
Abstract
Objective
The goal of this study was to evaluate the prevalence and change in perception of physical discomfort, including musculoskeletal discomfort, during the COVID-19 pandemic and to determine associations of demographic factors, telework activity, and home office characteristics with the highest prevalence of discomfort.
Background
The COVID-19 pandemic forced a substantial increase in telework in many countries. The sudden change from a regular workplace to an improvised “home office” may have an impact on working conditions and physical symptoms of office workers. However, investigations in this area remain limited.
Method
A cross-sectional study design was used to compare self-reported complaints of physical discomfort perceived from before with those during the pandemic. Associations between complaints and home office characteristics were investigated from 150 faculty and 51 administrative staff of an academic institution with an age range of 41.16 ± 10.20 (59% female).
Results
A significant increase of physical discomfort was found during the pandemic period for head, eyes, hand, and upper back for both staff and faculty and neck, shoulders, elbows, and lower back for faculty only. Logistic regression analyses point to associations with the lack of a laptop stand, uncomfortable desk, poor lighting, and sitting time, among others.
Conclusion
A high prevalence of physical discomfort was reported by teleworkers during the COVID-19 pandemic. Some home office characteristics were associated with these discomforts.
Application
Some telework characteristics seem to be risk factors for physical discomfort. Consideration should be given to teaching best practices for workstation setup and/or conducting other preventive interventions in the work environment.
On March 11, 2020, the World Health Organization (WHO) declared the coronavirus disease (COVID-19) to be a pandemic (WHO, 2020). In response to the global situation, many countries established strategies to prevent the spread of the virus, including quarantine plans, cancelation of public events, restriction of mobility, closing of nonessential businesses, and home confinement, among others. The majority of schools and universities were recommended or required by governments to close their premises. Since March 15, 2020, the national educational system in Ecuador was required to cancel on-campus classes and all faculty and staff to work from home (COE, 2020). This continued up to August 2021. “Working from home,” or home-based telework, has been defined as a form of work that uses information and communication technology such that workers are able to fulfill their occupational tasks while remaining at home (ILO, 2020).
Before the COVID-19 outbreak, only a small percentage of people had ever teleworked. For example, 15% of the EU workforce (European Commission, 2020) and 14.6% of the US labor force (Brynjolfsson et al., 2020) had worked from home. In Ecuador, only 12,888 employees were registered as teleworkers before the pandemic, which increased to 436,484 during the pandemic (Echeverria, 2020). Many workers were then required to shift abruptly to telework, hence, to face multiple challenges, including how to set up their home office space. It is highly probable that many workers who shifted to telework did not have the equipment or workstation infrastructure at home that allowed them to apply best practices for workstation setup (Siqueira et al., 2020). Moreover, their occupational sedentary behavior may have expanded due to the loss of activity such as teaching and laboratory work, or displacements to other locations. Computer office work is commonly characterized by prolonged sedentary time (Kirk & Rhodes, 2011; Parry & Straker, 2013), insufficient physical workload/exercise (Straker & Mathiassen, 2009), and prolonged uninterrupted sitting time (Ryde et al., 2013).
Several musculoskeletal disorders (MSDs) have been associated with these office work characteristics: an increase in musculoskeletal discomfort (Baker et al., 2018; Waongenngarm et al., 2020) a high prevalence (>50%) of low back (Bontrup et al., 2019; Celik et al., 2018), neck (Celik et al., 2018; Collins & O’Sullivan, 2015), and upper limb (Coenen et al., 2018; Harcombe et al., 2009; Gerr et al., 2004) pain. In addition, other physical discomforts, such as eye and head discomfort, have been associated with extensive computer work (Besharati et al., 2020).
Inappropriate workstation design, such as incorrect chair height and the lack of arm and back rests, has been related to upper limb pain (Rodrigues et al., 2017). Musculoskeletal pain in the back and neck area during office work has been related to inadequate support of the chair, the keyboard and mouse setup, head inclination while working (Celik et al., 2018), number of displays and display location (Zuniga & Côté, 2017), and other workstation characteristics. Conversely, the physical arrangement of the office and work environment is a critical component in the prevention of work-related physical discomfort and musculoskeletal pain (Celik et al., 2018; Mohammadipour et al., 2018; Ye et al., 2017).
The extent to which office workers were able to arrange their home working area according to best-practice guidelines during the COVID-19 pandemic was unknown, and it is likely that the consequence of the abrupt change from their common office workstation to the telework home office could result in an increase in physical discomfort. Thus, as telework expanded tremendously during the COVID-19 pandemic, the present study aimed (a) to investigate the prevalence and change in physical discomfort, including musculoskeletal discomfort, self-reported by faculty and administrative staff of an academic institution before and during the pandemic and (b) to determine whether and which demographic factors, home office and job characteristics, are associated with an increase in self-reported discomfort of specific body areas.
METHOD
Participants
The present study consisted of a cross-sectional design targeting the faculty and administrative staff of an academic institution, located in Quito, Ecuador, that were required to work from home during the COVID-19 pandemic. Inclusion criteria were an active full-time employment for at least 2 years at the institution and requirement for telework. Faculty and staff were invited to participate in the study via email in November 2020. Over a period of two months, 201 (25% of the total faculty and staff population) surveys were returned from 150 faculty and 51 staff. These included 119 women and 82 men with a mean ± standard deviation (M ± SD) age of 41.16 ± 10.20 years, height of 167.44 ± 9.08 cm, weight of 67.58 ± 13.99 kg, and BMI of 23.96 ± 3.82. All participants signed an informed consent form prior to responding to the survey. The study was approved by the Ethics Committee of the Universidad San Francisco de Quito (# 2020-058IN) and complied with the tenets of the Declaration of Helsinki.
