
Abstract
Objective
To investigate the biodynamics of human-exoskeleton interactions during patient handling tasks using a subject-specific modeling approach.
Background
Exoskeleton technology holds promise for mitigating musculoskeletal disorders caused by manual handling and most alarmingly by patient handling jobs. A deeper, more unified understanding of the biomechanical effects of exoskeleton use calls for advanced subject-specific models of complex, dynamic human-exoskeleton interactions.
Methods
Twelve sex-balanced healthy participants performed three simulated patient handling tasks along with a reference load-lifting task, with and without wearing the exoskeleton, while their full-body motion and ground reaction forces were measured. Subject-specific models were constructed using motion and force data. Biodynamic response variables derived from the models were analyzed to examine the effects of the exoskeleton. Model validation used load-lifting trials with known hand forces.
Results
The use of exoskeleton significantly reduced (19.7%–27.2%) the peak lumbar flexion moment but increased (26.4%–47.8%) the peak lumbar flexion motion, with greater moment percent reduction in more symmetric handling tasks; similarly affected the shoulder joint moments and motions but only during two more symmetric handling tasks; and significantly reduced the peak motions for the rest of the body joints.
Conclusion
Subject-specific biodynamic models simulating exoskeleton-assisted patient handling were constructed and validated, demonstrating that the exoskeleton effectively lessened the peak loading to the lumbar and shoulder joints as prime movers while redistributing more motions to these joints and less to the remaining joints.
Application
The findings offer new insights into biodynamic responses during exoskeleton-assisted patient handling, benefiting the development of more effective, possibly task- and individual-customized, exoskeletons.
Keywords
Introduction
While work-related musculoskeletal disorders (WMSDs) continue to be a significant source of disability for the US workforce, they are affecting the healthcare industry at an alarmingly higher rate than other sectors (BLS, 2023). The rate of overexertion injuries for hospital workers (63 per 10,000) and for nursing and residential care facilities (76 per 10,000) is about 2–3 times the average across all occupations (26 per 10,000) (BLS, 2021). Among these workers, nursing assistants have the highest incidence rates of cases involving days away from work. With over 1.3 million nursing assistants in the US providing basic care and assisting patients with daily activities, the occurrence of back-related musculoskeletal disorders is a major concern. In 2016, nursing assistants experienced 10,330 back-related WMSD cases, accounting for more than half of all WMSD cases reported in this occupation that year (BLS, 2018). The repetitive bending and lifting involved in patient handling tasks performed by nursing assistants contributes significantly to the risk of low-back injuries (Hwang et al., 2021). Prior studies have employed modeling tools such as OpenSim and 3DSSPP to evaluate the effects of assistive devices other than exoskeletons during patient transfer tasks (Banks et al., 2024; Ulin et al., 1997; Zhuang et al., 1999). However, few have incorporated both human-exoskeleton interaction forces and hand forces into the models (Banks et al., 2024). It is crucial to understand the biomechanics of the dynamic interactions during patient handling tasks to effectively mitigate the risk of musculoskeletal overexertion injuries associated with nursing assistants’ or caregivers’ work.
Exoskeletons have shown promise in enhancing workers’ strength, endurance, and overall physical performance (Chen et al., 2023; Ivaldi et al., 2021; Kim et al., 2020; Kim et al., 2018: Latella et al., 2022; Luo et al., 2024; Maurice et al., 2022; O’Connor, 2021; Riccoboni et al., 2021; Siviy et al., 2023; Zheng et al., 2021). Among different types of exoskeletons, passive back-support exoskeletons have gained increasing popularity due to their lightweight design and user-friendly features. Previous studies have highlighted the positive effects of back-support exoskeletons on reducing back muscle activities and modifying various joint kinematic parameters, such as trunk flexion, hip flexion, and lumbar flexion (Hwang et al., 2021; Koopman et al., 2019, 2020; Yin et al., 2023). However, it has been recognized that while reduced muscle activity is often associated with less spine loading, significant changes in lumbar kinematics induced by an exoskeleton can affect spine loading differently (Koopman et al., 2019; Ulrey & Fathallah, 2013). In modeling human-exoskeleton interactions (HEI), exoskeletons were often integrated into biomechanical models by rigidly linking specific parts to designated body segments (Agarwal et al., 2016; Jones et al., 2023; Manns et al., 2017). The exoskeleton’s effects were then simulated using motion data from conditions when the exoskeleton was not worn. These studies, by a forward dynamics approach, simulated but failed to experimentally verify the motion effects of the exoskeletons. Our study would address this limitation by an inverse dynamics approach using real motion data collected while participants wear the exoskeleton and incorporating forces directly into the actual exoskeleton-assisted motion. A deeper, more unified understanding of the biomechanical effects of wearing an exoskeleton requires advanced subject-specific models of the complex, dynamic HEI. These biodynamic models must be subject-specific to capture individualized responses and interplays between personal, task, and wearable factors. In return, such models would enable “what if” simulations that can inform the design of next-generation exoskeletons with better human-exoskeleton fit and personalization. Exoskeleton products tailored specifically for patient handling or healthcare workers are currently limited in availability (Zheng et al., 2022). The development of advanced biomechanical models could play a vital role not only in addressing this scarcity but also in providing exoskeleton developers with a more profound understanding of the unique challenges and requirements within healthcare settings.
Therefore, the current study was motivated by a research methodology goal and an application goal. First, we sought to establish a subject-specific modeling approach to investigating the biodynamics of HEI. Second, we aimed, with this approach, to study the effects of wearing a passive back exoskeleton on whole-body joint kinematics and kinetics during patient handling tasks. To achieve these goals, we designed and executed an experiment in which simulated patient handing tasks were performed while biodynamic data were acquired; we employed OpenSim, a musculoskeletal modeling software tool (Delp et al., 2007), to create subject-specific models incorporating data from optical motion capture, ground reaction force (GRF), and human-exoskeleton interactive force measurements. By leveraging digital modeling and simulation techniques, our long-term objective is to contribute to the design and development of more effective exoskeletons and promote safer manual handling practices.
Methods
Experiment
Twelve healthy individuals, six males (age: 27.7 ± 3.3 years, weight: 66.1 ± 5.9 kg, height: 1.71 ± 0.08 m) and six females (age: 22.7 ± 1.7 years, weight: 65.8 ± 11.8 kg, height: 1.69 ± 0.10 m), free from any musculoskeletal disorder or condition were recruited. The study protocol was approved by the Institutional Review Board of Texas A&M University. After providing written informed consent, the participants were given sufficient time to become familiarized with the use of exoskeleton (Laevo V2.5, Delft, The Netherlands) and experimental tasks. The Laevo was chosen because it is the most used passive back exoskeleton, as suggested by a recent critical review (Zheng et al., 2022).
The exoskeleton was adjusted based on each individual’s anthropometry, following the manufacturer’s guidelines (Yin et al., 2023). The initial flexion angle of the Laevo’s spring-loaded joint (Figure 2(a)) was set to 0°, ensuring that no support was provided when the user was in an upright standing position. The hip pads were securely attached to the pelvis, while the chest and leg pads were connected to the torso and legs via two pairs (four total) of rigid blue structural springs. This design redistributed forces primarily through the chest and thigh supports as participants bent at specific angles, with the springs functioning as a mechanical spine for the exoskeleton, effectively reducing the load on the lumbar spine and minimizing actual lumbar spine moments.
