
Abstract
In 2009, the newly elected FMLN government of El Salvador launched a comprehensive health reform, which gave the National Health Forum (NHF) a key role in developing community participation. This study aims to examine and analyze the content and impact of this social movement during the study period 2009–2018. The context was analyzed through relevant documents, which helped identify key stakeholders. Semi-structured interviews took place at 3 levels of decision making: the political level, the health professionals, and the community. Data were analyzed using a qualitative methodology. Participation is carried by a structure created by the Ministry of Health, the National Health Forum. The NHF developed 3 strategies: (1) leadership building in the communities through the strengthening of social, political, and economic skills, where they developed social accountability mechanisms at all decision-making levels of the health system; (2) the strategy carried by the sectoral working groups, where they responded to prioritized needs identified by the community; and (3) advocacy for human rights-based policies. The NHF, and its role in the strengthening of the National Public Health System, provides strong evidence of community participation strategies and co-governance with the health system within the social determinants of health scope.
Keywords
Background
Rationale of Social Participation in Health
Participation in health is a key concept that involves engagement with communities, or members of communities, in strategies for health service development and for community interventions. The principle underlying this approach is that health interventions will be more responsive to participants’ needs – and consequently more effective – if they incorporate stakeholders’ views. 1 The primary health care (PHC) paradigm was a key concept of the Alma Ata Declaration. 2 Thirty years after the Ottawa Charter, 3 empowered communities are more than ever considered essential for health promotion.
In 2008, the report “Closing the Gap in a Generation” of the WHO Commission on Social Determinants of Health, 4 critically analyzed the important impact of the social, political, and economic contexts on health. It highlights the relationship between socioeconomic status and health outcomes, strongly advocates for adequate community interventions, and underlines the need for social and economic change. In addition, there is a growing interest in how socioeconomic conditions contribute to health disparities, including poverty, inadequate educational opportunities, unemployment, limited access to basic services and goods such as nutritional foods, and poorer quality health care. 5 One approach to reducing health disparities has been to mobilize community representatives of target populations to work collaboratively with multisector public and private organizations to identify common health issues, develop program or policy interventions, and attempt to bring about community-level change that supports health-promoting opportunities and behaviors. 6
Nevertheless, contradictory practices exist, which vary from extremely utilitarian (for example, in relation to the role of community health workers, where the system takes advantage of the community-based skills to put health programs in practice) to empowerment approaches that enable communities, families, or individuals to make decisions on their own lives. Over time, recognition of these differences and of the importance of empowering strategies have increased.7,8 In addition, it is recognized that improved levels of health are achieved through a PHC-based health policy that includes universal financial coverage regulated or overseen by the government, equitable distribution of resources, integrated services, and zero or low co-pays for services at the first level of care. 9
In September 2003, during the 44th Directing Council, PAHO/WHO approved the resolution CD44.R6, inviting member states to a series of recommendations to strengthen PHC in their report “Renewing Primary Health Care in the Americas.” 10 After a long period of repression in El Salvador, the newly elected leftist government, FMLN, incorporated these guidelines to formulate the Health Reform in 2010, giving special emphasis to the following principles: responding to the health needs of the population, orientation toward quality, responsibility and accountability of governments, social justice, sustainability, participation, and intersectoriality. The reform’s design is based on PHC and its values, since it is made up of a set of essential structural and functional elements that guarantee coverage and universal access to services, which are acceptable to the population and promote equity; provide comprehensive, integrated, and appropriate care over time; emphasize prevention and promotion; and take families and communities as a basis for planning and action.9,11 Hence, a central strategy of the health reform was to enable participation,11,12 meaning participation turns individuals into active partners in decision making about the allocation and use of resources, in the definition of priorities, and in the guarantee of accountability.
El Salvador and Its National Public Health System
The history of El Salvador has been characterized by abysmal inequalities in the management of social relations and power imbalance. In the 1970s, the country was under a strong military repression and ranked among the 5 most unhealthy countries. 13 The doctor-to-patient ratio was the lowest in Latin America. Eighty percent of rural peasants had no potable water, and 60% had no access to health services. When civil war broke out in 1980, the health budget had already been cut by 50%, and the health ministry completely pulled out of many regions, so that funds could be allocated to military. Life expectancy fell from an already dismal 56 years to 50.7 years, with 3 out of 4 children suffering malnutrition, and a mortality rate of 87 per 1,000 for children under 5. 14
Later, during the war, the health system was totally decommissioned, and FMLN guerrilleros forces trained lay health workers in rebel-controlled areas where the Ministry of Health had closed clinics in the early 1980s.12,13 The resistance organizations collected the accumulated knowledge of rural social organizations to consolidate this “alternative” health system. Self-managed health structures were created, mainly run by health promoters or trained voluntary health workers from solidarity groups. The communities proposed these promoters themselves: they chose people who could read and write, who had leadership abilities, and who had a commitment to their community, hence strong organization skills were learned from that.12,15 Also, during this war period, there were many forced displacements, terrible massacres and abductions, and many social groups fled to neighboring countries, mainly Honduras. These migrations led to the creation of refugee camps. The refugees organized themselves in different areas of work, including ensuring a clean water supply, food production, health, education, and security. Consequently, different types of organizations and decision-making mechanisms were created, including general assemblies and meetings between sector and area coordinators.