Questionnaire
The study design involved the collection of quantitative and qualitative data through an online survey consisting of 54 questions in Spanish divided into five sections. The first section consisted of demographic questions including age, weight, height, gender, job position, time at current job, days/week of telework, hr/week of telework, and any other job performed.
The second section included a physical discomfort questionnaire, adapted from the Cornell Musculoskeletal Discomfort Questionnaires (Carrasquero, 2015; Hedge et al., 1999) and the Nordic Questionnaire (Dawson, et al., 2009; Kuorinka et al., 1987), in which participants were asked to rate the severity and frequency of discomfort of 10 body parts, perceived during the 12 months before the pandemic confinement (retrospective report of discomfort from their office work before March 2020), and during the pandemic confinement (from March 2020 up to the moment they completed the survey). Severity of discomfort was rated and weighted as follows: none = 0, slightly uncomfortable = 1, moderately uncomfortable = 2, and very uncomfortable = 3. Frequency of discomfort was rated and weighted as follows: never = 0, 1–2 times a week = 1.5, 3–4 times a week = 3.5, once a day = 5, or several times a day = 10.
The third section, which referred to work activity, included questions regarding hr/workday sitting, hr/workday standing, hr/workday walking, activities in leisure time, hr/week performing mild and/or high intensity leisure activities, type of rest-breaks during telework, duration of rest-breaks during telework, and number of rest-breaks during telework.
The fourth section referred to workstation characteristics such as the chair, table or desk, desktop/laptop computer, accessories, and postures. This section included questions regarding seat height, seat cushioning, chair stability, backrest adjustability, armrests, head rest, sitting posture, table/desk height, forearm angle, monitor position, and type of computer (desktop vs. laptop), among others. These questions were selected specifically for the target groups from validated surveys and checklists including ROSA (Diego-Mas, 2019; Sonne et al., 2012), OSHA’s computer workstation e-tool checklist evaluation (OSHA, n.d.), and the European Working Conditions questionnaire (Eurofound, 2015). The last section included an overall comparison of the current home office workspace with the on-campus office, and desired changes to the home office.
Analysis
A two-step analysis was carried out. First, the total discomfort scores (weighted rating scores mean) for physical discomfort frequency and severity were obtained by multiplying the two dimensions for each body area. For each group and category, before and during the COVID-19 pandemic, scores were compared using Wilcoxon signed-rank test for each outcome variable (severity, frequency, and total discomfort), respectively. Then, body areas were selected for a logistic regression analysis if at least two of their discomfort outcome variables significantly increased during the pandemic. These ratings were dichotomized with 1 for severe and moderate discomfort with frequencies of 3–4 times a week, once a day and/or several times a day, and 0 for the none and slight discomfort with frequencies of never and/or 1–2 times a week. The other 46 multiple choice or quantitative questions were dichotomized with 0 corresponding to none, low or moderate exposure, or good workstation design (according to best-practices and guidelines) and 1 representing high exposure or poor workstation design (not according to best-practices and guidelines).
Open-ended questions, questions with skewed distribution having less than 10% of responses on either side, and questions with more than 10% of missing values were discarded from the statistical analysis. Thus, 37 questions (variables) were used for chi-square goodness of fit testing to evaluate correlations for each significant body area. The variables with a phi coefficient equal to or lower than 0.1 and a p-value > .25 (Agresti, 2002) were not considered in the logistic regression analysis. Overall, between 5 and 11 variables were used for the logistic regression analysis of each body area.
Odds ratio (OR) and confidence limits (CL) were obtained using a stepwise logistic regression for the total discomfort score of each significant body area at p = .05. Age and gender were forced into the models. Age was classified in two groups, <50 and ≥50 years old, dichotomized as 0 and 1, respectively. For gender, males and females were, respectively, dichotomized as 0 and 1. All statistical analyses were performed with SAS Studio (SAS Institute, North Carolina, USA). The variable names presented in the result sections were shortened and translated from the original questionnaire. The questionnaire and complete questions can be found in the supplementary material of this manuscript. All logistic regression models fulfilled the Hosmer and Lemeshow Goodness of Fit Test. Nagelkerke’s R square is presented in the results for each model.
