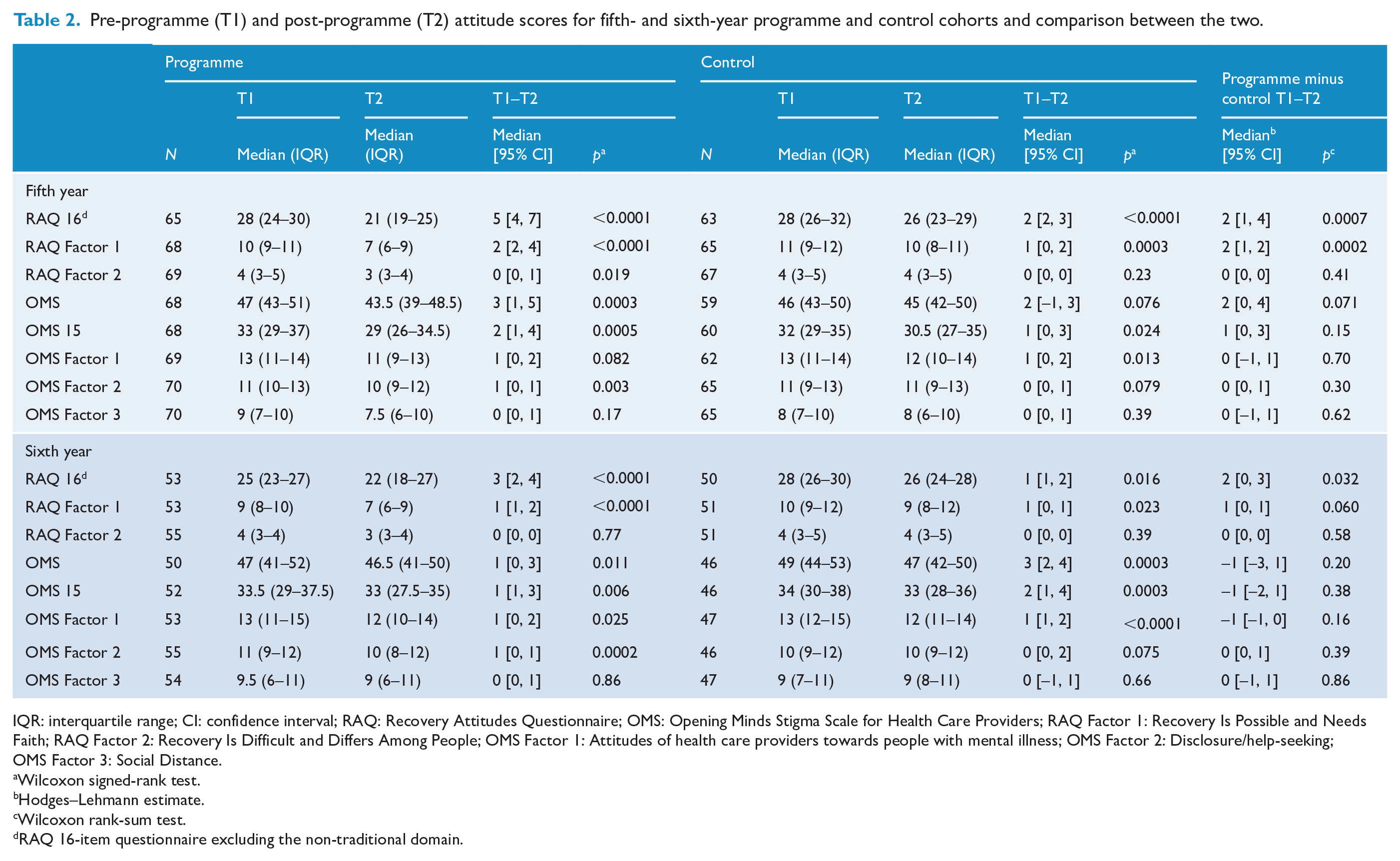
IQR: interquartile range; CI: confidence interval; RAQ: Recovery Attitudes Questionnaire; OMS: Opening Minds Stigma Scale for Health Care Providers; RAQ Factor 1: Recovery Is Possible and Needs Faith; RAQ Factor 2: Recovery Is Difficult and Differs Among People; OMS Factor 1: Attitudes of health care providers towards people with mental illness; OMS Factor 2: Disclosure/help-seeking; OMS Factor 3: Social Distance.
Wilcoxon signed-rank test.
Hodges–Lehmann estimate.
Wilcoxon rank-sum test.
RAQ 16-item questionnaire excluding the non-traditional domain.
Subdomain analysis of both control cohorts showed significant changes in the RAQ subdomain of ‘recovery is possible and needs faith’ but not in the subdomain of ‘recovery is difficult and differs among people’. Both control cohorts also showed significant change for the OMS subdomain of ‘attitudes of health care providers towards people with mental illness’ but no significant changes in the OMS subdomains of ‘social distancing’ and ‘disclosure/help-seeking’.