12
These structures and procedures were maintained and refined after the refugees returned to El Salvador. The communities generated many organizational mechanisms during the civil war. These resources were developed before and during the conflict. After the peace agreements the organizational mechanisms were activated in the struggle for access to medicines, against the privatization of public entities, all of them were important […] – Vice-minister of public health policies
The end of the 1990s saw the growth of a movement for neoliberal reforms in Latin America, 17 which in El Salvador mobilized health personnel, trade unions, and the general population to go on strike and take to the streets in demonstrations and white-coat marches, forcing negotiation with the government to halt initiatives toward privatization.9,10,17 In 1999, the social movement led to the creation of the Council on Health Sector Reform (Consejo de Reforma del Sector Salud – CRSS), which was entrusted with reforming the sector in consultation with a group of public and private institutions. The council concluded that the Salvadoran health system had adopted a centrist model that excluded much of the population and constrained the democratic exercise of decision making. 18 In parallel, new spaces of social expression were born, such as the Citizen Alliance against the Privatization of Health advocating for policies aimed at achieving greater equality and universal access to health services. They promoted the idea of conceiving health as a public asset, a fundamental human right, and the result of a dynamic interaction between a range of different determinants (socioeconomic, political, biological, cultural, demographic, and environmental).11,19
In 2009, the FMLN – the former guerrilla movement turned into a left-wing political party – won the national elections. They immediately launched a national health system reform.11,19 In 2010, the Ministry of Health (MoH) introduced a health system reform, based on more than a decade of discussions and debates between different sectors, focusing on people-centered care and the right to health, and launched the health policy “Building Hope.” 19
The development of a national public health system based on primary health care principles was a central priority for the new government. The Ministry of Health explicitly committed itself to the right to health for all Salvadorans, ensuring free health care in the public system by eliminating co-pays in the health services to reduce economic barriers, as out-of-pocket expenditures by Salvadoran households represented 87% of total private spending on health (34% of national expenditure) in 2010. 20 The primary health care concept was not limited to “well organized first line services,” but referred to an integrating approach for the whole national health system. Frontline care was dramatically expanded, improving the health coverage in the poorest municipalities, with the introduction of community family health teams (equipos comunitarios de salud familiar – ECOSFs). In addition, a reconfiguration of the management model through the creation of comprehensive, integrated service networks (redes integrales e integradas de servicios de salud – RIIS) 21 made it possible to reorganize the services and improve the coordination between the first and second level of care. Health prevention and promotion strategies were established through intersectoral initiatives coordinated by the Intersectoral Health Commission (CISALUD) to ensure a comprehensive approach under a “health in all policies” scope. 22
One of the main strategies of the health reform focuses on the promotion of social and community participation.
19
From the very outset, we knew that in order to achieve this vision and these objectives,
10
we would need to strengthen both community organizations and social participation, so that society would be able to both take part in the decision-making process, and identify and successfully tackle the determinants of health. – Ma Isabel Rodríguez, Minister of Health 2009–2014
The National Health Forum
Background
The National Health Forum (NHF) was formally created in 2010, with 3 fundamental objectives:
To build people’s power and strengthen the organizational fabric To face the mercantile nature of health of the previous neoliberal governments To stimulate and promote an effective social participation in health
As mentioned earlier, the organizational and decision-making structures and the high levels of social participation from the years of the war were maintained and collectively strengthened during the period following the signature of the peace agreements. These existing social structures and participatory processes have served as the starting point for the creation of the NHF. During the process of formulating the health reform in 2009, many of these organizations, including the Citizen Alliance against the Privatization of Health (ACCPS), were encouraged to take part in “Open Social Dialogue tables” (discussion panels that were established to include civil society in the design of the health reform 19 ) to channel proposals and recommendations to be included in the new health policy.9,11,19,23 This commitment is recorded in the policy document “Building Hope” 19 : “The participatory process already begun will have immediate continuity with the creation of a National Health Forum, which formulates the elements and contribution to the taking of the fundamental decisions for the construction of the new health system.”
The National Health Forum was therefore a space for civil society participation in the health decision-making process, with a legal basis independent of the Salvadoran Health Ministry, that allows the National Health System of El Salvador to advance within the social justice model proposed by the new health reform. It’s constitution is embodied in the strategic consideration that “health is a collective task in which everyone takes part.”
24
Their legal support is guaranteed through different official publication documents, including these 2 main ones:
Legislative Agreement No. 126, published in the Republic Official Gazette No. 33. February 17, 2010, in which the National Health Policy is approved and indicates the formation of the National Health Forum (NHF) as part of the process of reform. Agreement No. 1422 of the Republic Official Gazette, volume 413, number 182, dated October 3, 2016, which recognizes the National Health Policy 2015–2019 and where the NHF constitutes the fifth axis of the fourth strategy: Deepening and expanding the Strategic Axes of the Health Reform.
The NHF has succeeded in developing consensus on a strategic decision-making process that emphasizes equity, quality, and inclusion, as well as an intersectoral approach based on the social determinants of health through a broad process of proactive and vigilant citizen participation within the framework of exercising the right to health.
Governance and Decision Making Within the NHF
During the first months since the health reform was launched and the structure of the NHF was formulated, various community organizations participated in this policy formulation. The organizations detailed in the NHF’s website (https://fnssv.com) are those that conformed and continue to be part of the NHF; and, the civil society elected members of these organizations as leaders of the NHF for their extensive expertise in community participation in health. This is the case of the director of the NHF, who was a member of APROCSAL – Association of Salvadoran Community Promoters. APROCSAL is an institution with a critical and purposeful sense, dedicating its work and effort to be a health reference based on the promotion, organization, citizen participation, and alternative use of natural medicine, which provides and demands a comprehensive health care alternative with a human rights approach within the reach of the most vulnerable population, with an emphasis on women and youth, to contribute to the improvement of their living conditions with gender equity. When the NHF was being established, the minister of health at the time, Ma Isabel Rodriguez, proposed Margarita Posada, a member of APROCSAL, as coordinator of the organization and creation process of NHF due to her work with the communities as well as her expertise in community participation strategies; and her position as NHF’s director was ratified by the civil society during the NHF’s first assembly. 24 Each of the coordinators at the different levels are appointed periodically (normally every year) by membership consultation in the different territories. At the community level and working with the community health units, community coordinators are in charge of assessing the health needs and follow-up and support of the health policies implemented.