RESULTS
Severity, Frequency, and Total Scores of Physical Discomfort in Faculty and Staff
Severity, Frequency, and Total Scores of Physical Discomfort Reported by Administrative Staff
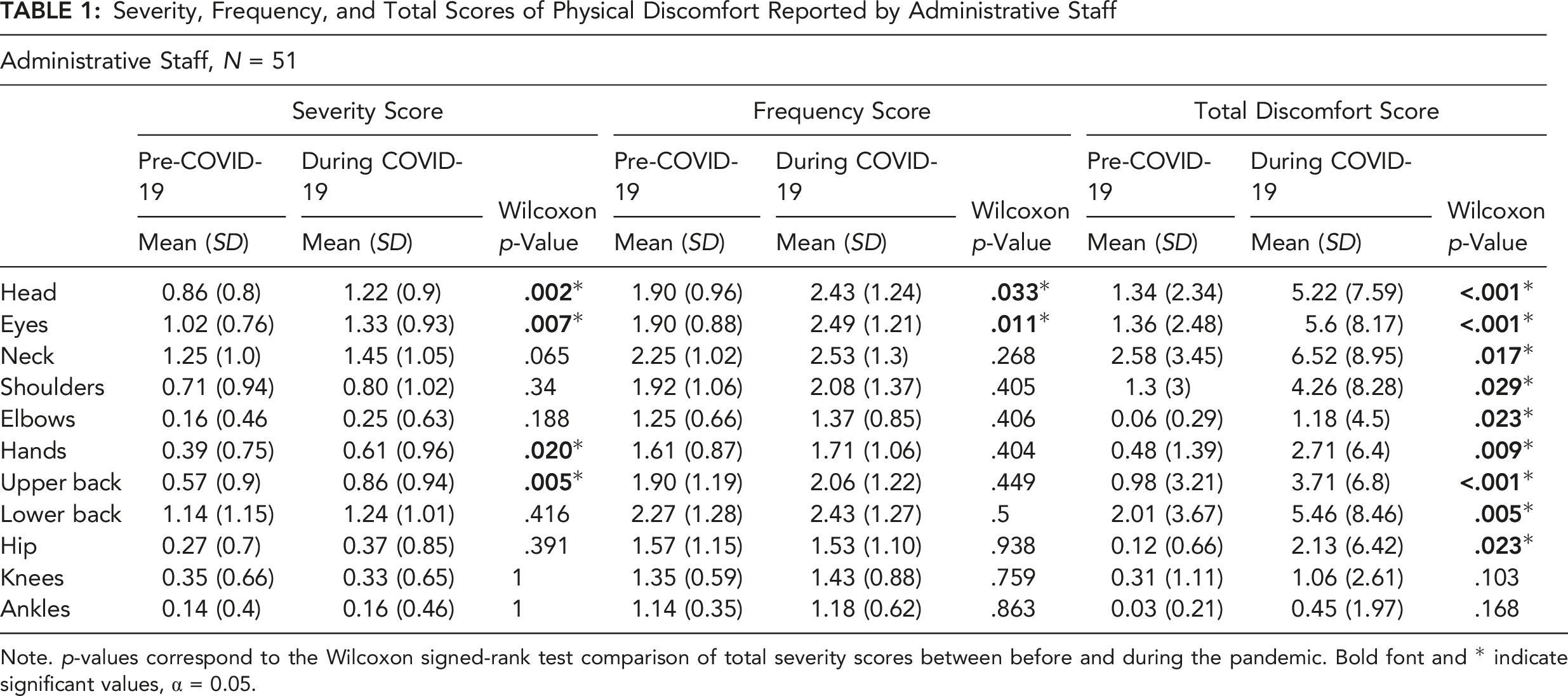
Note. p-values correspond to the Wilcoxon signed-rank test comparison of total severity scores between before and during the pandemic. Bold font and * indicate significant values, α = 0.05.
Severity, Frequency, and Total Scores of Physical Discomfort Reported by Faculty
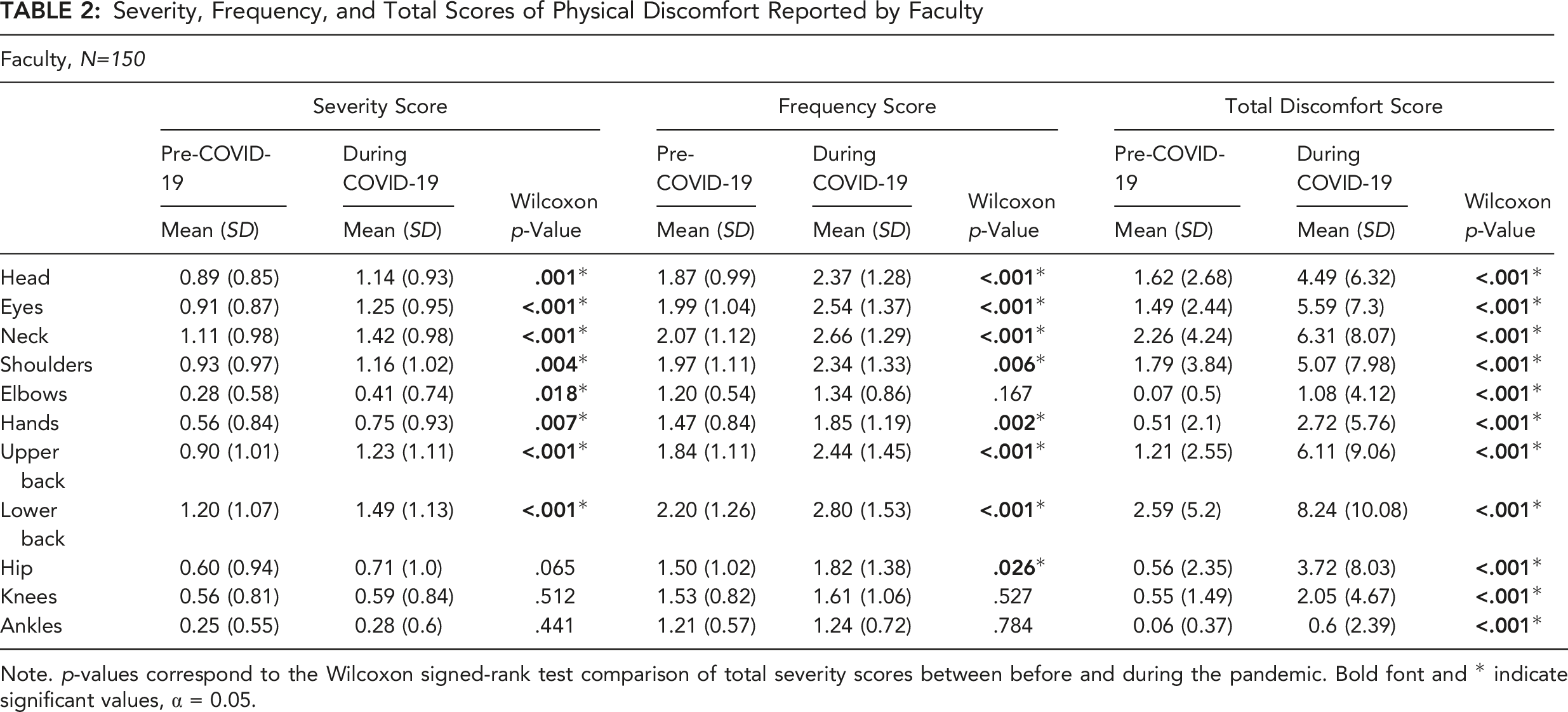
Note. p-values correspond to the Wilcoxon signed-rank test comparison of total severity scores between before and during the pandemic. Bold font and * indicate significant values, α = 0.05.
