
Abstract
This article discusses the colonial policies around public health, sanitary measures and control of venereal diseases in the Madras Presidency in the 1860s and 1870s, and describes how these policies shaped urban development of Madras. It investigates how British colonial measures to curtail venereal diseases concurred with concerns about ‘public health’ in the 1860s and 1870s in the Madras Presidency and the city of Madras. It questions the extent to which British ‘public health’ policies encompassed the Indian population. Although there is a recent increase in scholarly interest in studying the medical and sanitary history of the Madras Presidency, very few historians have focused on the ways in which colonial morality influenced town-planning and sanitary policies in the area. Earlier, scholars believed that segregation was key to maintaining public health in colonial cities; however, recent scholarship has questioned the notions of ‘dual city’ by highlighting the blurred lines. This article also investigates how far the colonial administration successfully segregated the European population from the Indian population and the Indian labouring and service-providing poor from the non-labouring poor.
In a letter to the Government of Madras and Robert Stanton Ellis, the chief secretary, on the workings of the Indian Contagious Diseases Act (1868) in its first six months, H. Stanborough, suggested that the health officer appointed to register and control cases of venereal diseases among women practising prostitution should extend his services to the entire city. 1 Most historians have assumed that venereal diseases were a problem confined to British troops, but it is clear from the colonial archive that the British officers treated these diseases as a peril to the broader public health of Madras. The subject of the control of venereal diseases and prostitution is incomplete, therefore, without discussing colonial policies towards public health, urban planning and sanitation. These policies overlapped with one another during the mid-nineteenth century when South Asian colonial cities such as Madras, Bombay and Calcutta began to take a visibly urban form. 2 The urban planning of these emerging cities often focused on the spatial containment of the labouring and sexualised bodies of inhabitants in the name of sanitation and public health. 3 This article examines the concurrence between measures to control prostitution and venereal diseases, on the one hand, and measures to improve the sanitary condition of Madras during the 1860s and 1870s, on the other. I primarily address the broader context of colonial public health and urban planning of Madras and other cantonment towns such as Wellington, Vellore, Bangalore, Secunderabad and Trichinopoly in the Madras Presidency. Evidently, these were driven by the need to tackle issues of overcrowding, filth and diseases such as cholera and malaria. I also suggest that most of the sanitary policies which focused on improving public health also incorporated—and indeed sometimes overlapped with—measures to control venereal diseases and prostitution.
Existing works on venereal diseases have focused on their impact on the British military in India and measures taken by colonial health authorities to confine European as well as Indian prostitutes. 4 Comparatively less attention, however, has been paid to the measures taken by the colonial government to control or cure venereal diseases among the Indian population. Erica Wald argues that any health concerns related to venereal disease were limited primarily to European soldiers. Except for a single footnote—which documents a suggestion made in 1810 by William Ingledew, a surgeon at Mysore, about the majority of Indian men in that town suffering from venereal disease—Wald claims that there was no concern about venereal disease among either sepoys or the Indian public for most of the nineteenth century. 5 Wald further explains that although the Medical Boards of Bengal and Madras suggested that government authorities should interfere or extend policies related to the control of venereal diseases into the public sphere on the grounds of public health, military and medical officers were never wholly successful in persuading civil magistrates to cooperate with their designs. 6 Wald suggests, moreover, that the mention of public health in these reports should not be misunderstood as relating to the Indian masses but instead only to those Indians whose health might negatively impact European soldiers. 7 In exploring the changing nature of the colonial state, and a shift in focus from the healthcare of only the military to ‘public health’, Stephen Legg also concludes that the colonial government’s main concern was with the military rather than the broader Indian population. 8 Legg’s work sheds some light on the evolution of the notion of ‘social hygiene’, which expanded from that of ‘imperial hygiene’, wherein the perspective on tackling issues of maintaining hygiene moved from an individual threat and self-discipline to a more public approach. 9
Before we discuss how measures to control venereal diseases overlapped with concerns around public health, it is important to understand what this meant to the British administration. It is a complex task, as ‘public health’ meant different things at different times. 10 Wald has argued that in colonial documents, public health concerns were initially limited to European soldiers and civilians, and only to that portion of the Indian population which could negatively impact the health of the British population in India. It is the argument of this article that the Indian people also eventually became a part of colonial public health concerns. Public health in early nineteenth-century Madras initially concerned the European army and civil population, but by the 1860s it slowly began to incorporate the labouring and service-providing Indian population as well. Over this period, colonial public health concerns also served to segregate as well as protect the service-providing section of the Indian population from the non-labouring destitute Indian population. The regulation of this section of the population eventually became the defining element of colonial sanitation and broader urbanisation. Colonial concerns around public health sought to segregate the labouring from the non-labouring Indian population, but in practice, such segregation was neither rigid nor precise.