The organizational structure of the NHF is detailed in Figure 1 and follows a parallel organizational structure as the MoH (white boxes). 22
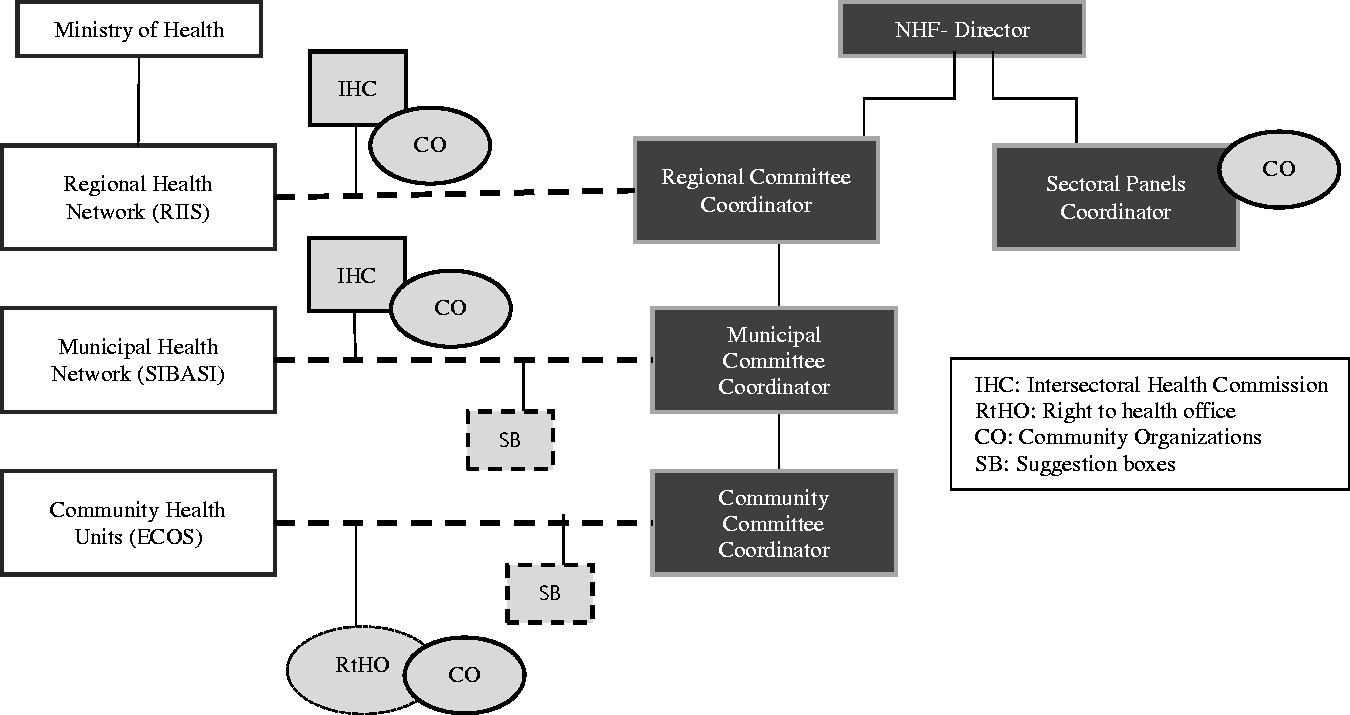
Scheme of the organizational structure of the National Health Forum (grey boxes) and the Ministry of Health (white boxes).
There are 4 levels of decision making:
Community level: Both the MoH and NHF have committees where strategic actions are developed to respond to community needs. At this level and within each community health unit are “right to health offices,” where both institutions engage along with other stakeholders such community organizations and civil societies. The main function of this offices is to address accountability issues such as shortage of medication, quality of care, and human rights. At this level are also “suggestion boxes” where civilians can express their claims. Municipal level: This level includes hospitals (second and third level) where they meet monthly at the Intersectoral Health Commission (IHC) with other stakeholders, such as the NHF and community organizations. Issues discussed include coordination with the other levels of decision making, implementation of strategic plans, the comprehensive epidemiological vigilance, and compliance with certain statements such as the participatory law. Suggestion boxes have been placed at health structures at this level. Regional level: 4 regional health structures are represented at each of the 4 regions of the country. At the IHC matters discussed at lower levels of decision making are addressed and used to inform policymaking. National level: The Ministry of Health is divided in 2 departments: Vice-Ministry of Health Policies and Vice-Ministry of Health Services. The Vice-Ministry of Health Policies ensure that policy formulation with different stakeholders is being developed and the NHF has a role of “social comptrollership” so that policies are issued with a human right basis.”
Within the NHF, different decisions are prioritized and moved to higher levels of decision making, to the municipal and departmental committees, which in turn collect issues at their level of decision making and formulate recommendations to be discussed at the health assemblies held annually. Within the sectoral organization, the coordinators are selected based on their experience, with the panel’s thematic and thorough membership consultation. The coordinator changes every 2 years, and the same person can be elected.