The frequency of physical discomfort for staff was significantly higher (p < .05) for total frequency scores (weighted rating scores mean) during the pandemic for head (54.90% vs. 74.51% with answers including “Slightly frequent” to “Always”) and eyes (62.75% vs. 80.39%). For faculty, a significant increase (p < .05) of total frequency scores during the pandemic was observed for head (56.67% vs. 70.75%), eyes (62.00% vs. 76.03%), neck (66.67% vs. 81.21%), shoulders (59.33% vs. 68.46%), hands (30.00% vs. 47.30%), upper back (49.33% vs. 67.35%), lower back (62.67% vs. 74.15%), and hip (27.52% vs. 32.89%). Overall, for staff, the highest prevalence of “very frequent” and “always” ratings during the pandemic were found for head (21.5%), eyes (23.5%), and neck (27.5%). For faculty, the highest prevalence of “very frequent” and “always” ratings were found for the lower back (40.2%), eyes (28.8%), and neck (28.2%). For “always” ratings only, the highest frequency was found for neck (9.8%) and lower back (11.8%) of staff and upper (13.6%) and lower back (19.1%) of faculty.
For the total discomfort scores, results showed that for staff, the total discomfort scores were significantly higher (p < .05) during the pandemic for head, eyes, neck, shoulder, elbow, hand, upper back, lower back, and hips. For faculty, the total discomfort scores were significantly higher (p < .05) during the pandemic for all body areas. Overall, the greatest increase was observed for eye discomfort of staff and lower back discomfort of faculty. Moreover, the highest scores (above 5 points) of total discomfort during the pandemic was found for head, eyes, neck, and lower back for staff (Table 1) and eyes, neck, shoulders, upper back, and lower back for faculty (Table 2).
Overview of Telework Characteristics for Administrative Staff and Faculty
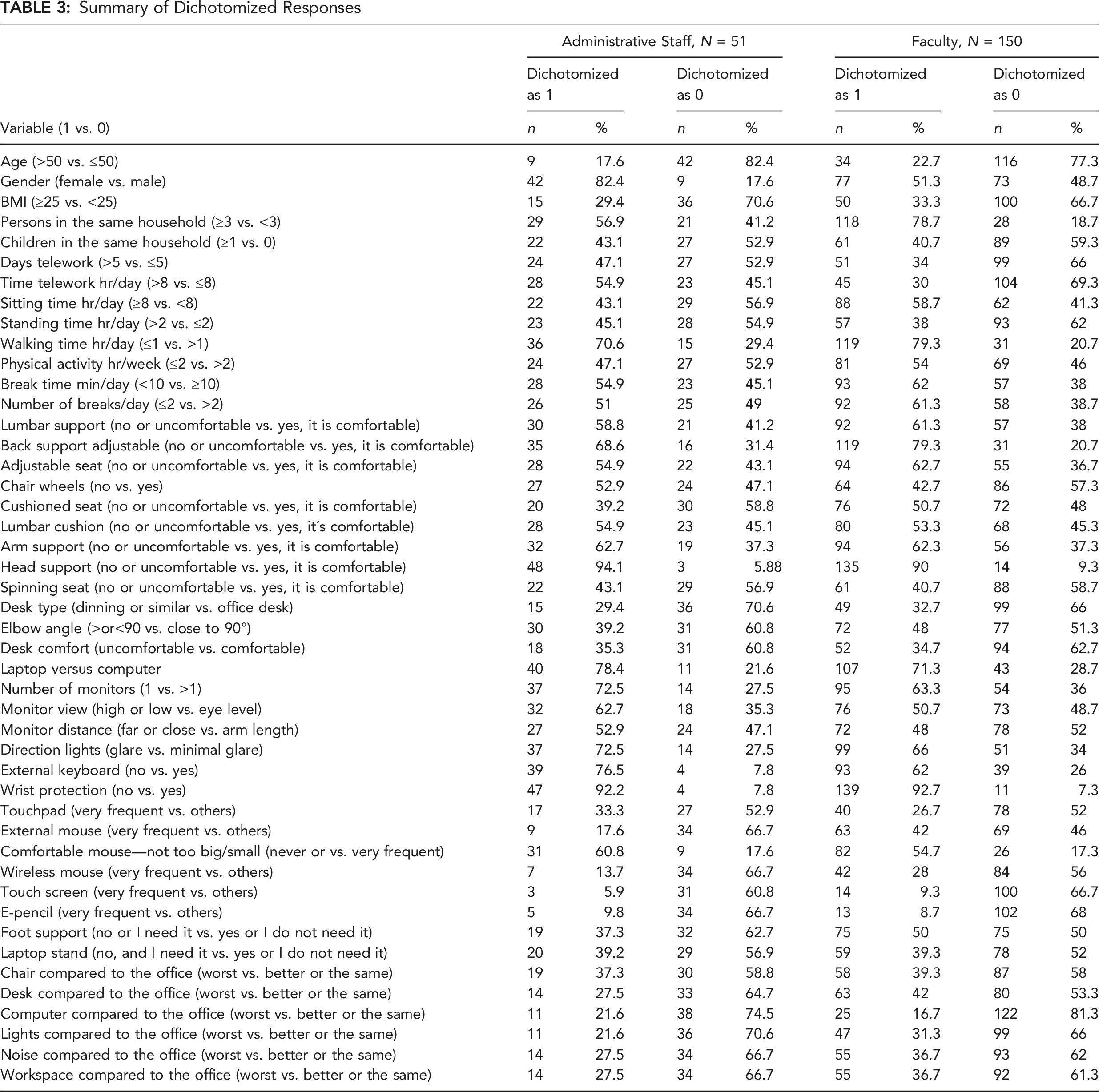
Summary of Dichotomized Responses
Logistic Regression Analysis for Staff
Associations Between Significant Body Regions and Telework Characteristics for Administrative Staff
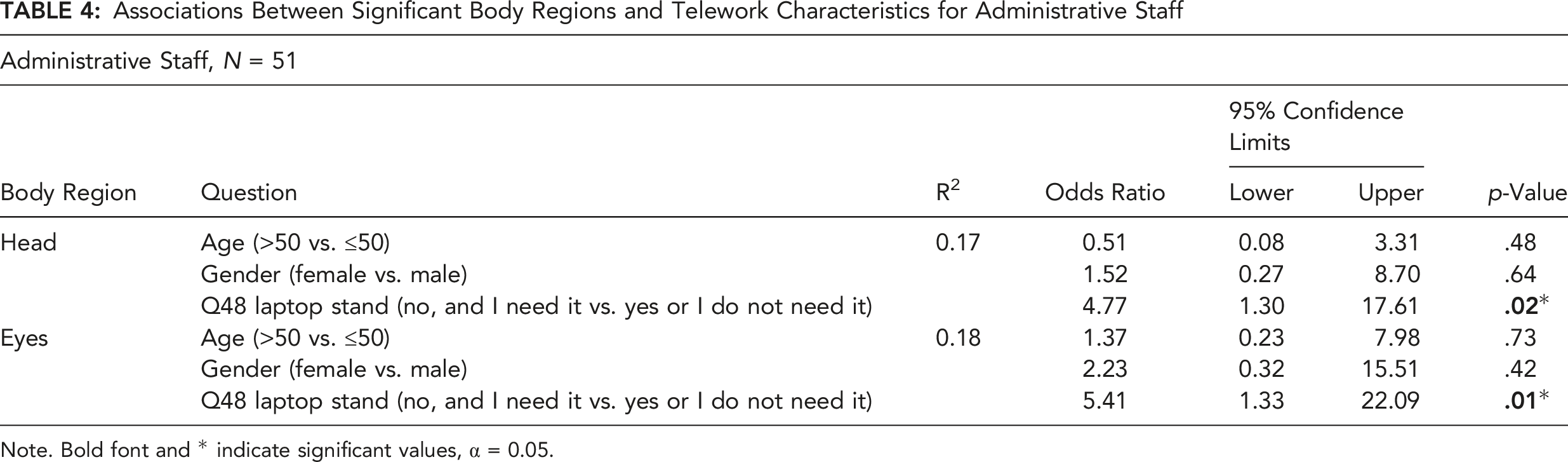
Note. Bold font and * indicate significant values, α = 0.05.