The expansion of healthcare facilities and sanitation was partly driven by self-preservation, partly by a sense of responsibility for the welfare of the Indian population, and partly to facilitate colonial commercial interests. The necessity of quarantine measures in the Red Sea due to the prevalence of cholera and the consequent disruption to colonial trade had put pressure on the colonial Government of India to establish domestic quarantine in Indian port cities, to regulate shipping and cleanse, disinfect and generally improve Indian cities through better planning and control. 11 Colonial urban planning often revolved around public health and facilitating the needs of colonial elites. Khaled Fahmy’s work on Cairo has explored the creation of the ‘colonial dual city’, where the elite and urban poor were segregated by colonial town planning in the name of maintaining public hygiene. 12 Several works on colonial urbanism in South Asia have gone beyond this concept of the ‘dual city’ to show that segregation lines between coloniser and colonised enclaves were often blurred. 13 Segregation was, however, a primary aspect of colonial urbanism where urban planning attempted to hide the unpleasant aspects visible in different pockets of emerging cities as well as to control the sensory environments of these places. Carl Nightingale has also argued that segregation has been a key element in all historical urban settlements and highlights the interconnection between the history of urban development and segregation. 14 Nightingale acknowledges the messiness of this segregation whereby populations often crossed borders to provide different services and at times to engage in illegal exchange with the elite inhabitants of the cities; he emphasises, moreover, that other dynamics such as religious rivalry, class divisions, gender and power hierarchies ensured and maintained the lines of segregation. 15
Scholars such as Biswamoy Pati, Chandi Nanda and Jane Buckingham who have worked on leprosy and the leprosy asylums in colonial Orissa and Madras have argued that colonial discourses around public health often revolved around the removal or control of certain sections of the urban population who were considered undesirable and a source of infection. 16 Prostitutes and women suspected of practising prostitution were certainly one of the undesired sections of the urban population which colonial town planners wanted to regulate and render invisible, not just due to concerns over public health but also due to anxiety over the morality of the colonial city. Ashwini Tambe examines Bombay’s transformation as a port city and the ways in which the prostitutes who provided sexual services to military, migrant and maritime workers had a significant influence on the planning of that city. Similarly, Legg’s work on colonial Delhi focuses on the development of policies to control and segregate prostitution to a particular area of the city to regulate British soldiers’ access to sex as well as to limit health risks. 17 Recent historiography of colonial medicine and science has started exploring different aspects of the Madras Presidency to better comprehend the history of colonial India. 18 However, very few works study the ways in which notions of colonial morality influenced town planning and sanitary policies or how measures to control venereal diseases overlapped with concerns of public health in the context of the Madras Presidency. 19
History of the City of Madras
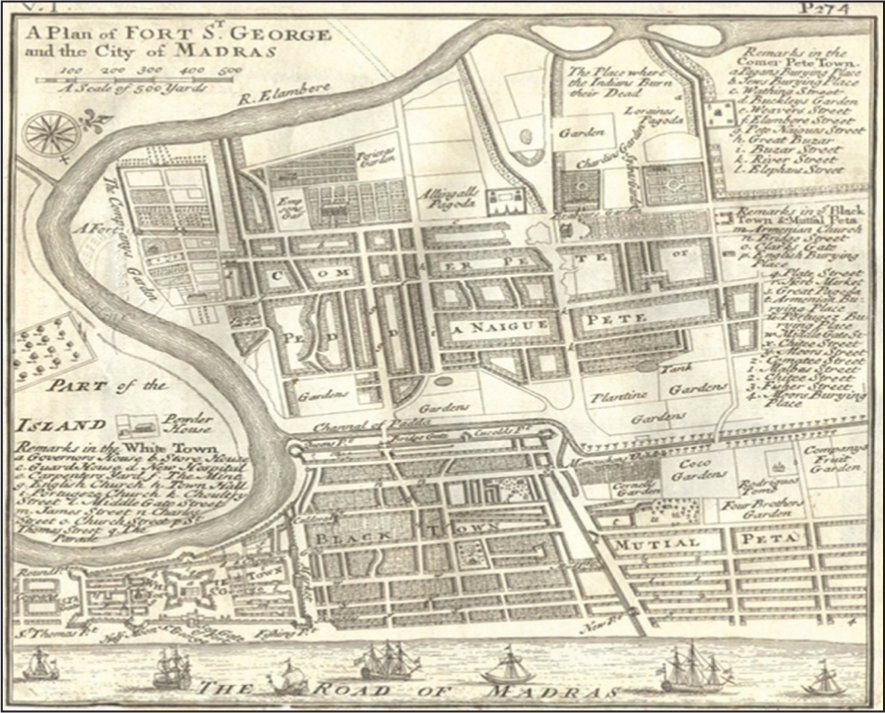
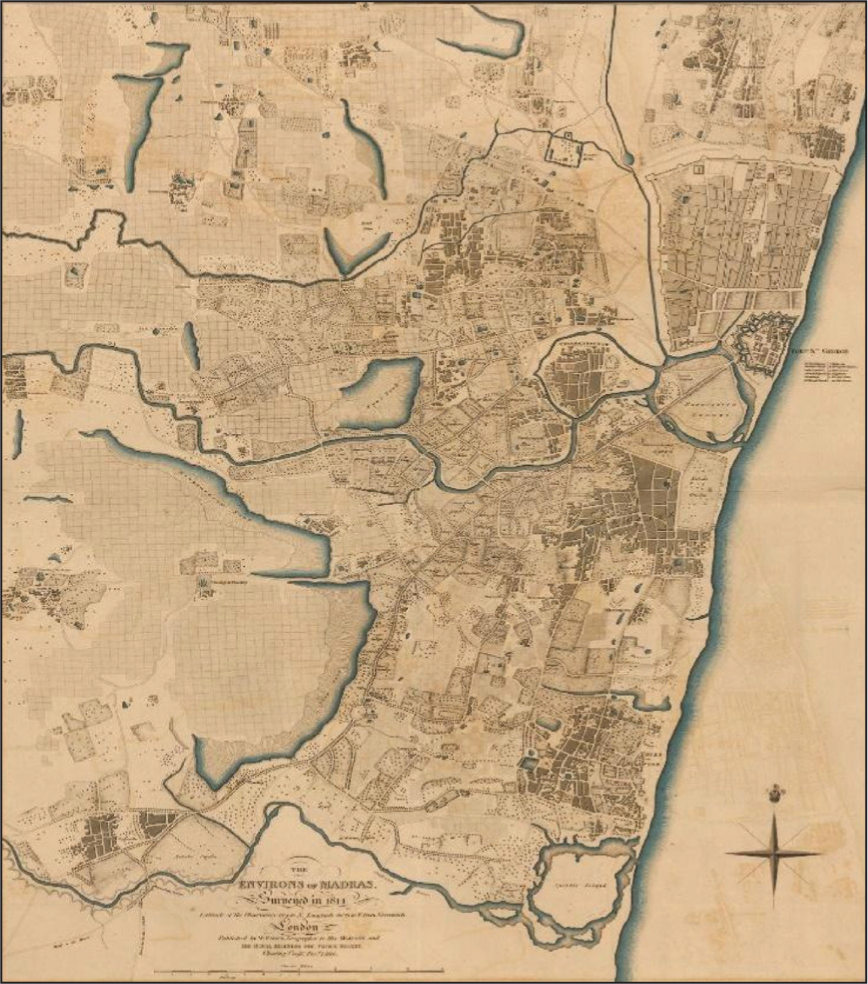
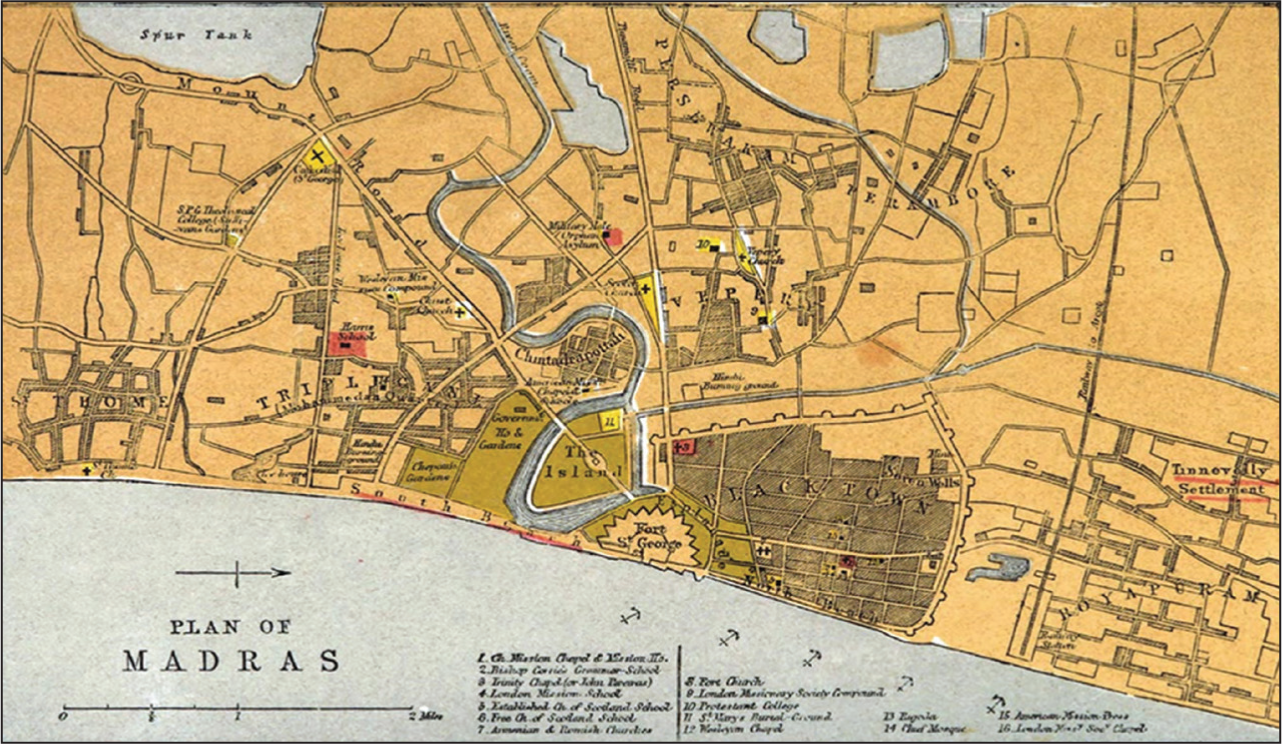
The city of Madras was developed by the English East India Company when they built Fort St George in the mid-1600s near the small fishing village of Tondaimandalam in the Bay of Bengal (Figure 1). 20 Susan Neild’s work on Madras in the eighteenth and nineteenth centuries shows that the city did not develop uniformly and had varied agrarian, urban and rural zones. 21 Unlike its counterparts Bombay and Calcutta, which, by the mid-nineteenth century, had major industries such as jute and cotton mills which attracted a large number of migrant labourers, Madras city had relatively fewer major industries and was known to be a city of colonial bureaucrats. 22 According to Neild, the city was essentially divided into two parts: the European enclave of Fort St George and the Black Town, which housed Indian labourers and service providers. These two centres were surrounded by the mirasi villages, which retained an agrarian and Indian quality. Susan Neild and Susan Lewandowski have argued that Madras was essentially segregated; Neild’s work in particular highlights that within Indian dwellings themselves, segregation was often caste based. 23 As mentioned earlier, recent South Asian historiography has moved beyond the concept of the ‘dual city’ and has highlighted the blurred lines between European and Indian dwellings. Neild acknowledges that there was pluralism in city spaces and that slowly by the nineteenth century the surrounding villages, suburbs and hamlets began to be absorbed into Madras city (Figures 2 and 3) and became colonial commercial localities retaining Indian qualities, where colonial service providers dwelled. 24 Despite not having many major industries, the growing European population at Fort St George, which was working for the Company in the form of bureaucrats, bankers and other Company employees, required the services of the Indian population in the form of skilled artisans, wage labourers, clerks and dubashe (translators). The majority of the Indian city dwellers of Madras provided daily services to the colonial bureaucrats. Even the mirasdar or the landed native elite of agrarian villages surrounding Fort St George and the Black Town worked for the Company and later for the British crown as agents, accountants or dubashe. The city was formed according to the needs of Company employees. 25 The surrounding suburbs and hamlets of Fort St George were often populated by a community of service providers which the company workers needed on a regular basis. For example, the localities of Chindrapet were predominantly weavers’ villages that made the company uniforms, while Washermenpet was populated by people doing laundry for these officials. The colonial city space of Madras was a complex entity, neither fully segregated as a ‘dual city’ nor completely intermingled with the European population. 26 While planners may have been unsuccessful in establishing rigid boundaries between the European and Indian enclaves, colonial sanitary measures did focus on segregation, confinement and the invisibility of certain sections of the population such as prostitutes and the non-labouring poor who could potentially harm the health and well-being of British and Indian elites. At the same time, the colonial government had to provide sanitary facilities for the labouring poor and, to some extent, to prostitutes to ensure that no harmful disease was communicated to the colonial employees (both European and Indian) who needed their services on a regular basis.