Therefore, within the membership of the NHF is a technical workforce composed of members of different community organizations and associations, which are in charge of supporting the training, organizational skills, and economic sustainability of the NHF, and an operational workforce composed of leaders of the communities or any person from the civil society who participates in the NHF, which are the ones responsible for implementing the different activities carried out by the NHF (this will be detailed in the following sections).
The NHF is part of an international global network, People’s Health Movement (PHM, https://phmovement.org), bringing together grassroots health activists, civil society organizations, and academic institutions from around the world, which acknowledge that popular pressure from civil society is essential to ensure the necessary action by the state on social determinants. PHM works on various programs and activities and is committed to comprehensive primary health care and addressing the social, environmental, and economic determinants of health.
This article aims to discuss the social and community participation approach with the example of the National Health Forum (NHF) in El Salvador since the implementation of the health reform up to now; therefore, the study period covered is from 2009 to 2018. We describe the community empowerment experience resulting from the comprehensive PHC reform launched in El Salvador in 2009. We describe the development of a participation initiative that evolves to a long-established social movement. We identify the key elements of the NHF’s strategy to enable community participation and empowerment in health decision making, within the health reform context in El Salvador.
Methods
The study is a descriptive case study, using qualitative methods. We first conducted a document analysis to gather information on the context of El Salvador. We searched PubMed to identify epidemiological data and community participation strategies. Our search strategy was (“Community Health Services” [MeSH]) OR “Community Participation” [MeSH]) AND El Salvador [tiab]. We retrieved 91 articles, of which 8 were full-text reviewed. We identified 3 relevant studies from the included reference list. We developed a second search in Google Academy to identify any kind of document which described the functioning of the Salvadoran health system or community health interventions during the civil war, as those reporting during and after the health reform: 20 references were included. Once identified and contacted with key stakeholders, they shared with us other relevant documents to be able to have a complete understanding of the context in El Salvador. This phase was conducted during November 2017–February 2018.
During 2 field visits in February and June 2018, we conducted semi-structured interviews with key stakeholders, for which we followed a purposive sampling methodology by selecting participants that had been identified through the document analysis, or referred to by the Ministry of Health and the NHF. The inclusion criteria related to participants of the 3 levels of decision making: the political level, the health professionals, and the community, which have collaborated with the NHF in the design or implementation of health strategies or are active members of the NHF during the study period. Interviews followed a predefined deductive thematic framework: (1) social understanding of community participation; (2) description of the NHF, its role within the health system, and strategic actions. This was developed through the application of a reflexive approach and the triangulation of data.
Data collection: 3 interviewers conducted 10 interviews during fieldwork: 3 members from the NHF; 2 cadres of the Vice-Ministry of Public Health Policies; one primary health care unit coordinator; one frontline professional; and 3 community leaders. Participants were encouraged to speak freely and allowed to lead the interview in the direction they found most interesting and important. Interviews lasted from 30 to 60 minutes and were recorded with participants’ written informed consent. The participants were free to leave at any time of the interview. After transcribing the content of audio-recorded interviews, data was coded using Nvivo® version 10 and then analyzed.
Ethical standards were compliant with those set by the National Health Ethics Committee of El Salvador (CNEIS/2018/005_A). This study is part of a wider research on El Salvador’s National Health System (protocol approved by the NIHR Global Health Research Programme 16/136/100, Queen Margaret University, UK).
Results
What Is Understood by Community Participation?
Community participation is conceived as a mechanism for change, an empowerment process with transforming capacity. The NHF, as a social movement, pursues a well-organized and non-instrumentalized, non-utilitarian participation that plays a role in decision making and generates ownership. As the vice-minister of public health policies details: The participation that is implemented is linked to the concept that was raised in Alma Ata, as one of the basic strategies of primary health care. We understand participation as meaningful participation, participation that is neither utilitarian nor an object of manipulation. It is a citizen participation – through its community organizations and its community leadership – in the formulation of public policies and in the exercise of social control on the performance of the national health system. – Vice-minister of public health policies The social movement in its struggle. Those were the people who organize themselves to generate change. When people are aware of their rights, they organize and participate in the NHF, in a significant way, and not – as in the past – in a type of instrumentalized participation by the Ministry of Health. In this way, real change is generated. – Director of the NHF Participation is a power exercise, because those who hold the power must give up part of it. If you want everyone to participate in the decisions and democratize the health facilities, you have to give up power. But also, the population must learn to take advantage of that opening. – Director of the NHF
Social determinants of health versus social determination of health
The primary health care concept promotes actions to tackle health inequalities. In this sense, the Salvadoran approach is not based on the (dominant) focus on “social determinants of health”4,25 but on the Latin-American concept of “social determination of health.”7,25 The vice-minister of public health policies clarifies: The concept of “social determinants of health” has the disadvantage of splitting up the reality in separate parts, while the “social determination of health” integrates these as a whole, giving importance to the collective determination over free will and individual life styles. – Vice-minister of public health policies The change of government and entry of the FMLN facilitated the health reform. I come from social medicine, and I have a commitment to work with the community in the health process. Ma Isabel Rodríguez, Minister of Health 2009–2014 It is important that the community knows that health is determined socially because that makes links to other struggles; struggles for problems that are generating a sick society, not only in our country, but also globally. – Director of the NHF A determination-based approach allows us to see that we cannot solve problems in isolation: they are related to the country’s production model, to decisions related to the population’s working conditions. Depending on how people work, that is how they will become ill. If we don’t question that, we will continue operating in the logic of covering gaps rather than going deeper into the model, and we won’t go very far. – Member of the NHF The right to health is not only the access to health care. It is a broader concept, including access to drinking water, an agriculture free of pesticides, uncontaminated air, etc. – Territorial development facilitator (member of the NHF) The Salvadoran population does not have a culture of participation, due to years of repression and armed conflict, where people exercising their right to participate run the risk of losing their lives. People tended not to participate […] but when communities perceive improvements through their participation, they are encouraged to continue […] I think they do it because they are empowered, they see changes and improvements in their living conditions, in their family, and in the community. – Member of the NHF Nowadays, the issue of social violence is limiting participation because of the violence generated in the territories. These youth gangs that control the territories are closing many community spaces, because they see it as a threat to them. – Territorial development facilitator (member of the NHF) There is a difference between living in residential blocks and living in a neighborhood, because of the issue of social violence. For instance, I was threatened because of the work I did in the community. – Community leader