Logistic Regression Analysis for Faculty
Associations Between Significantly Affected Body Regions and Telework Characteristics for Faculty
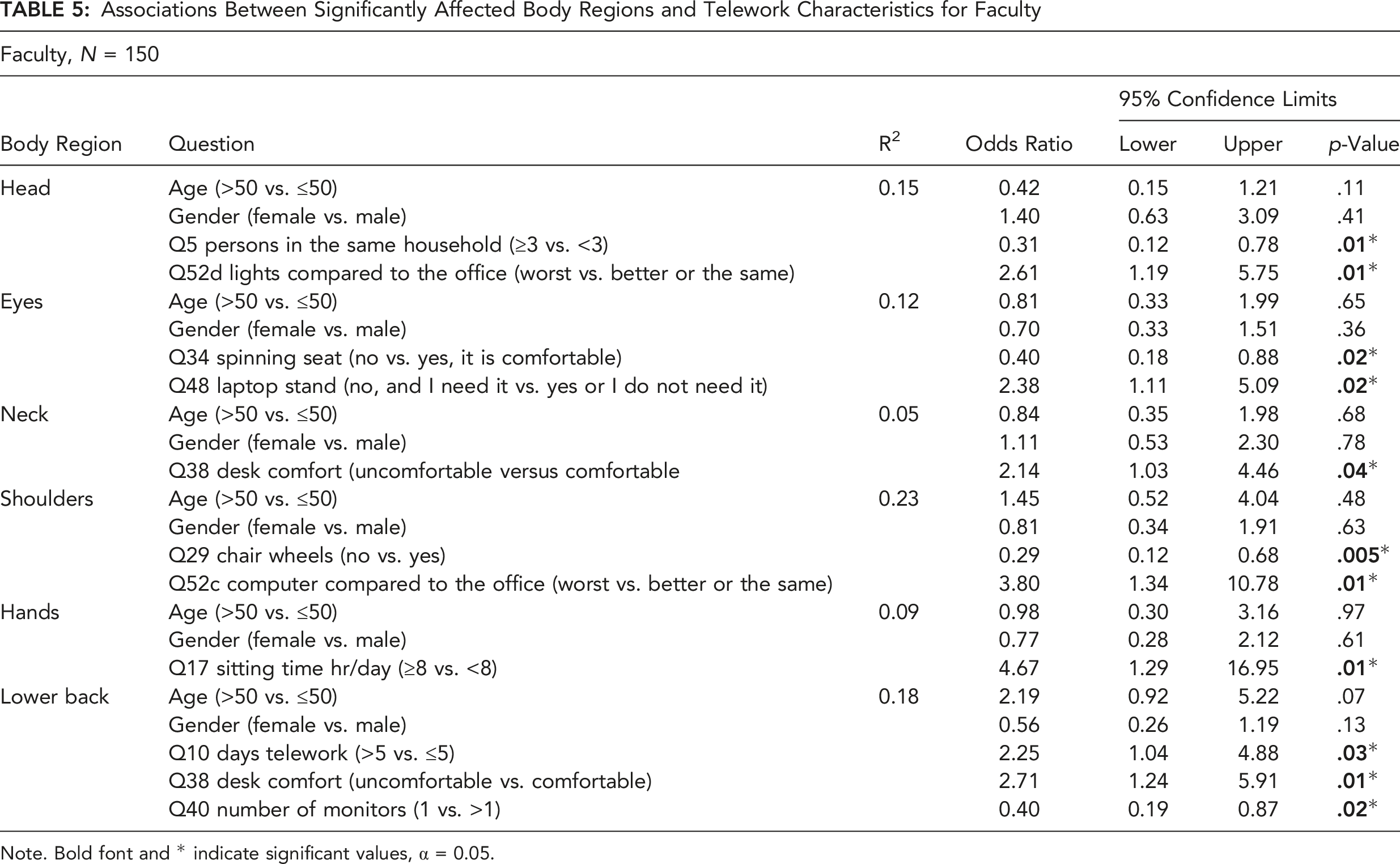
Note. Bold font and * indicate significant values, α = 0.05.
DISCUSSION
By means of a home office characteristics and physical discomfort questionnaire, this study evaluated the associations of telework characteristics during the COVID-19 pandemic with physical discomfort, including musculoskeletal discomfort, of surveyed faculty and staff of a university. Logistic regression analyses identified several home office and job characteristics associated with those body areas that showed a significant increase in self-reported physical discomfort during the pandemic. The strongest effect for administrative staff was eye discomfort associated with not having a laptop stand, while for faculty, it was hand discomfort associated with sitting more than 8 hr/day.
Self-reported Physical Discomfort During the COVID-19 Pandemic
The COVID-19 pandemic social distancing and isolation policies forced billions of people to work from home worldwide. Despite the likely benefit of these polices in controlling further spread of the virus, physical working conditions may have been negatively affected due to increased sedentarism and mostly improvised workstations in home offices. In the present study, during the pandemic, the total severity score was significantly higher for head, eyes, hands, and upper back for staff and head, eyes, neck, shoulders, elbows, hands, upper back, and lower back for faculty members. Similarly, during the pandemic, the total frequency scores were higher for head and eyes of staff and for head, eyes, neck, shoulders, hands, upper back, lower back, and hip of faculty members. These findings are in agreement with recent studies reporting on pain and effects of the COVID-19 pandemic in workers. (Moretti et al. 2020) indicated an increase in pain during telework, with more intensity in body parts such as head, neck, and back as a consequence of pandemic-induced changes. Likewise, another recent study reported that the COVID-19 quarantine resulted in a significant increase in low back pain intensity, prevalence, and most associated risk factors (Šagát et al., 2020). From the physical perspective in our study, several body regions, for which an increase in discomfort was reported during the pandemic, are among the most affected areas reported by office workers. These regions include the neck, shoulders, back, arms, and hands. In addition, eye discomfort was also reported to be higher during the pandemic. This is not surprising as computer work is commonly associated with visual fatigue, which includes symptoms such as burning sensations, redness, blurred vision, diplopia, irritation, and unspecific headaches (Besharati et al., 2020; Celik et al., 2018; Collins & O’Sullivan, 2015; Stark, 1984; Telles et al., 2006). Our analysis attempted to determine the potential risk factors.
