
Abstract
Why do nurses in training continue to draw on the ideal of compassion when responding to their experiences of nursing work in the UK National Health Service (NHS), despite the difficulties that they face in developing compassionate, long-term relationships with patients in practice? To answer this question, we draw from a psychosocial analysis of focus group data from 49 trainee nurses in the NHS. First, we show how this ideal leads them to blame qualified nurses for failures in patient care. We suggest this is an unconscious defence against the anxiety evoked both by the vulnerability of their position as those who need to gain access to the profession, and of being unable to conduct compassionate nursing work. Second, we emphasize that less powerful occupational groups, such as trainee nurses, may adopt defences that underpin dominant organizational policy, such as idealization, despite further disadvantaging their group and benefitting those in power. We conclude by questioning the particular emphasis on compassion in nurses’ training, which can prevent occupational solidarity and the ability to reflect on the structural and organizational factors required to conduct patient-centred nursing work.
Keywords
Introduction
In the last decade, there has been an active promotion of a more patient-centred and compassionate approach to nursing work in the UK. This is emphasized in both policy documents and professional statements (Commissioning Board Chief Nursing Officer and DH Chief Nursing Adviser, 2012) and in a nursing education stressing the moral and practical importance of ‘providing care with relationships based on empathy, respect and dignity’ (NHS England/Nursing Directorate, 2013: 4). However, nurses are expected to adopt and exercise these moral values in their work while facing intensified pressures. The argument for UK public service austerity has been used to justify continued cuts to health service funding (NHS England et al., 2014). The withdrawal in 2017 of the NHS bursary for nursing students, coupled with uncertainties around Brexit, led to significant problems with recruitment and retention (Adams, 2017). Furthermore, the rise in managerialism in the NHS since at least the 1990s has led to increasing external scrutiny and control of professional nursing work (Traynor, 1999), and a drive for performance improvements through cultural changes that seek both to change basic values and assumptions about the delivery of care and to streamline services (Hyde and Davies, 2004). As a consequence of these changes and structural forces, nurses experience new levels of conflict, work intensification and burnout (Manzano García and Ayala Calvo, 2012). Performing emotionally draining work in under-resourced environments over many years can thwart nurses’ attempts to incorporate the occupational values of holistic, compassionate care (Paley, 2014). Moreover, the observation by trainee nurses that qualified nurses do not appear to practise in this way (Maben et al., 2007) brings confusion and uncertainty about the role and how it should be performed.
Despite the challenges of adopting compassionate, patient-centred care in practice, the ideals of compassion prevail. Our aim in this article is to explore why nurses in training continue to draw on this ideal when responding to their experiences of NHS nursing work. We use a psychosocial perspective to investigate the unconscious manifestation of compassion as a pervasive discourse (Fairclough, 2003) in trainee nurses’ focus group talk.
We begin the article by discussing the current emphasis on compassion in the UK national health service and its influence on the developing professional identity of nurses. We then draw from systems psychodynamics research to question the unconscious reasons for the persistence of this ideal. Systems dynamics integrates the practice of psychoanalysis, the theories and methods of group relations, and open systems theory (Petriglieri and Petriglieri, 2020) to understand the role of the unconscious and how social defences may prevent organizational learning and change (Bain, 1998; Long, 1999). Much of systems psychodynamic thinking is now advanced by a psychosocial lens (Vince, 2019; see also Kenny and Fotaki, 2014), which adopts psychoanalytic theories beyond those of Kleinian or object relations schools along with additional conceptual frameworks such as discourse theory (e.g. Gough, 2004; Hollway and Jefferson, 2000). We adopt a psychosocial approach and use systems psychodynamics theory, drawing on concepts from Klein et al. (1952) and particularly Bion (1961) to investigate connections between the unconscious, subjective life of trainee nurses and the dynamics underpinning powerful discourses (Fotaki et al., 2012). We then describe the Methods and Findings, and end the article by highlighting our contributions to the literature on compassion and organization studies.
The compassion discourse in the nursing profession
While caring and compassion have long been claimed as distinctive moral characteristics of the nursing profession (Benner and Wrubel, 1989), as a result of a series of well-publicized nursing failures and patient-care scandals in the UK, notably poor care and high mortality rates in Stafford Hospital, nursing leaders have been compelled to restate an emphasis on compassion within the profession (Commissioning Board Chief Nursing Officer and DH Chief Nursing Adviser, 2012). The same failures have contributed to compassion becoming an enforced and overarching virtue designed to govern all levels of British healthcare (Pedersen and Roelsgaard Obling, 2019). This reflects a wider research and policy agenda that increasingly looks to compassion as a key to improving the quality of services, organizations and relationships (Fotaki, 2015; Lilius et al., 2011). It is not only viewed as a feeling that may or may not be present when nurses conduct their work, but has emerged as a dominant discourse within the nursing profession that influences and shapes employee subjectivity (Simpson et al., 2014). Despite appearing as a more humanistic means of managing healthcare, compassion is a continuation of the control and target culture of New Public Management and its preoccupation with measuring individual conduct and performance (Pedersen and Roelsgaard Obling, 2019). The approach to compassion in the nursing profession in the UK healthcare system is very much about the identities of the nurses who carry it out (Pedersen and Roelsgaard Obling, 2019). This is reflected in the report of a national inquiry into the failures at Stafford Hospital in the UK (Francis, 2013) which led to a renewed promotion of ‘Values Based’ recruitment of nurses (Department of Health, 2013). Performance management regimes now include a focus on ‘compassion’ which demands certain values and behaviours in healthcare workers (Tutton and Langstaff, 2015).
The compassion agenda, therefore, puts demands on the subjectivity and personal and moral character of the nurse who, having worked for years in under-resourced and over-stretched environments often experiences ‘compassion-fatigue’ (Sinclair et al., 2017). In practice, many nurses are burnt out and struggle to develop meaningful compassionate relationships with the people they care for (Grandey, 2003). Trainee nurses describe their encounters with qualified nurses as inconsistent with the ideals of compassion (Maben et al., 2007). The contradiction between the aims and values of the compassion discourse and the real difficulties that nurses experience in developing long-term, compassionate relationships in practice is an example of unrealistic healthcare policy that is far removed from operational realities (Fotaki, 2006) and raises questions about the persistence of the ideal of compassion. In the following, we first review some psychoanalytic concepts before showing how systems psychodynamics approaches help to explore the unconscious reasons for this persistence.