The National Health Forum
The National Health Forum (NHF) was created in 2010, within the framework of the health reform. The NHF pursues civil society consensus in strategic decision making, through a broad process of citizen participation under a social justice lens. Moreover, it fulfills the role of accountability within the health system, for which it developed parallel structures with the health system structures. The FNS, as a community structure, in alliance with many other actors, has developed capacities that health professionals do not have. They see beyond the health services, looking for more fundamental solutions to health problems. These are not limited to curative aspects. This stimulated a wider organization of society, bringing together other organizations that are not focused on the right to health. For example, the demand for justice, and people’s mobilizations for demands that are much broader than the health sector, such as mobilization against tax evasion and avoidance, in order to be able to finance stronger public services and funds for education and health. – Vice-minister of public health policies The FNS was born with high participation of different social movements, all united in the same direction. There were a series of problems, as they wanted to privatize health care […] The NHF was created when the health reform came into being. We, the NHF, are part of the reform, we are working in the reform to ensure participation. – NHF member Only with an active participation in health we will be able to consolidate a comprehensive health reform. – Vice-minister of public health policies
Role of the NHF in the health systems’ policymaking process
The NHF aims to build the capacity of social movements to interact with local government in the process of policymaking, thereby promoting a shared local governance (Figure 1), which underscores the move toward participatory processes of public policy making and devolves influence and power to local communities. The NHF facilitates the possibility that all health demands identified through their network of community health centers, including those of other frontline health professionals, are addressed in the political agenda. These demands permit the formulation of integrated, settings-based approaches that best respond to their needs, enabling people to increase control over and improve their health, following health promotion strategies. The communities that are more organized, or which are better supported by the NHF, are the ones that participate most in health campaigns, such as child vaccination, feline and canine vaccination, and dengue prevention. When the NHF is present, the population is well organized, you will notice, and everyone knows what their responsibility is. For example, to avoid mosquitoes, they already know that water containers must be covered and that this is the population’s responsibility […]. The NHF, which is very influential in communities and in health committees, makes the population aware of the fact that health is everyone’s responsibility, not only the ministry’s responsibility. And that health is not only about coming for a cure but should be more preventive. That’s where the NHF is helping a lot. – Coordinator of a primary health care unit All populations have knowledge and are essential in a process of reform. Sometimes the knowledge that communities have about health issues is underestimated. At the territorial level they are discussed through the discussion tables, and territorial trainings are held to open the debate on certain topics […] undoubtedly, people are the ones who know most about their reality, so you start to see how they incorporate all the concepts of the right to health into their reality and that is when you see changes and improvements. – Director of the NHF In order to get closer to youth, initiatives are set up directly with groups of adolescents, in schools or through the radio – many young people listen to the radio – and there they receive radio spots where they are given information. Health is specifically promoted. We also reach vulnerable populations through announcements on TV, and in the same way, people who come to the health units also have the opportunity to attend the health assembly we organize. Also, during parent meetings at the schools, there are opportunities that one takes advantage of. We also get closer during the social mobilizations that are held at the mayor’s office, or by visiting agricultural cooperatives related to chronic kidney disease. Where the NHF is, we have a closer and more effective way of working with the communities. – Frontline health professional The NHF also has a large and productive interaction with the community health teams and the community health units, which, although they initially rejected the NHF, today they recognize its importance. There are clear improvements in the places where the NHF operates, compared to the places where they are not yet present. – Vice-minister of public health policies The NHF has developed capacities that health personnel do not have, such as looking beyond health services to find more essential solutions to health problems. – Vice-minister of public health policies Due to the National Health System’s inability to respond to population needs, community members began to organize and demand their right to health. When the reform process began, the idea was proposed to stimulate the development of a community organization that mobilizes for the right to health, and this is when the NHF was launched. – Vice-minister of public health policies The NHF was created to generate a space for community participation and took advantage of the political opening given by the FMLN government. The population was massively involved against the privatization proposals for health care. That is where many of the organizations came together. We took the opportunity to create that space, the NHF. – Director of the NHF
Action strategies followed by the NHF
Territorial level
In June 2017, the NHF had 750 community committees in 82 municipalities throughout the country, within 12 of the 14 departments. 22 The territorial work is at the center of its activities. This territorial action seeks to generate an organizational fabric that strengthens the analysis of the social determination of health and contributes to generate health policies that reflect the concerns and realities of the communities and the population. The objective of this process is to provide or co-create knowledge, skills, tools, and resources to monitor the development of the health reform. Community leadership structures have been built up for this purpose. The NHS is organized at the level of the community, the municipality, the department, the region, and finally the nation.
Accountability mechanisms are one of the most essential elements the NHF is working on, in coordination with the health networks of the Ministry of Health. The objective is to supervise and evaluate the correct functioning of the health care system. This happens through (1) social control, through the offices of the right to health that exist in most of the health structures, (2) assessment of the service delivery, (3) evaluation of the quality and warmth of health care, (4) control of the supply of medicines, and (5) an overall evaluation of the health care offered.