Telework Factors Associated With Physical Discomfort
Several working conditions and factors, and workspace characteristics, have been associated with the increase in physical discomfort in office jobs. In general, office and computer work, a typically sedentary activity, can lead to musculoskeletal discomfort and other physical disorders, influenced by individual factors such as age, gender, body mass index, level of physical activity, among others. Moreover, occupational factors such as workload, psychosocial problems, psychological stress, hours worked at a computer, the use of a mouse and keyboard, and postures/force exertions sustained for long periods of time can generate overload within muscular structures (Cabral et al., 2019; Kim et al., 2021; Van Eerd et al., 2016). Furthermore, extensive computer work has been associated with visual and head discomfort (Blehm et al., 2005; Porcar et al., 2016; Stark, 1984). In our study, the highest positive association for the administrative staff was found for head and eye discomfort with not having a laptop stand. This characteristic was also associated with eye discomfort for faculty. According to best practice guidelines for workstation setup, the top of the laptop screen should be at the eye level and one arm length away from the user (OSHA, n.d.; Emerson et al., 2021). Due to the different anthropometric dimensions of each person, it is difficult to adjust the position of the laptop screen on a standard table. Hence, the user tends to flex/extend his/her neck to view the screen. Working with a constant flexion/extension of the neck for a long time can lead to neck related musculoskeletal disorders (Chaffin et al., 2006; Emerson et al., 2021; Norasi et al., 2022). Elevating the laptop display with a laptop stand may help satisfying some best practice for computer workstation setup. This change may also require adding an external keyboard and mouse to the setup when working with a laptop for an extended period of time (Sommerich et al., 2002). In addition, having the monitor positioned poorly relative to lighting or windows can increase glare that can cause eyestrain and headaches (Gowrisankaran & Sheedy, 2015). For faculty, having worse lighting at home than on campus was associated with head discomfort. A review by Blehm et al., (2005) indicated that improper lighting conditions are related to computer vision syndrome which includes symptoms of eye and head discomfort. Consequently, the results suggest the need for improvement in workspace characteristics by means of providing an adjustable laptop stand and improving lighting conditions for teleworkers to prevent or reduce head and eye discomfort.
Although logistic regression found several associations between the area of discomfort and workspace characteristics (see Table 5), the highest positive association for faculty members was found for hand discomfort with sitting for more than 8 hr/day. In this context, associations of musculoskeletal prevalence with particular workspace characteristics are relevant to office workers performing telework. In addition, the present findings also established different levels of musculoskeletal symptom prevalence in particular body regions between faculty and staff teleworkers. These findings are consistent with a previous study reporting on musculoskeletal problems and associated factors among office workers (Besharati et al., 2020). As the description of the physical environment is not detailed enough and largely variable between participants, a factorial analysis is not possible. Nevertheless, the results presented in Table 3 allow formulation of a few propositions to further explain the differences in symptoms between staff and faculty members working at home. These differences are likely to stem from changes in the physical aspect of work, work duration, and workstation characteristics. For example, faculty members almost exclusively teach while standing. This was replaced by seated video streaming/recording of lectures. Such a change is supported by equivalent sitting and standing times reported by both groups. Thus, reduction in alternative postures for faculty members, who are not used to remaining seated for long periods, can explain the significant increase in complaints associated with sitting. This interpretation is supported by localized muscle fatigue studies that show the detrimental effect of prolonged monotonous muscle activities and the benefit of posture alternation (Garcia et al., 2020) or monotony disruption (Kim et al., 2021). Thus, faculty may benefit from incorporating breaks that involve variation of muscle activity (Kim et al., 2021) during telework.
Although faculty members tend to have more monitors and cushioned seats, which are factors influencing body and neck posture (Zuniga & Côté, 2017), these advantages may have been strongly attenuated by the increased sitting time, more days of telework, and uncomfortable desks. The latter was associated with neck and lower back discomfort (Intolo et al., 2019). Moreover, it is important to notice that more than 70% of faculty reported working with a laptop during the pandemic instead of a “desktop” computer. All faculty offices on campus are equipped with “desktop” computers and independent monitors. Intolo et al. (2019) also noted shoulder discomfort when working with a laptop placed on a low-height table. Thus, the present association of shoulder discomfort with having a “worse” computer at home compared to the office may be related to uniquely using a laptop due to forced telework.
Some protective factors were found for head, eyes, shoulders, and lower back for faculty. Not having a rotating seat seems to alleviate visual discomfort, a fixed chair without casters may prevent shoulder discomfort, and working with only one monitor may prevent lower back discomfort. Avoiding movement of the chair or moving to observe a second monitor may favor a stable posture and thus a reduction of muscle activity. However, these associations need to be clarified in future studies, since prolonged static postures are not recommended. Surprisingly, we noted that having more than three persons in the same household could be a protective factor for head discomfort. This needs further examination as Radulović et al., (2021) noted that those who shared the household with others complain of disturbances. Overall, constraints imposed by the confinement may exacerbate the physical stress associated with “work in an office.” Hence, workers should incorporate interventions such as breaks, which may counteract the monotony (sustained postures) of seated work as well as prolonged staring at a video display/computer screen. Breaks may be an easy intervention for telework; however, studies need yet to determine whether duration, frequency, and type of work break can be optimized (Luger et al., 2019). Some workstation adaptation such as lighting conditions may not be too difficult to implement in a home setting. However, other adaptations like having an adjustable office desk may be more challenging, especially when considering the uncertainty of the duration of forced work at home and the cost of adequate equipment.