The systems psychodynamics tradition and psychosocial studies
Klein’s contributions to systems psychodynamics centre on the concepts of paranoid-schizoid and depressive positions. Proposed by her as being first experienced in infancy, they also provide useful understanding and explanation of psychic behaviours of groups in organizations. In the paranoid-schizoid position, opposing feelings of love and hate are managed through the splitting of the world as either wholly ‘good’ or wholly ‘bad’ (Klein et al., 1952). The ‘good’ is idealized as gratifying and reflects an unconscious striving towards what one is supposed to be (Freud, 1955) and protects against the ‘bad’ (Klein et al., 1952). This defence mechanism splits the ‘bad’ off from the self and projects it into others. This defends against being confronted by some truth about oneself, which may produce guilt or anxiety. In Klein et al.’s (1952) conceptualization, as the infant matures it moves to inhabit the depressive position, in which it can accept ambiguity, that the good and the bad can coexist in the same ‘object’, and the urge to control anxiety through splitting is reduced. This is a reparative state that entails understanding of complexity, but is also accompanied by loss, mourning and guilt.
Bion (1961) links Klein’s paranoid-schizoid and depressive positions to the mental states of groups to explore how unconscious dynamics influence group life. For Bion (1961: 143), ‘every group, however casual, meets to “do” something’. In the ‘work group’ state, the group is able to manage its task and its internal dynamics, is able to cope with ambiguity and is attuned to the demands of external ‘reality’ and the task at hand. ‘Basic assumptions’, on the other hand, describes a situation when a group is unable to focus on its task (Bion, 1961) by effortlessly forming mental states that coalesce around different patterns of drives, affects, mental contents, object relations and defences. To protect against feelings of isolation, group members act as if they believe the group has come together with the purpose of preserving the group rather than engaging in productive, creative activity. In this state, thinking becomes dogmatic and stereotypical and there is a lack of self-reflection (French and Simpson, 2010). There are three basic assumption states: ‘pairing’, ‘fight/flight’ and ‘dependent’ (Bion, 1961). Pairing is driven by an unconscious hope that implicit conflict is resolved by two members of the group creating a pair. When in fight/flight mode, the group acts as if it has come together to run away from something or to attack someone. Scapegoating, name-calling and blaming are common (French and Simpson, 2010). The dependency basic assumption is often active when individuals feel vulnerable and that they need to protect themselves (Bion, 1961) through dependency on something or someone, often an individual within it or the group itself. When a sense of unity with people in the group is created, there can be hostility to anything that is perceived as disturbing the link to each other (Hirschhorn, 1988: 61).
Idealization of compassion in healthcare policy
Menzies’ (1960) influential study drew on Klein and Bion to explore how defences such as splitting and idealization were embedded in the structure and culture of a London hospital to minimize the effect of difficult emotions evoked when nurses work with patients who are ill and dying. However, one consequence of practising emotionally detached nursing was that patients were treated as ‘tasks’ and nurses were unable to develop any meaningful relationships with them. This social defence system dehumanized the nursing work and produced alienation and stress among nurses. So while the nature of the task created a variety of feelings, the real source of anxiety was the defensive techniques used in the organization of nurses’ work; the attempt by the organization to rigidly control the relationship between the nurse and the patient, the ritual performance of prescribed tasks and the disciplining and punitive system (Halton, 2015).
For nurses to exercise their ‘capacity for concern, compassion, and sympathy’, Menzies (1960: 116–119) suggested ‘eliminating the task-list system and substituting some form of patient assignment’. As a consequence, Menzies’ research contributed to the later promotion of so called ‘patient-centred’ nursing work (Tutton and Langstaff, 2015). However, today, in under-resourced, routinized workplaces, nurses report feeling unable to develop meaningful relationships with patients (Tutton and Langstaff, 2015), suggesting that idealization in nursing has not disappeared since Menzies’ time; nurse training is based on ideals that are unrealistic in practice (Maben et al., 2007). Developments in systems psychodynamics thinking help to question why the ideal of compassion prevails, despite the obvious difficulties in practising compassionate nursing.
Healthcare by its nature manages people’s anxiety about annihilation (Obholzer, 1994) and healthcare policy is therefore prone to idealization (Fotaki, 2006), especially as a response to healthcare scandals and failures (Hoggett, 2006). However, since social defences often allow protection from anxiety for the powerful (Petriglieri and Petriglieri, 2020), idealization – when upheld by dominant policy – enables those in power to defend themselves against the painful reality of their own role in healthcare failures. Fotaki and Hyde (2015) demonstrate how healthcare policy entails a split between policy and implementation, removing policy makers from the effects of their decisions, enabling them to blame potential failures on individuals who implement the policies. In healthcare organizations, idealization ‘maintains contact with good, albeit unrealistic, feelings while bad feelings are externalized’ (Fotaki and Hyde, 2015: 447). Such processes become part of organizational structures and cultures, which organizational members then internalize (Schwartz, 1987) and take as appropriate solutions to organizational problems (Handy and Rowlands, 2017).
The nursing profession tends to evoke people’s sense of vulnerability and dependency (Dartington, 1994). Through the compassion discourse, this predominantly female occupation is given the ‘impossible task’ (Hoggett, 2006: 188) of reducing suffering and shielding against despair through nurses’ care and compassion. Nurses are allocated an ‘anxiety-containing’ function (Obholzer, 1994: 171), just like a mother’s role for her crying baby. Compassion appeals and is difficult to question, but its idealization distorts reality because it does not take into consideration the complexity of emotions entailed in the performance of nursing work: ‘The work situation arouses very strong and mixed feelings in the nurse: pity, compassion, and love; guilt and anxiety; hatred and resentment of the patients who arouse these strong feelings; envy of the care given the patient’ (Menzies, 1960: 98). As an example of top–down policy-making, the promotion of compassion leads to further formalization and standardization (Hoggett, 2015) through, for example, the measurement and testing of levels of compassion in individual recruits (Tutton and Langstaff, 2015). Existing research shows that trainee nurses experience anxiety about their personal ability to deliver ‘compassionate’ care in a context where experienced nurses do not appear to practise in this way (Curtis et al., 2012). Trainees have also been found to experience anxiety arising from their need to gain access to the profession by gaining the approval of mentors in the workplace who act as gatekeepers (Henderson et al., 2012). In line with Menzies’ (1960) arguments, the source of anxiety for the trainee nurse could then be hypothesized to be the punitive and controlling organization of trainees’ work – which has remained unchanged since Menzies’ time (Evans, 2015) and which is today reinforced by the compassion discourse.
A psychosocial approach
While systems psychodynamics perspectives have long explored how psychic and unconscious motivations interact with dominant political forces (Petriglieri and Petriglieri, 2020), psychosocial studies contribute by investigating defences in relation to wider structures of discourse (Hollway and Jefferson, 2000). We draw from this perspective to explore how the compassion discourse is bound up with trainee nurses’ unconscious psychic experiences (Gough, 2004; Kenny and Fotaki, 2014) and how trainees invest in this discourse as it protects them from anxiety and supports their self-narratives (Ford, 2010: 53). Gough (2004: 247) states that: in talk where the language used is evidently infused with anxiety and/or desire, where speakers passionately construct ‘others’ as threatening and/or weak, and where these others are vehemently decried and discursively expelled from ‘normal’ society (and self), then an exclusive focus on language and construction falls short.