The participants each performed three simulated patient handling tasks (Figure 1), with and without wearing the exoskeleton, wherein a mannequin (Harmonized Hybrid III 50th Male, 77.7 kg) was used to simulate the patient. These three tasks were selected as the most distinctively different from each other from a variety of patient handling tasks included in previous patient handling studies (Skotte et al., 2002). Simulated patient handling tasks performed by the subjects: (a) patient side-turning; (b) patient upper-body lifting; (c) patient sit-up assisting.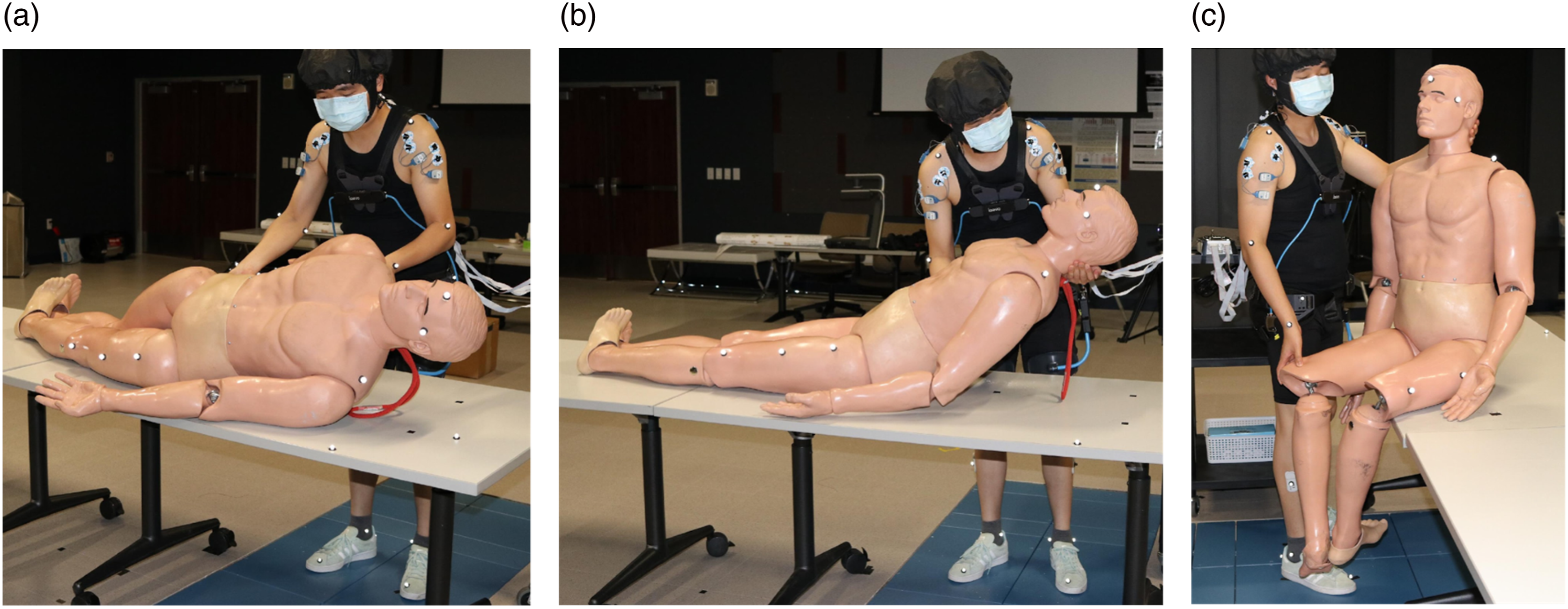
Task (a) patient side-turning: Starting from a static upright posture, the subject placed one hand on the patient’s shoulder and the other hand beneath the hip. The subject then proceeded to rotate the patient forward to an angle of 30°. At this point, a five-second countdown was initiated by Vicon software, serving as an auditory cue for the subject to maintain the posture for the specified duration. Following the completion of the countdown, the subject carefully returned the patient to the original position.
Task (b) patient upper-body lifting: Starting from a static upright posture, the subject placed his or her left forearm underneath the patient’s neck and his or her right forearm on the patient’s back. With a controlled motion, the subject lifted the patient’s torso to an angle of 45° relative to the horizontal plane. Once the required angle was reached, the Vicon software initiated a five-second countdown, providing an audible cue for the subject to sustain the posture. After the countdown, the subject carefully returned the patient to the original position.
Task (c) patient sit-up assisting: Starting from a static upright posture, the subject placed his or her left forearm underneath the patient’s neck and their right forearm on the patient’s back. The subject first lifted the torso to an upright sitting position. Then, the subject used his or her left hand to maintain the upright torso position, while using the right hand to reposition the patient’s legs to prepare for a sit-to-stand transition. The sitting position was maintained for 5 seconds.
Each task was repeated five times. The order of tasks (a), (b), and (c) was randomized with two-minute intertrial breaks. In addition, the order of tasks with and without exoskeleton was randomized with a one-hour break in between. Before the patient handling tasks, subjects were asked to perform 5 minutes of repeated symmetric load-lifting as a reference task, denoted as task (r), for benchmarking as well as validation purposes (see section Model Validation). The load being lifted weighed 6 kg.
Twenty-seven reflective markers were attached to palpable anatomical landmarks with a placement scheme (Figure 2) largely resembling the plug-in gait marker set (Davis et al., 1991). In trials with the exoskeleton, four of these markers (RAEXO, LAEXO, RPEXO, and LPEXO) were placed on the hip paddings of the exoskeleton to replace the pelvis markers (RASI, LASI, RPSI, and LPSI) which would interfere with the exoskeleton. Four additional markers were attached to chest pads and leg pads for measuring the flexion angle of the exoskeleton. Surface marker placement strategy under (a) with exoskeleton and (b) without exoskeleton conditions. In (a), four markers (RAEXO, LAEXO, RPEXO, LPEXO) were attached to the hip paddings of the exoskeleton to replace the four pelvis markers (RASI, LASI, RPSI, LPSI); four additional markers, two on the chest pads and two on the leg pads (rectangle-framed), were placed to acquire the flexion angle of the exoskeleton.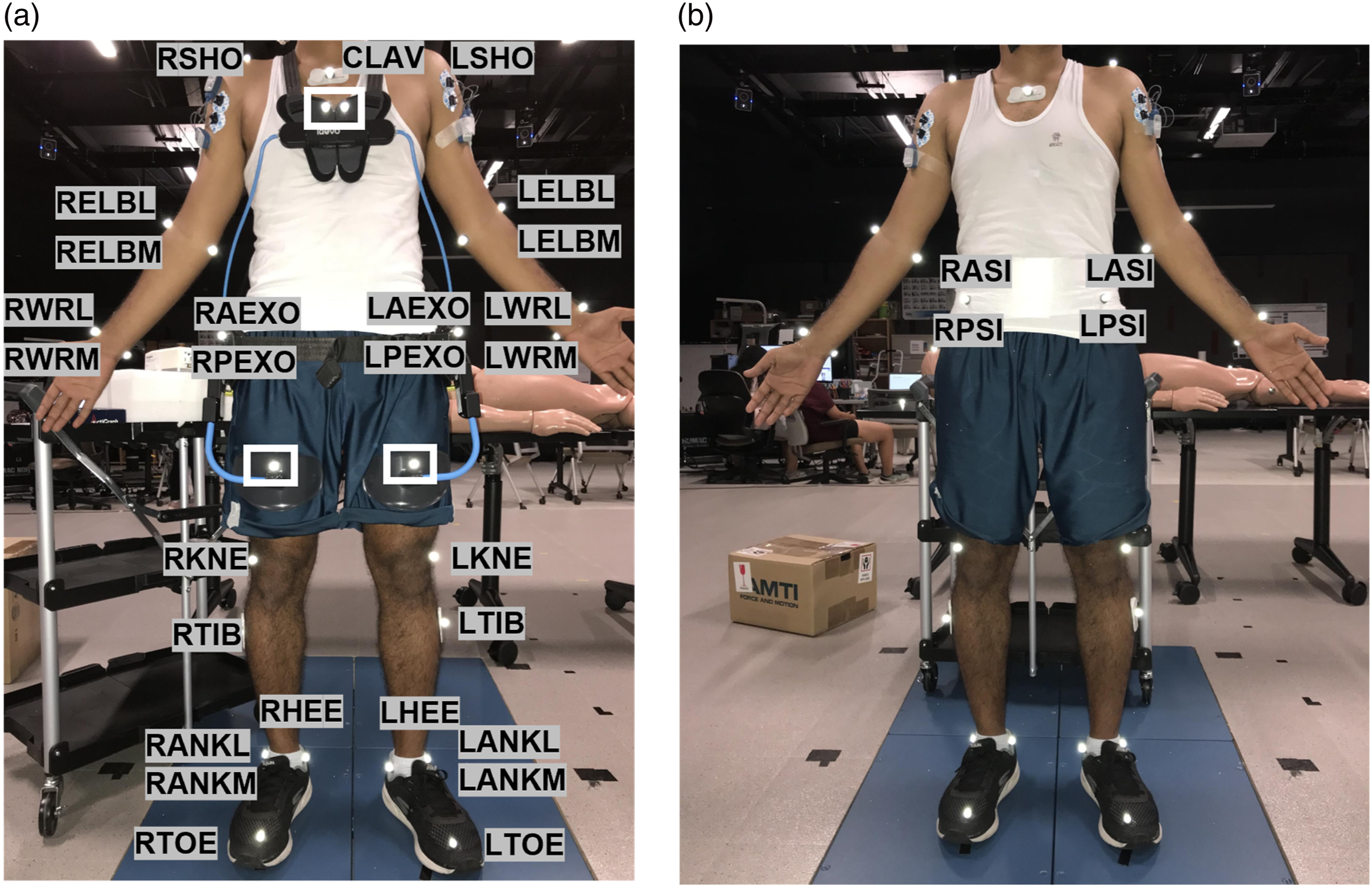
Data Preprocessing and Preparation
A twelve-camera Vicon system (Vicon Motion Systems, Oxford, UK) was used to record the motions of surface markers at a sampling rate of 50 Hz. The marker motion data were tracked and preprocessed by Nexus software. The GRFs were recorded by dual AMTI force plates (Advanced Mechanical Technology, Inc, Massachusetts, USA) at a sampling rate of 1000 Hz. The GRFs were filtered using a low-pass filter with a cut-off frequency of 5 Hz. The hand forces were estimated using the GRF measurement based on a bottom-up approach (Faber et al., 2013). For the trials with the exoskeleton, the forces generated by the exoskeleton were estimated using the Laevo angle-torque relationship measured by (Koopman et al., 2019) and the exoskeleton flexion angle calculated by markers placed on the chest pads and each leg pad (Figure 2). The Laevo angle-torque relationship was derived by measuring the force applied to the chest pad using a force transducer. The torque at the Laevo joint was then calculated as the cross product of the measured force and the vector from the force application point to the joint’s center of rotation (Koopman et al., 2019).