Public Hygiene and Indian Dwellings
The mid-nineteenth century saw the urbanisation of the South Asian colonial cities of Madras, Bombay, Delhi and Calcutta—a process that was extended to other cantonment towns. Scholars have discussed how campaigns and policies around public health in colonial cities forged a new urban formation, which often focused on the removal or control of the movement of a section of the population regarded as unpleasant. 27 In most cases, it is the poor who were identified as the source of infection which posed a threat to the moral and social order of the city and political stability. 28 These new urban formations demanded the removal and sanitisation of the urban poor and demolition of the old urban centres, especially the working-class slums, which would be replaced by office buildings and other commercial and retail stores. 29
A similar development is observable in the Madras Presidency, where native dwellings were reconstructed to suit the demands of the growing European and urban populations in the name of public health. 30 The need for better public hygiene required not just the removal of certain sections of the population but also the incorporation of some service providers into its public health scheme. The following section focuses on how sanitary measures which were initially directed to preserve the well-being of the British army and civilian population within cantonments were slowly extended to the poor Indian dwellings near the cantonments of Fort St George/Madras, St Thomas Mount, Secunderabad, Bangalore, Trichinopoly, Wellington and Vellore.
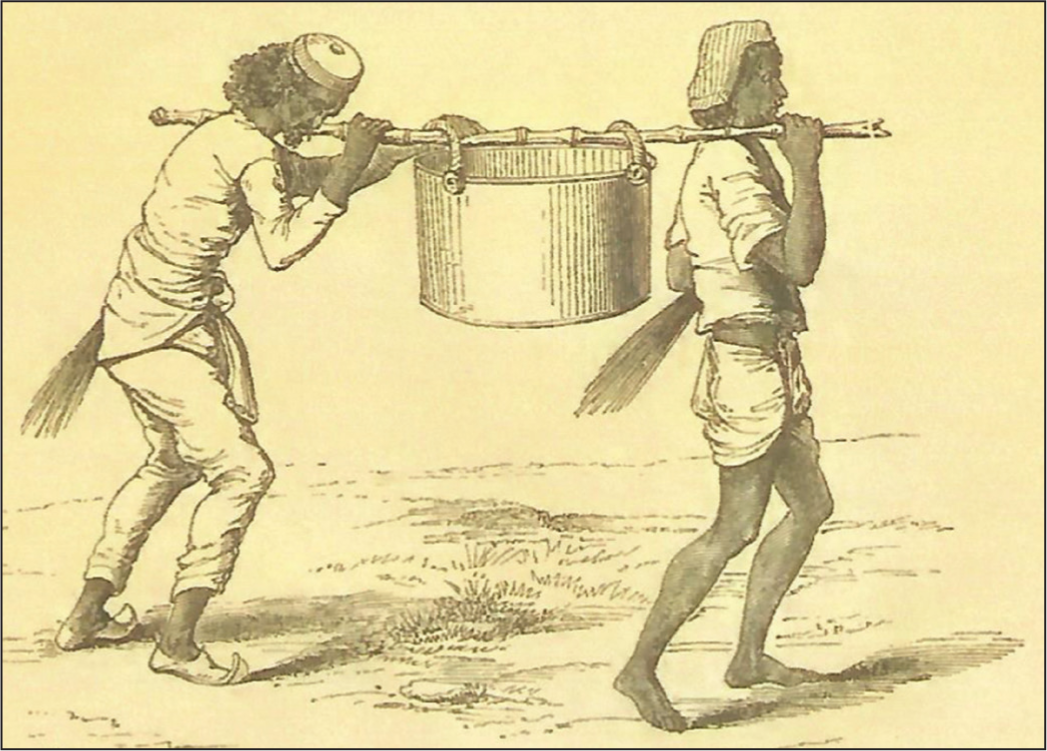
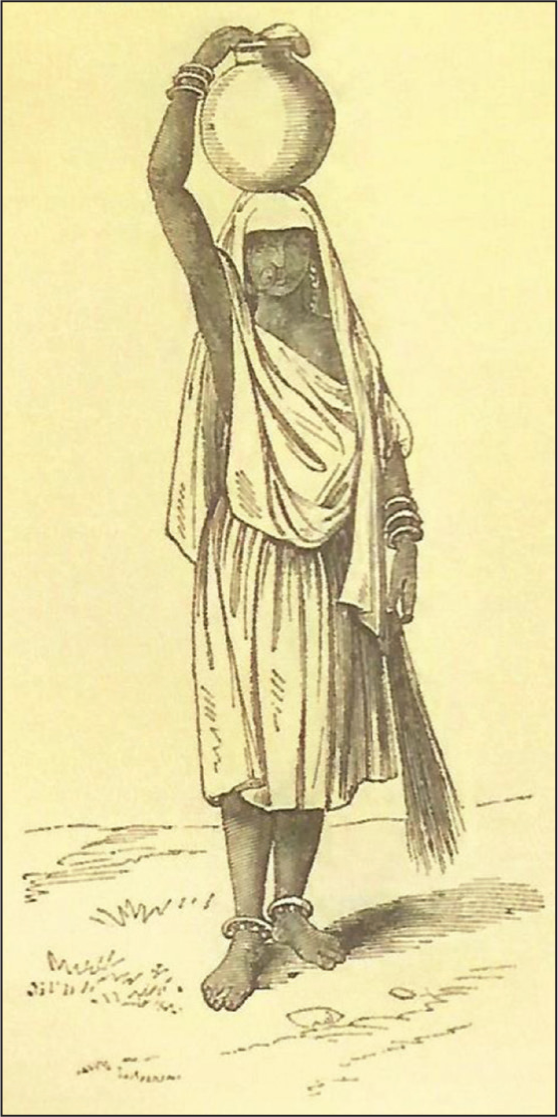
The reports of the Royal Commission of 1858 on the sanitary conditions of the British army stationed in India and Florence Nightingale’s reports on sanitary conditions in the cantonments of India both noted the unsanitary state of the cantonments and suggested measures for improvement. Most reports on the