We therefore decided to combine the discourse analytic approach originally planned with concepts from Klein and Bion to explore the possible unconscious influences on those discourses. While there are different ways of drawing from psychoanalysis in discourse analysis – for example, some influenced by object relations theory (Frosh et al., 2003; Hollway and Jefferson, 2000) and others by Lacan (Parker, 2010) – and though the emphasis on psychoanalysis has not been without controversy (see Baker and Kelan, 2019 for a review of this debate), the significance of psychoanalysis in the examination of talk and text continues to be acknowledged (Baker and Kelan, 2019). Our own approach is inspired by Gough (2004) who combines discourse analysis with Kleinian concepts to explore collective management of anxiety within focus groups, but we add to this by making substantive use of Bion’s (1961) insights into group dynamics. Psychosocial studies, therefore, allow consideration of the performative and unconscious effects of discourse, which we elaborate in the following.
Method
Focus groups were conducted to gain understanding of the developing occupational identities of nurses in training. Because of the emerging nature of our interest in these data, the groups were not run with any specific psychosocial or systems psychodynamics approach in mind. Nevertheless, the focus group method offered an opportunity to explore the replaying of defences in team-based workplaces within the groups. A disadvantage of focus groups is, however, that they tend to recreate normative discourses (Smithson, 2000: 105). The group can suppress individual opinions due to social desirability issues, and the general opinion can turn out to be more extreme than opinions expressed individually (Hollander, 2004). An alternative perspective considers that the group dynamic of focus groups is, in fact, what makes them interesting (Smithson, 2008). From this viewpoint, the group is the unit of analysis, rather than the sum of individual opinions, and the focus group is seen as a social process that provides fascinating access to ‘public’ discourses on a topic (Kitzinger, 1994). What matters is less individual’s ‘true’ opinions, than the interaction between the participants and how and why a ‘shared’ discourse may emerge. As a consequence, while differences between individuals are not insignificant, focus groups bring to light group phenomena; how certain views are reinforced, silenced or challenged. The accounts in any focus group are unavoidably products of the group context, public performances that emerge in that situation (Smithson, 2000). Furthermore, while members are temporarily interacting, focus groups offer a legitimate exploration of group behaviour because they ‘produce an interaction in which participants respond collectively and collaboratively, are aware of a common purpose, and reflexively act in terms of that purpose’ (Myers, 1998: 107). Despite evoking normative discourses, there usually exist tensions which are revealed by close analysis of the way in which normative discourses develop (Smithson, 2000). Exploring how counter-arguments are dealt with exposes the extent of emotional investment in discourses.
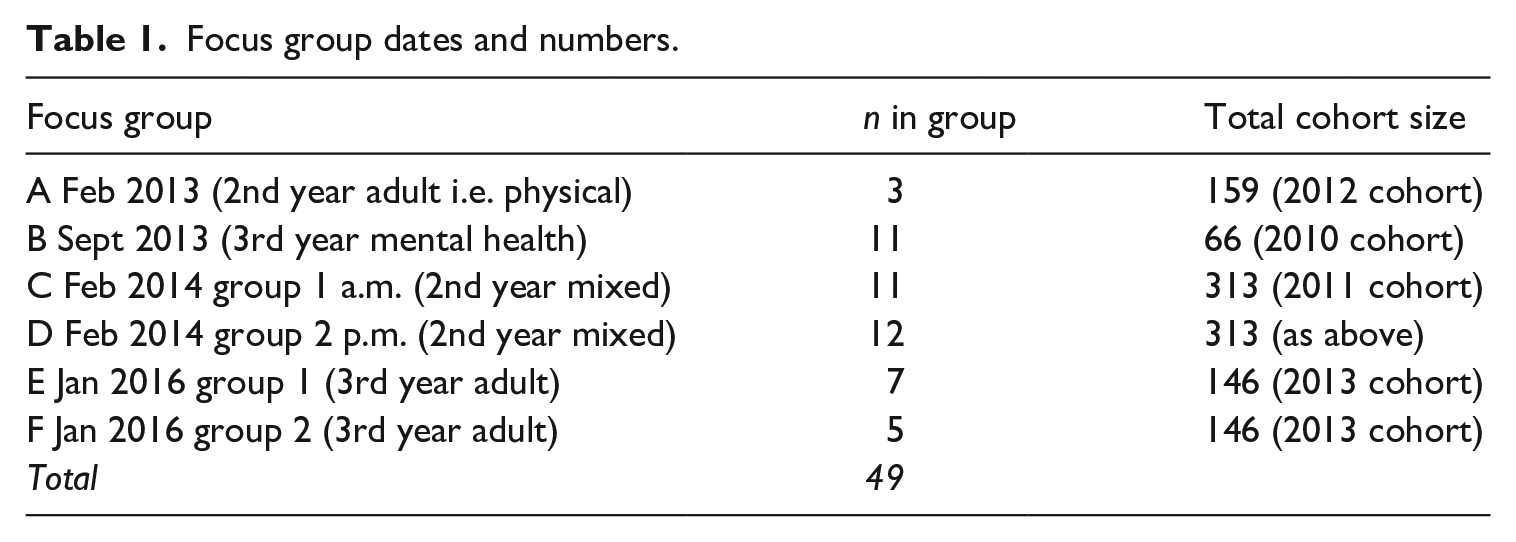
The data analysed in this article were collected at a London university between 2013 and 2016. With the permission of teaching staff and ethical approval from the university’s ethics committee, all groups of trainees who started BSc Nursing courses were invited in person by the third author to participate in focus groups. Six groups of volunteers were subsequently convened involving 49 trainees who were completing the second or third year of a three-year training for qualification either as a mental health nurse or an adult nurse providing physical care of adults (see Table 1). Trainees at these levels were chosen because they had accumulated experience in NHS workplace settings across a number of healthcare organizations. No demographic or biographical information regarding the participants were recorded. This was because at the time of study design the research emphasis was on group-level discussion, common in focus group research, as mentioned earlier. Nevertheless, it was noted that the great majority of the participants were female, reflecting the gendered character of the profession.
Focus group dates and numbers.
