
Abstract
Recent debates in healthcare have emphasized the need for more respectful and responsive services that meet patients’ preferences. These debates centre on patient experience, one of the most critical factors for measuring healthcare performance. In exploring the relevance of patient experience key questions need answers: what can managers or supervisors do to help improve the quality of healthcare? What is the role of employees? Addressing these questions, this study examines whether perceived supervisor support (PSS) promotes patient experience through a serial mediation involving perceived organizational support (POS), and positive employee outcomes such as engagement, involvement and advocacy. Using two-wave data from the British National Health Service, we show that PSS is strongly associated with POS, which in turn improves engagement, involvement and advocacy among employees. PSS also has a positive indirect influence on patient experience through POS and advocacy; but the indirect paths involving engagement and involvement are not supported. We offer useful guidance on how healthcare employers can support employees towards improving the quality of services rendered to patients.
Keywords
Introduction
As one of the largest sectors in the service industry, healthcare plays a vital role in modern societies. This role has many facets, including job creation, social welfare and the delivery of efficient care to individuals, families and communities. Nevertheless, healthcare systems face enormous challenges (e.g. an ageing population, rising healthcare expenditure, health and social inequalities) that remain at the forefront of public debates (Goedhart et al., 2017). A key priority in these debates concerns the need to improve patient experience, or the overall quality of respectful and responsive healthcare services as reported by patients (Doyle et al., 2013). Patient experience is increasingly recognized, alongside clinical performance and safety, as a critical measure of healthcare performance (Doyle et al., 2013; Murrells et al., 2013; Price et al., 2014). Academic and policy reports have outlined useful ways to improve patient experience, yet one pertinent issue remains conspicuously absent: the role of managerial support and the implications for employees’ healthcare delivery. Evidence suggests that employees are more likely to perform well when immediate managers or supervisors are perceived as being supportive (see Kirrane et al., 2017), but how relevant is this to debates around patient-centred care?
The concept of managerial support has generated a great deal of interest in non-healthcare settings, given its centrality to job resource theories (Bakker and Demerouti, 2007) and psychologically healthy workplaces (Parker and Price, 1994). When assessed from employees’ perspective, support from an immediate manager or supervisor stipulates the notion of perceived supervisor support (PSS: Kirrane et al., 2017; Saks, 2006). PSS refers to the extent to which employees perceive that their immediate managers, acting as agents of the organization, value and care for their well-being (Eisenberger et al., 2002). It has been associated with shared benefits for both employees (e.g. job satisfaction, commitment and work engagement) and the organization (e.g. productivity, reduced staff turnover and lower sickness absence rates) (Eisenberger et al., 2002; Kurtessis et al., 2017; Riggle et al., 2009; Saks, 2006). Despite these benefits, the links between managerial support and healthcare outcomes have received scant attention in the research literature. We lack adequate insights on how PSS might influence patients’ experience of healthcare quality, nor the underlying mechanisms for such effects. This indicates an important theoretical and empirical gap that should be explored systematically.
The present study seeks to fill this gap, looking at the mechanisms through which PSS might influence one of the most important performance outcomes in healthcare (i.e. patient experience). The goal is to determine whether PSS improves patient experience via its impact on another aspect of support: perceived organizational support (POS). POS represents employees’ shared perceptions about the employing organization’s favourable actions towards their well-being (Eisenberger et al., 1990; Kirrane et al., 2017; Riggle et al., 2009; Saks, 2006; Vardaman et al., 2016). POS has benefits in its own right, but also as a mechanism for workplace effectiveness (Kurtessis et al., 2017). As outlined in social exchange theory, adequate levels of organizational support create a conducive work environment, characterized by mutual trust, respect and cooperation between employees and management (Saks, 2006). This work environment inspires a sense of obligation, on the part of employees, to invest themselves both physically and emotionally in ways consistent with organizational goals. In other words, POS and corresponding employee outcomes may serve as underlying mechanisms between managerial support and enhanced healthcare quality.
We explore the nature of these mechanisms, focusing on three employee outcomes – engagement, involvement and advocacy. These outcomes constitute the British National Health Service’s (NHS) framework on employees’ role in improving patient experience (Admasachew and Dawson, 2011; Fletcher and Robinson, 2014; West and Dawson, 2012). Accordingly, the salient preconditions for enhanced patient-centred care are employees’ work motivation, their sense of work empowerment and willingness to engage in advocacy behaviours on the organization’s behalf (Admasachew and Dawson, 2011; Fletcher and Robinson, 2014). The NHS framework further outlines the importance of support for healthcare professionals (including over 1.5 million workers employed by the British NHS): thus, as long as healthcare workers are adequately supported to do their jobs, they will reciprocate through positive attitudes and behaviours, leading to better patient-centred services. Using this framework, we examine three serial mediation processes linking PSS to patient experience – a motivational indirect path (involving POS and engagement), an empowerment indirect path (involving POS and involvement) and a behavioural indirect path (involving POS and advocacy).
Our study enriches the literature in several notable ways. It provides deeper insights on how supportive resources at work might engender positive work attitudes and behaviours among employees, and ultimately improve patient experience – the latter being a fairly neglected domain in management research. We know from existing research that supportive practices at work offer a range of social, economic and psychological benefits; yet, the direct implications for patients and health service users are not fully understood. The present study addresses an important research gap, highlighting useful ways to support employees and improve the quality of services rendered to patients. This framework cuts across different, but relatively important, research disciplines such as human resource management (i.e. managerial and organizational support), organizational behaviour (work attitudes and behaviours) and healthcare management (patient experience). The goal is to generate insights on the most critical mechanisms linking perceived support at work to better outcomes for both employees and patients. Using two-wave, multi-source, repeated cross-sectional data from the British NHS, we apply robust empirical analyses on a set of complementary hypotheses (Figure 1).