sanitary conditions of the cantonment blamed the neighbouring Indian dwellings for their poor hygiene. Nightingale’s observation of the sanitary state of the army in India describes how the military camps, situated in close proximity to ‘low, wet or damp and unhealthy’ native or Indian towns and bazaars which were full of ‘nuisance’, were at great risk of diseases from health hazards. 31 The report mentions that in nearly all the British stations, ‘camp diseases’ were caused by bad water, bad drainage, filthy bazaars, poor ventilation and ‘surface overcrowding’ or not enough space in barrack huts and sick wards. 32 It was noted that most of the cantonments of the Madras Presidency had filthy water; the tanks always had questionable substances floating in them and often functioned as the endpoint for the drainage of filth. 33 It was reported that except in stations such as Wellington and Fort St George, there was grave suspicion about the purity of water supplies. Wherever anything like an account of the water quality was given, the water was unquestionably ‘bad and dangerous’. 34 In her 1863 report for the Royal Commission of 1861, Nightingale observed that ‘At Secunderabad, as much as 119 grs. [grams], of solid matter, and, as it would appear, 30 grs. [grams] of organic matter per gallon’, were found in some of the well and tank water. 35 The water drawn from these so-called ‘filthy’ places was believed to be the cause of diseases such as malaria (due to mosquitoes breeding in them), cholera and dysentery. 36 It was also noted by Nightingale that bheesties (water carriers) (Figures 4 and 5) were employed as ‘human water pipes’ to draw better quality water for the cantonments. 37 It was suggested that instead of employing bheesties, who were not only expensive but also drew water of questionable quality, proper equipment and the appliances of ‘civilization’—meaning buckets or pipes—be used to bring water to the cantonments and the neighbourhood. 38