The focus groups lasted between approximately 40 and 60 minutes and were facilitated by the third author who was not involved in delivering the programmes and was only known to the trainees as a senior member of the Faculty. This situation is likely to have re-produced, in the focus groups, discourses that the trainees have been exposed to in their training programme, and it is precisely such normative public discourses – and the way in which the trainees interact with these – that is our interest. The groups were held in university rooms during a break in the trainees’ timetable. The topic guide comprised open-ended questions about reasons for entering nursing, what participants looked forward to after qualification and any surprises they had encountered in practice. While the type of questions may have, to an extent, directed the responses, and even though probing questions were asked to encourage elaboration on certain topics, the discussions developed quite independently of the moderator’s active involvement. All group discussions were audio-recorded and transcribed verbatim by the group facilitator.
Psychosocial analysis
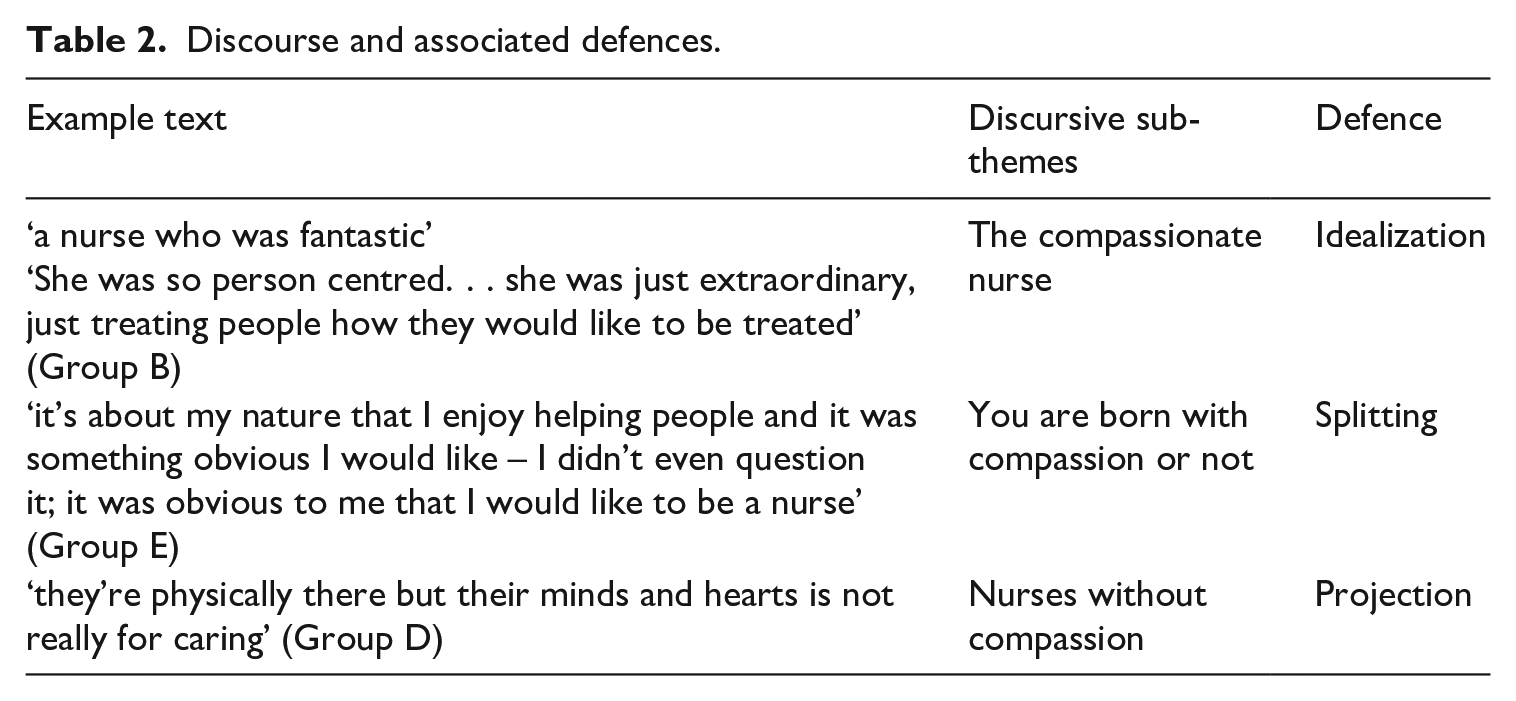
To begin our analysis process, the two authors who had not been involved in collecting the data each familiarized themselves with and inductively coded all the transcripts in order to identify possible key themes (Potter and Wetherell, 1987). All three authors then iteratively discussed this initial analysis to generate new ideas about the dataset and challenge individual analysts’ taken-for-granted interpretations. In this process, we noticed that the talk dealing with assertions of caring appeared central and encapsulated key aspects of the trainees’ occupational socialization. Thus, words and reference to terms such as ‘caring’, ‘compassionate’, ‘empathy’ and ‘relationships’ were seen together to make up the overarching theme of ‘compassion’. We focused on this in the continuing analysis and considered it to be made up of three distinct but interconnected sub-themes. We label these: ‘The compassionate nurse’, which includes talk that refers to ideas about what a compassionate nurse is; ‘Being born with compassion’, which includes talk about compassion being an in-born trait; and ‘Nurses without compassion’, which includes talk about experiences with nurses who lack compassion. The sub-themes are discussed below and are shown in Table 2.
Discourse and associated defences.
Next, we analysed the data organized into these themes following a discourse analytical framework, exploring language use and the discourses drawn on (Wetherell et al., 2001). This was the basis for a detailed analysis of how the participants constructed situated accounts and their social functions and intended actions (Potter and Wetherell, 1987). However, after reading and re-reading the focus group data, individually and together, we found the language to be often ‘uneasy’, apprehensive and accusatory. The apparently highly charged language pointed at something emotional. When people feel threatened, they unconsciously defend themselves by investing in certain discourses rather than others (Hollway and Jefferson, 2000). We therefore decided to explore the unconscious aspect of the discourse, focusing not only on the content of what was stated, but also on the ways in which it was said. We noted, for example, that the frequent occurrences of exaggerations, sensationalism and hyperbole in the language may point towards unconscious dynamics. Furthermore, repetitions and apparently unmonitored or spontaneously uttered statements indicate something about unconscious emotional life. We paid particular attention to images invoked or the use of evocative language and to inconsistencies within and across statements because these may express the tension between conscious and unconscious thought. Kleinian and Bionian concepts helped make sense of the unconscious and emotional underpinnings of the discursive themes and that may explain why certain discourses may be dominant. Because of the group context and trainees working within teams in their work placements, Bion (1961) seemed particularly helpful. The analysis, therefore, focused on how anxiety and responses to anxiety are interpersonally co-produced and shared within each focus group setting (Gough, 2004: 250). This fits within a systems psychodynamics perspective in which a social defence is seen to require collaboration within and between groups and arises ‘when members of an organization align their personal defences with each other and with the structure and culture of the organization’ (Halton, 2015: location 707). One of the means through which this aligning occurs is through discourse. The unit of analysis was thus the discourse of the group, and not the individuals within it. The debates and arguments held within the groups and the unconscious material were viewed as a result of a collective construction (Bion, 1961) and as co-constructed through the language used by the trainees to talk about themselves and others. The unconscious can itself be viewed as trans-individual (Hook, 2008), which reflects well Bion’s theory of how people within a group may spontaneously develop a ‘shared’ unconscious. While the talk on care and compassion was shared across the groups, the discourse within the groups was arranged in specific unconscious ways, which we highlight below. The quotations in the following were selected for discussion because they are exemplars that most succinctly illustrate the themes and the unconscious dynamics of the focus groups. Other similar passages could have been chosen to make similar points.
