
Abstract
Objective
To evaluate the feasibility of electromyography (EMG)-based human–machine interfaces (HMIs) for high-demand activities such as driving based on performance, cognitive workload, usability, and safety measures.
Background
Upper-limb amputees face challenges in performing everyday tasks, including driving. EMG-based HMIs offer potential solutions, particularly for wrist disarticulated and trans-radial amputee, but their effectiveness in complex tasks like driving requires further investigation.
Method
Nineteen able-bodied participants completed a driving simulation study using an EMG-based HMI, dominant hand, and both hands. Participants performed various driving maneuvers including straight lane driving, overtaking, and 90-degree turns at intersections. Driver performance, cognitive workload (measured by blink rate and subjective measures), usability (USE questionnaire), and safety were assessed.
Results
Using the EMG-based HMI led to higher lane offset and steering angle compared to conventional methods, but demonstrated lower steering entropy in some situations. Cognitive workload was higher for EMG-based HMI, while usability scores were lower. Safety measures were mixed, with EMG-based HMI showing better performance at intersections but lower lane offset and steering angle safety scores overall.
Conclusion
The study highlights both limitations and opportunities presented by EMG-based HMIs in high-demand tasks such as driving. While the system exhibited lower performance in some conditions, it demonstrated potential for controlled driving, particularly during specific maneuvers. The higher cognitive workload and lower usability scores indicate areas for improvement.
Application
The findings provide valuable insights for the development of more effective EMG-based HMIs, supporting future research and clinical trials aimed at enhancing mobility and independence for individuals with upper-limb amputations.
Introduction
About 391,000 people in the United States are currently living with upper-limb loss (Caruso & Harrington, 2024). The loss of upper-limb can significantly affect an amputee’s ability to work, diminishing their independence and impacting their quality of life (Meyer, 2003). These upper-limb amputations can occur at different levels, such as a transradial amputation (or below-elbow amputation), which occurs through the long bones of the radius and ulna, or a transhumeral amputation (or above-elbow amputation), which involves the humerus. Additionally, amputations that occur through a joint, rather than through a bone, are referred to as disarticulations (Jette et al., 2017). For many amputee patients, prosthetic devices are essential for carrying out Activities of Daily Living (ADLs), including tasks such as self-feeding, working, and homemaking (Park, Zahabi, et al., 2024). Despite their critical role, prosthetic devices are often reported as difficult to operate due to their complex control systems, leading to frustration, reduced usage, and in many cases, outright rejection (Engdahl et al., 2015; Montagnani et al., 2015). This highlights the pressing need for more intuitive and user-friendly solutions that can enhance the functionality and accessibility of prosthetic devices, ensuring they are better integrated into users’ lives.
Electromyography (EMG)-Based Human–Machine Interface (HMI)
Among different types of prosthetic controls such as Body-Powered Controls (Muilenburg et al., 1989), Passive Controls (Maat et al., 2018), Hybrid Controls (Cimolato et al., 2020), EMG, or myoelectric, control is one of the most commonly used powered upper-limb prosthetics due to their comfort and naturalness (Tavakoli et al., 2017; Williams, 1990). EMG sensors records the muscle movements from the surface of muscle cells when they are activated (Naik & Nguyen, 2015). EMG-based devices enable more intuitive and precise control, allowing users to perform complex, natural movements with greater ease. However, the performance of EMG-based systems is influenced by factors such as electrode positioning, muscle fatigue, and arm position (Parajuli et al., 2019). Our previous research (Park et al., 2024) investigated classification models for assessing cognitive workload (CW) in EMG-based prosthetic devices when performing ADLs using ocular measures, task performance data, and cognitive performance model (CPM) outcomes. Furthermore, we evaluated different control modes such as direct control (DC), pattern recognition (PR), and continuous control (CC), and their effects on CW and usability in both physical prosthetics settings and virtual reality-based simulations (Park et al., 2023). The findings supported the use of EMG-based prosthetics especially the PR configuration for upper-limb amputees in performing basic ADLs, such as grasping objects and simple motor tasks (Liu et al., 2024; Park et al., 2024). However, there is a need to assess the findings in high-demand everyday tasks such as driving.
In this study, surface EMG signals were acquired using four Delsys Trigno wireless sensors (Delsys Inc, 2003) and placed on the dominant forearm to target the flexor digitorum (FD), flexor carpi radialis (FCR), extensor carpi radialis longus (ECRL), and extensor digitorum (ED) muscles (Park, Berman, et al., 2024). Software including EMGworks® acquisition and Trigno Control Utility provided by Delysis Inc were utilized for EMG signal monitoring in real-time and MATLAB was used to train the pattern recognition (PR) control algorithm. We utilized the PR control configuration (Parajuli et al., 2019) for the EMG-based human–machine interface (HMI) in this study for the following reasons. First, PR control is based on the user’s intent, making it more intuitive and natural for participants compared to other prosthetic control modes such as direct control. This allows for smoother and more efficient execution of tasks, particularly when simultaneous joint operations are required (Liu et al., 2024). Additionally, PR control offers a comparable cognitive demand to more advanced control schemes like continuous control (CC), without the need for complex angle adjustments (Liu et al., 2024). Given the simplicity and user-friendliness of PR, it provided an ideal balance between usability and performance for our EMG-based HMI. In the PR control method, a classifier translates features from multichannel EMG signals into specific motion categories, such as opening/closing the hand or rotating the wrist (extension/flexion) (Liu et al., 2024).
The PR control classifies movement intent based on the patterns of EMG features. In this study, movements were classified into three categories: arm flexion, arm extension and neutral or no movement (Park et al., 2023). Each movement class was held for 5 s, followed by a 5-s rest period, with all movements performed twice. Signals were sampled at 2000 Hz using the Delsys Trigno Control Utility, which applied a hardware-based online band-pass filter (20–450 Hz) during acquisition. Filtered signals were streamed in real time via TCP/IP into MATLAB, where they were segmented into 50 ms sliding windows. A custom feature extraction function was used to compute four time-domain features from each window: mean absolute value (MAV), waveform length (WL), slope sign changes (SSC), and zero crossings (ZC) (Resnik et al., 2018; White et al., 2017). These features were then used to train a Linear Discriminant Analysis (LDA) classifier capable of recognizing user intent in real time. After feature extraction, predicted movement classes were gated using a user-defined EMG intensity threshold and sent to a downstream control client via TCP/IP. This architecture ensured responsive classification with minimal perceptual delay and provided a reliable testbed for evaluation.