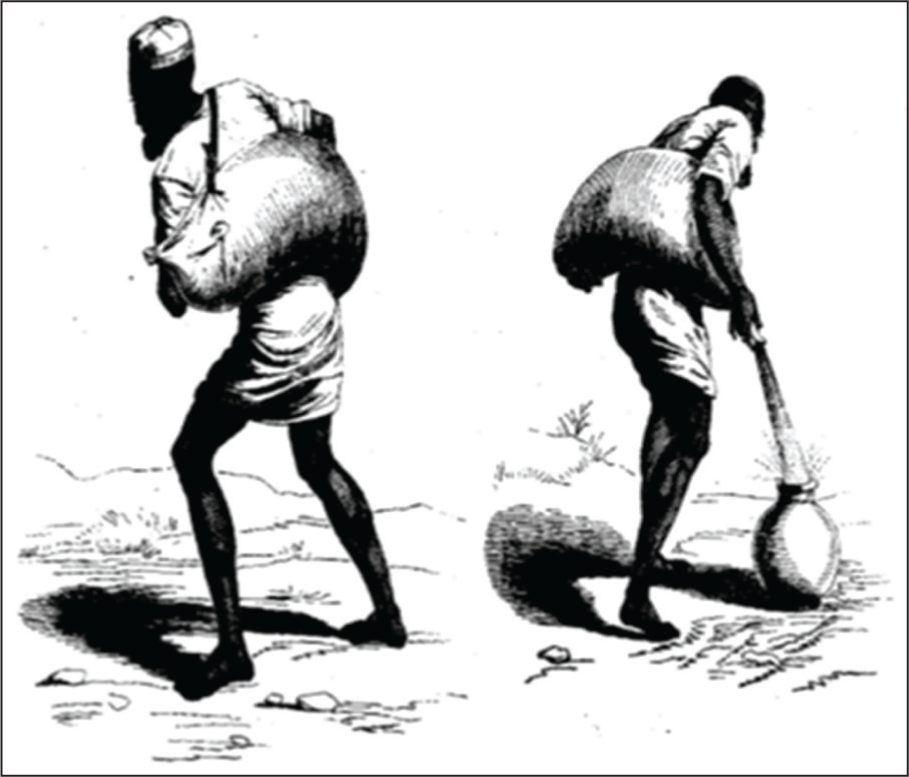
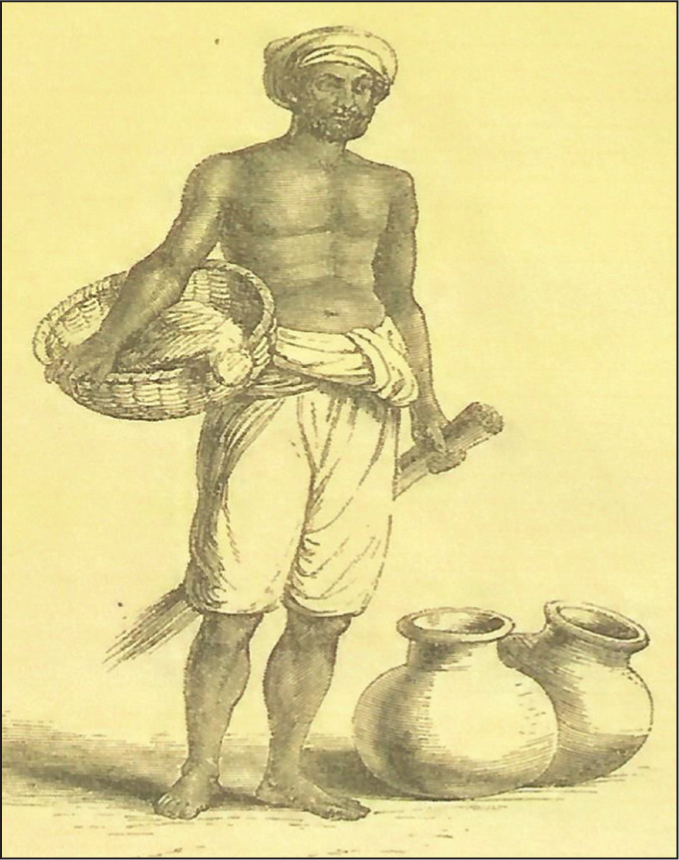
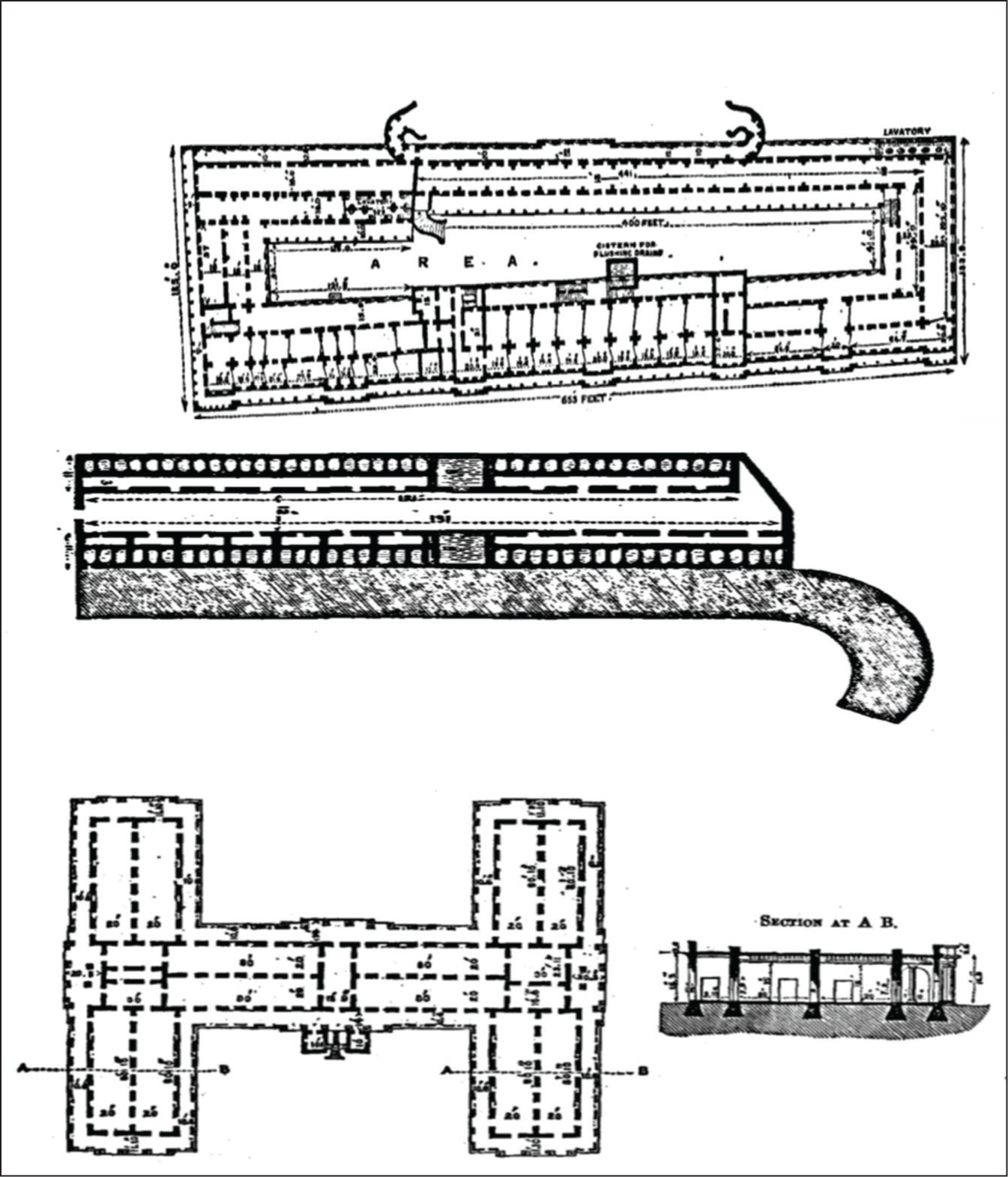
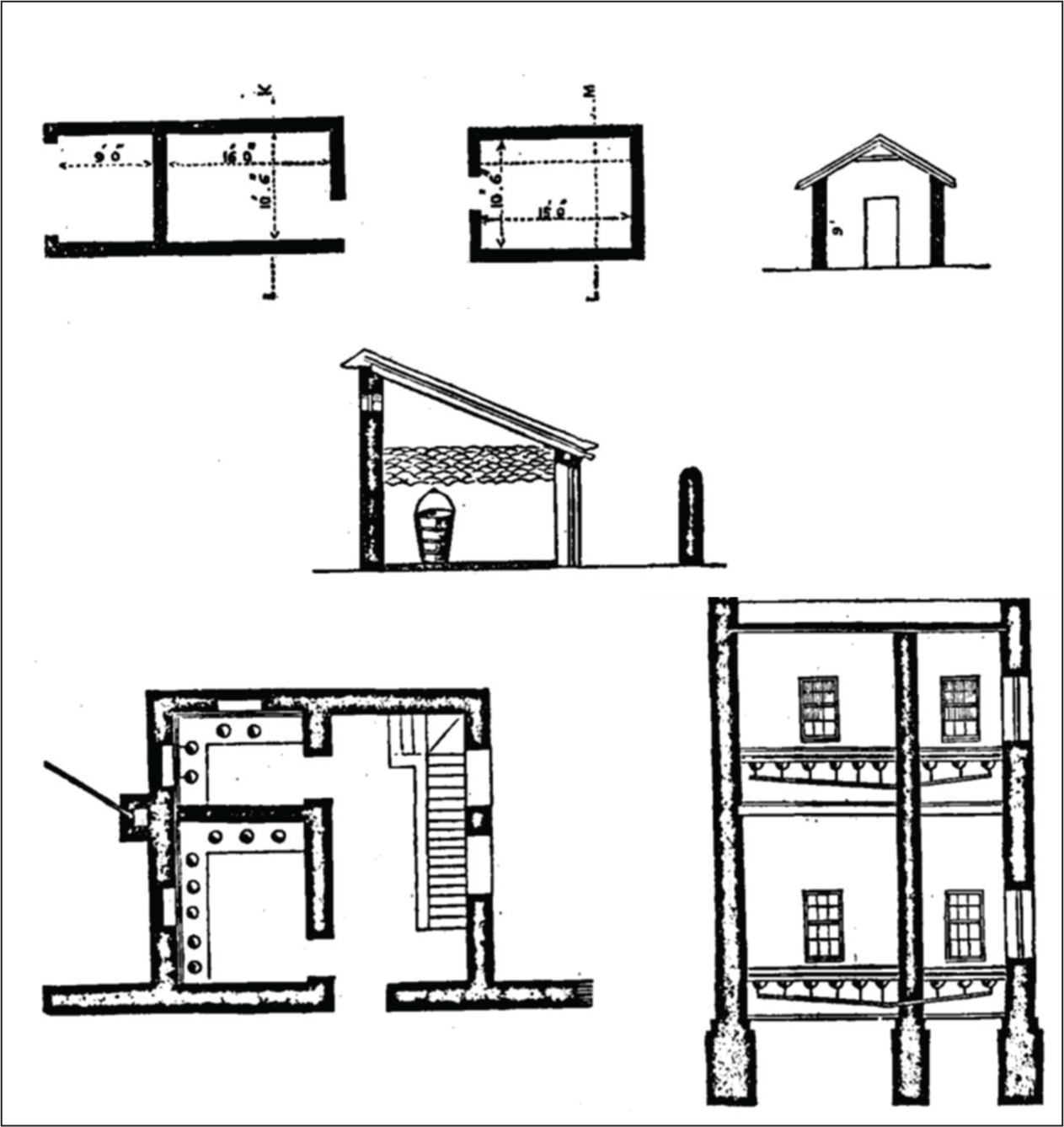
The sanitary report writers considered that bad drainage caused as much harm to public health as bad water. It was observed by Nightingale that most of the cantonments and stations did not have proper drainage systems, and where there was some sort of a cesspit, its contents were often removed by hand by mehter, or sweepers (Figure 6). 39 At Madras (Fort St George) the drainage was stated to be ‘worse than useless’. The main drain of the town was just 80 yards away from the European fort, and the effluvia from it was very offensive according to Nightingale. The arrangements at the native or Indian lines, as described in the reports, were simply ‘abominable’. The old privies in Fort St George were ‘as bad as they well could be’ (Figure 8). 40 The surface drainage was a major threat to public health; at most stations, the rainfall either ran off on the surface or was left to evaporate. 41 Usually, all the drainage was directed to sink in the subsoil; whatever did not evaporate or sink in the ground was removed with pails, skins or carts and dumped elsewhere. 42 It was noted in a number of reports that without careful and efficient drainage it was difficult to protect public health. 43 In the absence of a proper drainage system, the mehter were crucial for maintaining the cleanliness of the cantonments (Figure 7).
Overcrowding and an increasing population were considered other significant contributors to the excessive accumulation of surface filth.
44
The surface filth often led to epidemics such as cholera and dysentery. It was noticed by Nightingale that the Indian population that lived both within the cantonment and in the bazaars and the neighbourhood always exceeded the population of Europeans; she believed this to be the cause of bad sanitation. The term used by Nightingale and other report writers was ‘bad overcrowding’.