Data analysis
The most striking aspect of all the focus groups talk was the amount of attention paid to the qualified nurses with whom participants worked. Despite the fact that, in two of the groups, members discussed the harmful effects of high work pressures on how qualified nurses delivered patient care and treated trainees, the dominating talk in most focus groups was the trainees’ highly charged rejection of qualified nurses on the grounds that they were uncaring towards their patients. Three repeated discursive moves can be seen as underlying trainees’ disapproval of qualified nurses: development of ‘the compassionate nurse’ with which the trainees explicitly identified; the assertion of ‘being born with compassion’, their explanation for the presence or lack of caring behaviour; and ‘the nurse without compassion’, with which they associated many of the qualified nurses (see Table 2). We suggest that these can be interpreted respectively as idealization, splitting and projection. For the sake of analytical clarity, we discuss these separately below, but they should be understood as interrelated. All three can be viewed together as reflecting Bion’s basic assumption thinking. In our analysis, we begin by discussing idealization, splitting and projection and as the analysis unfolds, we make links to concepts from Bion. At other points in their talk, we speculate that the trainees’ occasional avoidance of accusatory language and apparent reflection on possible contextual factors point to ‘work group’ mentality.
Basic assumption thinking
Idealization: The compassionate nurse
Across all of the six focus groups, ‘compassion’ represented for the trainees the essential quality that a ‘good’ nurse possesses. The trainees made sense of their roles in relation to both a long-standing occupational discourse and a more recent policy promotion of compassion as a characteristic of ‘high-quality’ care. The idealization of the ‘compassionate nurse’ is reflected in the following passage in which a participant claims that compassionate nurses will prioritize spending time with patients so much so that they will be found working an extra two hours at the end of an all-day shift:
You can see the ones that cared and the ones that didn’t at the end of a shift, after a 12-hour shift. The ones that cared will still be there for the next two hours, writing out paperwork cause they’ve taken time to sit down and feed each patient and talk to them and make sure that everything they are receiving is what they want and need, whereas the ones that literally collect the pay cheque, done all the notes and their bag on their shoulder all ready to go, whether the handover’s finished or not.
Is that a common experience? [. . .]
They’ll take the extra time out of their hours as opposed to being, ‘well it’s 7 now, I’ve got to go home’. They’ll go, ‘well it’s 7.30, I haven’t finished my notes yet’. They’ll sit down and do them for an hour. (Group D. Mixed adult and mental health nurse trainees, 2014)
The rhetorical strategy is to draw an account of the behaviour of nurses who ‘care’ and differentiate them from those who do not, and this is presented as derived from direct observation (‘you can see’) – which makes the claim more credible – rather than from personal assumption. Those who care and those who do not are generalized without offering specific examples, which creates a vague account, and could be a discursive attempt to prevent others from offering counter-arguments (Edwards and Potter, 1992). The compassionate nurse is presented as someone who maintains an overwhelming commitment to the humanity of every patient to ‘make sure that everything they are receiving is what they want and need’ and this humanity overrides any consideration for normal working hours that might concern a less than ideal nurse. The exaggerated nature of these statements (‘the ones that cared will still be there for the next two hours’) suggests that the ideal nurse – while, as proposed below, informed by professional discourse – is to an extent the construction of imagination (Gough, 2004), suggesting the influence of the unconscious defence mechanism of idealization. Another participant, in a different group, linked the ideal nurse with an imagined historical professional past:
Me personally, from my experience, I’ve met good like, you know, sisters that are competent and really, really nice, but I’ve noticed that people that tend to be nicer to patients are sometimes newly qualified ones.
And it’s that whole, what nursing originated from – you were supposed to be understanding the patients, you’re supposed to be comforting, you’re supposed to be that person that patients feel that relationship with – that’s what nursing originated from, so if you’re a nurse who’s not nice but competent otherwise, then it doesn’t really correlate with why nursing started in the beginning. (Group F. Adult nurse trainees, 2016)
Here again a binary construction of the ‘good’ and the ‘bad’ nurse is created by Participant 4 who is making reference to qualified nurses as the bad ones (see below the section on splitting). The use of the term ‘from my experience’ is an acknowledgement that their observation may not be generalized to describe all nurses, and hence could be viewed as a ‘rational’ standpoint (Gough, 2004), one that could be more aligned with a work group mentality because it accepts complexity. However, the inflated language (‘sisters that are competent and really, really nice’) reveals the emotions and the process of idealization which underlies the apparently rational stance. Participant 3 corroborates the statement by Participant 4 by referring to the historical portrayal of the ‘understanding’ and ‘comforting’ nurse. The trainees in this study draw on this ideal as a moral trait that all nurses are ‘supposed’ to have. They talk less about compassion and care as something that drives their interest in the nursing profession or as significant in the effective execution of nursing tasks (Pedersen and Roelsgaard Obling, 2019), and more about it being an imperative and a trait that nurses inherently possess or not. This reflects the dogmatic and stereotypical thinking that characterizes the basic assumption state. As shown below, this entails splitting off the idealized nurse from the ‘bad’ nurse.
Splitting: Born with compassion
The dominant position across nearly all groups was that good nursing is related to one’s ‘natural personality’; one either has compassion or not, regardless of circumstances. There is a stark split between the ‘good’ nurse who is born with compassion and the ‘bad’ nurse who does not ‘have’ it. The following exchange presents a binary construction, which disregards organizational and situational (or any other) factors that may shape behaviour:
Um, I think for the nurses who are good, are quality nurses, I think it comes down to them enjoying the job. If it’s something that fits them and their personality naturally, it tends to make the work easier, more manageable, that’s what I believe.
Cause sometimes, it’s within your nature as well, like, if you’re forcing it when you’re burnt out, it will shine through. . .
Can you say a bit more what you meant by ‘in your nature’?
Yeah, I think it’s just down to you yourself, like some people, it’s just within their nature to be a caring person and just to love people and some people, it’s not like you have to pretend to be caring if that makes sense or kind of force it, that’s what I think.