Finally, suggestion boxes exist in most establishments, where people can propose improvements or criticize shortcomings in health care. The NHF is the key holder for these boxes (volunteers wielding this task are democratically elected within the community), which are opened periodically and discussed with the management of the establishment. Feedback is given to the health coordinators of these units and hospitals.
In 2018, this social control was functioning in 24 national hospitals and in 5 health regions. Since its opening, 6,708 applications have been considered and addressed appropriately.
23
Before, there was no regulation on how decisions were made and which decisions were made. We had to decide if we wanted to collaborate with the public institutions, to ensure a participation in decision making and monitoring of health services. This participation is not for individual interest but for the collective community. It is a meaningful participation that really brings benefits to the community. – Coordinator of an NHF working group Sometimes, health personnel have a technical training but do not give adequate treatment to people, (…) putting a mailbox made them very angry, it’s like the nurses do not agree with the mailboxes. (…) Nurses know already what people think and, therefore, do not agree with the mailboxes. – Community member Our work is complementary, because the MoH does the healing part and they see the patients and all that, but we do the knowledge part, the awareness, the promotion, the supervision. We say we follow the complaints that live in this town (…) so, for us it is important to know their work, to see how we can support, but also in what way we can do what is right. That is our role. – Facilitator on the territorial development (member of the NHF)
The NHF is training community leaders for the combined purposes of organizing participation and supervising health practices and services. These leaders serve as a bridge between the community and remove decision makers, channeling bottom-up participation. At the community level, differences are reported between territories. The NHF director points out that this flexible way of working is necessary for a social movement to grow, always placing communities’ perspectives at the center: The forum is a process under construction, and any social movement is changing in every way, in terms of agenda, in terms of stakeholders. A social movement cannot have a rigid structure, in any sense. The NHF has community leadership. People feel proud of belonging to the NHF. That motivates people to participate and to strengthen their networks. For example, for the day of the elderly, several communities come together to make a joint celebration. – Director of the NHF First of all, what keeps me here is the satisfaction of helping others, then the amount of knowledge that has been given to us and that we can replicate in the communities, where now more and more women know their rights and what types of violence exist. – Community leader People’s commitment is what ensures continuity, because they don’t get paid, nor do they have a management position. We are teammates who try to guarantee the right to health and that is our struggle. Perhaps, their commitment is what ensures that it works. – Member of the NHF
Sectoral level
The NHF has developed a broad structure within society where different institutions, organizations, and individuals converge in the movement for the right to health. The NHF has stimulated a wider organization of society, which brings together other organizations that are not focused on the right to health, but for example in the demand for justice, or on the electoral issue. It has stimulated organizations that have made broader demands, for example, the demand against tax evasion and avoidance. To have more public funds for social health programs. […] There are factors that cause the population to get sick and die, but the NHF has gone further, has gone to the fundamental causes that explain what makes the population sick, […] is demanding changes in the environment policies. And it demands greater participation in the development of health laws, according to its rising level of empowerment and fundamental interest to participate in health policies. – Vice-minister of public health policies
At the same time, through the reform, the health system started an intersectoral line of action that gathers different key actors in a shared space: the NHF as the community voice, governmental sectors as education, and the nongovernmental sector with community organizations and NGOs. That part that I told you about being organized is intersectoral, because the mayor’s office participates, the church participates, some community leaders participate, the health establishment, and on some occasions education, the police, the house of culture, (…) So that helps us to solve some situations, for example, if we have a pregnant adolescent who went to school, we talk to the director, and we say “look here we have to do more to avoid teen pregnancy,” and then we organize an activity with the school. – Coordinator of a health care unit
Advocacy
A last pillar, but not the least, is the advocacy work of the NHF on public policies in defense of the human right to health. Advocacy refers to what is linked to the exercise of power in a society, to the redistribution of power. This definition implies that the community should have the power to ensure an equitable share of health resources: We are focused on participating in a meaningful way, bringing benefits to our community, oversight and control of the resources where they are provided. This doesn’t imply that things are given to us, but that we, as citizens, also contribute to those institutional resources that are assigned to answer the needs of the population. A conscious and critical participation, a participation that has the aim to improve the living conditions of the population and bringing changes to our country. – NHF thematic group coordinator When the NHF calls to a concentration, or something massive in San Salvador, we all come together and, as we say, we are many, so that helps to strengthen the processes. – Facilitator on the territorial development (member of the NHF) When people are trained and given the space to debate, people mobilize and organize for the struggle to guarantee fundamental rights. – Coordinator of the sexual and reproductive health working group (member of the NHF) One of our limitations is that we do not measure the impact of our participation, what we have achieved – for example, that the national health reform is widely known. Also, we should assess how we have implemented our work and identify areas for improvement. We made advances in the culture of participation, also in supporting the implementation of health reform, and in changing the people’s mentality from a medicalized culture to a health (approach) that really guarantees a better life. To see it as something positive and something that has to do with all policies, and all those things that affect the communities in the territories. – Member of the NHF
From that moment on, the population mobilized, led by the NHF, for the approval of the drug law. In 2012, the drug law was approved thanks to citizen advocacy as expressed by the vice-minister of public health policies: For the approval of the drug law, the NHF had a much greater presence than that of the health personnel, and led the citizen pressure which permitted its approval.