45
The following abstract from the 1864 report of the Royal Commission on the sanitary condition of the Madras Presidency describes how the close proximity of this ‘bad crowding’ in Bangalore could result in a sanitary hazard for the European population:
Every military station in India has its bazaars, mostly in close proximity to the European lines. They consist of huts or houses arranged on no general plan, and without any regard at all to sanitary conditions. They have grown up anyhow, and have increased with the bazaar population, which always bears a very high proportion to that of the European troops at the station; for example, Bangalore, already referred to, has accommodation for about 1,700 European and 2,600 native troops.… There has hitherto been no limit to the proximity by which these large native populations may approach European barracks, nor to their position as regards prevailing winds.
46
The report went on to say that there were no regulations as to the general arrangement of Indian houses, the width of streets, the water supply or the direction of the drainage.
The habits of the natives are such that, unless they are closely watched, they cover the whole neighbouring surface with filth; and if there be any ravines or, pits in the neighbourhood they convert them into dangerous nuisances. There are generally no public necessaries. There are often open cesspits among the houses. The surface drainage sometimes flows into tanks, from which the water supply is derived. 47
The close proximity of Indian dwellings posed a major threat to the cantonments according to British sanitary policy makers. Even the wind which blew from their neighbourhood to the cantonments was believed to contain an odorous smell which could possibly harm the European population living there. 48 It was requested that strict policing of Indian dwellings be undertaken. 49 Reports focusing on the sanitary condition of cantonments have noted that Indian dwellings and bazaars near the cantonments were dirty, had unsanitary conditions and were responsible for spreading diseases such as smallpox and cholera in the cantonments. 50 It was generally asserted that Indian dwellings and bazaars near the cantonments were poorly ventilated, dirty and crowded. 51 Indian dwellings in other presidencies were also described in a similar manner. It was noted in their 1860 report on the sanitary condition of Poona by Colonel Charles Cameron Shute (6th Dragoons), William Deeble (Surgeon of the 56th Regiment) and W. J. Stuart (Surgeon of the 25th Regiment Native Infantry) that ‘The poor natives occupying small huts or otherwise crowding together and … objecting admission of light and air into their dwelling’ were predisposed to diseases such as cholera, gonorrhoea, syphilis and ophthalmia, especially among ‘the lower caste owing to their filthy habits of living and eating’. 52 Similarly, in another 1861 report on Vellore, a cantonment of Madras Presidency, Dr Sutherland noted that Indians remained ‘perfectly indifferent’ to the condition of their houses which were considered to be dung heaps, cesspits and ‘hot-beds’ of diseases. 53 It was also noted by the Royal Commission of 1863 that the killing of animals such as sheep and cattle and the viscera of slaughtered animals scattered around the cantonments could also cause serious damage to sanitary conditions. 54 The fish (mostly dried) sold in the native Indian bazaars was also considered harmful. 55 The 1863 Royal Commission suggested that regulation for preserving cleanliness in the bazaar was needed and that the appointment of sanitary police would benefit the cantonments greatly. 56 The Commission also suggested that a slaughterhouse be established far from the cantonments and that bad fish be removed ‘once at least every 24 hours’. 57 ‘Bad’ water and ‘bad’ drainage, coupled with the problem of ‘bad overcrowding’ and ‘poor ventilation’ were some of the common descriptions of the neighbouring Indian dwellings. Such dwellings were seen to pose a major threat not only to the Indian population living there but also to the British or Europeans who visited such places. It is interesting to see how these sanitary concerns overlapped with concerns around venereal diseases.
Venereal Diseases and Sanitary Measures
This section addresses how the efforts to control venereal diseases functioned within the process of sanitisation of the cities of the Madras Presidency. The concerns over venereal diseases among the men of the British army have been discussed in detail in many works which focused on the exclusive nature of these colonial measures and the vital roles British troops played in India to maintain colonial dominance. 58 Venereal diseases were the most prevalent disease among the British troops in India according to the Royal Commission of 1858. 59 Most of the British soldiers deployed in India were young and unmarried, confined to the barracks with little to no entertainment. The monotony led to various vices among army men such as gambling, alcohol addiction and seeking the company of prostitutes. The colonial administration tacitly tolerated prostitution to allow these men to satiate their ‘manly’ urges, fearing that a refusal to do so would lead to ‘sexual misconduct’ such as sodomy among the troops. 60 To ensure the health and well-being of the British troops, the colonial government implemented the Cantonment Act in 1864 and the Indian Contagious Diseases Act in 1868. Under these Acts, women suspected of practising prostitution were registered and examined either every fortnight or seven days. If they were found to be infected by venereal disease, they were confined to lock hospitals until they were cured. 61
By the mid-nineteenth century, efforts were initiated by the colonial government to provide healthcare facilities and treatment for venereal diseases to Indians as well, although the healthcare provided to the general Indian population was far less comprehensive than that provided to the British. There are a few examples of how venereal diseases among the Indian population were of concern to the colonial medical officers. For example, Sir Alexander Murray Tulloch claimed in 1861 that venereal diseases were as widespread among unmarried civilian men as among army officers and lower-level soldiers, but since many of them sought treatment from civil practitioners, due to lack of any sort of reports from these clinics, it was difficult to accurately measure how far a disease had spread among the general population. 62 Inspector General MacPherson reported in 1863 that syphilis was widespread among the Indian civilian population as well. He noted that it was prevalent in ‘the child of five year age [sic] and in the old hag of 60’. 63 In certain reports, it was noted that in populous and large cities like Madras as many as 30,000 people could be suffering from venereal diseases, which had to be curtailed to protect public health. 64 Colonial medical authorities were anxious about female and male civilian inhabitants of Madras city suffering from venereal disease in secret and evading the policing under the Act, which might spread the disease indirectly among British soldiers. In 1867, W. Mackenzie, Inspector General of the Indian Medical Department, reported the necessity to establish a separate general hospital to treat female civilian patients to prevent overcrowding and the mixing up of ‘respectable’ females—European, East Indian and native/Indian women—with the prostitutes who had been hitherto treated at the lock hospitals in the Vepery Dispensary in Madras. 65 Similarly, H. Stanbrough noted in 1869 that the male inhabitants of Madras who suffered from venereal diseases might infect the courtesans or prostitutes they visited, and this might have spread the disease to British sailors. 66 He ascertained that cases of syphilis had increased since the abolition of the district dispensaries and hospitals, which compelled the diseased, who could not afford to employ the private practitioners, ‘either to resort to the General Hospital, or the Monegar Choultry, a charitable institution, or to suffer in secret the effects of the disease’. 67 He noted that the smaller government dispensaries at the district level helped diseased persons obtain advice and treatment without observation or a sense of shame, whereas the large medical institutions such as the General Hospital and the Monegar Choultry would expose the diseased person to ‘the gaze of large establishment[s] of medical subordinates and pupils, and to feel that they are the subjects of mocking observation and humiliating jokes’. 68 It was suggested by medical surgeons and lock hospital superintendents that medical aid for venereal diseases be provided to civilians of Madras without moral judgement and that medical dispensaries be re-established at the district level in order to curtail the disease. 69 Within the lock hospitals and the lock wards of Madras Presidency, it was the desire of the benevolent medical officers that the patients be treated kindly and considerately. Of course, it is questionable how far these measures were carried out successfully, but a core argument of this article is that public health measures in terms of venereal diseases were no longer enclavist or exclusive. Even while medical aid provided to the general Indian population suffering from venereal diseases was limited and was more of a self-preserving act, these examples show that colonial authorities did incorporate the general Indian population to some extent into their scheme to protect public health in terms of venereal diseases.