I think that’s why when the proposal came up some few months ago about letting people go to healthcare assistant for a while [work as healthcare assistants before nurse training] –
– oh yeah
– to teach compassion. I’m sorry; you can’t teach compassion, it has to be in you. You can develop it but if you don’t have it, you don’t have it.
I’ve seen a lot of carers without compassion so that, if they’ve done that before, it’s not going to change it. (Group B. Mental health nurse trainees, 2013)
Being a good nurse is presented here as innate. This exchange splits off the idealized nurse from the demonized uncompassionate nurse and this is developed collectively. Participant 5 begins by emphasizing that ‘good’, ‘quality nurses’ manage better because of their ‘personality’. Participant 6 adds that it is ‘within their nature to be a caring person’. Others then augment this process of splitting by stating that it is not possible to ‘teach compassion’. By corroborating each other’s points, a sense of consensus is constructed. The emotional current within this group discussion is epitomized in the statement ‘I’m sorry’ by Participant 2, which expresses a sense of confidence in one’s correctness and an emotional investment in the ‘you can’t teach compassion’ narrative, despite (perhaps consciously) acknowledging that ‘you can develop it’. Ironically, this same participant later attempted to provide a different perspective and referred to shortage of staff and burnout as causes of lack of compassion: Participant 2: Well, on paper, nurses are supposed to be compassionate, they’re supposed to have empathy, be sensitive, caring and all that, but do we have all these qualities in one person, to be able to be called a good nurse? That is another question. (Group B. Mental health nurse trainees, 2013)
This statement was met first with silence, and then immediately after, the group returned to the ‘born with compassion’ discourse by someone reporting on an experience with a nurse without compassion. This collective process of splitting occurs alongside ‘dependency’ basic assumption thinking (Bion, 1961): it is of importance to the group to remain as a group that collectively demonizes qualified nurses. This thinking enables them to position themselves as good nurses while projecting outward the voiced fear of Participant 2 that in fact it may not be possible for all the idealized qualities listed to be present in one person. In order to maintain this position, Participant 2’s words are effectively dismissed with a lack of response followed by a change of subject, thereby denying any possibility of acknowledging a group member’s move into the work group mentality and so disrupting the links with other group members, suggesting the operation of dependency thinking. The dependency on the group to remain as a group is achieved. In other words, the insistence, within most of the focus groups, that compassion is something that is either present or not in a person suggests that the participants may not concede, in front of each other and the facilitator, any trace of the work group mentality with recognition of the possibility that they themselves might lack compassion. The emphasis put on care and compassion in the discussion makes it hard for any trainee to admit that they may have other – less ‘positive’ – feelings when carrying out their work with patients and to discuss the difficulties they may themselves experience in enacting compassionate care in practice. Instead, the ‘unwanted’ aspect of nursing was split off and projected onto the qualified nurses (see Petriglieri and Stein, 2012)enabling the trainees to maintain a basic assumption thinking.
Projection: Nurses without compassion
The accusatory discourse on the ‘uncompassionate’ nurse, prevalent across most of the groups, could be viewed as a form of projection that may ease the pain associated with an aspect of trainees’ selves that may be rejected, such as not having compassion. The following discussion which occurred early in one group in response to a question about motivation for joining the profession was characterized by strong criticism of qualified nurses:
… you tend to notice bad practice –
yeah
– or bad communication or no empathy, so it was right when we were in there doing our Access course. . . that it was, that it started to niggle at me, like well, I don’t want to be like that, I want to change the system, albeit whether that’s going to happen is another story for after, but yeah, so it’s also seeing bad and poor practice that’s inspired me to definitely push to get onto the degree [course]. Hmm.
Does anybody else have that?
yeah
Oh, nearly everybody
Yeah, I was definitely– it’s seeing, you know, old school nurses who can’t be bothered, they’re biding their time until their pension comes up [general laughter]. Yeah, that’s what it is, that’s what it is! They think they know better than the rest, you know and it’s looking at those, it’s I don’t want to be like that. . . (Group C. Mixed adult and mental health nurse trainees, 2014)
‘Bad and poor’ practice, such as one which involves ‘no communication’ and ‘no empathy’, is projected onto the ‘old school nurses’ (‘I don’t want to be like that’) who are also presented as detached from their work (waiting to retire) and arrogant. The strong language (‘they think they know better than the rest’) connotes unconscious emotions, possibly anxiety (Gough, 2004) or even envy. The laughter from the group indicates an outward appearance of collective complicity (and perhaps enjoyment) in such constructions. The statement made by the above participant that their motivation is to change the system (mentioned also in other focus groups) alludes specifically to a change in the bad practice of qualified nurses. There are some inconsistencies in this sentence. It could indicate an acknowledgement of alternative structural meanings and, hence, a move towards a work group mentality. However, it could also be interpreted as an unreflectively uttered claim, with unconscious grandiose motives, which is tempered with the admission that ‘whether that’s going to happen is another story for after . . .’. The incomplete sentence raises the question of whether the participant (privately) acknowledges, even for a brief moment, that they may not be able to, in the long-term, practise compassion after all, and hence could be a potential transfer to a work group mentality.
The ‘othering’ of qualified nurses – which appears throughout most of the focus groups – often takes the form of personal attacks centred on the qualified nurses’ age or moral failure. In all cases, the repulsive and amoral behaviour does not belong to oneself, but to the other:
Yeah, they have to do [the job] rather than they want to do it.
Is that what people think?
yeah
Yeah, I think once they’ve done the job for a long time, you know, it’s lack of compassion, lack of empathy, sympathy, you know, they don’t care. They just come in and do the job and go home. But what they have to think, first of all, empathy is the first thing. They have to put themselves into the patient’s shoes. Nobody wants to be in hospital, you know, lying down sick, and treated like they are nobody with a loss of dignity and respect.
It’s not necessarily the older nurses who’ve been there a long time, it’s also you get the younger nurses as well who have been there not so long and they still just sort of plod along and they’re like, I’m doing my job – why should I do other stuff, you know what I mean? (Group C. Mixed adult and mental health nurse trainees, 2014)
Participants 6 and 10 jointly construct an image of nurses with a ‘lack of compassion’. Participant 6 indicates that this attitude exists also in some (other, not me) younger nurses too, and aims to gain the agreement of rest of the group (‘you know what I mean?’) and succeeds as no one challenges this portrayal. In this apparent process of group-think (Janis, 1972), participants are unwilling to disrupt the consensus; a manifestation of basic assumption thinking and an unconscious wish to maintain the group as a group. There is at the same time a mechanism of a fight/flight basic assumption state of mind, in which, collectively, qualified nurses are attacked and blamed by the trainees for not being compassionate. Sometimes participants describe themselves as standing out against poor practice, despite workload demands provoking vulnerability. This is illustrated in the following exchange in which Participant 12 begins by professing that she opposed an instruction by a qualified nurse to not take too much time with a dementia patient:
Ok, for example, an elderly lady who has dementia and, of course, you know when I said to the nurse, Can I feed her? Oh, she said don’t take too much time with her – if she doesn’t want to eat, don’t bother. So, and I said, you know, you just have to take time you know cause especially with dementia people. . . and sometimes it annoys me cause you are trying to communicate with the patient, um getting to know each other so she will be comfortable with me and then suddenly [the nurses] will just like snap Oh, come on, just, you know, hurry up, you don’t have to stay the whole for long time, you have to, you know, do this, blah, blah, so it sometimes, it’s quite frustrating.