Subject-Specific Biodynamic Modeling
The subject-specific biodynamic models were constructed on the open-source musculoskeletal modeling software platform OpenSim 4.2, based on the full-body lumbar spine model (Raabe & Chaudhari, 2016). The model comprises 21 segments, encompassing a total of 30 degrees of freedom (Figure 3). A full-body lumbar spine model under exoskeleton condition. The blue markers are physical spherical markers placed on body surface landmarks for motion capture while the pink markers are virtual markers on the corresponding landmarks in OpenSim; the green arrows indicate the external forces, including the GRFs, hand forces, and exoskeleton forces (forces acting on the leg pads, chest pads and hip).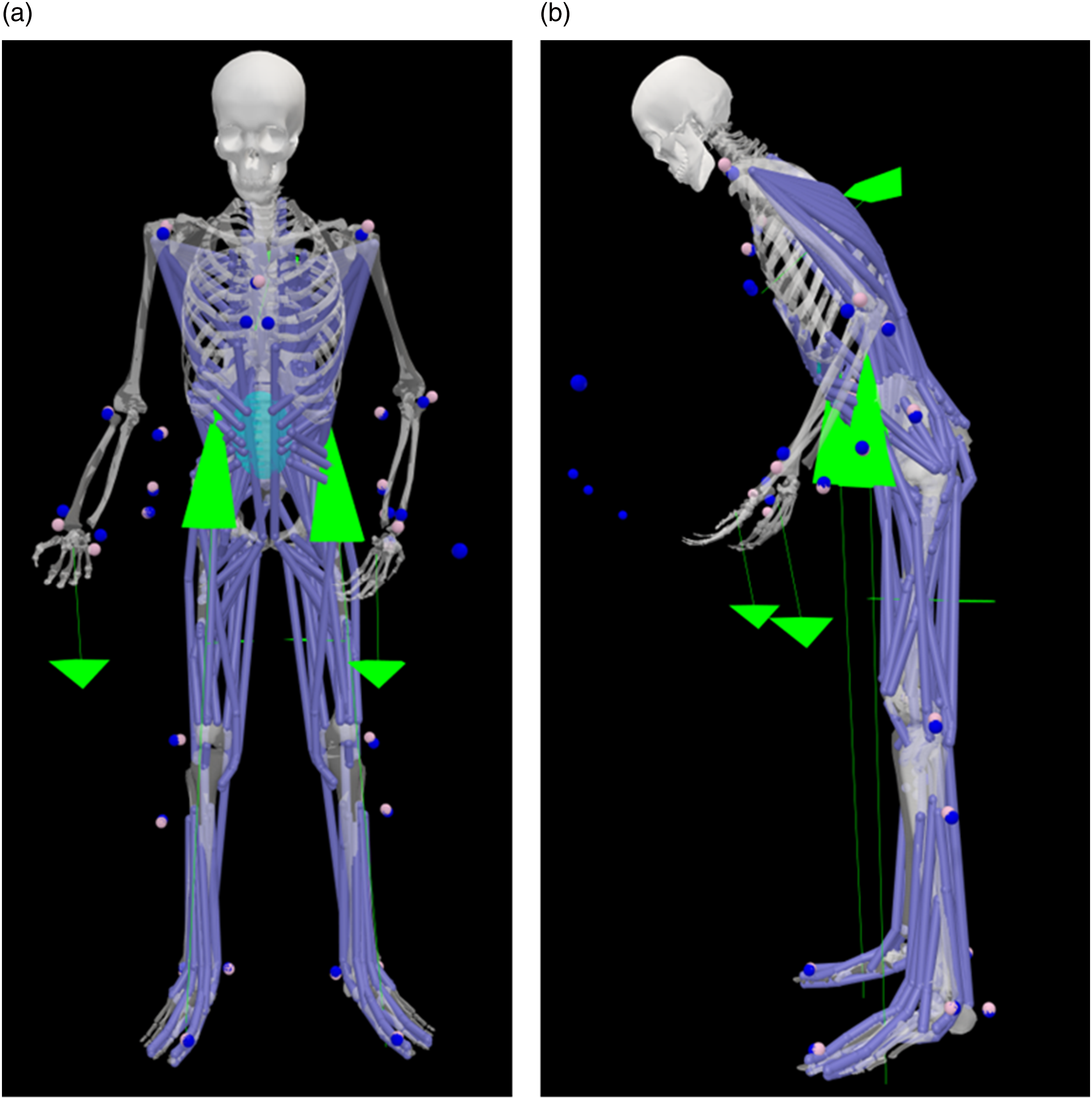
The modeling procedure followed a series of standard steps in OpenSim (Figure 4). The initial step involved generating two subject-specific models, one with and one without the exoskeleton, by scaling a generic model using surface marker data obtained from the subjects during a static stance trial, both with and without the exoskeleton. In the inverse kinematics procedure, the model determined the joint angles of the entire body by matching the virtual marker motions with measured surface marker motions obtained during dynamic trials. In the inverse dynamics procedure, the joint torques were derived from the inverse kinematics results and all the external forces, including GRFs, Exo forces, and hand forces. The logic diagram for constructing a subject-specific biodynamic model under WITH exoskeleton condition in OpenSim.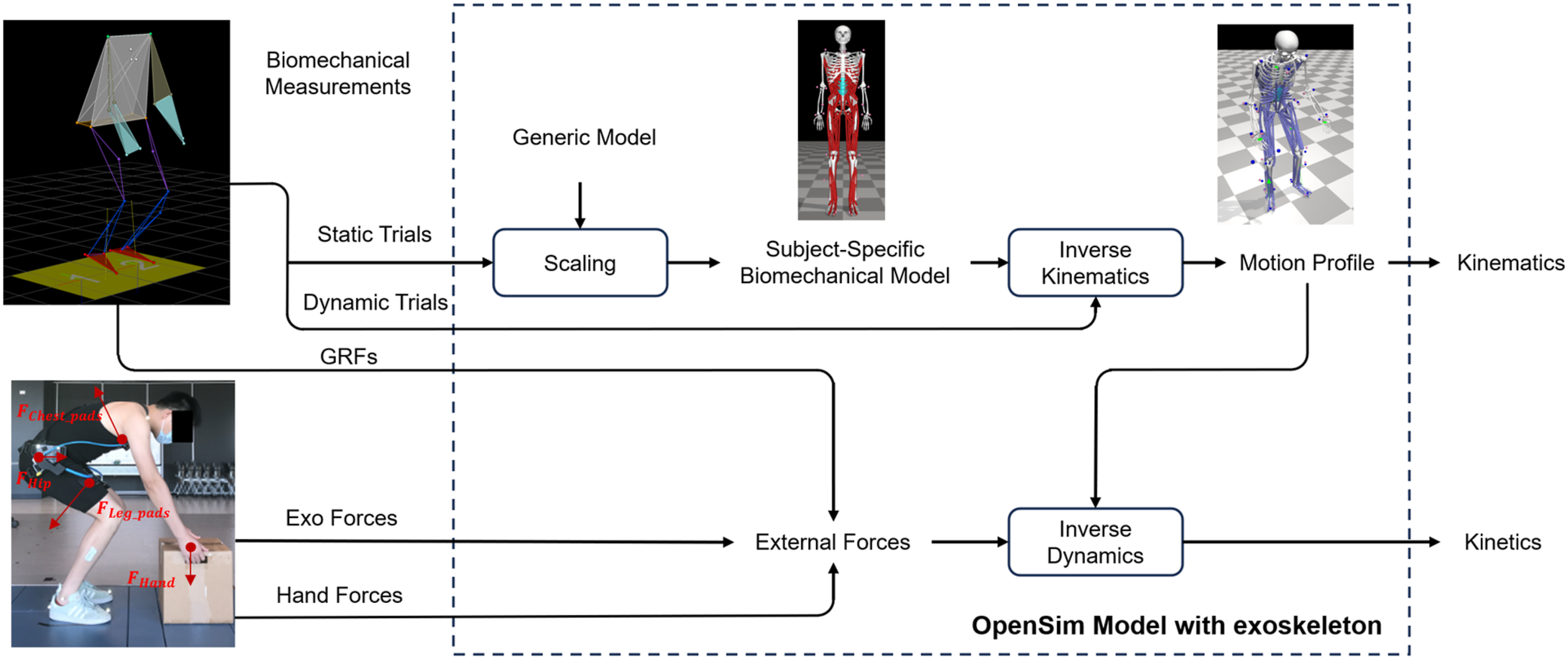
The dynamic modeling focused on the lifting phases in all tasks (r, a, b, and c). The modeling time frame started from the static upright posture assumed in all the tasks and ended when the subject just finished lifting the weight (r) or the patient (a, b, and c) to the designated position. These frames were determined by examining the velocity and acceleration profiles of two markers on the shoulders (LSHO and RSHO).
Model Validation
The reference task of symmetric two-handed load lifting, with known hand forces and GRF measurements, was designed to provide an opportunity to validate the subject-specific biodynamic models by comparing the estimated GRFs with the measured GRFs, with and without exoskeleton. The GRFs were estimated based on the top-down approach according to the following relationship:

A low RMES value showed the high accuracy of the parameters in computing the estimated GRFs using the relationship above, including the hand force estimates (
In addition, while the residual errors accumulated at the end-effector are expected to be identical between the top-down and bottom-up methods (Riemer et al., 2008), a bottom-up calculation of the hand forces (

This validation provides a foundation for utilizing the established relationship to estimate hand forces in the more complex patient handling tasks where
Statistical Analysis
Paired t-tests were employed to examine the effects of the exoskeleton on selected joint kinematic and kinetic variables. For variables that were not normally distributed, the Wilcoxon Signed Rank test was applied. The analysis was conducted on all subjects, with tasks as the grouping factor. To identify possible sex differences, paired t-tests were conducted to analyze the peak lumbar joint angle and moment, and the Wilcoxon Signed Rank test was also used for nonnormally distributed variables. Data were grouped by exoskeleton condition and tasks. A significance level of 0.05 was applied for all tests.
Results
Effects on Joint Kinematics
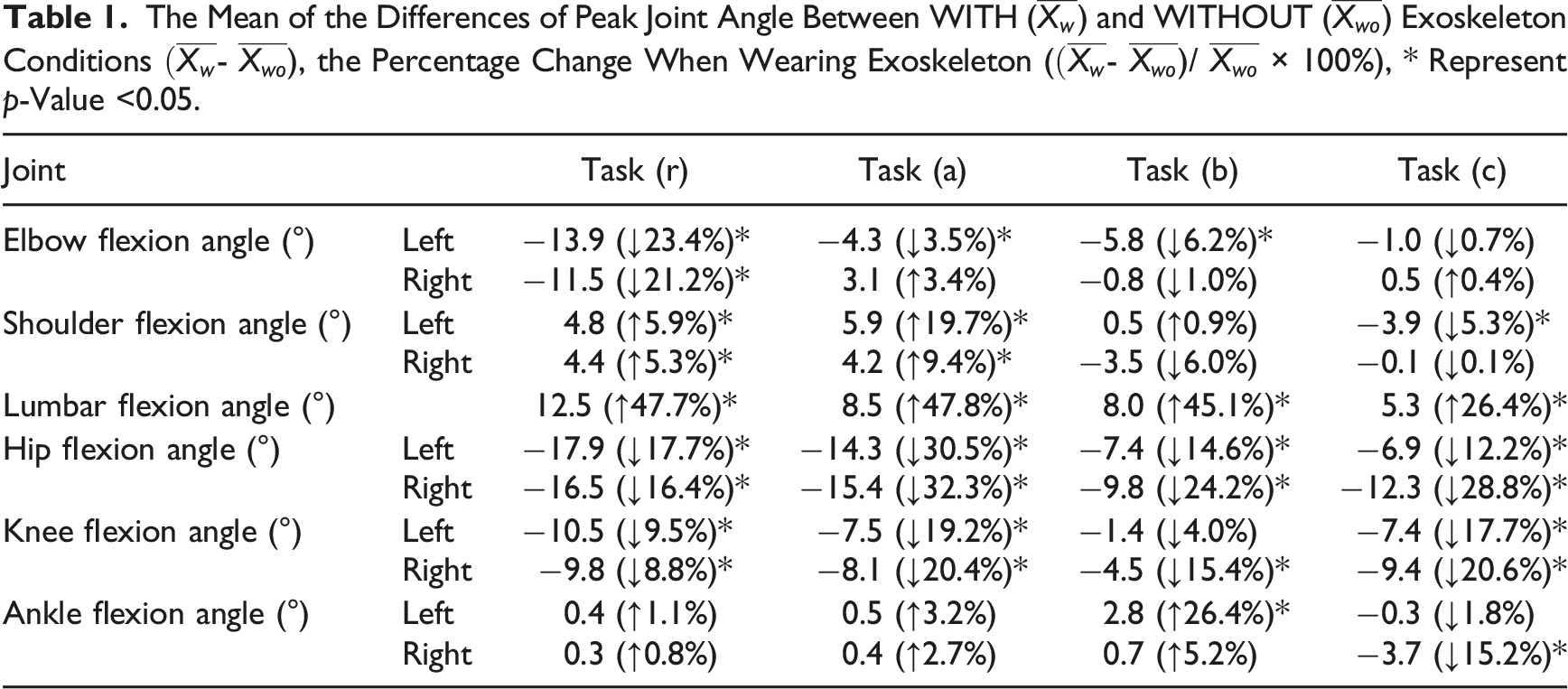
Wearing the exoskeleton significantly increased the peak lumbar flexion (p < 0.001) during tasks (r), (a), (b), and (c) by 47.7%, 47.8%, 45.1%, and 26.4%, respectively. Both the left and right hip peak flexions exhibited significant reductions (p < 0.001) ranging from 12.2% to 32.3% across all the tasks (Figure 5, Table 1). Both the left and right knee peak flexions were significantly reduced (p < 0.001) during all tasks except for the left knee flexion during task (b). No significant change (p > 0.05) was found in the ankle flexion angle during tasks (r) and (a). For the upper extremity, significantly increased (p < 0.05) peak shoulder flexions for both the left and right sides were found during task (r) and (a) and significantly reduced peak elbow flexions were observed in task (r) for both hands (p < 0.001), as well as in tasks (a) and (b) for the left elbow (p < 0.05). Peak joint motions across major joints (lumbar, hips, knees, ankles, shoulders, and elbows), with and without exoskeleton, during tasks (r), (a), (b), and (c). In task (r), each participant completed 5 trials with and without exoskeleton, resulting in a total of 60 data points per box. For each of the patient handling tasks (a, b, or c), participants completed 6 trials under the same conditions, yielding 72 data points per box. An asterisk (*) denotes a significant difference. The Mean of the Differences of Peak Joint Angle Between WITH (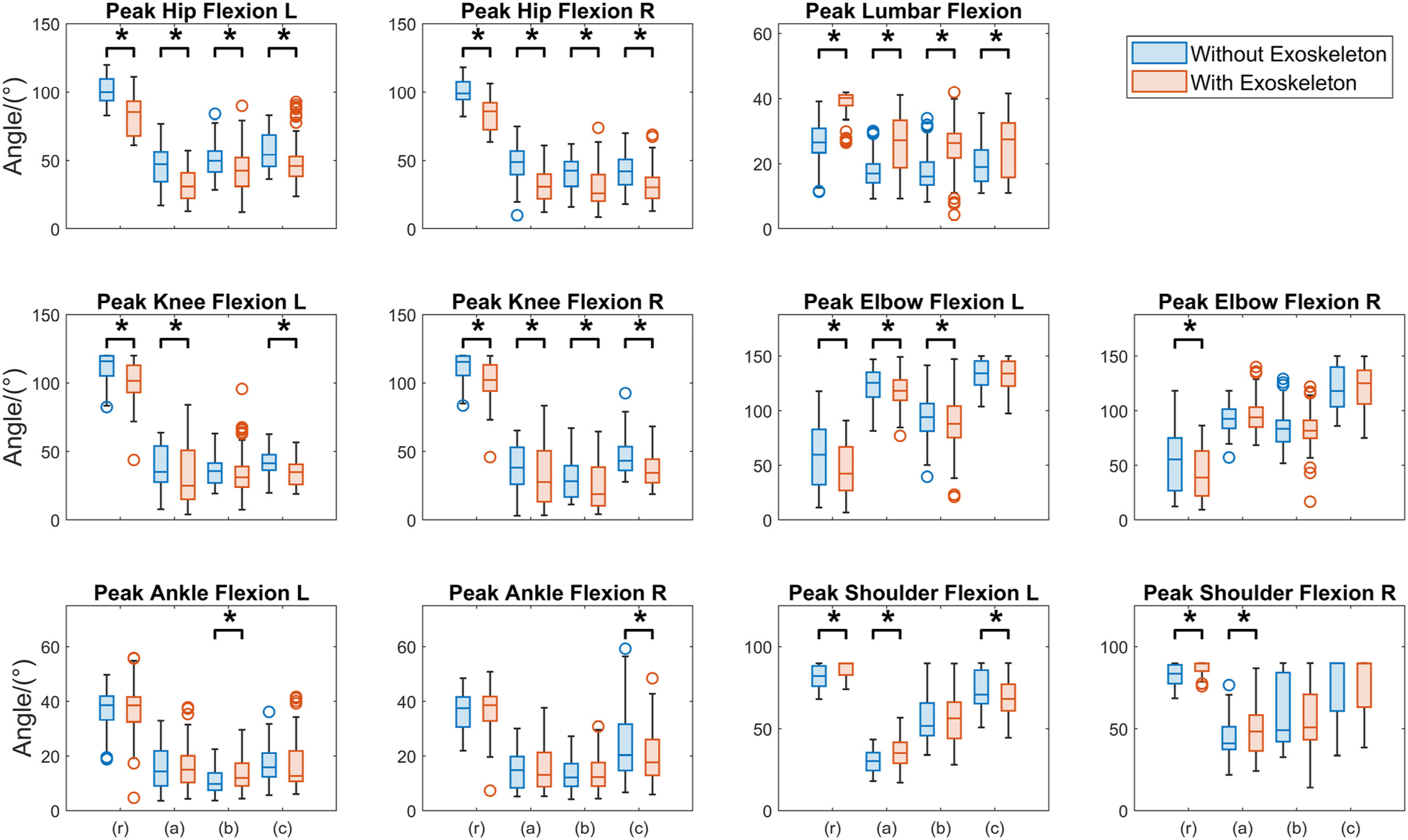
Effects on Joint Kinetics
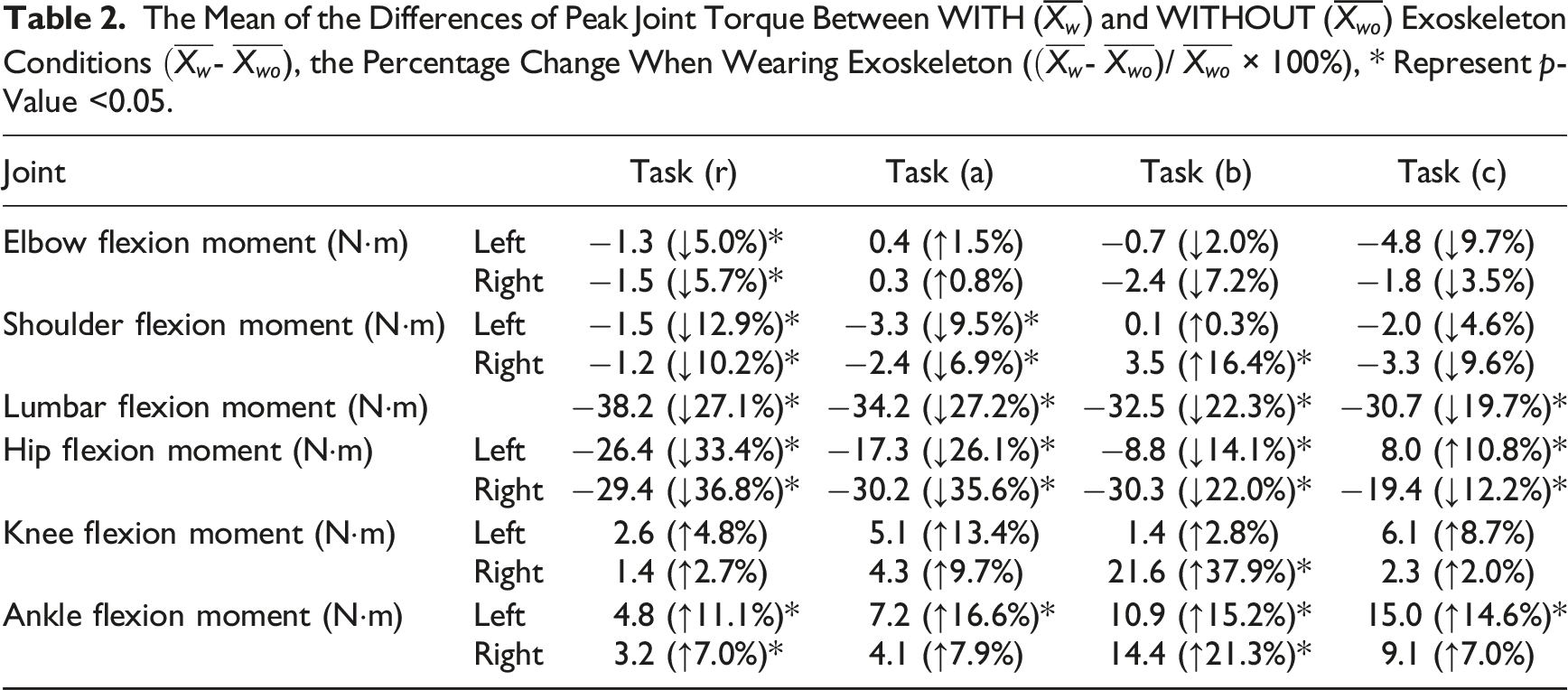
Wearing the exoskeleton significantly reduced the peak lumbar flexion moment (p < 0.001) during tasks (r), (a), (b), and (c) by 27.1%, 27.2%, 22.3%, and 19.3%, respectively, and reduced both left and right peak hip flexion moment (p < 0.001) by 10.8%–36.8% across all the tasks (Figure 6, Table 2). A significant reduction in peak shoulder flexion moment was observed in tasks (r) and (a), for both the left and right sides (p < 0.05). Additionally, a decrease in peak elbow flexion moment was identified specifically in task (r) (p < 0.05). No significant change was found in knee flexion moment during any of the tasks, other than a marked increase (p < 0.001) in the right knee flexion moment during task (b). Significant increases in the peak ankle flexion moment (p < 0.05) were observed in both ankles during tasks (r) and (b) and in the left ankle during tasks (a) and (c). Peak joint torques across major joints (lumbar, hips, knees, ankles, shoulders, and elbows), with and without exoskeleton, during tasks (r), (a), (b), and (c). An asterisk (*) denotes a significant difference. The Mean of the Differences of Peak Joint Torque Between WITH (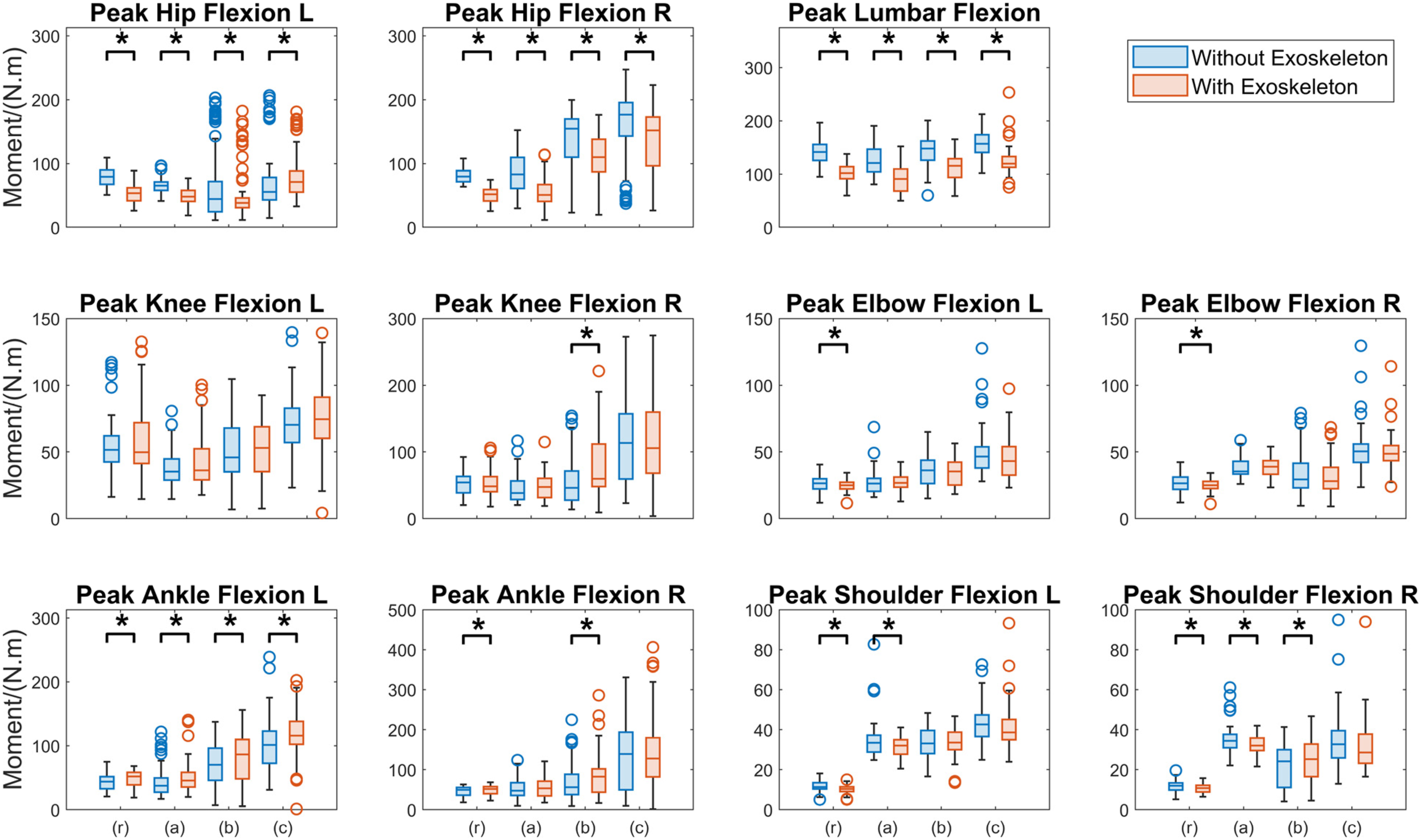
Sex Effect
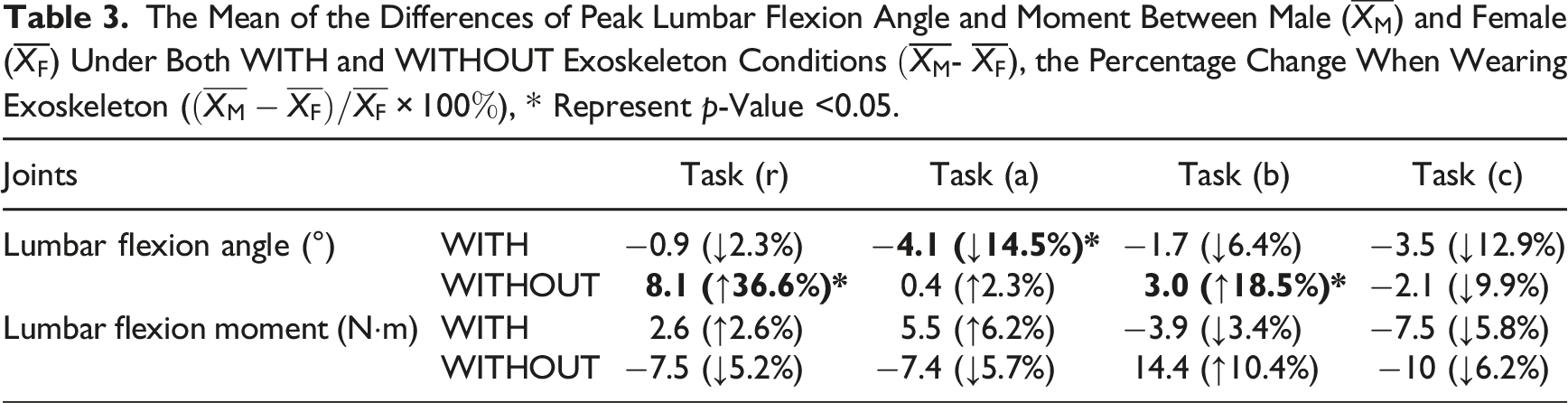
Significantly (Cohen’s d = 1.486, p < 0.001 for task r, Cohen’s d = 0.486, p = 0.024 for task b) greater lumbar flexions were exhibited by males than females during tasks (r) and (b) without the exoskeleton (Figure 7, Table 3). Note this effect could have been due to the height difference between the two groups, which was not the case given the minimal sex difference in stature. This sex difference in lumbar flexion motion diminished under the with exoskeleton condition. Further, there was no significant sex effect on lumbar flexion moment during any of the tasks, regardless of whether the exoskeleton was worn or not. A between-sex comparison of the peak lumbar flexion motion and moment across all four tasks. An asterisk (*) denotes a significant difference. The Mean of the Differences of Peak Lumbar Flexion Angle and Moment Between Male (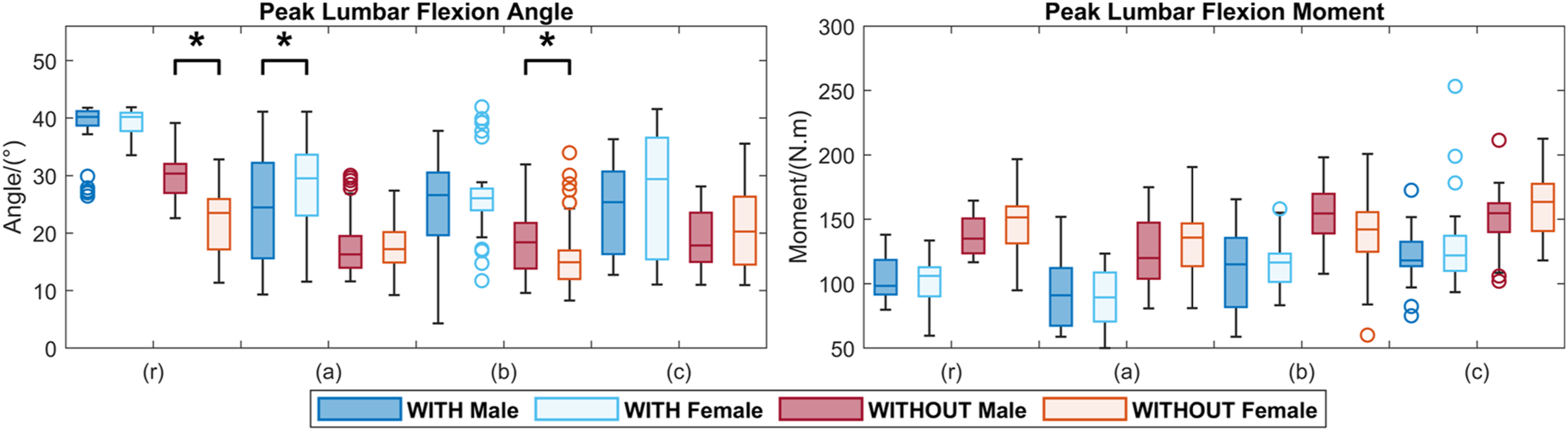
Model Validation
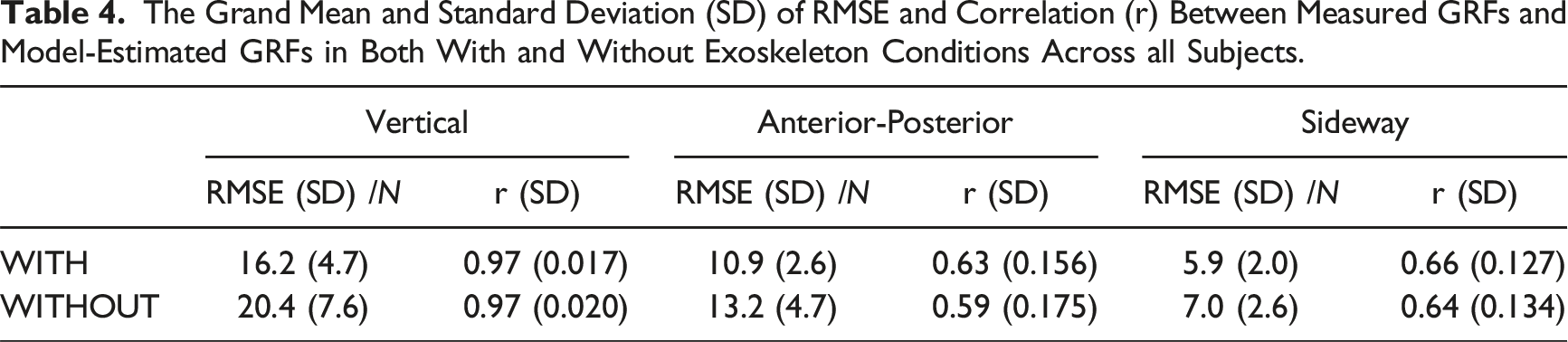