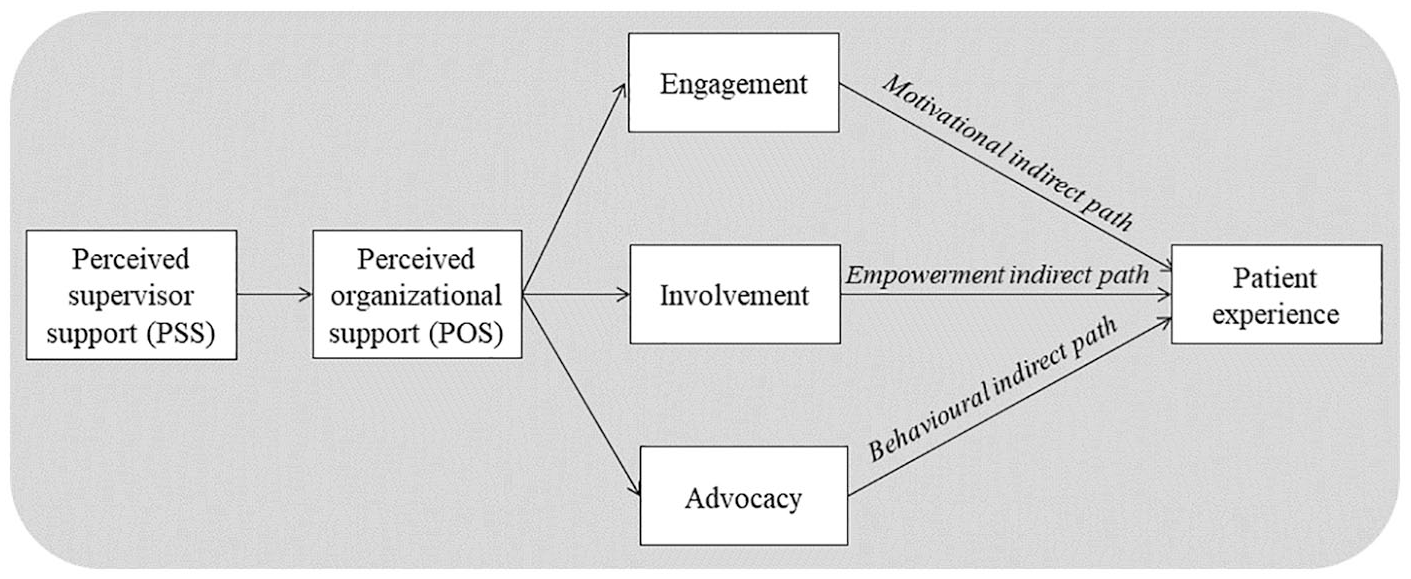
Serial mediation model linking PSS to patient experience via POS alongside engagement, involvement and advocacy.
Research background
It is acknowledged that managerial support improves employee morale and performance (Kirrane et al., 2017; Riggle et al., 2009; Rofcanin et al., 2019; Vardaman et al., 2016). Organizations are thus putting greater emphasis on practices that demonstrate adequate levels of concern for employees’ health, well-being and welfare. In public healthcare organizations, such as the British NHS, managerial support includes treating staff fairly, creating effective communication channels between employees and supervisors, helping staff to balance their work and home life and protecting staff from harassment and physical harm. These practices shape patient experience, which is an important proxy for healthcare performance (Doyle et al., 2013; Jenkinson et al., 2002; Murrells et al., 2013). Patient experience is defined as the sum of all interactions, shaped by the organization’s culture, that determine patients’ perceptions across the continuum of services in healthcare (Wolf et al., 2014). It is characterized by a range of factors including reduced waiting time in hospital, prompt and coordinated hospital care, perceptions of safety and physical comfort in hospital and involvement in decisions regarding patients’ care and treatment conditions (Doyle et al., 2013).
One of the most influential models for explaining supportive workplace relationships is social exchange theory (Byrne and Hochwarter, 2008; Eisenberger et al., 1990; Gould-Williams, 2007; Kurtessis et al., 2017; Ogbonnaya, 2019). At its core lies the assumption that positive actions taken by the organization, or its agents, in favour of employees can elicit positive workplace attitudes and behaviours. Such actions may be interpreted as the organization’s ‘goodwill’ towards the workforce, or perhaps, as a sign that the organization intends to establish high-quality employment relationships with employees (Eisenberger et al., 1990). Consequently, employees are inspired to exercise discretionary effort, engage in proactive behaviours and act in ways consistent with the organization’s strategic goals. The principle of social exchanges is premised on the norm of reciprocity, according to which people will respond favourably if actions performed by others are perceived as being of greater benefit (Gould-Williams, 2007). To put it differently, employees will likely respond favourably if actions performed by their immediate managers or supervisors are perceived as being supportive.
Drawing on social exchange theory, we examine the mechanisms via which PSS might influence patient outcomes. We argue that supportive managerial actions shape employees’ perceptions about the organization’s level of supportiveness towards them. This in turn stimulates employees’ desire to reciprocate through positive workplace attitudes and behaviours. In this context, the British NHS identifies three relevant employee outcomes (Admasachew and Dawson, 2011; MacLeod and Clarke, 2009; Purcell, 2014). Engagement represents employees’ feelings of enthusiasm or being completely immersed in their job. It includes the types of emotional states described by Schaufeli et al. (2002), such as intrinsic motivation, dedication and absorption at work. Involvement represents employees’ sense of empowerment, their ability to show initiative at work and their capacity to make improvements happen in their work area. Advocacy represents employees’ sense of pride in, and endorsement for, the quality of services offered by the healthcare organization. It stipulates employees’ willingness to promote the organization’s service standards and recommend the organization as a good healthcare provider. We investigate how PSS might improve patient experience through POS and these three outcomes, respectively.
Linking PSS to POS
Much has been written about managerial support and its role in promoting favourable employees’ perceptions about organizational support (Campbell et al., 2013; Eisenberger et al., 2002; Lapalme et al., 2009; Saks, 2006; Yoon and Lim, 1999). It is argued that employees interpret supportive managerial actions as indicative of the organization’s benevolence towards the workforce, and also as key factors influencing employees’ positive feelings towards the organization. Such feelings are reinforced by employees’ tendency to personify their organization or ascribe human-like characteristics to it (Eisenberger et al., 1986; Kurtessis et al., 2017). Thus, if employees perceive their immediate managers as being supportive and caring, they might respond favourably – such as thinking more positively about the organization as a whole (Eisenberger et al., 2002; Yoon and Lim, 1999). The reverse is also true as unpleasant managerial actions towards employees may result in negative perceptions about organizational support.
In a study of 343 social workers, Campbell et al. (2013) showed perceptions of organizational support depend largely on employees’ access to supportive supervisory relationships. Accordingly, positive supervisor–subordinate interactions strengthen employees’ morale, as well as general perceptions that the work environment is conducive for personal growth and development. In such an environment, employees feel more secure, confident and reassured that their interests are safeguarded by the organization (Yoon and Lim, 1999; Kurtessis et al., 2017). Similarly, in healthcare, research has shown that workers who feel valued and cared for by their supervisors may attribute such feelings as emanating from the organization itself (Ogbonnaya et al., 2018; West and Dawson, 2012). Supervisory support, particularly when it aids employees to deal with stressful situations at work, stimulates healthcare workers to view their employer as one that is genuine and committed to ensuring a safe work environment for workers. Along these lines, we might expect a positive relationship between PSS and favourable employees’ perceptions about organizational support.
Hypothesis 1: PSS is directly and positively associated with POS.