The discussions on improving public health and sanitary conditions in Madras Presidency also incorporated the dwellings of prostitutes and women under suspicion of practising prostitution. For example, Health Officer Stanbrough reported on the unsanitary conditions of the dwellings of suspected women in the Black Town of Madras:
In the houses of ill-fame inspected by me in the Black Town I saw no sanitary precautions. All the laws of sanitation are set at defiance in the abodes of these unfortunates. The houses in the Second Line Beach and the neighbourhood are located in narrow lanes reeking with the foetid odour of decayed animal and other substances; ill constructed, ill-ventilated, they have all that [sic] defects that must render them unhealthy, and the healthiest person who may be so unfortunate as to sleep in these dens of iniquity and disease for a night cannot escape contamination, and cannot be but become [sic] predisposed to be inoculated with venereal virus.
70
Stanbrough’s foremost concern was for the British or European men visiting these places for sexual services, who could get infected and spread it to others living within the cantonments. Stanbrough further requested that some law be established to regulate the number of persons occupying each house in this area. 71 He also reported on the defective drainage, noting that there were no means for speedily carrying off the ‘horrible filth that is produced within these houses’. 72 He noted that open drains ran through the courtyards through the length of the hovels, which tainted ‘the air in every part with the abominable exhalations which must be pregnant with disease’. 73 Stanbrough exclaimed that it was a wonder that sickness and disease were not more frequent in this ‘great plague spot’ of the city despite no deodorizers or antiseptics being used. 74 He further observed that most courtyards had a small well of brackish water used for culinary and washing purposes ‘into which the soldiers and sailors frequently urinate’ and that the water was ‘utterly unfit for culinary purposes’. 75 He requested that a freshwater scheme should incorporate a supply of water for the courtyards of native Indian houses as well ‘so that the open drain in them may be abundantly flushed, and thoroughly cleansed, for the public urinals and for flushing and cleansing sewers’. 76 The bheesties sold the drinking water at three paises for two small chatties (pots) full, or the same quantity contracted for at eight annas a month, equal to six rupees a year. 77
Lord Napier, the Governor of Madras, also suggested in his 1869 report that the Contagious Diseases Act and lock hospitals were the key to improving the sanitary conditions of Madras. 78 Elsewhere, I have highlighted the role of Indian subordinates such as Chowdranies, peons, dhais and gomastahs in controlling venereal diseases in Madras Presidency through their work at lock hospitals. 79 Sanitary reform, although mainly aimed at protecting the European population visiting Indian dwellings, might also provide better health conditions for the Indian population. Prostitutes were to be provided with a sanitised living atmosphere and housing schemes which were more suitable for a ‘healthy’ living condition so that the British troops who visited them were not affected by the sanitary hazards to which they were otherwise susceptible. 80 It was hoped by the sanitary policymakers that proper sanitary reform might render the services of the bheesties and mehters—whose services, it was often complained, were too expensive—superfluous. But in the short term, their labour was critical to public health, the corollary of which (for the British) was the importance of ensuring healthy living conditions for the labouring poor.
Selective Sanitation for ‘Service Provider’ Dwellings
The cantonment towns and cities such as Madras, Bangalore, Secunderabad and Wellington saw a great number of sanitary policies implemented during the mid-nineteenth century. Measures to improve the water supply, the drainage system and the cleansing of the streets as well as regulations around the general construction of buildings were clearly aimed at providing health and sanitary facilities to the European troops stationed in these cantonment towns (Figures 9 and 10). But they were also aimed at improving the conditions of the labouring poor. With regard to providing sanitary measures to the Indian population, the Governor of Madras Sir C. Trevelyan said:
I consider that not only the preservation of life and health is concerned, but the strength and comfort and general efficiency of the population are involved; they would be better and abler men, women, and children for all the purposes of life, if the average standard of mental and bodily vigour were improved by the removal of these local causes of a low state of health.
81
Sir C. Trevelyan was also responsible for re-introducing the lock hospitals to the Madras Presidency after they were abolished in 1835. 82
Stanbrough suggested that Indian dwellings in Madras, especially those visited by British soldiers (such as brothels or the dwellings of women suspected of practising prostitution), should also be provided with drinking water and cleaner courtyards and sewers. 83 However, the provision of these facilities altered the outlook of the native Indian dwellings and displaced certain sections of the population. The freely available water in Indian courtyards was replaced by drinkable water, which was provided by the municipality at a cost. Furthermore, the courtyard wells were flushed and cleansed so that they could be turned into public urinals, where soldiers and sailors could urinate. 84 This altered the way Indian dwellings were constructed; the new Indian houses and huts near urban centres around Fort St George slowly abandoned the construction of the traditional Tamil courtyard ponds by the early twentieth century. 85 The bazaars, lanes and streets in the native Indian quarter were also broadened in the later nineteenth century. 86 The government provided and laid the piping for drinking water, and hence, streets were dug up in the native lines. 87 Royal Commission reports also urged that public latrines should be erected and the Indian population should be forced to keep their surroundings clean and not cause any nuisance to public sanitation. 88 At Secunderabad the superintendent of police used to visit the bazaar and Indian neighbourhood once a week and fined the owners of any house where ‘filth’ or ‘nuisance’ was found. 89 Broadening the streets and digging up the lanes meant that Indian huts and houses that hindered any of these projects would have to be removed. 90 The houses which were huddled together, or those located at the intersection of pipelines and having improper drainage nullhas (channels), or those which were a general hindrance to municipal projects were slated for removal or remodelled by the sanitary commissioners. The cesspits in these Indian dwellings were also remodelled so that they could be accessible for cleaning by the mehter every 48 hours. 91 The 1863 report of the Royal Commission on Bombay also mentions how the crowded bazaars and their surrounding neighbourhood would be cleared in order to make room for public buildings and broader streets. 92 The report on the Indian neighbourhoods in Trichinopoly of Madras Presidency recommended levelling and filling up of the streets and pulling down ‘deserted’ huts and walls near the cantonment. 93 All these cases exemplify the ways in which sanitary policies implemented in the 1860s and 1870s impacted traditional Indian dwellings as well as changed the face of urban spaces in the Madras Presidency.
These sanitary projects aimed to protect the European population eventually incorporated the Indian labouring poor but saw the destitute poor as a threat to public health. The destitute and non-labouring poor became the target of most reports of the sanitary commissions in both Madras Presidency and Bombay Presidency. They were declared to be the source of infection and were removed from the bazaars and Indian dwellings altogether so that they did not cause any nuisance to neighbouring Indian dwellings and the British stations. 94 According to the Royal Commission report of 1861, a close watch was kept on people causing a ‘nuisance’ at Kamptee, and they were ‘taken up daily’ (possibly arrested). 95 There were regular patrols in the cantonment of Mangalore to prevent any ‘nuisance’. 96 At Kolhapur, two peons and two night police were appointed to prevent the nuisance of public defecation from being committed between 4 am and 10 am, and the offenders apprehended were fined by the superintendent of police. 97 The 1863 report on the Bombay Presidency also indicates how the broadened streets and construction of the public buildings were intended to remove all the unwanted populations from the native bazaar, along with those labouring poor whose services were no longer needed since there would be no further employment for them once the sanitary and construction projects were completed. 98 These examples demonstrate the ways in which the non-labouring poor were under constant surveillance and any mistakes committed by them would lead to them being removed or severely punished. They also suggest how even the labouring poor were only tolerated up to the point where their services were needed. Once their service was no longer necessary, they also fell in the category of the ‘unwanted’ destitute population causing a ‘nuisance’. Colonial policymakers thus differentiated the destitute from the labouring poor and tried to provide sanitation to the working population at risk from poor living conditions. The destitute poor or the non-labouring poor were of no use to them. Rather, they were a liability, causing a threat to public health. The policies directed towards prostitutes and women under suspicion of practising prostitution also functioned in a similar manner. Although their dwellings were incorporated into public health schemes for practical reasons of protecting the health of the British soldiers, policymakers tried to segregate and regulate this section of the population to maintain public—or rather, the soldiers’—health, thus maintaining their colonial position as upholders of superior morality.