To this day, many interests are still linked to pharmaceutical companies, which is why the NHF, through its pharmaceutical sectorial panel, remains vigilant to ensure access to essential medicines. As described by the leader of the NHF pharmaceutical sectorial panel: The process of regulating the drug culminates with the law in 2012, but for everything to happen, a whole process of pressure was necessary. Before there were some health tables and from there, not only the health reform was born but the issue of medicines was also raised. The NHF prioritized this issue and mobilized its forces, and we managed to eliminate many of the barriers to access essential medication. Now, we make a permanent evaluation that allows us to identify several things: periodically we meet with the general direction of medicines (MoH) so they can tell us what the advances are, and we can comment on the problems we have identified in the territory; in this way we are able to find common solutions. But, we are also responsible following their accountability, who forms part of the board, if they are following the quality protocols the law establishes. In parallel we work with the community. The main mandate of our working group is that we must work to make the community aware of what the right to medicines is, because the population does not have a clear idea of this, they don’t get taught this elsewhere, so we generate that knowledge in the communities, because knowing that we have that right makes us do things so that this right is fulfilled. – Coordinator of the pharmaceutical working group (member of the NHF)
In an impoverished state, small farmers cannot adequately prevent occupational risk factors. They are driven to use cheap synthetic pesticides, as these maximize their crop yield at a minimal cost. Many who work in farmer cooperatives for limited periods tend to overwork, as their income depends on volume of daily production, which causes them to neglect rehydration pauses, if they are even allowed to take them by their crew captains. Their regular diet is poor in essential nutrients. Use of unprescribed analgesics and alcohol abuse to kill pain from strenuous physical labor is widespread within this population group. With limited financial resources, many do not invest in necessary protective equipment while exposed to highly toxic pesticides. Nor do they use health services on a regular basis. All these factors combined can weaken the body’s immunological system and, therefore, overexpose them to health risks in their surrounding environment. Furthermore, study participants shared a sense that, while government disinvestment in rural areas is evident, the activities of large agrochemical corporations are in continuous expansion. These stark differences in economic outcomes between different sectors in society have generated a collective sense of injustice within rural communities, due to the perception of an existing collusion between government and large corporate interests. 26
Hence, this disease is an expression of inequities derived from a highly exclusive and inequitable socioeconomic model of development and consumption. It constitutes very high cost health problems at the individual and family level as well as at the health system level. Recognizing these consequences and with a social determination approach to the problem, it is essential that the plans for the comprehensive care of CKD include an analysis of the health disease process tending to influence the entire process, not only on the final effects at the individual level. Therefore, the strategies have to transcend the individual level toward upstream structural levels, through strategies based on health promotion to guarantee the right to health by acting on the protective factors of health; and the development of strategies focused on social participation and intersectoriality are fundamental.
The RIIS Health Networks of the MoH, in partnership with the grassroots-level NHF, play a vital role to enhance prevention by involving at-risk farmers in MeN prevention initiatives. The NHF-linked RIIS has established a coordination mechanism with hospital and health center–based health promoters to develop multidisciplinary teams, including educators and psychologists, to provide holistic care to MeN patients. The NHF created the sectoral panel Environmental Management and Climate Change, which, in its advisory capacity, has visited agricultural cooperatives to raise awareness of potential risk factors for chronic kidney disease. During these visits, NHF representatives also identify farmers’ health needs and then include them in the public health policy agenda for discussion during meetings with MoH representatives at the national and regional level. At the community level the NHF has also organized participatory discussion tables and made health prevention announcements regarding MeN through television and radio. This awareness led a portion of farmers to develop homegrown protective strategies to counter this threat, which have kept them disease-free. Furthermore, strong alliances with other organizations at the community level have been created, such as the “alliance against privatization of water,” where the NHF has a strong leadership in the advocacy strategies. This example illustrates how the coordination between MoH and social movement (led by the NHF) is on the track for managing such a relevant disease under the social determination of health scope, taking into consideration upstream determinants such as pesticides regulation; intermediate determinants such as water surveillance and access, adequate labor behaviors, and regulation; and downstream determinants through awareness campaigns and improving access to health in remote areas; therefore carrying out a comprehensive management based on the right to health principles.
Discussion
This case study gives an overview on how a social movement can effectively play a role in ensuring community participation in decision-making processes. We describe how the National Health Forum (NHF) has been developing its activities since the introduction of the health reform in El Salvador a decade ago. 19
First, the participants in our study reported that, both from the health system and community’s perspective, participation must be meaningful. It has to evolve from a utilitarian model to a social control model where the community is continuously empowered toward making decisions based on their needs. 30 The term empowerment, as described by participants, is closely linked to a rights approach, meaning that communities feel empowered to advocate for health care as it is their human right. A strong social movement is essential to be able to challenge the existing power imbalance. In the Salvadoran context, this was possible because of the following reasons: (1) the political will that was created with the entrance into government of the FMLN, revoking the neoliberal health policies that had been in place for a long time, and (2) the strength of a historically organized population. As reported by Espinoza and colleagues, 31 previous neoliberal governments did not promote the right to have access to essential preconditions for health but only the right to have access to health care services. The health reform moved away from a biomedical approach focusing mainly on curative actions, individual responsibility, and lifestyles, with little concern for the state’s responsibility to modify the contextual limitations and address the underlying and structural causes of health inequity, toward a committed government aiming at incorporating people’s voice.19,22
The differences between social determination and the social determinants of health are not only conceptual, they are mainly social, economic, and political. They are 2 divergent routes, different explanations on causality and health risks, with fundamental implications on power relations, and in the understanding of the health-disease process. 25 As reported in this study, 2 things are key in the concept of social determination of health: as power relations are involved, mechanisms are implemented to overcome power hierarchies, such as accountability mechanisms and involvement of the community in the formulation of health policies. The other aspect is that, to ensure significant and lasting change, upstream determinants of health 4 must be taken into consideration: this implies addressing structural aspects such as housing, agriculture, access to water, and social violence. Different stakeholders and organizations must unite. A success factor noted by participants was that strong and long-lasting intersectoral action and local community alliances are more likely to produce policy change.