– It’s time, time, it always comes down to time – there’s never enough time. It’s not that they don’t want to do it – some don’t want to – it’s not that they don’t want to do it, it’s that they literally don’t have the time to sit there and talk to the patient and there’s a lot of assumption going on, like they don’t want to eat, it’s fine. . . but no-one’s bothered to ask them if they like it or not – it’s always time. No one ever has enough time.
I find that often you see when somebody’s got sort of a lack of empathy as a nurse, you tend to see that they will do the basic tasks of being a nurse but not necessarily the sort of everything that you would assume a nurse does as part of that – like sort of talking to the patient, sort of getting to know them, sort of making sure that they understand what’s going on [. . .]. (Group D. Mixed trainees, 2014)
After Participant 12 complains about a ‘bad’ nurse, Participant 3 says that workload pressure can frustrate the motivation of qualified nurses: ‘it’s not that they don’t want to do it’, although she immediately tempers this suggestion ‘some don’t want to’. This statement is ignored by the group. The next person speaking (Participant 2) does not develop this argument and returns to the ‘lack of compassion’ narrative. The discussion in this group then continues with the passage presented earlier where Participant 4 idealizes nurses who ‘cared’ by claiming they would stay two hours extra after the end of their shift. An attempt to provide an alternative perspective – one that is less paranoid-schizoid – is blocked by the other participants.
Work group mentality: Acknowledging contextual factors and eruption of more complex emotions
In the above examples, opportunities to develop the talk towards a work group mode of thinking were ignored by the group. In two of the focus groups, however, trainees did not appear to engage uniformly in idealization, splitting or projection, and there was a discussion about the influence of workload or stress on nurses’ behaviour. This is one example:
[. . .] do you have any sense of how the bad ones got bad and the good ones got good?
I think it depends on personality and the manager as well – if manager don’t care.
I think it’s a lot about staffing –
Yeah, maybe it’s not about personality but it’s about that they are overwhelmed with work, so they are very nice people and very helpful, but, because they are overwhelmed by work and they are very stressed, they are just don’t really bother about having us students, because they have six other patients to look after, so they don’t have time to look after the student. (Group E. Adult nurse trainees, 2016)
Participant 5 begins by suggesting that nurses’ bad behaviour is not merely a result of individual personalities, but that the nature of management may also play a role. Participant 2 picks up on this idea of a structural cause and highlights lack of resources, something which Participant 4 then develops by referring to workload issues. Participant 4’s statement that qualified nurses ‘don’t have time to look after the student’ suggests a position of vulnerability and perhaps there is a feeling of envy for the care given to the patients and a sense of being abandoned by the mentors who are, after all, supposed to care for the trainees as well as patients (‘six other patients’). The discourse in this focus group is different from the other groups as such, more complex feelings are momentarily expressed. After the statement above by Participant 4, Participant 3 continues by recounting an experience where her belief about apparent poor behaviour on the part of a mentor was modified by an understanding that work pressures and management action might explain her behaviour: Participant 3: . . . then the manager gave my mentor less patients and we came back early, so I think it’s with the overload of the work as well and my mentor turned out to be really nice at the end, because she was really stressed and she didn’t want to talk with me initially, because she was stressed with her patients and she didn’t want to discuss anything, so I was kind of scared to ask any questions to her, although I was with her but we were just like focusing and running all around, but then, when they gave her time, she turned out to be a really nice person and explaining, [laughs] so I was thinking, no it’s not you, it’s the work, so I think it’s about management at some point. (Group E. Adult nurse trainees, 2016)
The discussion here goes beyond constructing behaviour as simply reflecting an inner quality of caring or its lack. The sense of being abandoned by mentors is here again allowed expression (‘she didn’t want to talk with me initially’). The talk is less antagonistic and accusatory, more reflective and there is an acknowledgement of the realities that nurses experience at work. This, therefore, is akin to a work group mentality as the interaction is characterized by an exchange of ideas and a creative dialogue, rather than consensus around blame. The more paranoid-schizoid communications usually start by a participant bringing up experiences of bad practice and others joining in. In contrast, in Group E above, a participant begins by providing an ambivalent viewpoint and the discussion mostly continues in that fashion.
Discussion
As an individualizing solution to system-level problems, the idealization of compassion transfers blame of inadequate services onto nurses (Fotaki, 2015). As a consequence, the ideal influences trainee nurses’ valuations of their own and others’ behaviour (see Handy and Rowlands, 2017). Our first contribution is to the compassion literature (Pedersen and Roelsgaard Obling, 2019; Simpson et al., 2014), which is to explore the unconscious reasons for the persistence of the ideal of compassion, despite practical difficulties healthcare workers experience in exercising compassion in their work. We show that the process of idealization, splitting and blame is internalized by trainee nurses and unconsciously protects them from anxiety evoked by the vulnerability of their position as those who need to gain access to the profession and when being unable to conduct compassionate nursing work, because of practical difficulties.
In idealization, an object is overvalued to protect it from the anxiety that originates from the persecutory ‘bad’ object (Klein et al., 1952), which is, in the trainees’ imagination, the ‘uncaring nurse’. This mechanism of splitting enables trainee nurses to deal with the anxiety brought about by the conflict between being expected to be compassionate in their work, and possibly struggling with this in practice, by projecting the ‘bad’ non-compassionate nurse on to the qualified nurses. Projection is often involved in the process of scapegoating (Eagle and Newton, 1981). When people feel anxious at work, ‘they project their sense of blame and failure outward, often scapegoating the person they must cooperate with to reduce the uncertainty they face’ (Hirschhorn, 1988: 3). When making sense of their role, trainee nurses may face aspects of themselves that do not fit that role – such as hatred of patients who make demands on them or envy for the care given to them by their mentors – especially if workplace pressures increasingly impede holistic patient-centred care. The idealization of compassion by trainees could thus be viewed as partly a defence against envy (Stein, 2000). They may then assign unwanted characteristics of the nursing role – ones that appear less compassionate – to others, which can help to reduce the anxiety of not feeling ‘compassionate’ and support an understanding of self that is appropriate, as dictated by the compassion discourse. As such, our study suggests that the expectation to identify with ideals perpetuated by social or policy discourse provokes nurses to project unacceptable aspects onto others with whom they work closely (see Petriglieri and Stein, 2012: 1220). In line with research showing how policy changes may trigger antagonistic relationships at work (Fraher, 2017), we found that the compassion discourse produces othering, and obstructs the development of a sense of alliance with qualified nurses, despite the qualified nurses being exposed to similar obstacles and difficulties as the trainees. The lost opportunity for solidarity contributes to a perpetuating of the scapegoating of nursing failures for wider system problems and policy failures.