Resident’s Reaction to Lock Hospitals
By the mid-nineteenth century, Madras had become a symbol of colonial modernity with the provision of sanitary facilities such as drinking water, bathrooms, latrines and reasonably planned streets. By this time the colonial presence in India was also justified on the basis of their moral superiority. 99 This complicated the incorporation of dwellings of prostitutes into the colonial idea of ‘public’ health further. Having Indian prostitutes roam the streets of Madras, which had become a symbol of colonial modernity, was considered ‘lamentable’ by the colonial administration as well as by respectable city dwellers. Victorian morality demanded that anything related to sex or sexuality should be rendered invisible, and any ‘undesired’ sections of the population should be segregated and regulated. 100 Lock hospitals, which functioned as the primary place to restrict and regulate women practising or suspected of practising prostitution, became the centre of debate among residents of Madras city. Two important lock hospitals in the city of Madras were located near Popham’s Broadway in the heart of the Black Town and in Vepery near Periamoot (current-day Periyamet), and residents near these lock hospitals often complained and requested that the lock hospital be moved elsewhere. Although the race of the residents who raised complaints regarding the lock hospitals is not revealed in these newspaper articles, it can be assumed that most of these complaints were raised by European residents of the Black Town. But given the diversity in the population in the Black Town with substantial part of it formed by Indian dubashes, artisans and weavers, it can be presumed that if not all, at least some of these complaints could have been raised by the well-off Indian dubashes living in the Black Town. For example, in 1869 it was reported that residents of Vepery complained about the presence of a lock hospital near their property. They urged that proper supervision be exercised over the institution, which had led to the relocation of two or three of the elderly residents of Vepery, who moved out of the area to avoid hearing the Babel of foul languages used outside the lock hospital. The article goes on to mention that one of the property owners had petitioned the government to move the lock hospital as his nearby property value had depreciated and the hospital had driven away tenants from his house. 101 Similarly, a resident of the Black Town complained in 1871 about the lock hospital in Popham’s Broadway. The letter noted that residents of the area, especially Europeans and East Indians, lamented that by establishing a lock hospital in the heart of the Black Town the government had exhibited very little consideration for ‘their morals or their feelings’. The resident further exclaimed that the proximity of the lock hospital was a nuisance for the residents and suggested that it be moved to a different location outside of the Black Town. 102 The residents petitioned the government to use the old civil orphanage building outside the Black Town as a lock hospital instead of the location near Seemboodoss Street. 103
The lock hospitals of the Black Town and Vepery remained in that same location despite constant complaints from residents of the area at least until the 1880s when the campaign against the Contagious Diseases Act was growing stronger. 104 The government did try to segregate the lock hospitals by building walls around them, but this measure did not have the desired effect. Instead, the wall itself sometimes became the very thing which created a nuisance for residents: a resident of Seemboodoss Street in the Black Town complained that ‘filthy’ words both in Tamil and English were written on the wall. 105 Complaints against the use of ‘filthy’ words in Tamil on the walls of lock hospitals also indicate the possibility of Indian residents raising these complaints. 106 The wall also often failed to conceal the premises completely, and the neighbouring residents complained that houses which were in the other direction and those which were not covered by the wall would not likely benefit from it. 107 Even the slightest gap in the wall would lead to distress among the residents of the locality. For example, the residents of Seemboodoss Street asked the municipality to quickly close the unsightly gap in the wall around the lock hospital, which had been created due to a new construction project. The residents were worried that the gap had led to ‘natives’ of all classes being able to peep into the lock hospital and to hold conversations with the inmates. 108 Any alteration to improve the lock hospital that led to the modification of the Black Town or more specifically Semboodoss Street was not welcomed and was often met with dispute and discontentment. For example, an August 1874 newspaper article revealed that the residents of Semboodoss Street were not pleased that a water fountain near Tucker’s Chapel, adjacent to the Eastern wall of the lock hospital, was slated for demolition in order to pave the way for the new entrance to the hospital. 109 The article illustrated that the residents believed that the reconstruction would be an ‘eyesore’ in the street, and the government seems to have dropped the plan. 110
The ongoing complaints by residents of the Black Town led to the appointment of a committee to find a suitable building for the lock hospital so that it could be removed from its current site. The committee concluded that the lock hospital could not be moved due to no other suitable site being available, and the committee suggested some alterations to the institution to satisfy the complaints. 111 The location of the lock hospital in Black Town near a chapel was also considered worrisome by local residents. In an 1877 letter to the Madras Mail, a resident signed ‘Veritas’ complained about the proximity of the lock hospitals to the Church Mission Chapel and the adjacent boys’ and girls’ schools. This letter also reveals that the lock hospital was functioning as an orphanage before it was converted into a hospital and that the children were moved to an asylum elsewhere. Veritas suggested that the committee looking into relocating the lock hospital should have been directed to the Egmore Asylum rather than the Grand Jail, as the Egmore Asylum had more space to accommodate inmates as well as the health officers, matrons and apothecaries. The resident further suggested that the orphanage be moved back to the Black Town and listed a number of merits of the institution. 112 Another newspaper article from 1889 recounted how the bishop and the clergy of Madras wanted the lock hospital to be moved to a less populous part of the town. The article also revealed how the bishop and the clergy were not opposed to lock hospitals and encouraged the supervision and medical treatment under lock hospitals, but rather objected to the compulsory nature of it, as well as its situation at the centre of town. 113
These examples reveal how the very institution which the colonial administration created to protect public health and uphold morality was itself seen as a source of public nuisance and vice by nearby residents as well as clergymen. In addition to the perceived threat of moral contagion, local residents also brought sanitary hazards near the lock hospital to the attention of the municipality. One resident of the Black Town complained about the drainage problem near the lock hospital, pointing out that all the waste from its privies was allowed to concentrate in the drain in Tucker’s Lane and flow around Mr Dring’s and Mr Jackson’s premises before finding its way to the main drain in Davidson’s Street. The resident suggested that this nuisance could easily be overcome by constructing another drain covered from Popham’s Broadway to meet the main drain. 114 It is unclear whether this suggestion was accepted, but these examples reveal the active participation of the residents of Madras (at least those residents who had privilege and influence) in planning or administering the city in the mid-nineteenth century. Unfortunately, the sources do not reveal what the women in prostitution who were confined to the lock hospitals thought about the sanitary measures and city planning.
The decisions of the colonial government were often driven by self-protection and self-benefit. But on many occasions the administration had to take local elements and ground level practicality into consideration. They had to incorporate public opinion—or those sections of the public who could express their opinions—into their health and sanitary measures as well as urban planning. Moving a step further, the colonial government slowly but eventually had to incorporate the general Indian population into their idea of ‘public’ and ‘public health’ and provide them with sanitation as well as healthcare facilities. 115
Conclusion
This article has built on the scholarly understanding of venereal diseases in colonial India to examine the subject of public health, sanitary measures and aspects of the urban planning of Madras city and other cantonment towns within the Presidency. The attempt was to understand the complex process of the segregation and incorporation of ‘undesired’ and ‘essential’ sections of the population within colonial sanitary policies, pointing to the ways in which facilities such as water supply, toilets and street cleaning were provided selectively to the labouring poor by the colonial government. In contrast, the non-labouring poor were considered a nuisance that needed to be regulated or removed from the city. Efforts to protect the European and Indian elites’ need for, and indeed dependence on, labourers and prostitutes meant that these groups were incorporated into a colonial scheme of public health. While the dwellings of prostitutes were incorporated into sanitary schemes, the institution of the lock hospital which was used to regulate these women became a site of concern for residents. A colonial project of moral sanitisation was thus complicated by the Victorian morality of the residents of Madras, who saw the institution of the lock hospital as a nuisance that should be segregated from the respectable areas of residence. The process of the incorporation of the dwellings of service-providing sections of society into colonial sanitary schemes, and a desire to segregate the institutions such as lock hospitals which regulated women in public, shaped Madras city and other cantonment towns in particular ways.