The context has a strong impact on building a basis that permits the social movement to move forward and to empower. Previous studies on El Salvador, as e.g., the experience of “The Construction of the Community Health System of Guarjila,” 15 describe how a strong social fabric developed in times of war. The community created strong resilience mechanisms that later transformed into organizational capacity and self-management. Many of these communities acquired organizational experience during the difficult struggles of the 1970s and 80s, making it possible for peasants to self-govern their small communities when the government withdrew from the area. They had to solve vital problems such as health, education, food, and other daily needs, with few resources. Community organization made it possible to address problems, i.e., involving the larger community in decision making. Solidarity and the constant search for equity were ensured through different community processes. 32
In line with a review of experiences,
33
which demonstrates that comprehensive approaches to address the social determinants of health effectively need to explicitly tackle issues of participation, equity, governance and the politics of power, decision making, and empowerment, some common elements can be highlighted:
Political will and policy coherence: The NHF was created as one of the main elements of a comprehensive health reform, meaning that political leaders recognize the relevance of social participation in the process off public policy making and the setting of a local health agenda. Decentralization strategies: A territorial approach aims at building strong leadership at all levels, in parallel with the health system. This has helped redirect resources to meet actual needs of the communities. A similar experience in neighboring Nicaragua stresses the importance of local governance.
34
Knowledge of participation generated in fragile sociopolitical context, throughout the years: Strong transfer of organizational and participation knowledge from preexisting organizations and further training of community leaders and health professionals to work together is needed. An intersectoral approach with the creation of thematic working groups, focusing on prioritized areas identified by the community: The need for an integrated approach and comprehensive public health and development plans responds to the need to provide “windows” for support that integrates people’s own vision and struggle. Advocacy work as transversal action: Working with other stakeholders on the right to health leads to an understanding that health is context-determined, and therefore other factors such as access to water, farmers’ working conditions, and adequate regulatory policies must be included in the struggle for the right to health. Alliances increase the likelihood of advocacy success, as they are more likely to produce policy change.
Social movements are important agents for social change because they raise awareness on people’s health rights and challenge both the process and the outcome of social and political decision making at local and global levels. 35 The example of the NHF through organized communities and strong participation strategies can play an essential role in ensuring the implementation of adequate government policies to address health inequities. This is what is required to assert the right to health.
Limitations
The limitations of the analytical framework applied in this study reflect the current lack of evidence-based theoretical frameworks to grasp and generalize the complexity of community processes. This study aims to contribute to the growing body of evidence on community participation and empowerment. Further systematization of this experience is recommended for future research. In addition, the high level of community violence in El Salvador at times limited the scope of the fieldwork carried out. These challenges were partially solved thanks to the support of key community members and health system personnel, who accompanied the field research group.
Conclusion
The Salvadoran experience in social mobilization, led by the National Health Forum, and its role in the development of the National Public Health System over the period 2009–2018, provides a strong example of community participation in health. The NHF’s focus on the role of participation strategies, empowerment, and co-governance with health institutions such as the Ministry of Health under the social determinants of health scope. The National Health Forum, a nationwide popular movement belonging to the People’s Health Movement, 36 plays a central role in the strengthening of the health system. 35
Supplemental Material
JOH905262 Supplemental material1 - Supplemental material for The Role of Social Movements in Strengthening Health Systems: The Experience of the National Health Forum in El Salvador (2009–2018)
Supplemental material, JOH905262 Supplemental material1 for The Role of Social Movements in Strengthening Health Systems: The Experience of the National Health Forum in El Salvador (2009–2018) by Montserrat León, Marta Jiménez, Nicole Vidal, Keven Bermúdez and Pol De Vos in International Journal of Health Services
Supplemental Material
JOH905262 Supplemental material2 - Supplemental material for The Role of Social Movements in Strengthening Health Systems: The Experience of the National Health Forum in El Salvador (2009–2018)
Supplemental material, JOH905262 Supplemental material2 for The Role of Social Movements in Strengthening Health Systems: The Experience of the National Health Forum in El Salvador (2009–2018) by Montserrat León, Marta Jiménez, Nicole Vidal, Keven Bermúdez and Pol De Vos in International Journal of Health Services
Footnotes
Acknowledgments
This research was possible thanks to support from members of the Ministry of Public Health Policies, the National Health Form (FNS), and the Public Health Policies Observatory, University of El Salvador, which facilitated access to different communities that might otherwise be difficult to reach because of ongoing social violence. We appreciate all the help and support given by Queen Margaret University specially Claire Mc Lellan, Jone García, and Alastair Ager. The authors would especially like to thank Eduardo Espinoza, Margarita Posada, Ma Isabel Rodriguez, Angela Elıas, Rina Abrego, Morena Murillo, Henry Palacios, Rene Domınguez, Alex Martınez, Emma Cortez, Moises Garcıa, Juana Rivas, Jorge Irazola, Luzmila Argueta, Guillermo Argueta, and community members for their warm welcome. Montserrat León García is a PhD candidate at Universitat Autónoma de Barcelona, and this work will be part of her PhD work on shared decision making.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIHR Global Health Research Programme 16/136/100, Queen Margaret University. The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NHR or the UK Department of Health and Social Care.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.