Driving
In addition to basic self-care activities, driving plays a crucial role in maintaining independence and mobility, serving as an essential component of daily living for many individuals, particularly in the United States. Whether commuting to work, running errands, or participating in social activities, the ability to drive enables people to lead independent lives. According to Strogatz et al. (2020), 83.3% of rural drivers, and 76.9% of urban drivers rated driving as “completely important” in the US. Studies have highlighted that driving is a complex everyday task requiring perception, attention, learning, memory, decision making, and control (Groeger, 2000; Salvucci et al., 2004). For individuals with upper limb amputations, driving can present significant challenges. Most people with upper limb amputations require at least one vehicle adaptation to drive safely, underscoring the difficulties they face in operating standard controls. To address these challenges, various vehicle adaptations have been developed, such as automatically or electronically operated transmission, knob on the steering wheel, and control devices operable without releasing the steering wheel (Burger & Marinček, 2013). Despite the advancements, these solutions are not always effective, as only 25% of the participants found their prosthetics beneficial for driving according to Datta et al. (2004). Moreover, existing prosthetic devices often require significant cognitive and physical effort from users, making prolonged use challenging (Park & Zahabi, 2022; Park et al., 2023). This highlights the need for more advanced solutions that offer greater functionality and ease of use. Some studies have employed EMG-based prosthetics, such as Myo armband and surface-EMG, to perform basic driving maneuvers in driving simulators, including tasks such as making a U-turn (Nacpil & Nakano, 2020) and changing lanes (Nacpil et al., 2019; Wang et al., 2021). However, these studies focus on very basic driving maneuvers, which do not fully represent the complexity and uncertainty of real-world driving such as navigating through traffic and intersections, and overtaking other vehicles.
Research Gaps and Objectives
While the previous studies have highlighted the potential of EMG-based prosthetics in simplified driving maneuvers such as changing lanes, limited research has been conducted to study the feasibility of EMG-based Human–Machine Interfaces (HMIs) for driving in more realistic scenarios. Driving in the real world often involves not only basic/operational vehicle control tasks such as controlling vehicle speed, performing steering actions, and negotiating curves, but also tactical tasks associated with driving such as overtaking moving vehicles and negotiating intersections (Walker et al., 2015). Our research seeks to bridge this gap by incorporating both operational and tactical tasks in more realistic driving scenarios to better evaluate the feasibility of EMG-based HMIs in terms of driver performance, cognitive workload, safety, and usability and compare it to conventional methods (hand steering) with dominant hand and both hands.
In the context of this study, driver performance refers to the ability of a driver to efficiently, and accurately operate a vehicle tailored to context-specific driving conditions or environments, as reflected by objective metrics such as mean velocity deviation, lane offset, steering angle, and steering entropy (Shahini et al., 2024). Likewise, cognitive workload refers to the perceived and physiological mental demands placed on the driver while completing the driving tasks, assessed in this study using the Driver Activity Load Index (DALI) questionnaire and pupillometry measures (Shahini et al., 2024). Safety is defined as the driver’s capacity to maintain stable control and avoid adverse events, as reflected by measurable thresholds in velocity (e.g., 40 ± 8 km/h), lane offset (e.g., within ±0.3 m), and steering behavior (e.g., within ±2°, with low reversal rates and yaw rate error) (Bowers et al., 2010; Cao et al., 2021; Fitch et al., 2009; Gordon et al., 2009). Finally, usability refers to how useful, easy to use, easy to learn, and satisfying the EMG-based human–machine interface is for participants, as measured using the USE questionnaire (Park et al., 2023).
Evaluating cognitive workload and usability is essential because the EMG-based HMI introduces a fundamentally different mode of interaction compared to traditional driver controls. Rather than relying on mechanical input (e.g., steering wheels), users generate control signals through isometric muscle contractions, a process that can be less intuitive and more cognitively demanding. Such control is influenced by factors such as muscle fatigue, signal stability, and the user’s ability to maintain consistent muscle activation. By assessing cognitive workload and usability, we ensure that the interface is not only functional but also practical, learnable, and comfortable for real-world use.
Research Hypothesis
List of Hypotheses.
Although the broader goal of this work is to support individuals with upper-limb loss, particularly those with wrist disarticulation and trans-radial amputations, this study uses able-bodied participants as a first step toward system evaluation. This approach is consistent with prior EMG-based HMI research that leverages the preserved musculature of able-bodied individuals to model and evaluate control strategies applicable to trans-radial users. Previous studies have demonstrated that such early-stage testing can provide meaningful insights into performance, workload, and usability characteristics (Merad et al., 2018; Park et al., 2023), and supports informed system adaptation for clinical testing in subsequent phases.
Method
Participants
Nineteen healthy participants (8 males, 11 females) were recruited for the study (Age: M = 25.9 years; SD = 7.1 years) with an average daily driving time of 97.5 min. The sample size was estimated using the G*power software (Faul et al., 2007) with an
Apparatus
Delsys Trigno EMG sensors
The EMG-based HMI used in this study was implemented using four Delsys Trigno wireless sensors placed on the dominant forearm, targeting the flexor digitorum (FD), flexor carpi radialis (FCR), extensor carpi radialis longus (ECRL), and extensor digitorum (ED) muscles (Figure 1). The design of the EMG interface was guided by several key considerations. First, it was developed with wrist-disarticulated and trans-radial amputees in mind, who typically retain sufficient forearm musculature for surface EMG control (Grushko et al., 2020; Resnik et al., 2018). This informed the selection of targeted muscles, which are commonly preserved and provided functionally distinct signals. Second, a pattern recognition (PR) control scheme was employed, offering more intuitive and user friendly control, particularly for tasks requiring graded input and simultaneous muscle activation (Liu et al., 2024; Parajuli et al., 2019). The PR control classifies movement intent based on the patterns of EMG features. Movements were classified into three categories: arm flexion, arm extension, and neutral or no movement (Figure 1). Third, the design was optimized for driving task’s demand, ensuring reliable signal output during fine motor control, quick directional inputs, and stable steering under both predictable (intersections) and dynamic (overtakes) scenarios. Finally, it was designed for feasibility in early-stage evaluation with able-bodied subjects, allowing effective testing of the interface without prosthetic hardware while maintaining relevant control dynamics. EMG sensors placement and arm positions: (a) Neutral position, (b) Flexion, (c) Extension.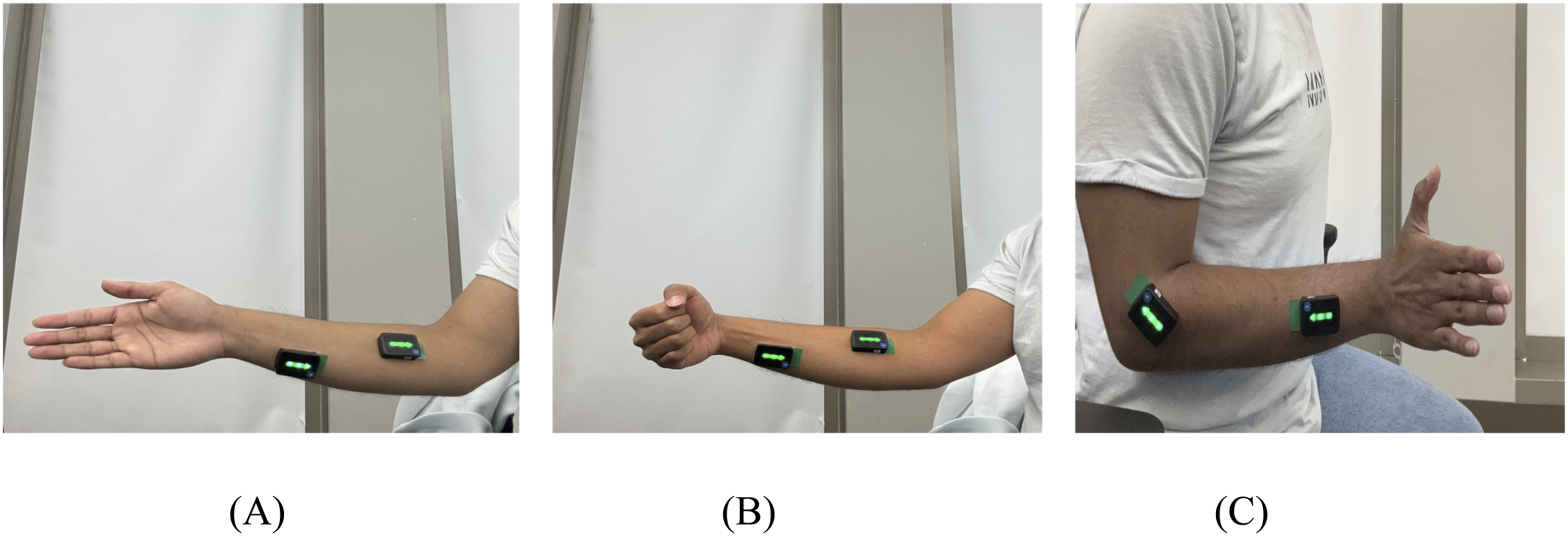
Eye-Tracking
A Pupil-core eye tracking system (Pupil Labs, Germany) was used to collect blink rate data. The system hardware included one world camera and two eye cameras (Figure 2). The eye cameras detected and tracked the pupil with 3-dimensional models at a frequency of 200 HZ. To streamline data collection, we developed a custom Python script that interfaced directly with the eye-tracker, enabling real-time extraction of blink rate data. The eye-tracking system was calibrated using Apriltag markers. Dismissing rate during the calibration was consistently controlled to be <20% based on the criteria defined by the manufacturer (Pupil Labs). Pupil-core eye tracker (left) and RTI driving simulator with a participant controlling the vehicle using an EMG-based HMI (right).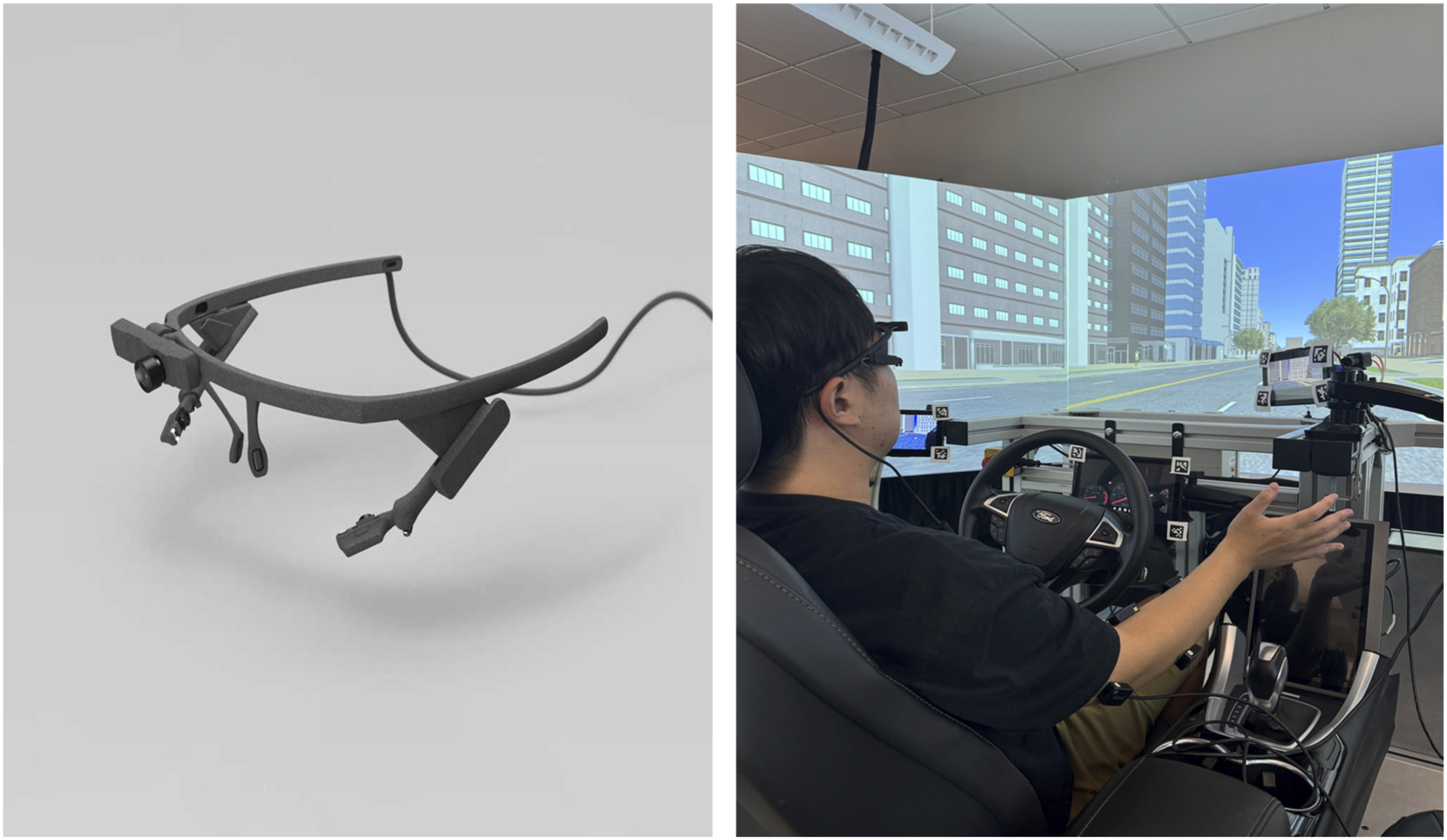
Driving Simulator
A high-fidelity driving simulator (Realtime technologies, Inc, Ann Arbour, MI) was used in the study (Figure 2). The simulator provides 300
Task
Participants drove in an urban environment using the driving simulator under three conditions: driving with the dominant hand, driving with both hands, and driving with the EMG-based HMI. The order of these conditions was randomized using a Latin square randomization. Each condition involved two trials, with each trial comprising maneuvers such as straight lane driving, overtaking a lead vehicle, and making 90-degree turns at intersections (Figure 3). To enhance realism, traffic was present in the opposite lane during each scenario. For driving with the EMG-based HMI, three movement classes were used to control the steering wheel: flexion turned the wheel left, extension turned it right, and neutral (no movement) maintained the wheel’s angular position. Driving maneuvers: (a) Straight Road, (b) Intersections, and (c) Overtaking a lead vehicle.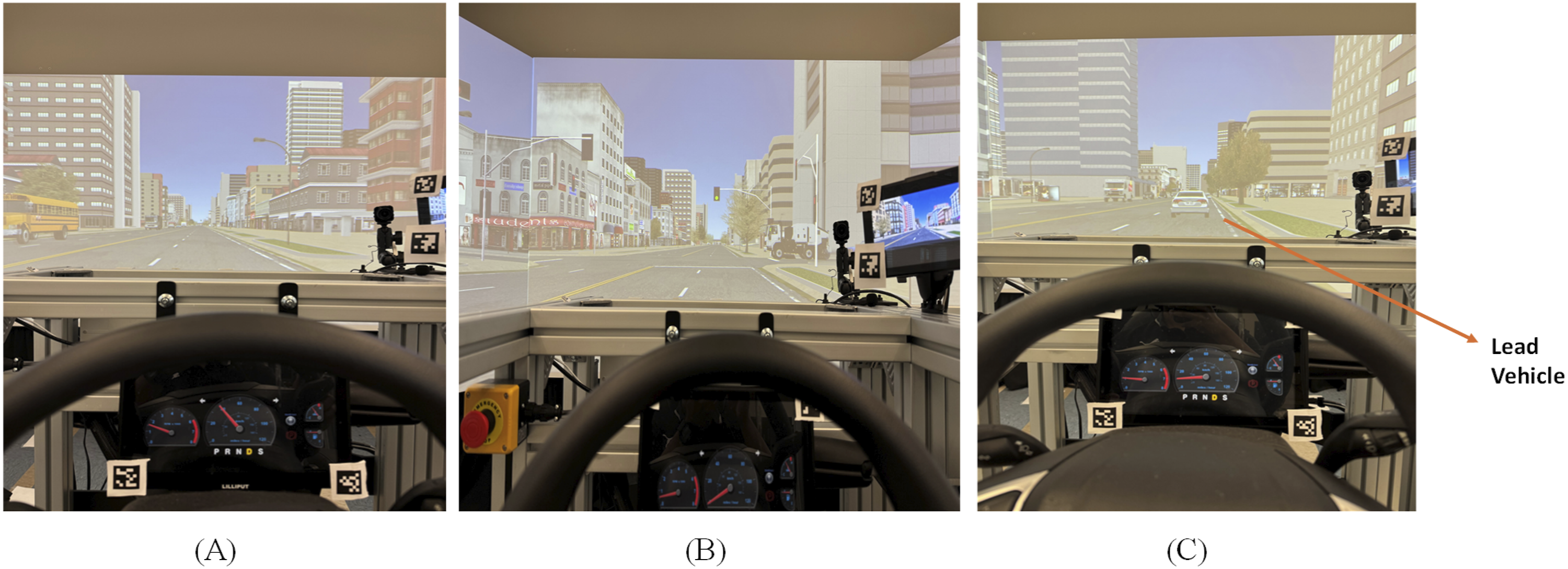
Experiment Design and Variables
The experiment followed a within-subject design with two independent variables: control mode and driving maneuver. Each participant completed all three control modes (i.e., dominant hand, both hands, and EMG-based HMI), with the order of control modes randomized to counterbalance any order effects. After being assigned a specific sequence of control modes, participants underwent training trials for each mode, followed by two experimental trials. The experimental trials involved three types of driving maneuvers: straight lane driving, overtaking a lead vehicle, and making 90-degree turns at intersections.
The dependent variables in this study included driver performance, cognitive workload, safety scores, and usability (using the USE questionnaire) (Liebner et al., 2013; Nacpil et al., 2019; Park & Zahabi, 2022; Wang et al., 2021). Driver performance was recorded using the driving simulator, which captured metrics such as mean velocity, lane offset, and steering angle. Mean velocity refers to the average speed of a vehicle over a specified time or distance. It is determined by summing all recorded velocities at various points and dividing this total by the number of observations (Söderström, 2023). Lane offset refers to the lateral distance between the center of a vehicle’s lane and its actual position on the road, serving as a measure of the vehicle’s ability to maintain its lane. This metric can be influenced by factors like road curvature, driver behavior, and external conditions (Liu et al., 2016). Steering angle refers to the angle between a vehicle’s wheels and its longitudinal axis, indicating how much the wheels are turned relative to the direction of the vehicle. It is a crucial parameter for controlling the direction and maintaining the stability of a vehicle during various maneuvers, such as turning and lane changes (Chen et al., 2021). Additional performance variables, including mean velocity deviation, calculated as the absolute difference between the vehicle’s speed and the posted speed limits (40 mph on straight roads and 20 mph at intersections) and steering entropy was calculated by recording steering angle data, using a second-order Taylor expansion to predict angles, and measuring differences between actual and predicted values. Shannon’s entropy formula was then applied to these prediction errors to determine the entropy, indicating the predictability of steering behavior (Zhang et al., 2022).
Safety scores in this study were derived from key performance metrics, including mean velocity, lane offset, steering angle, and steering entropy to assess the stability and control of drivers. Specific thresholds were established for different driving conditions based on a synthesis of findings from relevant literature. Safety score for mean velocity in this study were designed to manage speeds effectively at intersections and on straight road sections. Based on findings from Stephens et al. (2017), we set an acceptable speed threshold of 40 ± 8 mph for straight roads and 20 ± 4 mph for intersections. Additionally, these limits also aligned with 80% of expert driving performance in our driving simulator. Similarly, steering angle below 2° during straight-road segments was used as an indicator of stable vehicle control, aligning with general principles of maintaining lane position under minimal steering input, as discussed in Sanghavi et al. (2020). For intersection maneuvers, an acceptable range of 45 ± 10° was selected to ensure a balance between maneuverability and stability on vehicle control during intersections (Ding et al., 2021). To further assess the consistency of steering behavior, we used steering entropy, a unitless quantity ranging from 0 to 1 reflecting variation in steering predictability over time (Zhang et al., 2022), as a complementary measure. For straight-road conditions, a threshold of 0.5 was used, as maintaining low steering entropy suggests stable control and consistent lane-keeping (Zhang et al., 2022). During overtaking maneuvers, a threshold of 0.7 was adopted, allowing for the slightly increased variability required for lane changes while still maintaining controlled steering inputs. For intersections, a maximum entropy value of 0.8 was set, reflecting the need for greater steering flexibility when navigating curves (Nartey et al., 2023).
Cognitive workload (CW) was assessed using both blink rate and perceived or subjective workload ratings. Subjective assessment of CW was carried out using the Driving Activity Load Index (DALI) questionnaire. Participants’ DALI scores and weights for each dimension were collected based on the procedure described in Pauzié (2008). Participants rated their experience across six dimensions (Effort of Attention, Visual Demand, Auditory Demand, Temporal Demand, Interference, and Situational Stress) after completing each experiment trial. The scores were weighted and averaged to calculate the overall workload score. For physiological assessment of CW, blink rate (BR) was also captured throughout all the experiment trials using the Pupil Labs eye-tracking device. BR is a well-established indicator of CW, defined as the number of eye closures over a given period (Yahoodik et al., 2020). A reduction in eye blinks is typically associated with an increase in workload. In this study, BR was calculated as blinks per second rather than the traditional blinks per minute unit, as the duration of certain driving maneuvers was too short for a per-minute rate to yield meaningful values.
Usability was measured using the USE questionnaire, which is a composite assessment focusing on three key components: usability, satisfaction, and ease of learning (Lund, 2001). The USE survey captures subjective user experience, evaluating how easy and satisfying the device is to use. Participants were asked to rate the usability of each control method upon completion of the second driving scenario.
Procedure
Participants were recruited based on the following criteria: (i) normal or corrected-to-normal 20/20 vision and (ii) right-hand dominance. Before the experimental trials, participants provided informed consent and completed a demographics questionnaire. Participants were then asked to take the Edinburgh Handedness Test followed by the Purdue Pegboard Test (PPT) which was then administered three times to assess manipulative dexterity (Lawson, 2019; Veale, 2014). Participants qualified for the experiment if their right-hand dominance score was 0.7 or above (Gonzalez & Nelson, 2021) and PPT score was within one standard deviation of the average dexterity for their age and gender group (Lawson, 2019).
All participants completed the three control modes (dominant hand, both hands, and EMG-based HMI), with the sequence of control modes randomized to minimize any order effects. Prior to attaching the EMG electrodes, the participant’s right arm was properly cleaned with alcohol wipes and shaved where necessary to ensure that hand hair did not interfere with the EMG signals. For the EMG-based HMI method, EMG electrodes were attached to the participant’s right arm to capture muscle activity during three specific movements: flexion, extension, and neutral. Both the participants and the experimenter observed real-time EMG signals via the EMGworks® software, which displayed the distinct signal patterns for each movement class. Participants were then instructed on how these movements would control the steering wheel: flexion to turn left, extension to turn right, and neutral to hold the current position. Three movements were repeated twice, and features were recorded to train the Linear Discriminant Analysis (LDA) classifier model. After the model training, the movements were classified into three categories (flexion, extension, and neutral) in real-time. After training, participants practiced the movements until they felt comfortable with the EMG-based HMI. The classifier’s accuracy for each movement was then evaluated over a 10-s window. If the accuracy for all three movements was below 80%, the classifier was retrained until this criterion was met. This threshold was established based on observations from pilot data.
After completing the EMG calibration, the eye-tracking system was calibrated for each participant. Following a 5-min break, participants were instructed to begin the training trials in the driving simulator. During the training, participants were given specific instructions: (i) maintain a speed of 40 mph on straight roads and while overtaking and (ii) reduce speed to 20 mph at intersections. Each participant performed at least three training trials for each control method. They were required to meet two performance thresholds: (i) maintain a speed within the range of 40 ± 8 mph (Stephens et al., 2017) and (ii) stay within a lane offset range of <3 feet based on findings from 80% of expert driving performance. Additional training trials were conducted if either performance criterion was not met. These training trials were conducted on a separate road segment from the experimental trials to minimize any potential learning effects. After completing the training trials, participants were given a 5-min rest before starting the experimental trials. Figure 4 illustrates the experimental procedure, detailing the sequence from initial screening and calibration through training trials in the simulator, followed by experimental trials, and concluding with the postexperiment debrief. Experiment procedure.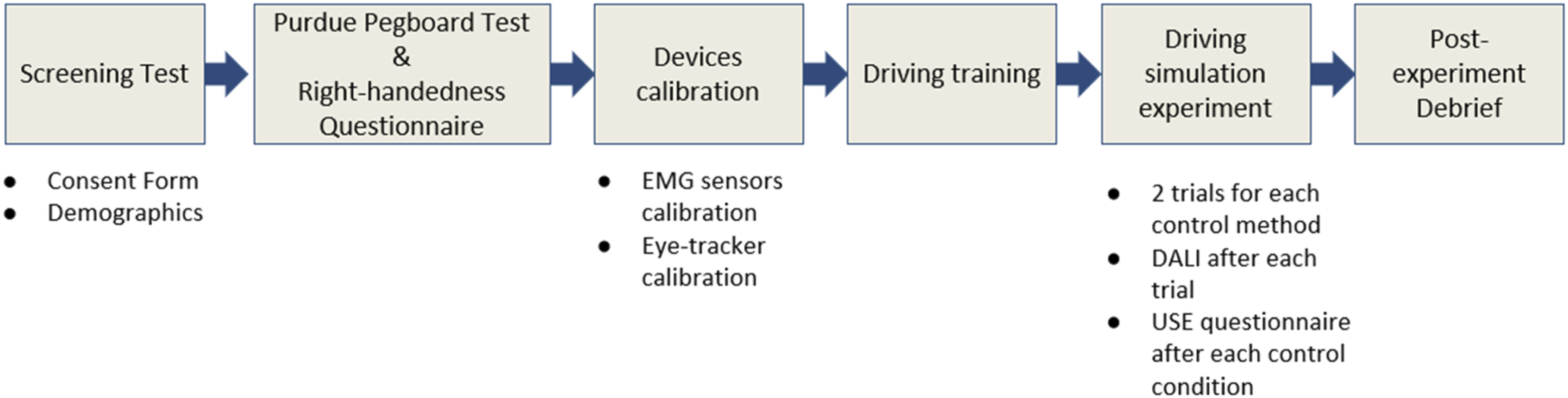
For the experimental trials, participants followed the same driving instructions as during the training trials. To minimize any learning effects between trials, the order of the experimental trials was randomized. In total, participants completed six driving scenarios across the three control modes: dominant hand, both hands, and EMG-based HMI (two scenarios per each control mode). For the EMG-based HMI trials, participants were only allowed to use their dominant hand, as the sensors were attached to this arm. During the dominant hand condition, participants could drive using only their right arm, while in the both-arms condition, they could use both hands on the steering wheel.
Data Analysis
Summary of Descriptive Statistics for all Variables.
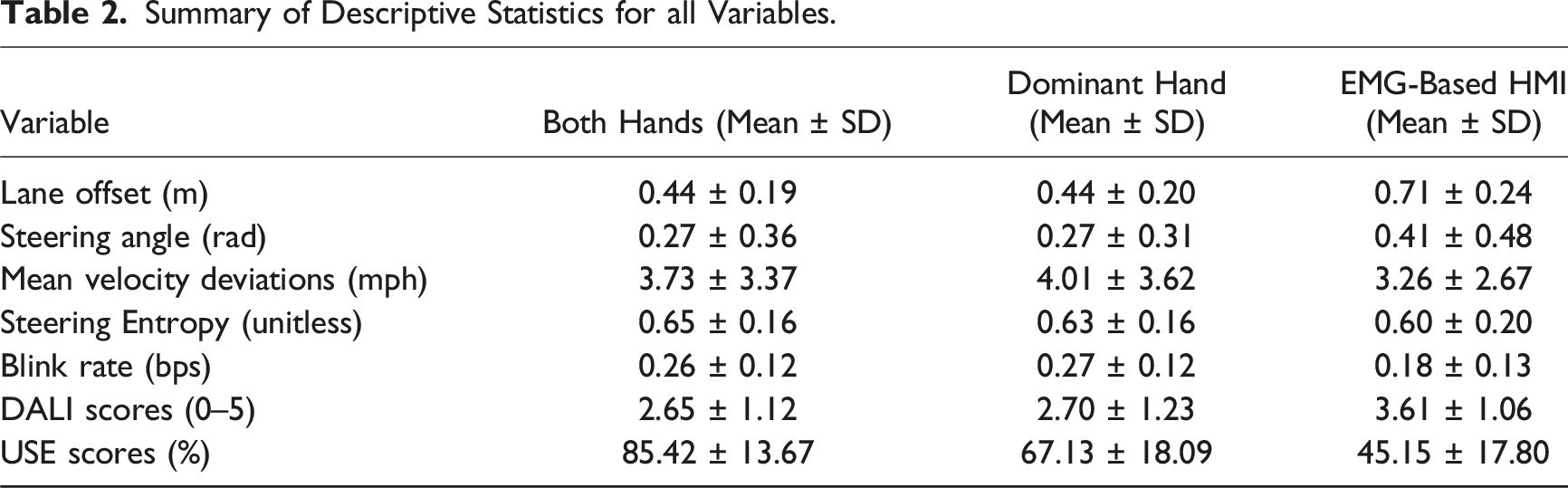
Before conducting inferential statistics, outliers were removed from the data using video recordings and Cook’s D criteria (Cook, 1979). The data were first tested for normality using Shapiro–Wilk’s test and homogeneity of variance using Levene’s test (O’neill & Mathews, 2002). For data that violated parametric test assumptions (mean velocity deviation, lane offset, steering angle, DALI, and USE), box-cox transformation (Box & Cox, 1964) was applied. We employed a two-way repeated measures analysis of variance (ANOVA) to examine the independent variables’ impact on response variables, followed by Bonferroni-corrected post-hoc comparisons. For data that did not meet parametric assumptions, including steering entropy and blink rate, the aligned rank transform (ART) ANOVA was applied (Wobbrock et al., 2011). Binary measures, such as velocity safety score, steering angle safety score, and lane offset safety score (categorized as 0 for unsafe and 1 for safe), were analyzed using a logistic regression model (LaValley, 2008) and one-way AVOVA was used to analyze subjective scores (DALI and USE) as these outcomes were collected after each experimental trial, which encompassed all driving maneuvers.
Results
Driving Performance and Safety Outcomes
Mean Velocity Deviation (MVD)
The control method did not have a statistically significant effect on mean velocity deviation (F (2,36) = 2.42, p > .05, Interaction plot illustrating the effect of control modes and driving maneuvers on Mean Velocity Deviation (MVD). Error bars represent standard error (SE). EMG-based HMI = Electromyography-based Human–Machine Interface.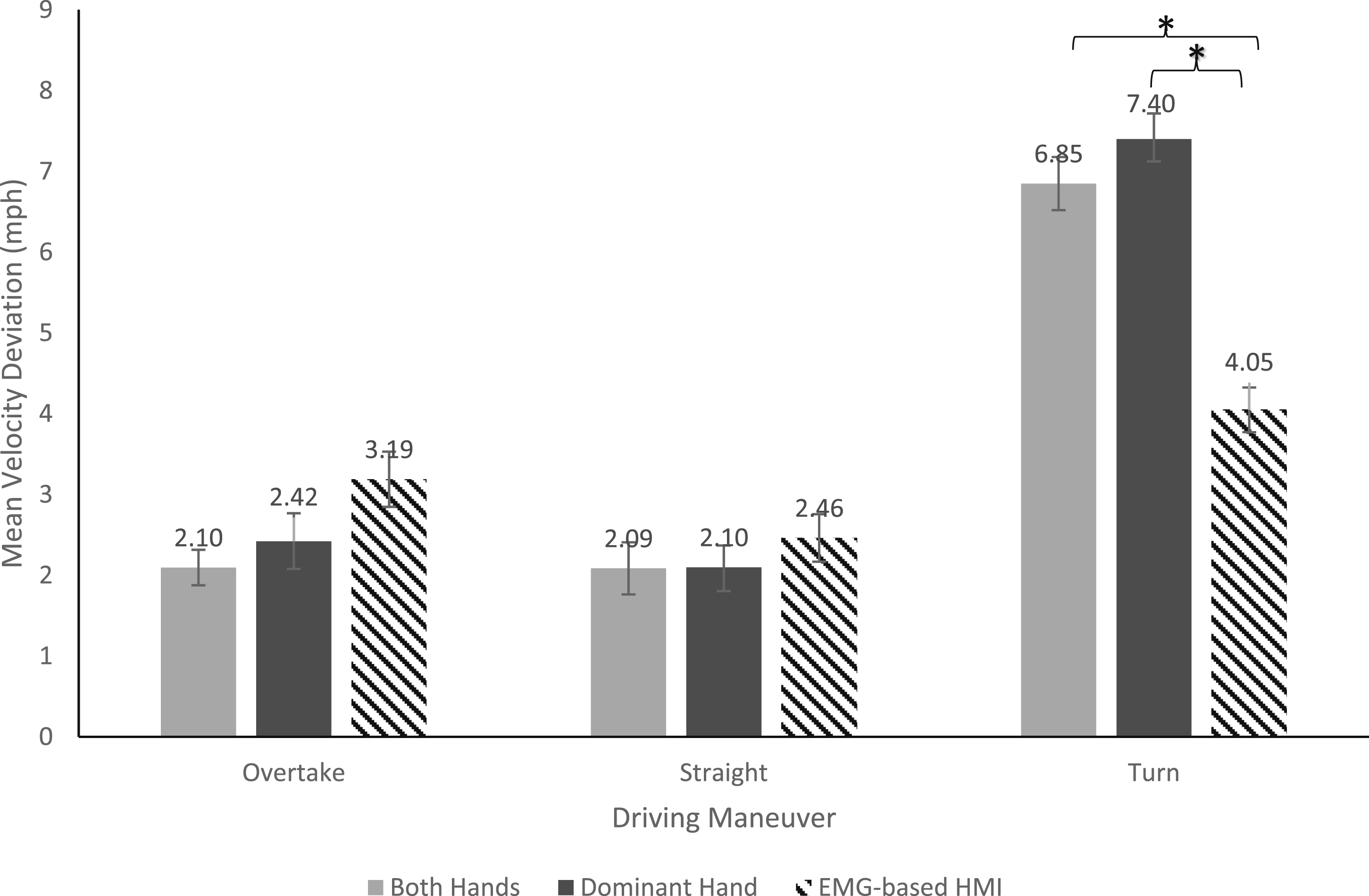
Lane Offset
There was a statistically significant effect of the control mode on lane offset (F (2, 36) = 159.20, p < .001,
Steering Angle
Control mode had a significant effect on steering angle (F (2, 36) = 120.84, p < .001,
Steering Entropy
Steering entropy was significantly affected by the control method (F (2, 36) = 3.96, p < .05,
Cognitive Workload
Blink Rate
There was a significant effect of control mode on blink rate (F (2, 36) = 39.52, p < .001,
DALI Scores
The DALI scores exhibited significant differences across control methods (F (2, 36) = 7.63, p < .001,
Usability Outcomes
The control mode had a significant effect on the USE score (F (2,36) = 26.72, p < .001.
Discussion
The objective of this study was to investigate the feasibility of an EMG-based HMI for driving by measuring driver performance, CW, usability, and safety of such method compared to conventional hand steering methods, that is, with dominant hand and both hands. The evidence collected in the study offers partial support for H1 which posited that performance of the EMG-based HMI driving will be better than that of dominant hand driving and both hand driving. The driving performance results revealed that using the EMG-based HMI resulted in higher lane offset and steering angle compared to dominant hand and both hands driving. These findings can be attributed to two factors: (i) Participants, being able-bodied and not accustomed to using EMG-based HMIs in their daily lives, particularly for activities like driving, lacked familiarity with these systems and (ii) EMG-based HMIs could induce muscle fatigue if used for a prolonged period of time and in this study, required the arm to be held perpendicular to the body to control the steering wheel (Lalitharatne et al., 2012). This was further verified during the post experiment debriefing when participants reported feeling fatigue in their dominant hand, where the sensors were attached. Another performance metrics, mean velocity deviation (MVD), showed that the EMG-based HMI resulted in lower MVD compared to other control methods, but only during intersections. This finding suggests that the EMG-based HMI may facilitate more precise speed regulation when navigating intersections. However, since this effect was not observed in other driving maneuvers, the benefits of the EMG-based HMI for velocity control may be specific to situations that require heightened attention and control, such as intersections. This finding is also consistent with previous findings by Nacpil et al. (2019), who reported that EMG-based steering interfaces demonstrated comparable or superior path-following accuracy to conventional steering only in specific, controlled scenarios, such as low-speed U-turns or 90° turns, while their advantages diminished in more complex or dynamic tasks and at higher speeds (Nacpil et al., 2019). EMG-based HMI demonstrated a unique behavior in terms of steering entropy, which quantifies the unpredictability or randomness of steering control. Higher steering entropy typically indicates more erratic, less predictable steering and is often associated with higher workload, distraction, or corrective responses to unexpected situations or errors (Paul et al., 2005). Conversely, lower steering entropy suggests more predictable, smoother, and potentially more controlled steering behavior (Paul et al., 2005). In our study, we found that steering entropy was lower for the EMG-based HMI compared to both-hand driving. This finding suggests that steering actions were more consistent and less erratic, possibly indicating that the EMG-based HMI enabled users to maintain a steadier steering pattern with fewer abrupt corrections or random fluctuations. However, it is important to note that lower steering entropy is not always associated with better driving performance; in some cases, overly rigid or infrequent steering corrections can also reduce entropy but may compromise safety (Paul et al., 2005). Thus, entropy should be interpreted alongside other performance metrics. Our driving scenarios were designed to be predictable and followed fixed trajectories, without the inclusion of dynamic external factors such as abrupt lane changes, sudden changes in traffic flow, merging vehicles, or unexpected braking. As a result, situations requiring frequent micro-adjustments to steering were minimized, making lower steering entropy both expected and desirable in this context. However, in situations with greater unpredictability, a higher level of steering entropy may actually indicate the driver’s ability to make necessary adaptive adjustments in response to changing conditions. These mixed outcomes are consistent with the findings of Nacpil et al. (2019), who also reported that the performance of EMG-based HMIs was comparable to traditional steering only in certain controlled scenarios (low speed U-turns or 90° turns), with limitations becoming apparent in more complex or variable driving tasks.
The findings supported H2, which suggested that cognitive workload for EMG-based HMI driving would be higher than that of dominant and both hands driving. Consistent with a study by Paskett et al. (2022), this elevated workload indicates that EMG-based HMI imposes a higher cognitive load on participants due to the lack of natural automaticity associated with prosthetics control, unlike the intuitive, automatic movements of an intact limb. Prior studies also suggest that learning to control prosthetics requires increased mental effort (Park et al., 2023), as participants often struggle with performing tasks that are otherwise intuitive with their natural limbs. This contrast was evident in dominant hand and both arm driving, which were more familiar and intuitive for able-bodied participants, aligning with their daily motor habits. The DALI scores further validated these findings, with participants reporting the highest workload for EMG-based HMI driving, followed by dominant hand driving, and the lowest for both hands driving.
H3, which posited lower usability of EMG-based HMI driving, as compared to dominant hand and both hands driving, was supported. It was found that there were significant differences in terms of usefulness, satisfaction, and ease of use across the three control methods. A similar study by Paskett et al. (2022) found that usability of EMG-based HMI remains a significant challenge due to the cognitive demand associated with its control as compared to using a natural limb. This increased cognitive load can reduce user satisfaction and ease of use, contributing to high abandonment rates of prostheses. For our study, it was inferred that, because the participants were able-bodied, they found EMG-based HMI driving less useful, satisfying, and easy to use, as they could not relate to the technology relevant in their daily lives. However, during postexperiment debriefing, when they were asked if they thought this form of prosthetics driving would be beneficial for upper-limb amputee drivers, participants unanimously acknowledged its potential application.