Statistically significant differences between programme and control cohorts were found for improvements in recovery attitudes at both fifth and sixth year. For fifth year, this appears to reflect large differences in the subdomain of the RAQ ‘recovery is possible and needs faith’. There were no significant differences found for any of the other RAQ subdomains at either fifth or sixth year. Overall changes in the Opening Minds Scale were not significantly different between the programme and control cohorts and no differences were highlighted on any of the subdomains of the OMS.
Discussion
The major finding of this study was that the inclusion of the service user-led World of Difference anti-stigma and discrimination programme was associated with a significantly greater improvement in medical students’ recovery attitudes than the standard psychological medical attachment. Both the intervention and study design serve to address current limitations in the literature. Unlike one-off interventions, the intervention included facilitating multiple forms of social contact, the promotion of recovery, and respect for human rights, being delivered across two years of the undergraduate medical teaching.
Of note, both cohorts experienced significant change in terms of more positive attitudes towards recovery of, and less stigmatising attitudes towards, people with lived experience of mental distress. In the control cohort, the fact that significant decreases in stigma were found as measured by the OMS-15 but not the OMS-HC-20 in fifth year probably reflects the former being more sensitive to change. The World of Difference programme intervention led to significantly greater improvement than the standard attachment in terms of more positive attitudes towards recovery, particularly in terms of the concept that recovery is possible and needs faith. As promotion of recovery is one of the most effective characteristics of successful anti-stigma and discrimination programmes (Knaak et al., 2014), it is somewhat surprising that the significant difference between the cohorts in relation to recovery did not translate into stigma reduction. There are two possible reasons for this discrepancy. One is that factors associated with the measure and the methodology used for the study, and the interplay between the two, were at issue (e.g. lack of sensitivity to change, ceiling effects, change discrepancy, study being underpowered). However, the fact that significant changes within the cohorts were observed suggests that these were not the reason for the discrepancy. The other possible reason for the discrepancy concerns the impact of other aspects of the overall attachment. Students may experience a form of cognitive dissonance and the apparent need to have to choose between what they perceive as two ‘contradictory’ perspectives and approaches (those promoted through the World of Difference programme and those promoted through the other teaching and clinical placements associated with the overall attachment). This seems to be a particular issue in relation to the human rights focus in sixth year. The lack of systematic training and awareness raising for healthcare providers on human rights is considered to allow stigma and discrimination to continue in health settings (United Nations High Commissioner for Human Rights, 2017). However, it is questionable as to whether human rights teaching can contribute to reducing stigma and discrimination when the delivery of services is potentially antithetical to what is being proposed in terms of service orientation to become compliant with international human rights obligations. This form of epistemic injustice is problematic throughout medical student teaching.
One of the most concerning findings of this work is that neither the programme nor the control cohorts had a significant impact on the OMS subdomain of ‘social distancing’ which refers to one’s desire to maintain distance from people with mental illness (Kassam et al., 2012). Arguably, this would be most impacted by favourable social contact. Despite the World of Difference programme facilitating multiple forms of such contact, it is possibly still not extensive enough to counteract the continued dominance and impact of engagement with patients of inpatient wards, which ‘… seems to reinforce the beliefs of chronicity and incurability of mental illnesses such as schizophrenia’ (Luigi et al., 2020: 6). While the students involved in this study were different at each year level for both the programme and control cohorts (e.g. not the same group of students tracked over years), as fifth-year students, the sixth-year cohort students did engage in the same programme as the fifth-year cohort students, in the year prior. Hence, it is interesting to note that for both the programme and control cohorts, the scores for both the RAQ and the OMS-HC were better at the end of fifth year than the beginning of sixth year. This suggests reductions in efficacy over time, as occurs in response to less intensive interventions. What is needed therefore is the tracking of students in response to interventions delivered over time to determine if repeated teaching over years is required.
Limitations of the study include its non-randomised design; however, such a design is not feasible due to the manner in which medical programmes are delivered. Rather this is real-world implementation research. Demographic data were not collected so we were unable to assess any difference between the groups in this respect. However, there is no reason to think there are any systematic differences between the groups that would impact on the area of interest. Furthermore, not all students participated and some students completed only part of the questionnaires. This may have biased the data, if, for example, students with improved attitudes were more likely to respond. Unfortunately, this study did not involve any follow-up to assess if improvements were sustained beyond the short term, in contrast to other less intensive interventions. Furthermore, it would be valuable to assess the impact of the individual components of the programme and particularly those novel elements such as the placements and assessment. While that is not feasible utilising the method of attitude assessment employed through this study, as it would place an undue burden on students, other approaches to evaluating the impact of these individual elements are currently underway.
Conclusion
The psychological medicine attachment encompassing the comprehensive service user-led World of Difference anti-stigma and discrimination programme was found to be superior to a standard psychological medicine attachment in terms of supporting more positive attitudes towards recovery. Programmes such as this, or this programme, should be considered for inclusion into medical school training as a component of psychological medicine attachments on the basis of their face value and evidence of improvements in student attitudes, particularly in relation to recovery, the support of which is an expectation of international and national mental health plans and policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by funding received from the Health Promotion Agency (grant number 6192).