POS and positive employee outcomes
Extant research has reported strong links between POS and positive employees’ attitudes and behaviours (Byrne and Hochwarter, 2008; Eisenberger et al., 1990; Kurtessis et al., 2017; Riggle et al., 2009; Rofcanin et al., 2019). The more employees perceive their organization as being supportive, the more likely they are to report better levels of satisfaction, engagement, motivation and in-role performance. Research in this area invokes social exchange theory, the idea that supportive work environments engender respectful and cooperative employer–employee relationships (Gould-Williams, 2007). Employees in such environments are viewed as valuable assets whose contributions to performance are valued and appreciated by the organization (Eisenberger et al., 2002). Thus, as part of the positive social exchange process, employees may feel obliged to repay the organization by investing themselves, both physically and cognitively, when performing their duties (Ogbonnaya, 2019).
Drawing on social exchange principles, Saks’ (2006) study of 102 Canadian workers showed positive links between POS and employee engagement towards the job and the organization. Saks defined job engagement as being highly absorbed in one’s role, and organization engagement as one’s level of active involvement in organizational activities. Similarly, Byrne and Hochwarter’s (2008) study of full-time employees showed positive links between POS and employee outcomes such as organizational citizenship behaviours, in-role and extra-role performance. Byrne and Hochwarter described POS as a key resource that promotes employees’ work experiences through positive employer–employee relationships. These relationships, in turn, stimulate employees’ deeper sense of involvement and dedication to their role, leading them to discretionary actions and behaviours. By extension, we argue that POS would have positive effects on other workplace outcomes such as employees’ sense of empowerment and advocacy behaviours. Specifically, POS should improve not only employees’ motivation at work, but also their sense of empowerment, and willingness to promote the organization and the quality of its healthcare services.
Hypothesis 2: POS is directly and positively associated with: (a) engagement; (b) involvement; and (c) advocacy.
In the subsequent sections, we explore PSS’ impact on patient experience via a motivational indirect path (involving POS and engagement), an empowerment path (involving POS and involvement) and a behavioural path (involving POS and advocacy). The premise is that supportive actions taken by managers in favour of employees will convey positive cues as to whether the organization values and cares about employee well-being (Ogbonnaya and Messersmith, 2019; Saks, 2006). Employees perceive these cues as indicative of the organization’s goodwill, prompting favourable reactions among employees (Eisenberger et al., 2002; Kurtessis et al., 2017). In healthcare, such favourable reactions increase employees’ overall performance, and ultimately, patients’ access to appropriate care.
Motivational indirect path via POS and engagement
Psychologically engaged workers are generally more enthusiastic about their jobs, and therefore well positioned to perform well (e.g. Harter et al., 2002; Karatepe, 2013; Salanova et al., 2005). Engaged workers are also more likely to prioritize organizational goals, such as offering high-quality services to customers and organizational clients (Harter et al., 2002). In exploring these assumptions, Salanova et al. (2005) reported positive effects for employee engagement on both job performance and customer loyalty. Salanova et al. emphasized the importance of organizational support in promoting employees’ emotional attachment towards the job, with positive implications for the quality of services rendered to customers. Similarly, Karatepe (2013) analysed employee engagement as an important mediator between human resource management and extra-role customer service (defined as the capacity to serve customers beyond the formal requirements of the job). Karatepe stressed the importance of such practices in creating a productive work environment where employees feel inspired to respond adaptively and thoughtfully towards customers’ needs.
Notwithstanding, data from the British NHS have shown mixed effects. Although some studies have reported positive links between work engagement and patient outcomes (e.g. Wake and Green, 2019; West and Dawson, 2012), others, particularly those looking at the psychological facets of engagement (e.g. Ogbonnaya and Valizade, 2018; Ogbonnaya et al., 2018) reported marginal effects. Ogbonnaya et al. (2018) explained that the correlations between psychological engagement and patient outcomes are generally weak, and in most cases, partly distorted by patients’ own beliefs and high expectations for quality care. In spite of this, there are logical reasons to expect a positive impact of engagement on patient experience. One example is that engaged workers are generally motivated to perform their duties well (Schaufeli et al., 2002). Another example is that engaged workers tend to express a greater sense of dedication towards ensuring that patients are treated with both dignity and respect (West and Dawson, 2012). Going by these examples, we predict a positive relationship between workplace support and employee engagement, and in turn, improved patient experience.
Hypothesis 3: PSS will positively influence patient experience through a serial mediation involving POS and engagement.
Empowerment indirect path via POS and involvement
As with engagement, employee involvement has received considerable attention in the literature, both in terms of human resource management and organizational support practices. Job involvement increases employees’ capacity to directly influence their work tasks and responsibilities (May et al., 2004; Wood et al., 2012). Employees are able to show initiative in their role, engage in positive decision making and accomplish meaningful organizational goals (May et al., 2004). In the healthcare literature, employee involvement is generally discussed under the umbrella term of ‘structural empowerment’ – defined as having the ability to mobilize information and resources through opportunities to learn and grow (Goedhart et al., 2017; Laschinger et al., 2003; Metcalf et al., 2018). Empowerment in this sense means giving employees the responsibility and autonomy to manage their own jobs and make decisions about their own work priorities (Goedhart et al., 2017). Empowered healthcare workers are thus able to perform their day-to-day duties in a professional fashion, which is essential for health services that meet high-quality standards.
In their study of respiratory care physicians, Metcalf et al. (2018) examined the importance of organizational support in promoting employees’ sense of empowerment and improving patients’ experience of care. Metcalf et al. described organizational support as a vital resource needed for workers to respond both adaptively and proactively when confronting issues that may arise during patient care delivery. Similarly, Laschinger et al. (2003) discussed nurses’ sense of empowerment in relation to supportive resources at work. Laschinger et al. argued that nurses are generally more efficient in offering safer healthcare services to patients if they are empowered and supported to do their jobs. Along these lines, we argue that a supportive healthcare environment, where employees are empowered, cared for and respected, will encourage better patient outcomes. Employees will be able to perform their jobs at optimal levels, such as solving problems as soon as they are identified and offering the quality of services that makes a difference to patients.
Hypothesis 4: PSS will positively influence patient experience through a serial mediation involving POS and involvement.
Behavioural indirect path via POS and advocacy
Of the three employee outcomes, advocacy is possibly the least studied in management research. Much of what we know about advocacy comes from the marketing literature, where employee advocates are described as ‘brand ambassadors’, ‘brand maniacs’, ‘brand champions’ and ‘brand evangelists’ (Morhart et al., 2009: 123). Advocacy is conceptually different from, but closely related to, service-orientated commitment and organizational citizenship behaviours (Bettencourt et al., 2001). It represents employees’ willingness to undertake voluntary actions on the organization’s behalf, such as generating positive publicity for the organization’s brand image and recommending the organization as a good provider of high-quality services (Bettencourt et al., 2001; Miles and Mangold, 2004; Morhart et al., 2009). In the healthcare context, advocacy encapsulates employees’ confidence in, and endorsement of, the organization’s healthcare standards (Wake and Green, 2019; West and Dawson, 2012). Employee advocates may, for example, endorse the quality of services rendered by the hospital or recommend the hospital if a friend or relative needed treatment (Fletcher and Robinson, 2014). Notwithstanding how advocacy is measured or conceptualized, it is an important determinant of good customer (or patient) service performance.