H4 posited that safety of using the EMG-based HMI for driving will be better than that of dominant hand driving and both hands driving. This was partially supported by the study’s findings. It was found that using the EMG-based HMI resulted in lower lane offset safety score and steering angle safety score compared to dominant and both hands driving which are in line with the findings from H1. However, the mean velocity deviation safety scores indicate that the EMG-based HMI enabled participants to maintain speeds at intersections with a precision better than conventional steering methods, suggesting higher safety in terms of velocity control under these predictable conditions. The superior performance of EMG-based control at intersections may be partly explained by cognitive mechanisms that become more effective in slower, more predictable conditions. At lower speeds (20 mph around intersections), drivers are afforded more time to engage in predictive motor control, where they can rely on muscle memory for smoother, stable steering (Summala, 2007; Zhao & Wu, 2013). The consistent muscle activation required for EMG-based control aligns well with such conditions, where minimal rapid adjustments are needed. Additionally, the proprioceptive feedback from muscle activation in EMG may further enhance control by providing immediate sensory cues that support fine-tuned steering. In contrast, higher speeds (40 mph on straight roads and during overtakes) may demand more adaptive motor planning, requiring drivers to continuously monitor and adjust their movements, a process that relies on fast, flexible decision making (He et al., 2014). Such dynamic conditions can reduce the effectiveness of EMG-based control, where maintaining precise muscle activation without immediate feedback becomes more challenging (Engström et al., 2017). This difference in cognitive demands across speed contexts may help explain why the advantages of EMG-based control were more pronounced at intersections. Additionally, the lower steering entropy observed with the EMG-based HMI during intersections compared to overtakes reflected more predictable steering behavior, which translated into higher safety scores for this metric in scenarios with fixed trajectories and minimal external disturbances. While low steering entropy typically reflects higher predictability, it does not always translate to safer driving across all situations. In certain scenarios, low entropy may actually reflect inflexible or overly rigid steering behavior, where drivers are not making the continuous micro-adjustments necessary for optimal lane-keeping. Therefore, the safety advantages of lower steering entropy observed in our study with the EMG-based HMI are most relevant to predictable, structured environments (such as standard intersections or straight roads) but may require further evaluation to be generalized to more complex or unpredictable driving conditions.
Limitations
One of the limitations of our study is the assumption that upper limb amputees drive exclusively with their prosthetic devices, without assistance from the other hand. This may not fully reflect real-world scenarios where amputees might use both prosthetic arm and their other hand for driving. Additionally, the current findings are based on data from able-bodied participants, which may not capture the full range of muscle activation patterns present in the target user group. Our approach aligns with existing research in EMG-based prosthetic systems, where over 60% of cognitive workload and usability studies involve able-bodied subjects with or without bypass devices for early evaluations (Park & Zahabi, 2022). The sensor placement and control structure were specifically designed with wrist-disarticulated and trans-radial users in mind, and this approach is consistent with prior work in EMG interface development (Legrand et al., 2018; Nacpil & Nakano, 2020; Park et al., 2023). However, we acknowledge that these findings may not be directly generalizable to the target population at this stage. Instead, they should be viewed as a foundation for future research and clinical trials aimed at evaluating EMG-based HMIs with trans-radial amputee users to ensure broader generalizability and clinical relevance.
Another limitation relates to our sample size estimation approach. The effect size used in our power analysis was empirically derived from pilot data, which, due to its limited sample size, may be subject to imprecision and sampling variability. Relying solely on pilot-based estimates or generalized benchmarks can undermine the accuracy and contextual relevance of power analyses. For future studies, we recommend exploring the Bayesian approach to sample size planning, which may offer more robust guidance in early-stage research. Furthermore, while blink rate was used as the primary pupillometry-based measure of cognitive workload in this study, future research should explore a broader range of ocular metrics, such as pupil diameter or percent change in pupil size (PCPS), to provide a more comprehensive understanding of cognitive workload.
Conclusion
This study assessed the feasibility of using an EMG-based HMI for driving compared to conventional steering methods using the dominant hand or both hands with able-bodied subjects. While the EMG-based HMI reduced driving performance in terms of lane offset and steering angle, it offered more precise velocity control, particularly at intersections, and predictable steering behavior overall indicating its potential for controlled yet realistic driving context. Cognitive workload was found to be higher with the EMG-based HMI, as expected, due to the unfamiliarity of participants with the novel interface. Usability, measured through user satisfaction and ease of use, was lower for the EMG-based HMI, as participants found it less intuitive than conventional methods. However, participants acknowledged the potential benefits of that interface for amputees. In terms of safety, mean velocity deviation results suggested that the EMG-based HMI performed well during turn maneuvers and steering entropy findings suggested that the EMG-based HMI performed better overall compared to dominant and both hands driving, suggesting its potential for safe vehicle control with training. Although the study used able-bodied participants, sensor placement and control design were tailored for wrist-disarticulated and trans-radial users.
This study makes several key scientific contributions. First, it demonstrated the context-dependent performance of EMG-based control, with superior outcomes in predictable environments (e.g., intersections) but reduced effectiveness in dynamic conditions (e.g., overtakes). Second, it introduced a multi-dimensional evaluation framework, assessing driver performance, cognitive workload, usability, and safety using both objective (mean velocity deviation, lane offset, steering entropy) and subjective (DALI, USE) measures. Third, unlike prior studies that focused on basic or controlled tasks, this study tested EMG-based control in a realistic driving environment, offering insights directly applicable to real-world scenarios. Future work should involve upper-limb amputees to assess usability and effectiveness in real-world driving contexts and to support clinical translation of EMG-based driving technologies.
Key Points
• This study investigates the feasibility of an EMG-based HMI as an alternative control method for driving, focusing on how it impacts performance, cognitive workload, usability, and safety. • The study found that EMG-based HMI allowed for precise velocity control, especially at intersections, and consistent steering patterns, shown through lower steering entropy than both-hand driving. However, it led to higher lane offset, suggesting that while EMG-based HMI provided controlled steering, its performance could benefit from further refinement for accurate lane-keeping. • EMG-based HMI increased cognitive workload due to participants’ lack of familiarity with the interface, requiring greater mental effort than conventional controls. Despite lower usability scores, EMG-based HMI exhibited stronger safety performance at intersections, showing its potential for controlled driving tasks with further development. • Although these findings may not yet be directly generalizable to trans-radial amputees, they provide a strong foundation for future research and highlight the promise of EMG-based interfaces as a pathway toward safer and more intuitive driving control options for individuals with upper-limb amputations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Science Foundation (No. IIS-1856676). The opinions expressed in this report are those of the authors and do not necessarily reflect the views of the National Science Foundation.