Furthermore, we hypothesize that a basic assumption mindset, which involves a defence of feeling blamed for having emotions that do not correspond to the ideal of compassion, may have implications for the way nurses conduct their work with patients. Compassionate care can become a surface-acting emotional labour, contributing to further burnout, as suggested by research on compassion-fatigue (Sinclair et al., 2017). Indeed, Menzies did not appear to foresee that ‘compassion’ could become an idealized discourse that serves to promote a certain type of subjectivity, nor that it could be used to blame nurses for healthcare failures. Recently, the emphasis put on the depressive position – which underpinned Menzies’ suggestions for change in the hospital she studied – has been criticized by Gerard (2020), who argues that the desire to address the needs of others – which is promoted by the compassion discourse – if taken too far, can lead to a ‘compulsion to repair’, imposing excessive guilt on workers for having any needs of their own. In our study, trainees were largely unable to properly express their own needs to be taken care of. However, the defences encouraged by the compassion discourse (splitting, projection and idealization) are paranoid-schizoid, rather than depressive because they focus on protecting the nurses themselves, rather than on care for the patient. The compassion agenda may therefore be counterproductive. Enforcing care for patients in nurses may have the opposite effect if existing system-wide defences that blame nurses for failures are not challenged (see Hyde and Davis, 2004).
As a consequence, rather than emphasizing compassion, educators should consider ‘consciousness-raising’ among trainees regarding the organizational and political realities of work in the profession. We hypothesize that this will help develop the work group mentality among trainees. In our focus groups, there are examples of attempts to articulate a work group mode of thinking in each group, some of which misfire (in the context of the dominance of the basic assumption mentality), but in two of the groups the perspective manages to ‘hold’ to some extent. There is nothing about the composition of these groups that suggests an explanation for this difference. The explanation may be in the group dynamics: often, the way in which the discussions started seemed to have set the trend for the remainder of the discussion in the groups. However, the basic assumption position governed the talk across all of the six focus groups. Splitting and idealization prevent people from listening to those who continuously question unrealistic strivings (Fotaki and Hyde, 2015). This is a function of the basic assumption group in which ‘a struggle takes place to suppress [an alternative] idea because it is felt that the emergence of the new idea threatens the status quo’ (Bion, 1961: 155). Basic assumption thinking is against learning and development and it inhibits discussion about the variety of complex feelings involved in nurses’ work. Investment in the compassion discourse and rejection of alternative ways of understanding organizational realities protect trainees from anxiety (Ford, 2010), but distract them from consciousness of structural problems, such as lack of resources, that appear to thwart the provision of adequate services, or even reference to the commonly accepted phenomenon of ‘burnout’ (Fearon and Nicol, 2011). Idealization allows a continued belief in compassion as the solution to healthcare failings, both at a policy level and among nurses, which may prevent policy makers from taking responsibility, leaving individual nurses to carry the burden. A strengthened work group mentality would help healthcare professionals to work through the variety of complex feelings they experience at work, to focus on what they require to conduct their day-to-day tasks and to demand adequate resources and structures that enable them to practise patient-centred, compassionate care.
Basic assumption thinking, on the other hand, does not enable critical review of wider organizational failings, including government policy regarding the NHS (Fotaki, 2006). This serves the government’s interests, using nurses as a scapegoat for their own failed healthcare policies. Our research therefore confirms claims in the literature that social defences often provide protection for the powerful (Petriglieri and Petriglieri, 2020). This leads us to our second contribution, which is to emphasize how less powerful occupational groups, such as trainee nurses may adopt defences that underpin dominant organizational policy and that further disadvantage those groups. While existing literature points to the role of affect and emotion in perpetuating powerful organizational discourses (e.g. Baker and Kelan, 2019; Fotaki et al., 2017; Kenny, 2012) and, in particular, to how social defences allow protection for the powerful (Petriglieri and Petriglieri, 2020), there is little discussion of how this dynamic is manifested in – and sustained through – unconscious processes in less powerful groups. We demonstrate that analysing focus group data may help to explore this. We struggled to find published focus group studies that draw rigorously on Bion’s theory to explore unconscious processes in focus groups (see Smit and Cilliers, 2006 for one exception), despite the emphasis on groups in organizational systems psychodynamics research. Our psychosocial analysis suggests how unconscious group dynamics among ‘lower status’ members of organizations contribute to the maintenance of systemic and dominant social defence mechanisms. Participants did not simply view the focus group as a setting in which their task is to answer questions regarding a certain topic, but they interpreted it as an opportunity to defend against the anxiety produced by the compassion discourse by, ironically, perpetuating it, and hence strengthening the defence mechanisms established by those in power. This exposes how defences may be shared by both ‘lower status’ groups and those in power, in ways that benefit the latter and disadvantage the former. Given the emphasis on the team-based nature of many occupations, it is pertinent to investigate, following Bion, how unconscious and emotional dynamics function through interaction within groups, and the role of these processes in maintaining or contesting dominant discourses. This helps to gain an understanding of the extent to which less powerful groups may come to share the defences of those in power, even if the defences protect against different anxieties or emotions in the two groups. By considering how discourses may intersect with unconscious dynamics that are co-produced in lower status groups, we gain a better grasp of how power may operate through preventing work group thinking in those groups.
A limitation of our research is that we could not determine if the reason that the work group mentality took hold in two groups was a result of the workplace experiences or the characteristics of the specific participants in those groups. Hence, future research should take into consideration the highly complex relation between the discourses expressed in focus groups, demographic characteristics, the nature of the work that participants do and the organizations they are placed in. Data on demographics and organizational placements are important for a more rounded psychosocial analysis, furthering understanding of how situated work experience and embodied differences, including gender and other ‘identity’ markers, may shape the ways in which trainees interact with the compassion discourse. We suggest that this is an opportunity for future research.
Footnotes
Acknowledgements
We wish to thank Anne-Wil Harzing for her invaluable support and guidance in writing this article. We are also grateful to Tim Freeman for his constructive feedback on earlier versions of the article. Furthermore, we are thankful to the Associate Editor Jackie Ford and three anonymous reviewers for their insight and comments, which helped to improve the article significantly.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.