Morhart et al.’s (2009) study of 269 frontline employees highlights the role of organizational support, particularly a leader’s commitment to encouraging and motivating his/her followers, in shaping advocacy behaviours among employees. Supportive leader–follower relationships create a proper alignment between employees’ interests and the organization’s service priorities. This encourages greater employee trust and confidence in the organization, prompting employees to endorse the organization’s customer-oriented branding efforts (Morhart et al., 2009). Similarly, research in the healthcare context has linked different types of workplace support to advocacy behaviours among workers. West and Dawson (2012), for example, explained that employees will express a deeper sense of appreciation for organizational values and uphold the organization’s healthcare standards when they feel adequately supported. Echoing this, Wake and Green (2019) noted that employee advocates are themselves quite keen and motivated to deliver high-quality care to patients. Such workers envision long-term employment relationships with the organization and therefore invest their time and effort towards ensuring better levels of healthcare services.
Hypothesis 5: PSS will positively influence patient experience through a serial mediation involving POS and advocacy.
Methodology
The study uses two-wave (2010 and 2011), repeated cross-sectional data from the NHS Staff Survey, matched with data from the 2011 NHS Adult Inpatients Survey. The NHS Staff Survey provides information on employees’ working conditions across different acute, mental health, ambulance services and community health NHS Trusts. NHS Trusts are, by definition, legal entities or organizations authorized to manage social, health and hospital services for the communities or locations they serve. A single Trust thus comprises multiple clinics, departments and health service centres, serving a specified local area. Data were gathered by self-completion questionnaires distributed to a random selection of employees in participating Trusts, including doctors, nurses, midwives and allied health professionals of different age and ethnic backgrounds. Around 164,916 questionnaires from 386 NHS Trusts were completed and returned in 2010. The median number of respondents in sampled Trusts was 446, and the range was 44 to 833. The 2011 survey includes 134,967 completed questionnaires from 368 NHS Trusts. The median number of respondents in the sampled NHS Trusts was 425, and the range was 28 to 678.
Data for the Adult Inpatients Survey are collected annually to assess patients’ perspectives on the quality of care and treatment received in hospital. The survey covers a wide range of issues such as the experience of coordinated care, physical and emotional comfort in hospital, quality of interaction with healthcare professionals, quality of care and treatment received, and waiting time in hospital. As with the Staff Survey, data for the Adult Inpatients Survey include respondents of different age, ethnic and socio-economic backgrounds. Around 70,863 patient respondents from 161 NHS Trusts completed the survey in 2011, with a response rate of 53%. The median number of respondents in sampled NHS Trusts was 850, and the range was 502 to 855.
We applied a systematic data management strategy to accomplish two main objectives: (1) to minimize artefactual covariation due to common method bias; and (2) to match and merge multiple sources of data appropriately. The first objective was achieved using multiple sources of data: measurement items for PSS were derived from the 2010 NHS Staff Survey, whereas measurement items for the mediators (i.e. POS, engagement, involvement and advocacy) were from the 2011 version of the survey. This provides necessary temporal separation between the predictor and mediators (Podsakoff et al., 2003). To further alleviate concerns of common method bias, data from the 2011 NHS Staff data were split randomly into two groups, so that half of the respondents provided information on POS and the other half provided information on engagement, involvement and advocacy, respectively. As patient experience was measured from a different source, the 2011 Adult Inpatients Survey, we ensured adequate temporal and methodological separation between the predictor and outcome.
The second objective was achieved by aggregating all measurement items as mean scores at the NHS Trust level. This crucial step was performed with the intent of matching and combining data from the different sources into a unified dataset. Prior to data aggregation, Intraclass Correlation Coefficients 1 and 2 (ICC1 and ICC2) were tested to verify interrater reliability among individual respondents. ICC1 values for the 2010/2011 NHS Staff Surveys ranged from 0.02 to 0.06, suggesting less than 6% of variability in employees’ responses was accounted for by each individual in the survey (Bliese, 2000: 356). ICC2 values ranged from 0.60 to 0.95, suggesting that employees were relatively consistent in terms of their collective workplace experiences. Similarly, ICC1 values for the 2011 Adult Inpatients Survey ranged from 0.03 to 0.08, whereas ICC2 values ranged from 0.61 to 0.96. All ICC values in the current study fall within the recommended thresholds for justifying data aggregation (LeBreton and Senter, 2008). Once data were aggregated and merged into a unified dataset, the final sample size was 161 NHS Trusts.
Measures
Perceived supervisor support (PSS) was measured by five items from the 2010 NHS Staff Survey (see details in Table 1). All items are consistent with those from previous research (e.g. Eisenberger et al., 2002; Kirrane et al., 2017; Saks, 2006).
Study variables, observed items, Cronbach’s alpha (α), composite reliability (CR), average variance extracted (AVE) and response scale.
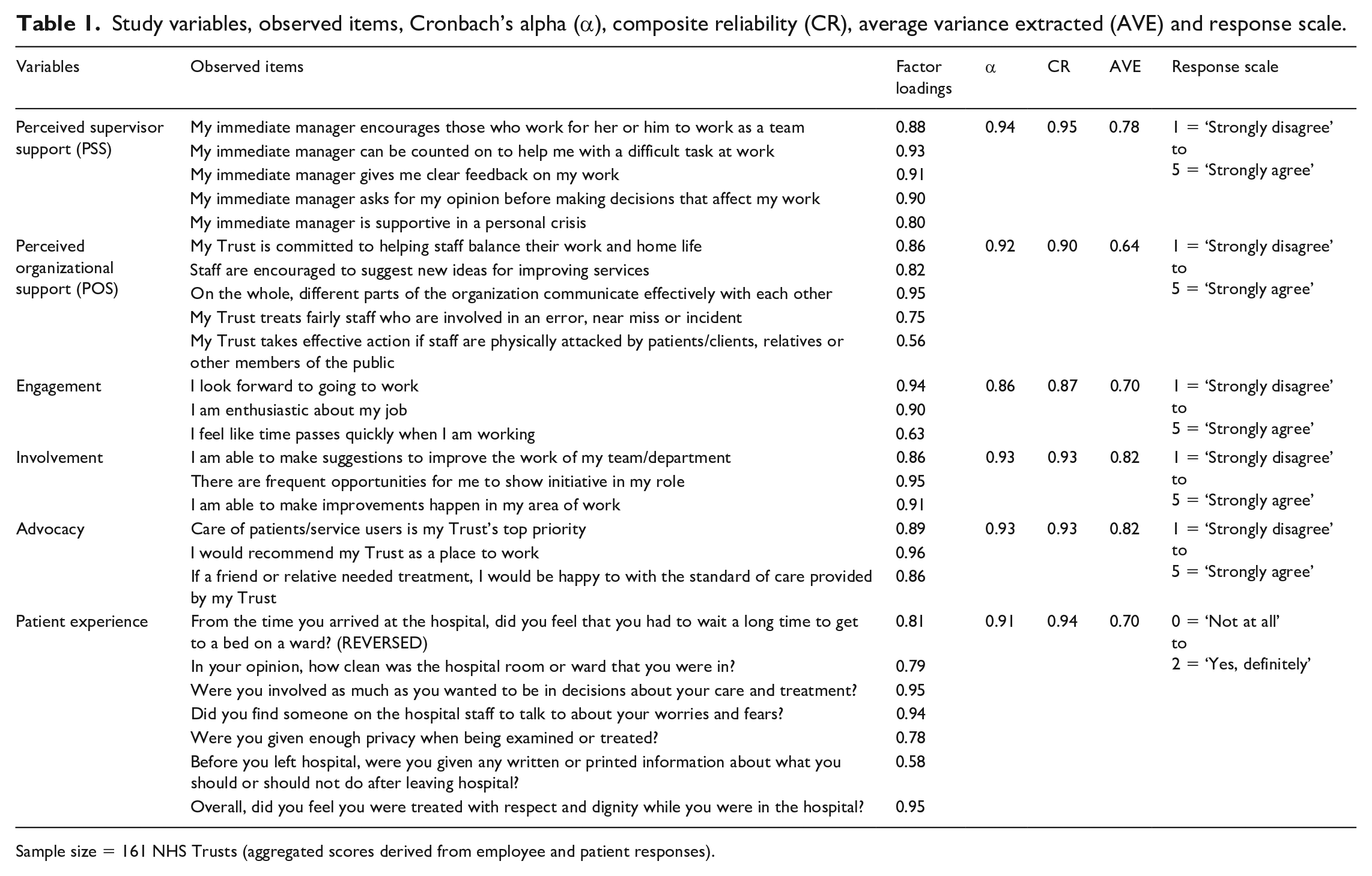
Sample size = 161 NHS Trusts (aggregated scores derived from employee and patient responses).
Perceived organizational support (POS) was measured by five items from the 2011 NHS Staff Survey, selected based on the precedents in previous organizational support research (e.g. Eisenberger et al., 2002) and adapting these to the British NHS’ context (see details in Table 1).
Engagement was measured by three items from the 2011 NHS Staff Survey, measured on a five-point Likert scale (see Table 1). These items were derived from Schaufeli et al.’s (2002) work engagement scale, but adjusted to match the British NHS’ context (Admasachew and Dawson, 2011).
Involvement was measured by three items from the 2011 NHS Staff Survey. These items assessed three key issues: whether employees were able to make suggestions to improve their work, whether employees had frequent opportunities to show initiative in their role and whether employees were able to make improvements happen in their area of work (see Table 1).
Advocacy was measured by three items assessing the degree to which employees would recommend the Trust as a place to work, or as a place to receive high-quality care (Admasachew and Dawson, 2011; Fletcher and Robinson, 2014; Purcell, 2014; West and Dawson, 2012). These items were from the 2011 NHS Staff Survey.
Patient experience was measured by seven items from the 2011 Adult Inpatients Survey, measured along the lines suggested by previous studies (e.g. Doyle et al., 2013; Jenkinson et al., 2002; Murrells et al., 2013). These items cover aspects of both relational care (e.g. patient experience of emotional support and involvement in decisions regarding patients’ health and treatment) and functional care (e.g. patient experience of privacy and reduced waiting time).
Control variables: in line with previous studies (e.g. Ogbonnaya and Valizade, 2018; Ogbonnaya et al., 2018; Powell et al., 2014), we applied the following control variables to the current analysis: patients’ length of stay in hospital; patients’ age (four age bands, reference category is ‘66 years and above’); patients’ gender (reference category is female); hours worked by employees (reference category is ‘less than 30 hours’); extent of employee contact with patients (reference category is ‘no contact’); and occupational group (10 categories, reference category is ‘registered nurses and midwives’). These variables have strong implications for patient experience: for example, long working hours are potential stress factors that increase the likelihood of errors and near misses in hospital care, whereas employees’ face-to-face interactions with patients could potentially affect the quality and efficiency of healthcare services. All control variables were measured as aggregated proxies at the NHS Trust level (see Table 1).
Analytical procedure
Data were analysed by Structural Equation Modelling (SEM) with latent variables, using the Mplus software program (version 7.1). The estimator of choice was the robust maximum likelihood (MLR) estimator, which adjusts for measurement errors in large-scale survey data (Asparouhov and Muthén, 2006). The measurement component of the model comprised six latent variables, including PSS, POS, engagement, involvement, advocacy and patient experience. Overall goodness-of-fit was adequate: X2 = 459.92; df = 280; p-value < .001; Root Mean Square Error of Approximation (RMSEA) = 0.06; Comparative Fit Index (CFI) = 0.96, Tucker-Lewis Index (TLI) = 0.95, Standardized Root Mean Square Residual (SRMR) = 0.08. An alternative one-factor measurement model was estimated to determine whether all six variables were reducible to a single latent construct. This model failed to fit the data adequately: RMSEA = 0.22; CFI = 0.44; TLI = 0.39; SRMR = 0.16; thus, confirming that the latent constructs are discrete and less likely influenced by common method bias. A two-factor measurement model – one factor for PSS and POS, and the other for engagement, involvement, advocacy and patient experience – also failed to fit the data adequately: RMSEA = 0.24; CFI = 0.34; TLI = 0.28; SRMR = 0.18.
The structural component of the analysis examined a serial mediation model whereby three mediators (engagement, involvement and advocacy) were influenced by another mediator (POS). The analysis comprised the following set of equations: (1) the latent construct for POS was regressed on the latent construct for PSS; (2) the latent constructs for engagement, involvement and advocacy were respectively regressed on the latent constructs for PSS and POS; (3) the latent construct for patient experience was regressed on the latent constructs for PSS, POS, engagement, involvement and advocacy, and the control variables; and (4) a syntax to generate parameter estimates for indirect effects. This syntax is based on the product-of-coefficient method (MacKinnon et al., 2007), where each indirect effect represents the product of three regression coefficients: (1) between the predictor and first mediator; (2) between the first and second mediator; and (3) between the second mediator and outcome.
Results
Table 2 shows that the bivariate correlations among study variables were mostly consistent with expectations. PSS was positively correlated with POS, the three employee outcomes and patient experience. POS had similar positive correlations with these variables. Involvement and advocacy were positively correlated with patient experience, whereas engagement was not significantly correlated with patient experience (r = 0.08, p > .05).
Means, standard deviations (SD) and bivariate correlations among study variables.
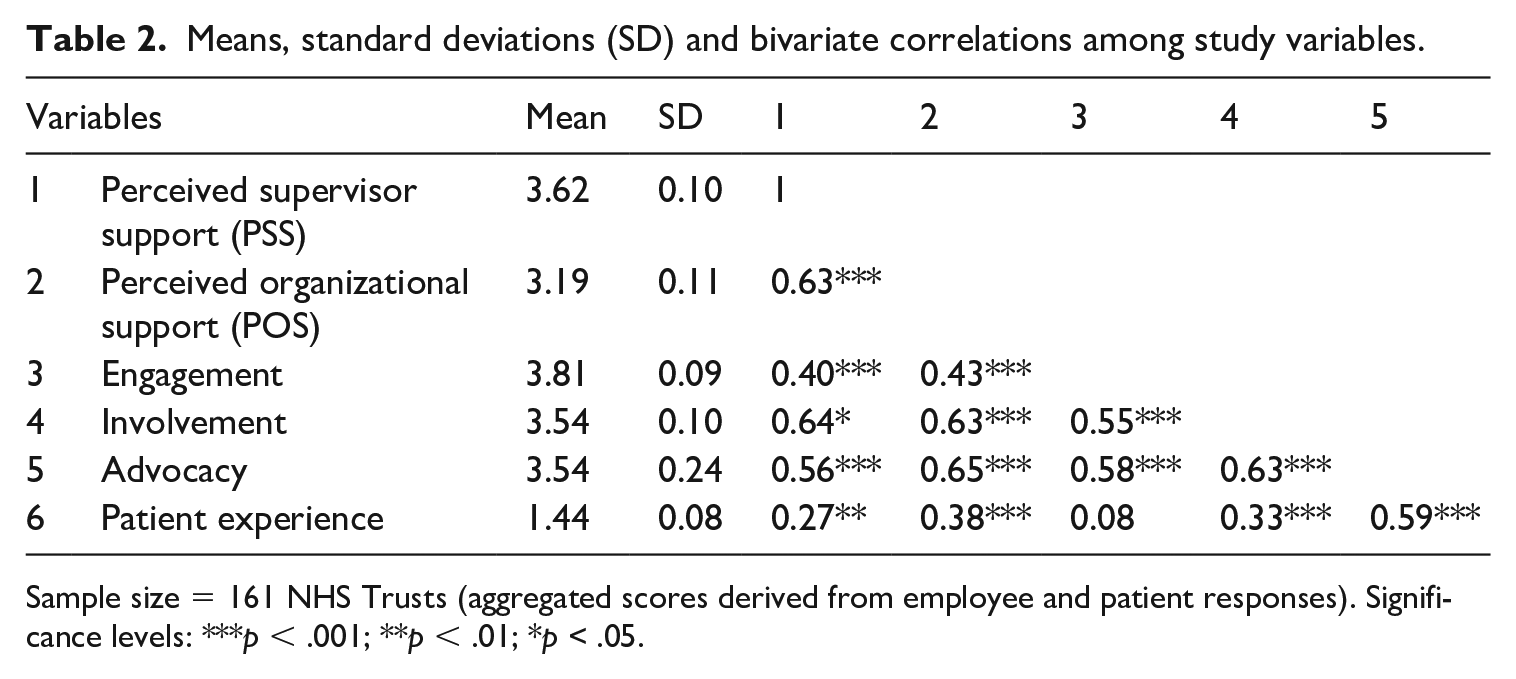
Sample size = 161 NHS Trusts (aggregated scores derived from employee and patient responses). Significance levels: ***p < .001; **p < .01; *p < .05.
Table 3 reports parameter estimates for all direct and indirect effects in the model. As predicted, PSS had a direct positive relationship with POS (β = 0.25, p < .001), indicating full support for Hypothesis 1. This positive result echoes prior claims that adequate levels of support from an immediate manager encourage employees to reflect more positively about organizational actions towards the workforce. Hypotheses 2a, 2b and 2c, concerning the direct relationships between POS and the three employee outcomes, were also fully supported by the data. Parameter estimates for these relationships were both significant and positive: engagement (β = 0.24, p < .001), involvement (β = 0.20, p < .001) and advocacy (β = 0.43, p < .001). Our study therefore corroborates the social exchange principle that employees are likely to respond with desirable attitudes and behaviours if they feel adequately supported and cared for.
Results showing all direct and indirect effects.
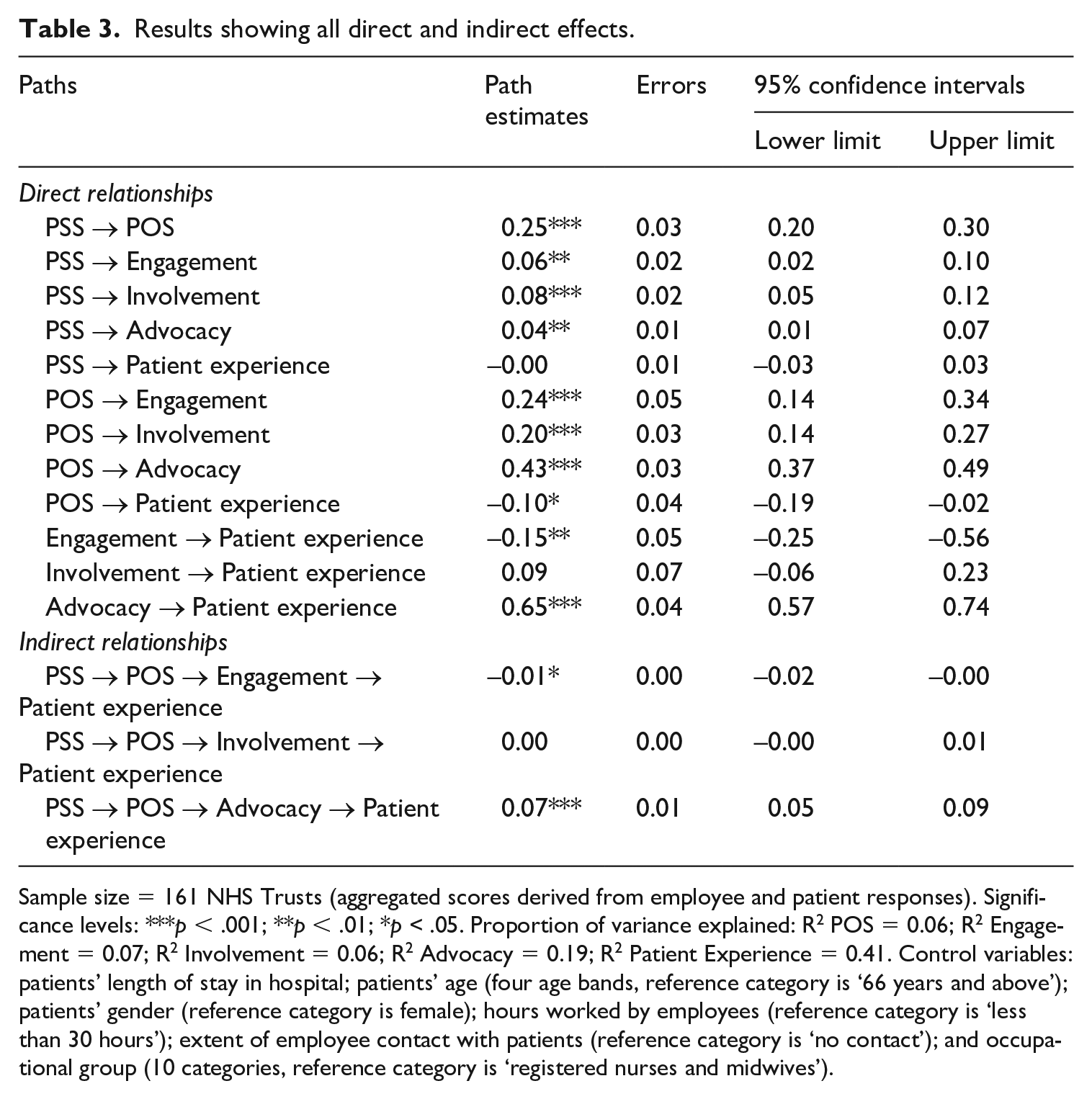
Sample size = 161 NHS Trusts (aggregated scores derived from employee and patient responses). Significance levels: ***p < .001; **p < .01; *p < .05. Proportion of variance explained: R2 POS = 0.06; R2 Engagement = 0.07; R2 Involvement = 0.06; R2 Advocacy = 0.19; R2 Patient Experience = 0.41. Control variables: patients’ length of stay in hospital; patients’ age (four age bands, reference category is ‘66 years and above’); patients’ gender (reference category is female); hours worked by employees (reference category is ‘less than 30 hours’); extent of employee contact with patients (reference category is ‘no contact’); and occupational group (10 categories, reference category is ‘registered nurses and midwives’).
As reported in Table 3, PSS (β = −0.00, p = .96) and involvement (β = 0.09, p = .23), respectively, had no significant direct effects on patient experience, whereas POS (β = −0.10, p < .05) and engagement (β = −0.15, p < .01), respectively, had significant and negative effects on patient experience. These results may be interpreted to suggest that PSS, POS, engagement and involvement do not, in themselves, engender any significant improvements in patient experience. In contrast, advocacy (β = 0.65, p < .001) had a significant and positive direct relationship with patient experience. Thus, compared to engagement and involvement, advocacy satisfied the relevant precondition to act as a mediator between PSS and patient experience.
Hypothesis 3 suggests that PSS will positively influence patient experience through a serial mediation involving POS and engagement (i.e. a motivational indirect path). As reported in Table 3, this hypothesis was not supported as the observed indirect effect was significant and negative (αβ = −0.01, p < .05). This unexpected result indicates a type of inconsistent mediation (MacKinnon et al., 2000) or suppression effect (Conger, 1974). Suppression effects are said to occur when the respective effects of the predictor and mediator on the outcome cancel each other, causing either a full, or perhaps partial, distortion in the overall predictive relationship. In the present analysis, this distortion may have resulted from a relatively strong POS–engagement relationship, versus a relatively weak engagement–patient experience path.
Hypothesis 4, concerning the positive influence of PSS on patient experience via a serial mediation involving POS and involvement, was not supported. The parameter estimate for this indirect path was positive but not statistically significant (αβ = 0.00, p = .25). Thus, as with the motivational indirect path, PSS may not necessarily influence patient experience through the empowerment indirect route. In contrast, the parameter estimate for the behavioural indirect path, involving POS and advocacy, was significant and positive (αβ =0.07, p < .001). This result supports the prediction that PSS will improve patient experience via both employees’ positive perceptions of organizational support and advocacy behaviours (full support for Hypothesis 5).
Discussion
The idea of managerial support continues to enjoy widespread popularity among scholars. Several studies have documented its role in shaping favourable employees’ dispositions towards the organization, as well as employees’ positive attitudes and behaviours at work. Nevertheless, there have been fewer insights on the nature and outcomes of managerial support practices in the healthcare context. Inspired by social exchange principles, the current study examined the mechanisms via which PSS might improve patient experience, focusing on POS and three employee outcomes (i.e. engagement, involvement and advocacy). Using two-wave data from the British NHS, we report differential effects between these outcomes and patient experience.
We found a strong, positive relationship between PSS and POS. This positive relationship echoes previous reports that supportive actions by managers encourage favourable employees’ perceptions about organizational support (Eisenberger et al., 2002; Yoon and Lim, 1999). Immediate managers or supervisors are often seen as organizational representatives whose levels of care and support may be interpreted as the organization’s benevolence towards employees. The more employees experience supportive managerial relationships, the more they perceive the organization as being supportive. In addition, we found that POS relates positively to all three employee outcomes – engagement, involvement and advocacy. These positive effects corroborate social exchange principles that employees will respond favourably, with positive attitudes and behaviours, when in a supportive work environment (Saks, 2006). In such an environment, employees perceive positive signals about the extent to which they are valued by either the organization or its agents (in this case immediate managers). These signals are interpreted as the organization’s intent to foster positive employment relationships with the workforce, thereby encouraging positive employee attitudes and behaviours (Ogbonnaya and Messersmith, 2019).
Contrary to expectations, our test for a positive indirect relationship between PSS and patient experience via POS and engagement returned a negative effect; that is, the motivational indirect path from PSS to patient experience was not supported. This rather contradictory result deviates from previous research linking high levels of engagement to better customer service experience (e.g. Salanova et al., 2005). A possible explanation might be due to suppression effects, whereby a relatively weak correlation between engagement and patient experience offsets the impact of managerial support on patient experience (Ogbonnaya et al., 2018). An alternative explanation, perhaps, is the idea that psychological engagement represents one’s feelings (i.e. an affective state of mind), rather than one’s concrete actions. In other words, ‘feeling engaged’ does not automatically imply ‘acting engaged’. Indeed, psychologically engaged workers may feel quite enthusiastic about their job, but this would not necessarily result in positive patient outcomes unless such feelings are backed by concrete patient-centred actions. Ultimately, further research is needed to shed further light on the true nature of these relationships.
Another unexpected finding concerns PSS’ indirect effect on patient experience via POS and involvement (i.e. the empowerment indirect path), which was positive and non-significant. This finding, though with a relatively weak effect size, contradicts previous evidence from both the healthcare (e.g. Goedhart et al., 2017; Metcalf et al., 2018) and non-healthcare (e.g. Wood et al., 2012) contexts. Typically, employee involvement is considered as a vital resource for employees to perform well and make significant improvements happen in their work area. Involvement is also viewed as a major source of employee empowerment (Laschinger et al., 2003), with positive implications for employee performance and ability to help the organization achieve its objectives. Nevertheless, as revealed in the current analysis, involvement could have negligible effects when explored as a mediator between employees’ perceptions of support and patients’ experience of healthcare. We argue that both forms of workplace support, PSS and POS, influence employee involvement significantly and positively; yet, critical questions remain as to whether involvement has significant implications for patient experience.
Of the three employee outcomes examined, only advocacy played a significant and positive role in terms of our proposed behavioural indirect path. Specifically, PSS had a positive indirect relationship with patient experience via POS serially linked with advocacy. This result is expected given prior evidence that employees’ brand-building, extra-role and citizenship behaviours have widespread benefits for organizations (e.g. Morhart et al., 2009). The result also strengthens the relevance of advocacy behaviours in terms of patient-centred care. Because advocacy behaviours entail employees’ appreciation of, and endorsement for, the quality of services offered by the organization, such behaviours encourage employees themselves to render high-quality care that meets patients’ expectations (Fletcher and Robinson, 2014). Thus, we argue that PSS, through its positive effects on both POS and advocacy, represents a key determinant of patient experience. Healthcare employers would be better served by supporting employees, treating them fairly and encouraging their positive behaviours towards organizational goals and values.
Implications for theory
This study offers important theoretical insights. By exploring the PSS–POS nexus and highlighting its significance for both employee and patient outcomes, the study provides a more nuanced understanding of key social exchange principles. In particular, the study illustrates how supportive workplace relationships can be nurtured and translated into more respectful and responsive services for patients. The study thus extends key tenets of social exchange theory beyond the management and psychological disciplines where they are mostly examined. Our results are not only pertinent, but also consistent with Eisenberger et al.’s (1990) core proposition: that immediate managers, or those with supervisory authority over employees, are seen as organizational agents whose supportive actions increase employees’ positive feelings about the organization. Such feelings inspire employees to express higher levels of energy at work, strive to make improvements happen in their work area, and treat patients with dignity and respect.
One impetus for the current research was to establish the various pathways via which workplace support (i.e. support from immediate managers and the organization alike) might improve patient-centred care. In this vein, our results underline the role of PSS in fostering a conducive work environment where healthcare workers feel inspired to provide the quality of services that most patients will appreciate; the caveat, however, is not all employee outcomes contribute significantly to patient experience. In fact, two employee outcomes, engagement and involvement, which have been studied quite extensively in management research, showed little or no positive effects on patient experience; whereas the least studied outcome (i.e. advocacy) had a relatively strong positive effect. Clearly the data examined in the current study cannot provide definitive answers to these inconsistencies, but future research may delve more deeply into the intricate processes through which PSS might influence patient outcomes.
Implications for practice
The present study provides practical guidance on organizational support practices for improving the quality of services offered to patients. The study has shown particularly that positive social exchanges between employees and immediate managers play an important role in ensuring valuable and meaningful services for patients. In other words, when managerial efforts are focused on supporting employees and encouraging them to perform well, this will stimulate employees’ positive perceptions of organizational support, and strengthen the quality of care that patients receive. The key message, therefore, is to recognize that healthcare efficiency may not always arise from further restructuring of healthcare systems (a phenomenon that has, in recent times, characterized the public healthcare sector), but perhaps by strengthening workplace support policies and encouraging positive employees’ perceptions about organizational support. Healthcare employers should examine the nature of such policies, particularly how they can be deployed towards inspiring employees and encouraging high-quality services that make a difference to patients. For healthcare organizations such as the British NHS, where some of these support policies are already in place (e.g. through the Improving Working Lives (IWL) framework), the present study highlights the most important benefits for patients and healthcare users.
Another practical message for healthcare employers is to recognize that certain workplace attitudes and behaviours may not generate optimal effects when aiming to improve healthcare efficiency. Whereas positive employees’ attitudes towards the organization and its values (e.g. advocacy behaviours) are beneficial for patient-centred care, the effects of employees’ affective state (e.g. engagement) and sense of involvement are negligible. This has practical implications for the British NHS where employees belong to different occupational groups (e.g. social care, clerical staff, nursing, housekeeping and technical staff). Crucially, healthcare employers should consider the kinds of support structures available across occupational groups, and in so doing, employ best practices that encourage employees to deliver the quality of services that makes a difference.
Strengths and limitations of study
The strengths of the present study are varied. For example, our use of large-scale, archival data from the British NHS – one of the world’s largest public healthcare organizations – enabled a more comprehensive exploration of different support structures at work and the implications for both employee- and patient-centred outcomes. In addition, our use of well-founded theory, coupled with our robust two-wave analytical strategy, reinforced the overall contributions that we make. Despite these strengths, one source of weakness is the use of aggregated data. Although data aggregation was necessary to ensure appropriate matching and merging of multiple sources of data, and to minimize artefactual covariation due to common method bias, it has important drawbacks in terms of level of analysis (i.e. individual-level theory versus organizational-level methodology). Nevertheless, post-hoc analyses revealed statistical estimates were largely consistent for both aggregated and non-aggregated versions of our data. Another possible study limitation lies in the fact that POS, engagement, involvement and advocacy data were derived from the same survey instrument (i.e. the 2011 NHS Staff Survey). Although we have applied standard statistical procedures in addressing the potential problems of self-reported measures, we advise caution when interpreting our results beyond this limitation.
A natural progression from our study is to examine managerial and organizational support practices in terms of a much wider range of healthcare antecedents and outcomes. Future research may, for example, examine whether advocacy, relative to engagement and involvement, has stronger positive effects on patient safety and mortality rates across different healthcare departments or units. Such research will add value to the organizational support literature and provide deeper insights regarding efficiency and effectiveness of operations in healthcare. Research is also needed to better understand the boundary conditions under which different forms of support might influence employee and patient outcomes. Researchers may, for example, establish whether the impacts of support on employee outcomes are conditional on demographic characteristics such as personality types, educational attainment, gender and age differences. Research in this area will not only inform policy debates, but accentuate the importance of organizational support for a more diverse range of employment characteristics.
Footnotes
Acknowledgements
We gratefully acknowledge the Health Care Management Division of the Academy of Management for recognizing this research with the Outstanding Paper Based on a Dissertation Award at the 78th Annual Meeting.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.