The grand mean RMSE that quantified the overall discrepancy between measured and inverse-dynamics (ID)-estimated vertical GRFs across all subjects during lifting trials was found to be 16.2 N and 20.4 N, with and without the exoskeleton, respectively; the coefficient of correlation r was 0.97 (Figure 8, Table 4). For the anterior-posterior and sideway forces, the RMSE ranged from 5.9 N to 13.2 N while r ranged from 0.59 to 0.66. Representative GRF profiles (subject01, BW = 72.4 kg) as model validation results, with (upper panels) and without (lower panels) exoskeleton. The solid lines are the measured GRF mean, the colored dashed lines are the estimated GRFs mean, and the shaded areas are the mean ± SD. The vertical black dash lines represent the mean timeframe at which the hands made initial contact with the load; to the left is the lowering phase and right is the lifting phase. The Grand Mean and Standard Deviation (SD) of RMSE and Correlation (r) Between Measured GRFs and Model-Estimated GRFs in Both With and Without Exoskeleton Conditions Across all Subjects.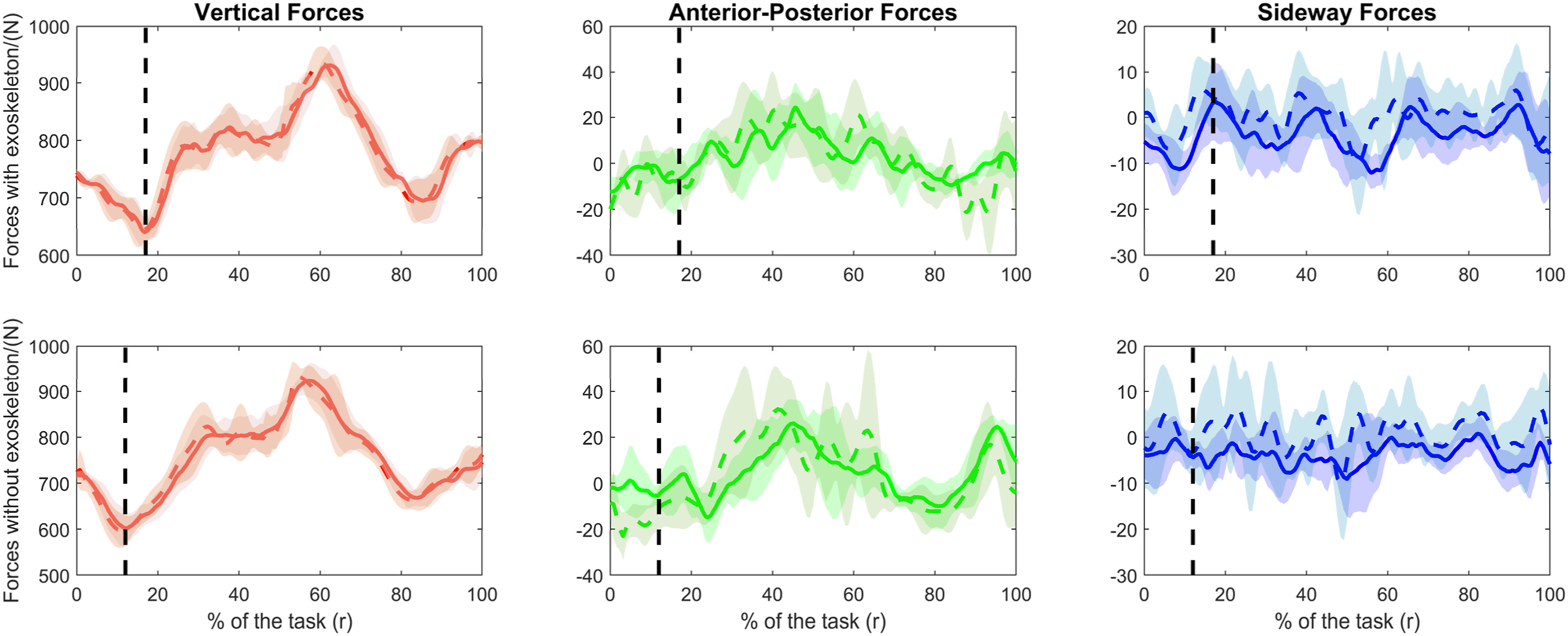
Discussion
In this study, we successfully constructed subject-specific biodynamic models of a group of subjects performing patient handling tasks, with or without wearing an exoskeleton, and used these models for an in silico investigation of the biomechanical consequences of the exoskeleton. Two novel solutions contributed by this study are (1) the representation of human-exoskeleton force interactions in modeling and (2) the design of lifting tasks with known hand forces into the experiment to allow validation of model prediction. According to the modeling recommendation protocol (Hicks et al., 2015), the model validity was considered good, as it fell within 2 SD when compared to similar motions. The low magnitude RMSE and the high correlation coefficient r (Kodama & Watanabe, 2016) between the measured GRFs and the top-down estimated GRFs during lifting trials, with and without exoskeleton, provides additional confidence to the models.
In several simulation-based studies of HEI, the condition with the exoskeleton was modeled based on the motion data from subjects not wearing the exoskeleton. For instance, Agarwal et al. (2016) developed a model with a simulated sinusoidal flexion-extension trajectory, while Jones et al. (2023) and Manns et al. (2017) constructed their models from motion data of subjects not wearing an exoskeleton. In the present study, we model the HEI using real motion data collected from participants wearing the exoskeleton and incorporate the interactive forces directly into the actual exoskeleton-assisted movements.
We identified a trade-off between lumbar flexion motion and flexion moment introduced by using a passive back exoskeleton. Wearing the exoskeleton incurred a decrease in peak lumbar flexion moment, indicating a reduction in the lumbar loading, which is consistent with findings from previous investigations (Bosch et al., 2016; Hwang et al., 2021; Koopman et al., 2019, 2020; Madinei & Nussbaum, 2023). However, this reduction was accompanied by an increase in peak lumbar flexion motion, suggesting more aggressive and dynamic torso movement when the exoskeleton was worn. This was corroborated by an inspection of the angular acceleration of the lumbar joint and the duration of the task: despite the extended lifting duration while wearing the exoskeleton for tasks r (Cohen’s d = 0.888, p < 0.001), a (Cohen’s d = 0.491, p = 0.001), b (Cohen’s d = 0.340, p = 0.001), and c (Cohen’s d = 0.179, p = 0.085), notable increases in peak angular acceleration at the lumbar joint were observed across all tasks but task c, which was the most challenging task (Cohen’s d = 0.731, p < 0.001 for task a, Cohen’s d = 0.397, p = 0.005 for task b, Cohen’s d = 0.311, p = 0.062 for task b, and Cohen’s d = 0.133, p = 0.446 for task c). This suggests that the exoskeleton “empowers” handlers in utilizing their back motion. Even though wearing the exoskeleton may lead to increased peak lumbar flexion, the added support from the “exoskeleton spine” helps re-distribute the lumbar loads, resulting in a reduced peak lumbar flexion moment. The exoskeleton was found to alter the handlers’ movement strategy, encouraging a greater lumbar flexion motion, consistent with findings from a previous study (Hwang et al., 2021). This forward trunk bending may also be a compensatory response to the perceived stiffness or constraints imposed by the exoskeleton on the lower limbs. Although increased trunk flexion can lead to a greater trunk moment due to an extended moment arm between the lumbar spine and the torso’s center of mass, the additional support provided by the exoskeleton may effectively reduce the overall loading to the lumbar region. While previous studies involving healthcare workers performing patient-assisting tasks did not report lumbar moment data, the L5/S1 disc compression forces obtained from the current study were comparable in order of magnitude to what was reported (Banks et al., 2024; Jager et al., 2013; Troster et al., 2020). A similar trade-off was observed between shoulder flexion moment and motion: with the use of the exoskeleton, the shoulder flexion motion increased while the shoulder flexion moment decreased, but only during the more symmetric lifting task (r) and task (a).
The task-dependent impact of an exoskeleton (Kuber et al., 2022) was also evidenced in this study. For instance, the percent decrease in lumbar flexion moment and thus the spine loading was greater in more symmetric handling tasks (r and a) and less in more asymmetric, complex handling tasks (b and c). As Laevo was designed mainly for assisting repeated load lifting (Baltrusch et al., 2019), its biomechanical benefits could be curtailed for more complex, asymmetric handling tasks such as patient transfer and assistance (Zhu et al., 2021). From a whole-body biomechanics point of view, the exoskeleton appeared to influence the overall movement of the hip, knee, elbow, shoulder, and lumbar joints: individuals tended to adopt a more prudent, “motion economy” (not necessarily moment economy) strategy in hip, knee, and elbow joint motions while promoting a more aggressive approach in their lumbar and shoulder joints when performing tasks (r and a). Although the knee and ankle moments may increase due to the additional weight of the exoskeleton, this adaptation strategy highlights the exoskeleton’s effectiveness in redistributing joint movements and mechanical loads, ultimately reducing the overall risk of injury. This endorses the exoskeleton in providing assistance where needed, contributing to safer and more efficient task execution. On the other hand, it also highlights the importance of design issues such as whether back exoskeletons should be made to better suit different types of manual handling and what the typology should be.
The current study may have unveiled a potential sex difference in lumbar motion responses to the exoskeleton when performing tasks (r) and (b). Without wearing the exoskeleton, males tended to bend more when compared to females, which has been previously reported (Plamondon et al., 2014). However, an interesting finding is that under the exoskeleton condition, no sex effect on lumbar flexion angle was detected. This suggests that the use of an exoskeleton may reduce the variability in motion between sexes and potentially across individuals in general, particularly for relatively simple symmetric lifting motions.
Several limitations of this study are acknowledged. First, this was a laboratory-based study employing laboratory-bound force plates, marker-based motion capture systems, and time-consuming subject-specific biomechanical model building. There remain technological barriers to real-time naturalistic studies of HEI, especially when complex, highly dynamic tasks are involved. We believe a potential solution lies in the nascent flexible sensor technology (Yin et al., 2023). Second, direct measurement of the exoskeleton forces and hand forces remains a formidable challenge. While a top-down validation protocol was devised to take advantage of lifting trials with known hand forces, it was limited to scenarios when forces are predominantly in the vertical direction. Third, this study used college students to represent novice workers having first-time exposure to exoskeleton use. Exploring how novice workers learn to adapt exoskeletons as compared to skilled workers, with or without exoskeleton experience, would be a worthy research topic. Finally, given the limited sample size, caution must be exercised when interpreting the exoskeleton’s sex-specific results. Further studies with larger sample sizes are warranted to confirm these sex-specific effects.
Conclusion
In this study, we developed a subject-specific modeling approach to examine the biodynamics of human-exoskeleton interactions. Using the subject-specific models, we identified significant effects of wearing a passive back exoskeleton on whole-body joint kinematics and kinetics during simulated patient-handling tasks, revealing notable task dependencies and potential sex differences. The approach and findings can help better understand the role of exoskeletons in promoting safer patient handling and better design future generation exoskeletons.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC). Mention of any company or product does not constitute endorsement by NIOSH/CDC.
Key Points
• Two types of subject-specific biodynamic models, with and without wearing an exoskeleton, were constructed for a group of subjects during patient handling tasks. • A validation process was conducted for the lifting task, ensuring both the models and the hand forces estimation method could be extended to patient handling tasks. • A trade-off between lumbar flexion motion and flexion moment introduced by the use of a passive back exoskeleton in the selected patient handling tasks was identified. • The use of an exoskeleton may reduce the variability in motion between sexes and potentially across individuals in general, particularly for relatively simple symmetric lifting motions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Occupational Safety and Health.