Study Limitations
The results of the present study must be interpreted in light of several limitations. Due to the self-report method for data gathering, our findings have to be cautiously interpreted. The unpredicted nature of the pandemic did not allow a longitudinal study; thus, participants were required to recall the discomfort perceived when working at their campus offices before the pandemic. This recollection may present some bias. However, participants were asked to recall a behavior and feelings that they were used to for at least two years and compare it to the abrupt and new change required by the pandemic. In addition, the subjective perception of certain variables such as the estimation of physical activity may differ from corresponding objective measures. Although controversies on subjective evaluations and their recall over time are discussed in the literature, retrospective reports of symptoms/discomfort/pain and their severity rating can be integrated over a period and thus be considered “reasonably reliable” (Brauer et al., 2003). In addition, those currently experiencing symptoms are, in significant proportion, more likely to remember (or over report) symptoms (Miranda et al., 2006). The property of recall through a sensory trigger, which shows the associative properties of memory illustrated by the famous “madeleine of Proust” (Righetti, 2021), is implicitly alluded to in Miranda et al., (2006) and supporting their interpretation. Hence, based on the properties of integration and association, it is assumed that retrospective information about pain/discomfort can be “reliable enough” in the context of this investigation, in which recall of symptoms/discomfort is for a prepandemic period only 8 months old with a specific abrupt transition.
The present study did not consider other factors, such as psychosocial, psychological, and organizational, that may have influenced the perception of pain/discomfort experienced by the teleworkers. These nonphysical risk factors are known to play a role in the development of musculoskeletal disorders (e.g., Bongers et al., 1993; Carayon et al., 1999; Graveling et al., 2021), and some factors may be more relevant than others, as reported by Sutarto et al. (2022). However, their analysis and complex relationship with physical factors and subjective outcomes (Graveling et al., 2021; Sutarto et al., 2022), which are mediated by multiple mechanisms (biomechanical, neurological, physiological, and neuroendocrine), was beyond the scope of this study. Such endeavor would have required additional questionnaires and thus reduced the number and quality of responses. Furthermore, to provide a valuable analysis, a differentiation of cohorts of office workers and teleworkers would have been required, which de facto was impossible by context. Finally, it is important to note that some psychosocial factors may have either a positive or negative effect (Graveling, et al., 2021). These factors should be considered in future studies but they would require a holistic approach with a nonnegligible added complexity to investigate the “psychological–physical” relationships. Here we may consider that nonphysical influences are embedded in the results. Finally, since this study was done among administrative staff and faculty members, the results may not be generalizable to other working groups.
CONCLUSIONS
For both faculty and staff that were required to telework, self-reported discomfort of head, eyes, neck, and lower back were present with a prevalence of over 70% during the COVID-19 pandemic. Additionally, the discomfort of these body areas was reported more frequently during the pandemic. Several home office and job characteristics were associated with head and eye discomfort of staff and head, eye, neck shoulder, hand, and lower back discomfort of faculty. The highest positive association for administrative staff was eye discomfort and not having a laptop stand, while the highest positive association for faculty was hand discomfort and sitting for more than 8 hr/day. These findings suggest that improving physical working conditions can mitigate musculoskeletal and other physical discomfort related to home office work. However, adapting home workstations may present a difficult challenge due to cost and space available at home and uncertainty of confinement duration. Work breaks may be an easy intervention to implement to counteract the physical and visual burdens; however, studies are needed to explore the effectiveness of this intervention in telework.
KEY POINTS
More than 70% of staff and faculty that were required to telework during the COVID-19 pandemic reported head, eyes, neck, and lower back discomfort. Both faculty and staff that were required to telework during the COVID-19 pandemic perceived a significant increase in the total discomfort score of most body areas. Head and eye discomfort of staff was associated with not having a laptop stand. For faculty, hand discomfort was associated with siting more than 8 hr/day, while back and neck discomfort was associated with an uncomfortable table.
Footnotes
Acknowledgments
The authors thank Maggie Graf for her collaboration on the final draft and all academic and administrative personnel that participated in this study.
Maria-Gabriela Garcia is an associate professor in the Department of Industrial Engineering at the Universidad San Francisco de Quito. She received her DSc in health sciences and technology in 2017 from ETH Zürich, Switzerland. Email:
Byron Aguiar is a research collaborator in the Department of Industrial Engineering at the Universidad San Francisco de Quito. He received his industrial engineering degree in 2020 from Universidad San Francisco de Quito, Ecuador. Email:
Sofia Bonilla is a research collaborator in the Department of Industrial Engineering at the Universidad San Francisco de Quito. She received her industrial engineering degree in 2020 from Universidad San Francisco de Quito, Ecuador. Email:
Nicolas Yepez is a research collaborator in the Department of Industrial Engineering at the Universidad San Francisco de Quito. He received his industrial engineering degree in 2020 from Universidad San Francisco de Quito, Ecuador. Email:
Paul G. Arauz is an assistant professor in the Department of Mechanical Engineering at the Universidad San Francisco de Quito. He received his PhD in mechanical engineering in 2016 from the State University of New York at Stony Brook and held a 2-year Post-Doctoral Research Fellow position at the Massachusetts General Hospital and Harvard Medical School in 2017. Email:
Bernard Martin is a professor in the Department of Industrial and Operations Engineering at the University of Michigan, USA, and is an affiliate faculty of the Department of Biomedical Engineering. He was awarded a PhD in bioengineering in 1981 and a doctor of science degree in life science in 1989 from the University of Provence, France. Email: