
Abstract
Objective:
We studied the patterns of digits and numbers used when programming infusion pumps with the aim of informing the design of number entry interfaces.
Background:
Number entry systems on medical devices are designed with little thought given to the numbers that will be entered. In other fields, text and number entry interfaces are designed specifically for the task that they will be used for. Doing so allows for faster and more accurate interaction.
Method:
In Study 1, logs were taken from infusion pumps used in a hospital. Information about the numbers being typed was extracted. For Study 2, three common number entry interfaces were evaluated in light of these results to determine which were best suited to the task of programming infusions.
Results:
There are clear patterns in the numbers being used in hospitals. The digit 0 is used far more frequently than any other digit. The numbers 1,000, 100, and 50 are used in nearly half of all infusions. Study 2 demonstrates that interfaces are not optimized for entering such data.
Conclusion:
Changes could be made to the design of the number entry interface on infusion pumps, leading to a reduction in the number of key presses necessary to program a device. We offer a set of four heuristics to guide the design of number entry interfaces on infusion devices.
Application:
Improving the design of the number entry interface of medical devices, such as infusion pumps, would lead to improved efficiency and a reduction in the likelihood of errors.
Introduction
In recent years, there has been a growing focus on interactive systems in health care (see the recent Human Factors and Ergonomics Society “Symposium on Human Factors and Ergonomics in Health Care: Bridging the Gap 2012”). There have been many serious incidents in hospitals resulting from errors committed while using medical devices, many of which have involved number entry (Adam, 2011; Food and Drug Administration, 2009; Institute for Safe Medication Practices Canada, 2007; Vicente, Kada-Bekhaled, Hillel, Cassano, & Orser, 2003). Often the interfaces used on medical products, such as infusion pumps, have generic layouts, which are not designed with any specific task in mind.
Infusion pumps administer drugs to patients and are programmed by users who input data into the pumps regarding the speed and volume of drugs to be delivered. In this article, we present an analysis of the digits and numbers being used when programming infusion devices across multiple wards at a single hospital during a 5-year period. In this article, number refers to the whole number entered, for example, 500, and digit refers to the digits within that number; in the example case, these are 5, 0, and 0. We show that there are patterns in the digits being used and that these patterns are stable across multiple years. We can also see how only a few digits can be used to program most infusions across this 5-year period. We then consider how this information can be used to design and evaluate interfaces that better suit the task of programming infusions and how these designs may help prevent error.
Number Entry Interface Design
When programming infusion pumps, medical workers are asked to program the device by reading numerical values from a separate prescription chart and then programming these values into the device. This procedure is essentially a transcription task in that it involves the perception of input material, the parsing of this material, and outputting it in the form of translation and motor input on a device (Salthouse, 1986). Knowledge about how people perform number transcription tasks is limited; there has not been a large amount of research into this domain at present (Oladimeji, Thimbleby, & Cox, 2011; Thimbleby & Cairns, 2010; Wiseman, Cairns, & Cox, 2011). However, the text transcription domain has benefited from a large amount of research into trying to understand aspects of the text transcription process (Crump & Logan, 2010; McCloskey, Caramazza, & Basili, 1985; Salthouse, 1986). It may be possible to apply results from the text entry domain to the number entry field to understand more about how people transcribe numbers.
Recently, researchers analyzed the types of errors made when transcribing numbers (Wiseman et al., 2011). The number entry error taxonomy produced from this work showed that there is a wide variety of possible number entry errors, more than have been considered previously. These errors included transposition errors, missing characters, and, worrisomely, errors involving entering the decimal point for zero and the zero for decimal point. These types of error often result in entering a number that is far greater or smaller than intended. The consequences of such number entry errors in a medical domain could lead to serious patient harm or death. Interface design that can reduce the possibility of these errors could reduce the amount of unnecessary harm to patients.
Adapting a system such that fewer key presses are required is one way to reduce the chances of error. Such adaptation can be done by using a smart pump system that uses bar code scanning to input numbers. This system is in use in some hospitals and, as such, has been analyzed to determine whether there are indeed benefits to such a system. Unfortunately, the bar code system is prone to its own set of problems. Recent studies into its use in hospitals in the United States has shown that medical workers had to use 31 different types of workaround to use the system when parts of it had degraded, for instance, when bar code labels were defaced or missing or when the technology failed (Koppel, Wetterneck, Telles, & Karsh, 2008). These failings can result in manual overrides, thus undoing any benefit that bar code scanning may have. There are additional issues with the bar code system. To create a bar code representing a patient’s drug administration data, a pharmacist at the beginning of the process must still enter numbers manually. Using a bar code system also abstracts the numbers away from the medical workers; by not having to enter any numbers, it is possible that workers do not check the numbers as thoroughly as they would have. Currently, bar code systems in hospitals appear merely to change when and where errors occur. Until these systems can be made more reliable, alternative methods for reducing necessary key presses should be investigated.
Adapting the interface to fit the specific task is one way of reducing the number of key presses needed to enter the data being transcribed. There are a number of examples of interfaces designed with character frequency in mind outside of the medical domain. One example is the .com button that appears on certain touchscreen phones when the user is typing a URL in the address bar. The .com suffix is the most common of all top-level domains, and designers of these interfaces have clearly incorporated its common use.
Similarly, on many financial calculators, there is a 00 button to make entering round monetary amounts into the system quicker and easier, and shop tills often have buttons for common currency denomination. These shortcuts are based on the frequency of digits and characters that are entered in these particular settings. Context is important when designing these shortcuts: If the .com button appeared every time one wanted to send a text message, it would be considered a waste of screen space as, for that task, the occurrence of the characters in that order would not necessarily be significantly greater than other strings. With knowledge about which digits and numbers are being used in hospitals, it might be possible to adapt the number entry interfaces on infusion devices in similar ways so as to meet the needs of the specific task. This approach has been used in the design of some opticians’ software that is used for entering the prescription of lenses to be ordered (Figure 1). The user is provided with a standard number pad with some added buttons that represent the set of four possible end digits that a prescription may have (.00, .25, .50, and .75).
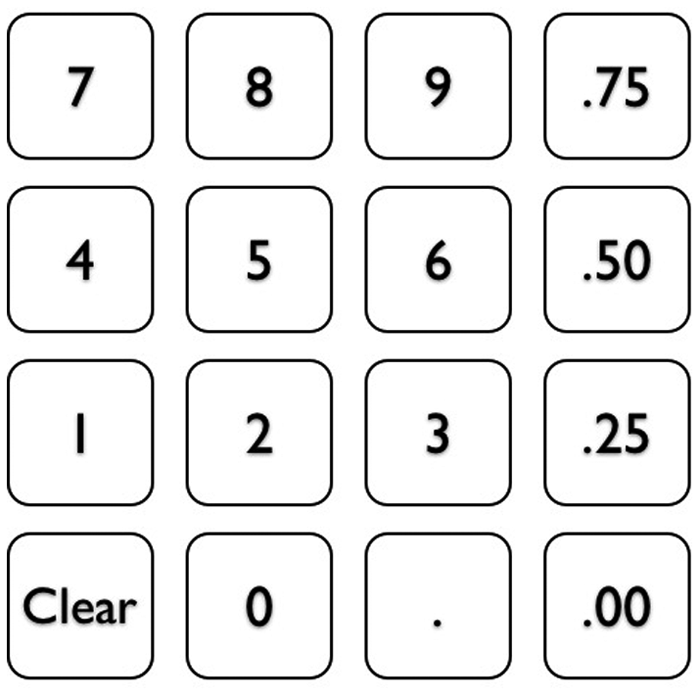
Number entry interface for optician software. The interface is adapted to the task.
In this article, we present two studies in which we investigate the extent to which such design decisions could be sensibly implemented into infusion devices. The first study is an analysis of numbers and digits currently used when programming infusion devices within a hospital. The aim of this work is to ascertain whether the frequencies of digits and numbers used when programming infusion pumps vary greatly. These results are used to inform the second study, in which we evaluate current interfaces and how well they suit the task of programming infusion pumps.
Digit and Number Distributions
To provide information that will guide the design of number entry interfaces on medical devices, such as infusion devices, we need to first be able to answer the question, Which numbers and digits are being used in infusion tasks? Existing research on digit distributions in a number of other contexts suggests that digits do not have an equal likelihood of appearing in a particular place within a number.
One of the most famous examples of digit distribution analysis is Benford’s law, which is noted in many naturally occurring data sets (Benford, 1938). For example, stock market prices (Ley, 1996), fraud detection (Durtschi, Hillison, & Pacini, 2004) and country populations (Sandron, 2002). This law states that in naturally occurring numbers, the probability that the leading significant digit is 1 is close to 30%—greater than the expectation of around 11% if one assumes all digits bar zero have an equal possibility of being the leading digit in a number. This trend continues with 2 being more likely than 3, which is in turn more likely than 4, and so on. We might, therefore, expect to see a Benford distribution in the numbers used when programming infusion pumps. However, this finding would not give a complete understanding, as Benford’s law applies only to the first digit of a number and so therefore does not provide frequency predictions for all digits entered for a number. It is also not clear as to whether the numbers being used in programming infusion pumps constitute a “naturally occurring data set” as is required for a Benford-like distribution to be found.
There has also been some effort to look at the distribution of terminal digit preference in a medical context (Nietert, Wessell, Feifer, & Ornstein, 2006; Wen, Kramer, Hoey, Hanley, & Usher, 1993). In the study by Wen et al. (1993), it was shown that human preference has an effect on which digit a blood pressure reading is likely to end in. It was found that 78% of the time, the reading will end in 0; 5%, it will end in 5; 15%, in an even digit; and 2% of the time, will end in an odd number other than 5. This finding shows the doctors’ natural bias when choosing how to record blood pressure readings and suggests that this bias possibly has a large influence on these findings. However, this research considers only the last digit of numbers and says nothing about the distribution of all digits entered in such tasks.
In addition to the work that has focused on analysis of single digits, there has been research into the frequency of whole numbers. To determine whether experiences with numbers are similar throughout different cultures, researchers have investigated the frequency of number words and numerals occurring in set corpuses from many different languages (Dehaene & Mehler, 1992). This research showed that the patterns for each country were very similar. For numbers 1 through 9 and 10 through 90, there was a decreasing pattern, with 1 and 10 happening most frequently and all numbers occurring less frequently after that. This finding mimics Benford’s law in terms of the decreasing frequency of numbers, but note that this research considers full numbers rather than leading digits. Interestingly, for all numbers from 1 to 1 billion, some numbers appear as spikes in the frequency graph, showing that they occur more often than expected. These numbers are 10, 12, 15, 20, and 100. These numbers clearly adhere to Benford’s law (1 is the most common leading digit, then 2) and also show similar patterns in their terminal digits to the study on terminal digits in blood pressure readings.
But how much can these results tell us about the distributions we might expect to see in the digits and numbers used for programming infusion pumps? Dehaene and Mehler (1992) looked at the numbers occurring in a vast array of sources, including government documents and newspapers, so the numbers collected represent many different things, but still they seem to adhere to a Benford’s law–like distribution, with smaller numbers occurring more frequently than larger numbers. This finding may mean we can expect the same sort of patterns with numbers used for programming infusion pumps. On a digit level, the numbers that were unexpectedly frequent terminated in 0, 5, or 2, similar to studies of terminal digit choice. Again, this finding may suggest that we will see terminal digits in infusion pump programming data sets follow a similar pattern.
However, overall, it is very difficult to determine whether such research might predict the distributions found in our data set. First, two of the reported distributions predict only a single digit within the number. Second, it is difficult to say whether numbers used to program pumps represent “natural” numbers. These numbers may be based on the size of saline bag that is being infused (there will be certain set sizes of bag) and may also be based on standard, predetermined rates and volumes, which will not allow for natural variation in the numbers used. It is, however, critical that we know the numbers that are being used specifically in this medical context if we are to be able to make useful safety recommendations about the design of number entry interfaces on infusion pumps.
Study 1: Digit and Number Distribution Analysis
Data Set
Hospitals do not keep records of dosage information for drugs administered separately from patient information; thus the dosage data are private information. The least intrusive method for collecting data on the numbers being entered into hospital infusion pumps, therefore, was to gather logs from machines currently in use. A total of 154 log files were collected from 104 pumps from 4 different years. All the pumps had a numeric keypad that was used to enter numbers. On average, each log covered a period of 15 days, with the longest log lasting for 173 days and the shortest covering just a single day. The pumps used in this study were located in different wards throughout the hospital, including oncology, surgery, pediatrics, midwifery, and general medical.
The log files contained a large amount of information, recorded at an event level. An event could be anything from starting and stopping the machine to an alarm going off if an infusion finished. At each stage, information about the rate of infusion, the volume of drug to be administered or “volume to be infused” (VTBI), and volume already infused was logged. For this study, the information needed included all digit keys that a medical worker would have had to press to program the pump for a particular infusion. The log reported data to two decimal places as standard. Trailing zeros after the decimal place were therefore ignored, as they did not represent digits that a medical worker would have explicitly entered into the pump. The decimal point was also ignored if it was followed by zeros. The pump being used required the rate and VTBI to be entered to start an infusion. The rate and VTBI were collected from the logs every time a new infusion was started. The rate is entered into the pump as the amount per hour to be infused. For example, a rate of 550 mL/hr would be entered simply as the number 550.
Method
A python script was written to extract these data from the logs. This script could be made to analyze the data on a year-by-year basis, look at each ward separately, or distinguish between numbers used for rate and numbers used for VTBI. The script output the raw data into CSV (comma-separated values) files for inspection in a spreadsheet program. The python script also produced the graphs seen in this article.
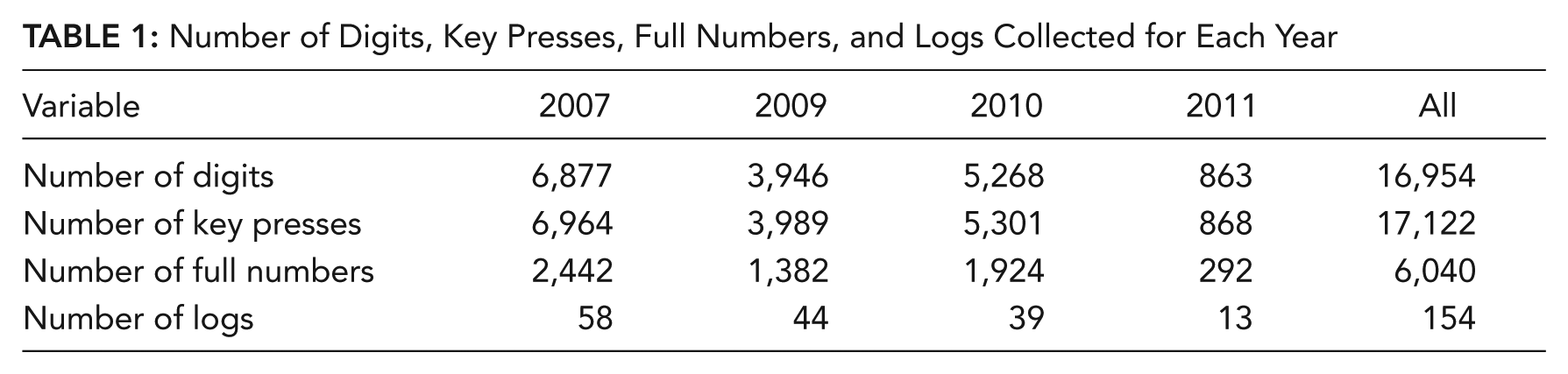
A total of 6,040 numbers were gathered from the logs, 168 of which included decimal places, resulting in 17,122 key presses being collected. In terms of digit distribution, 16,954 digits were collected in total. The spread throughout the years can be seen in Table 1.
Number of Digits, Key Presses, Full Numbers, and Logs Collected for Each Year
Results
The information from the logs was analyzed in a number of ways: by looking at the digit distributions, the whole number distributions, and the length of numbers used. In the following section, we report these data for each year, for each ward, and for both rate and VTBI. Here we describe the results.
Digit distribution in the hospital
The first analysis involved looking at the digit distributions used per year. These digit distributions represented the key presses on the devices. The year-by-year analysis of the digit distributions shows that there is a clear pattern of digits that remains stable across each of the 4 years (see Figure 2). In all cases, 0 is by far the most common digit, accounting for slightly more than 40% of all key presses on these pumps, with the digits 1, 2, and 5 being the next most common digits.
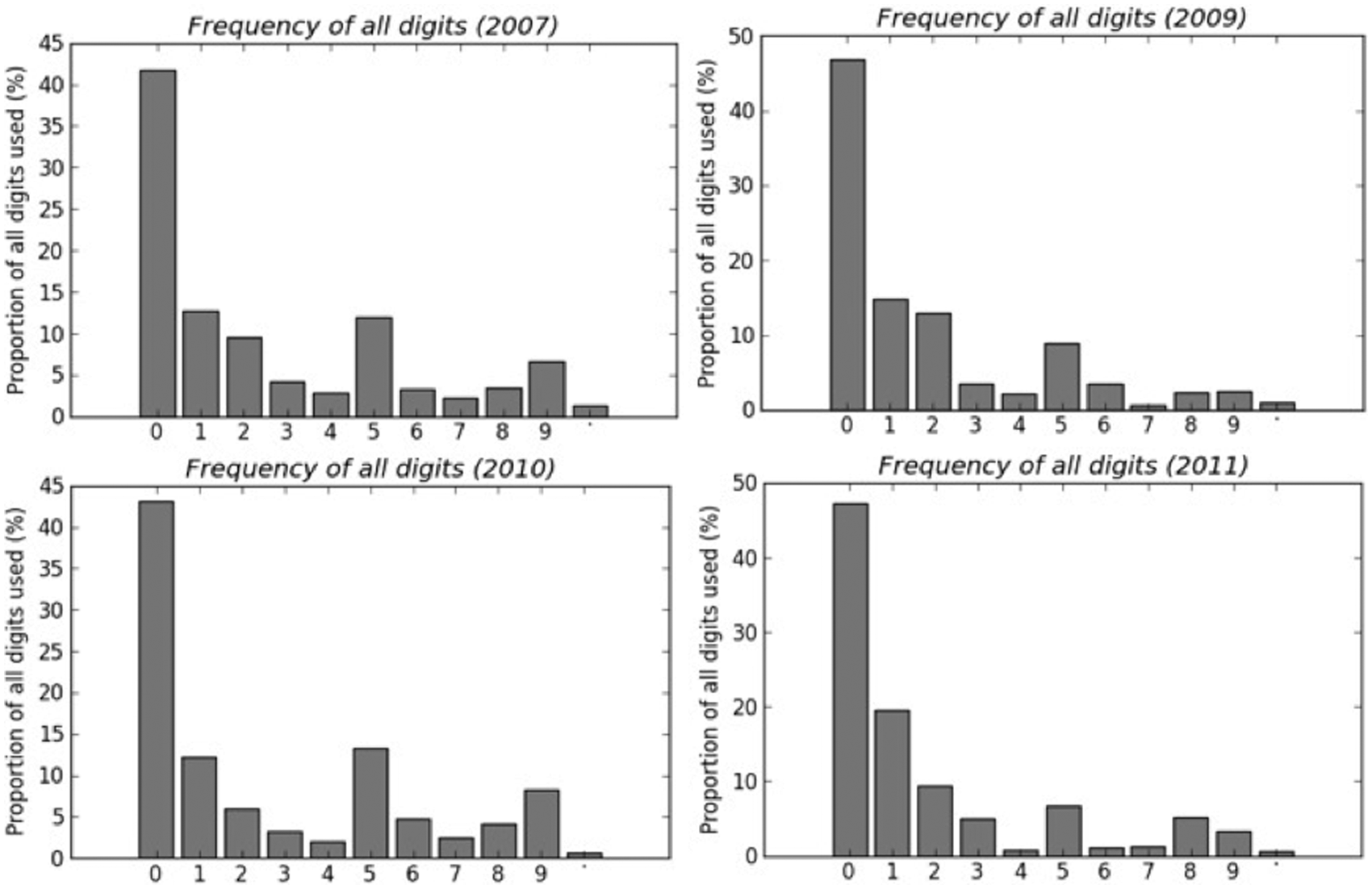
Year-by-year analysis of all digits used to program infusion pumps.
Although Figure 2 shows the distribution of all digits, it is important to consider the distribution of just the leading digit to determine whether Benford’s law is applicable to this data set. The results show that digit 1 is the most frequent leading digit for the numbers gathered in this study, then the digit 2, but the distribution then diverges from a Benford’s law distribution with infrequent 3s and 4s and overly frequent 5s. This finding suggests that the numbers used when programming infusion pumps may not be naturally occurring numbers.
We now turn our attention to analysis of the terminal digit of numbers in the data set. The terminal digit across all years is 0 in approximately 70% of cases, similar to the 78% found by Wen et al. (1993). In both instances, the digit 5 is the next most common digit for a number to end on. However, again, the distribution seen in this study diverges from previously seen patterns: 9 and 3 appear fairly frequently as terminal digits in this study, whereas in Wen et al.’s study, these two numbers are very infrequent.
Digit distribution in the ward
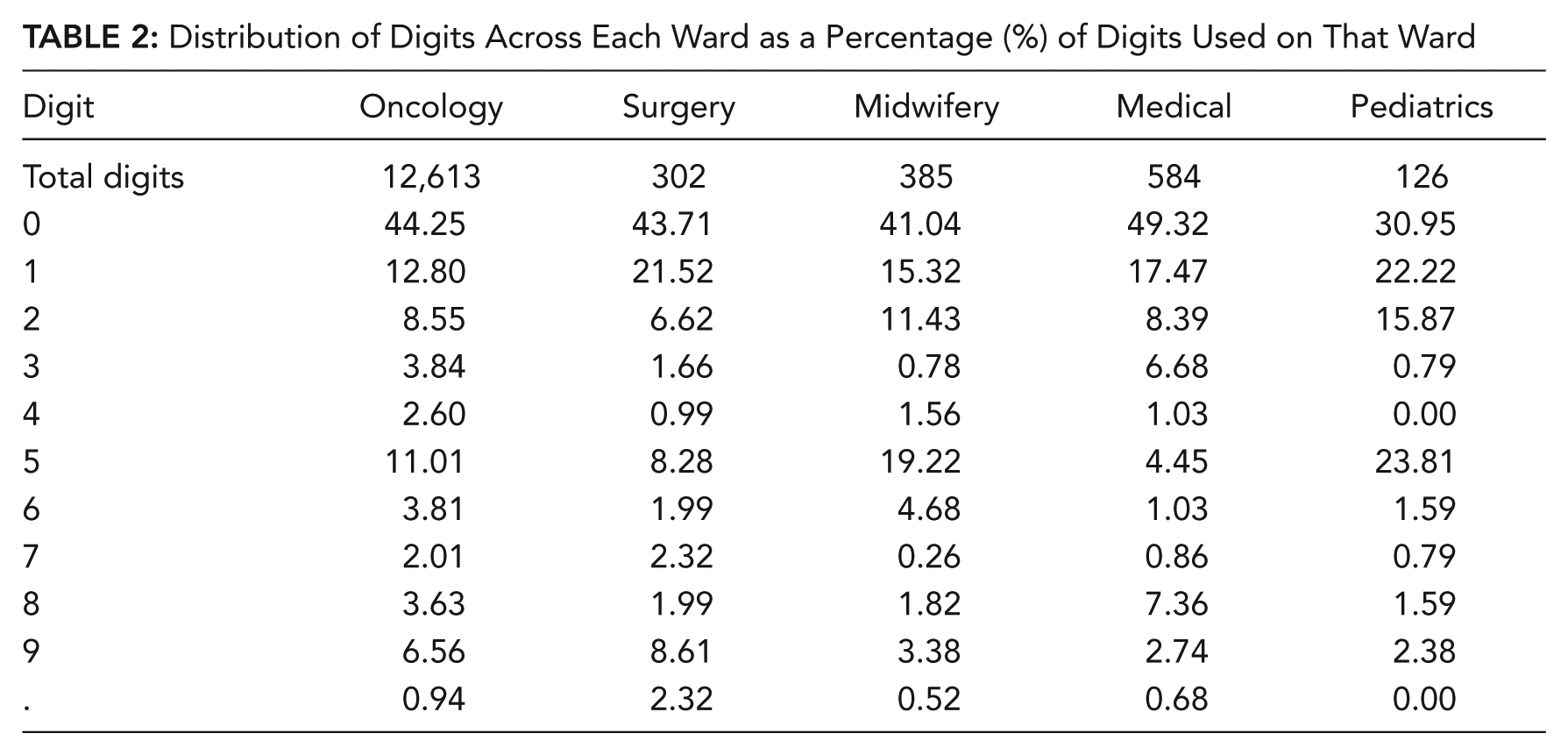
Table 2 shows the distribution of digits across each ward as a percentage of all digits used in that ward. The pattern across the wards is fairly stable but with some exceptions. In the pediatric wards, the prevalence of the digit 0 is less common than in other wards. This finding may be as a result of the length of numbers used in that ward: Smaller numbers have fewer spaces for 0s after the leading digits. (This finding is investigated further in the Number Length section.) Surgery and oncology use a higher number of 9s than other wards.
Distribution of Digits Across Each Ward as a Percentage (%) of Digits Used on That Ward
Digit distribution across rate and VTBI
So far, we have analyzed the digits and key presses for all interactions with the infusion pumps. It is also possible to look at which digits were used for rate and which were used for VTBI. Table 3 shows the number of digits and key presses used for each of the two input values. Although there is an equal number of numbers for rate and VTBI, there were slightly more digits and key presses used for rate than for VTBI.
Number of Digits Used for Rate and VTBI
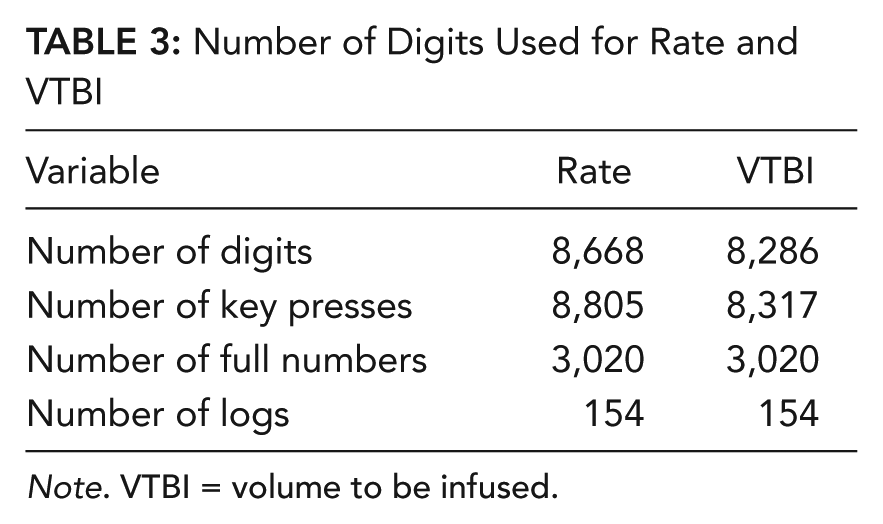
Note. VTBI = volume to be infused.
Figure 3 shows the distribution of digits for rate and VTBI. The overall frequency of digits in rate shows a lot more variability than the digits for VTBI. The majority of digits used in VTBI are 0, 1, and 5, whereas the distribution for digits used for rate is a lot flatter, with each remaining digit being more commonly used for rate than for VTBI. This finding may be attributable to the constraints of bag size, meaning that VTBI has fewer number options, whereas rate can be almost any value. One of the most noticeable instances in which the digit is more likely as rate than as VTBI is for the digit 9. Entering multiple 9s would allow the maximum rate to be set on the pump; therefore, this graph may show that setting the maximum rate of 999 mL/hr is a relatively common task (for instance, when treating local anesthetic toxicity; Holmes, Jefferson, & Ball, 2009), whereas the maximum VTBI is likely to be constrained by the size of the bag of fluid (for example, 1,000 mL).
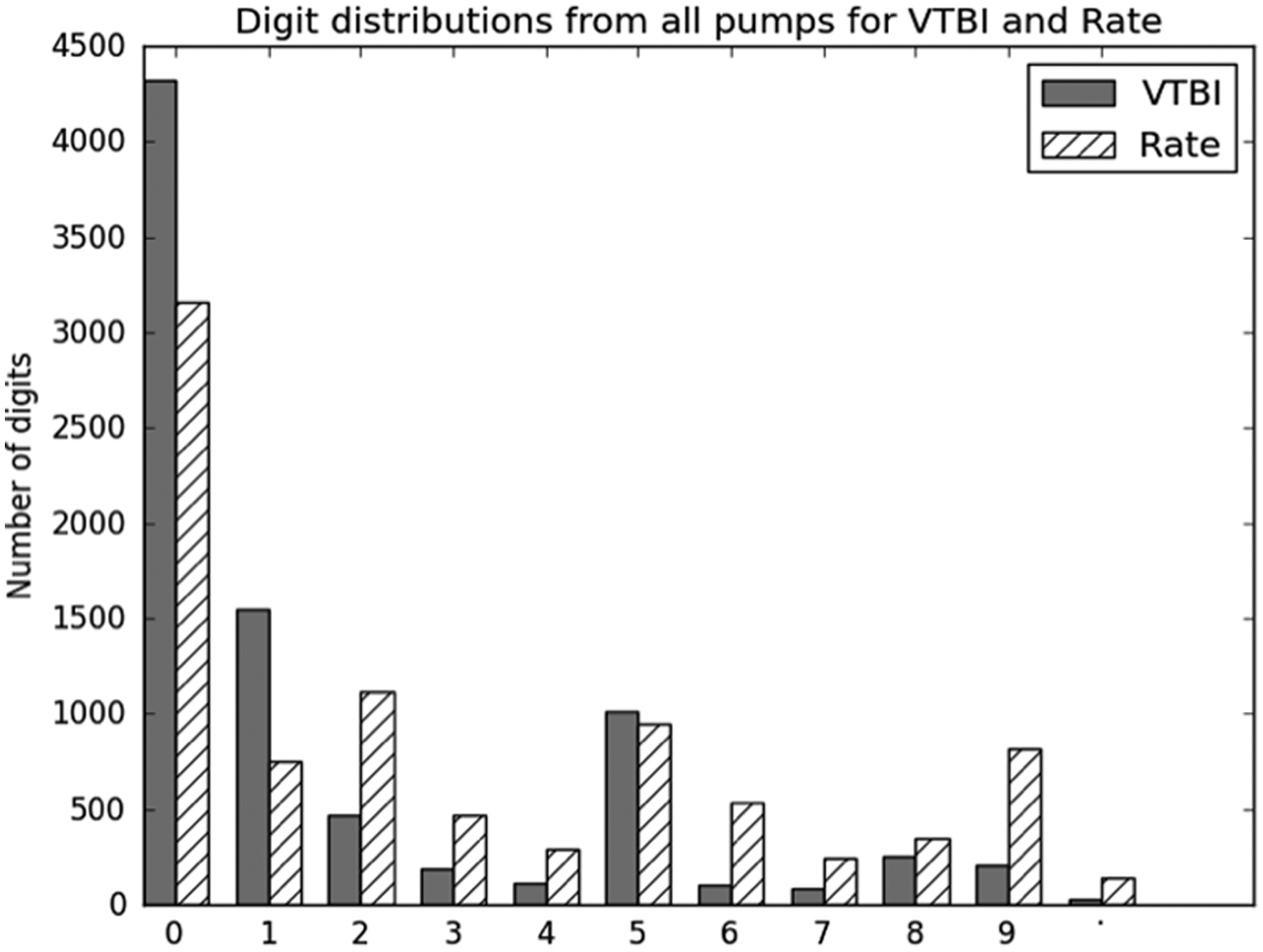
Digit distributions showing the difference between the digits used for programming rate and volume to be injected.
Number distribution in the hospital
In the previous sections, we considered the task of programming an infusion pump in terms of which key presses were required. We will now look at the full numbers that medical workers are dealing with to determine whether there are patterns to these numbers and whether some are more common than others.
Table 4 provides data about the numbers being used for rate and volume across all years and all wards. It can be seen that there is a larger range of numbers used for rate than there is for VTBI (170 numbers used for rate and 153 numbers for VTBI). The values for VTBI vary more greatly than those for rate: The variations in VTBI range between 0.1 and 9,999 mL, whereas rate varies between 1 and 999 mL/hr. This variation may be as a result of the physical limits of the pump in terms of ability to vary rate. It may also be as a result of a preprogrammed minimum and maximum value having been set by a technician.
Variation in Numbers Used Across All Years and All Wards
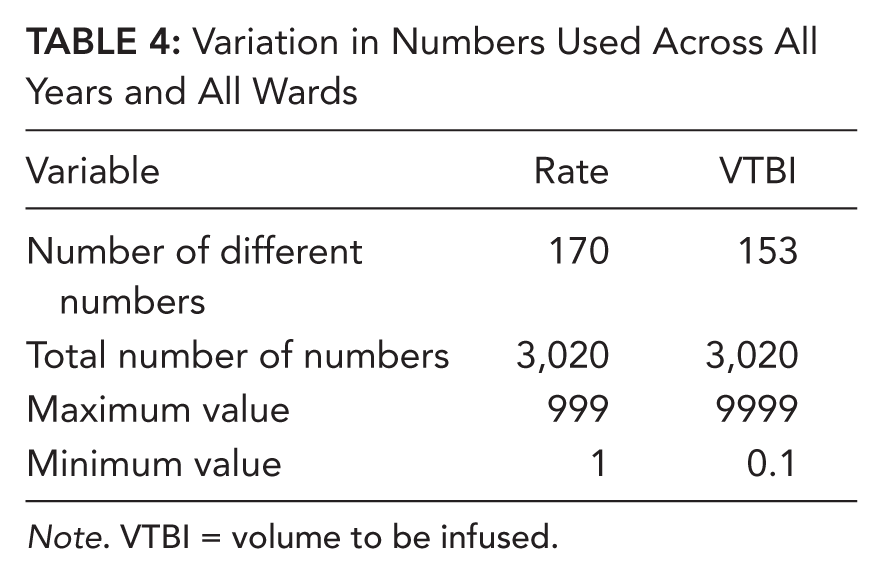
Note. VTBI = volume to be infused.
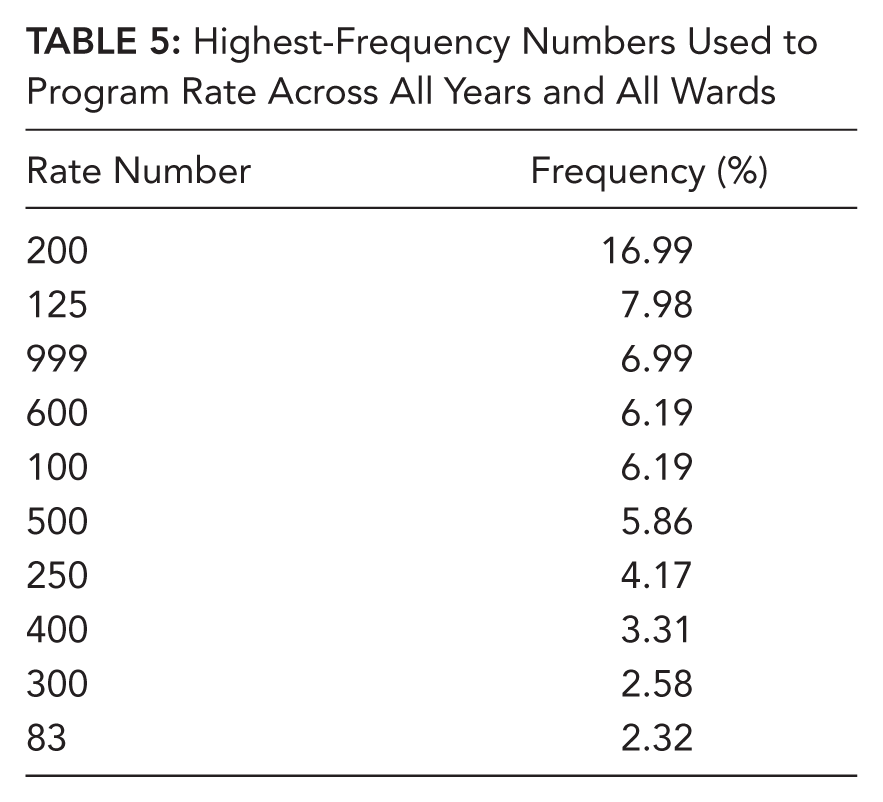
The 10 most common values for rate and VTBI are listed in the Tables 5 and 6. These top 10 numbers represent 64.11% of all numbers used for rate and 72.12% of all numbers used for VTBI.
Highest-Frequency Numbers Used to Program Rate Across All Years and All Wards
Highest-Frequency Numbers Used to Program VTBI Across All Years and Wards
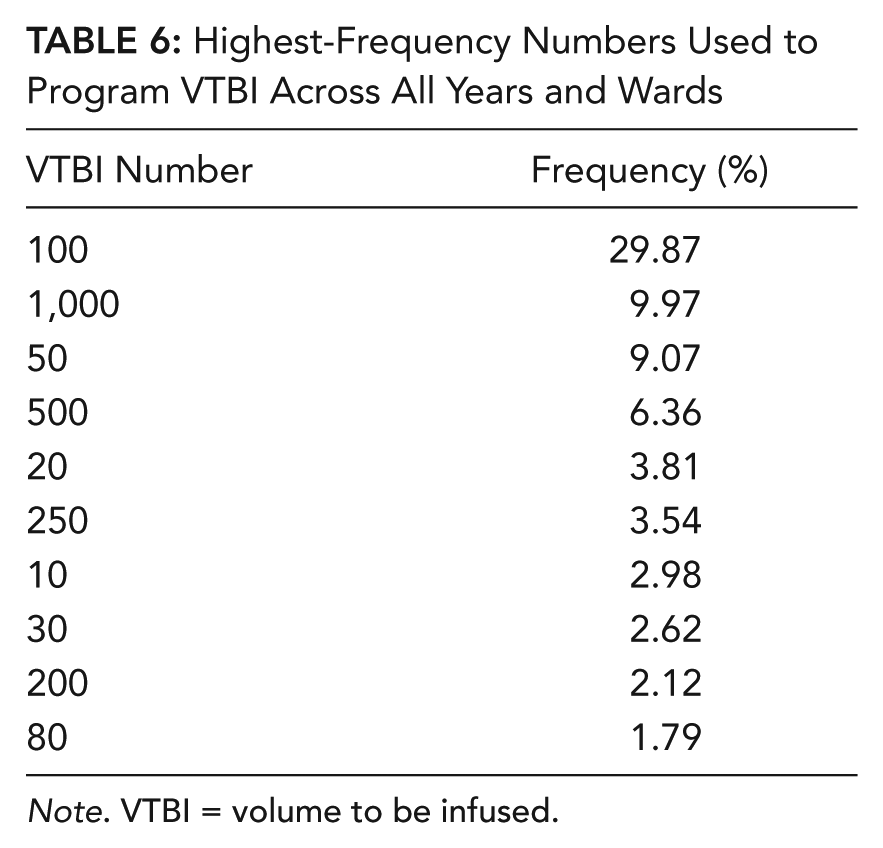
Note. VTBI = volume to be infused.
For both rate and VTBI, the most common values are predominantly round numbers, ending in 0s; in the case of VTBI, every one of the 10 most frequent values being used ends in a 0. The third most common value for rate is 999. This finding supports the previous hypotheses that the large number of 9s seen for programming rate are used at the same time to infuse at the maximum rate possible for the device.
The most common number used for VTBI is 100, which makes up almost a third of all VTBIs programmed into the infusion pumps.
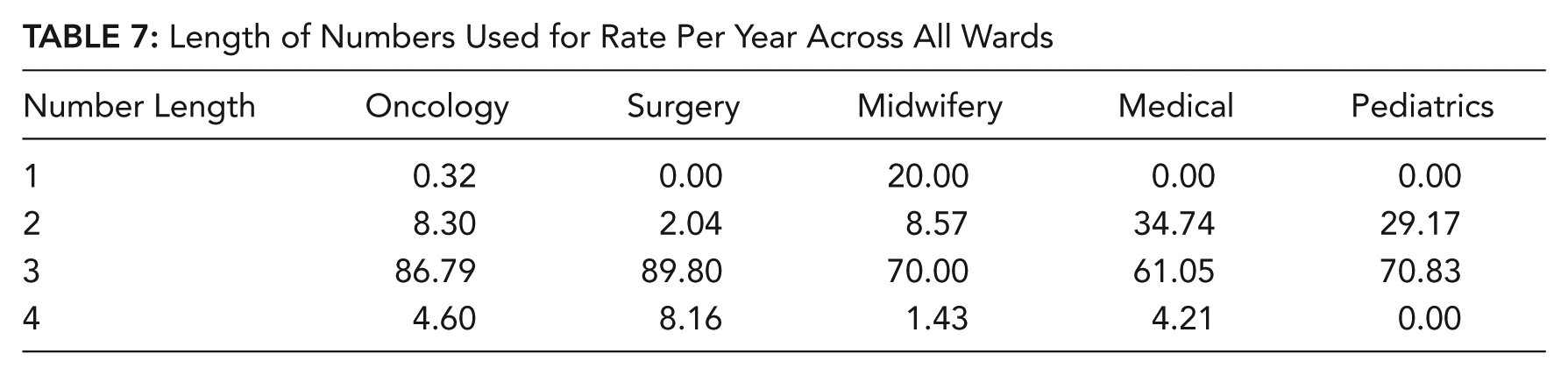
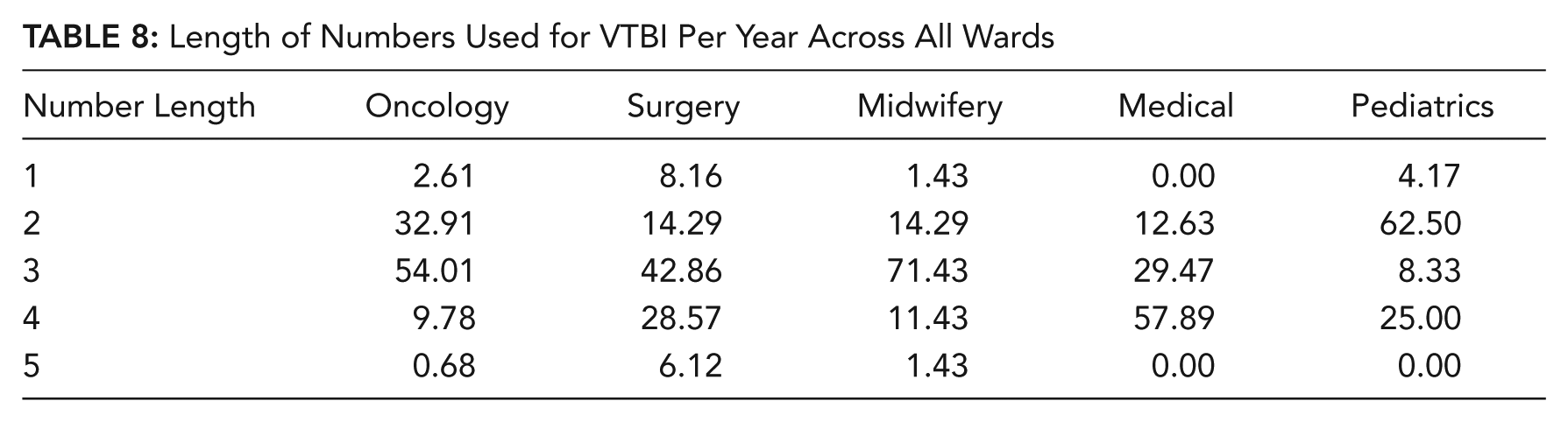
Length of numbers per ward
The length of the numbers (i.e., the number of digits in the numbers) used per ward for both rate and VTBI had some interesting variations, most notably in the pediatric ward, where the numbers were generally far smaller (Tables 7 and 8). This finding is understandable in terms of volume, as doses for children are often smaller; however, it was interesting, too, that the rate was smaller than other wards, as this finding was not anticipated.
Length of Numbers Used for Rate Per Year Across All Wards
Length of Numbers Used for VTBI Per Year Across All Wards
Discussion
Beginning this analysis, we wanted to know whether existing knowledge about digit distribution could be used to predict the digits used when programming infusion pumps. We can see now that the answer is no, digit distributions used to program infusions do not adhere to Benford’s law, nor do they match predictions about terminal digit preference gathered by Wen et al. (1993). This conclusion, first, suggests that these numbers are not taken from a naturally occurring data set but are determined by other things. The VTBIs could be determined by the sizes of bags available to hold the drugs being given to patients. However, rate can vary to any value, yet still we do not see Benford-like distributions, largely caused by the abundance of the number 999.
The observed digit distributions were more than likely the result of human bias in selecting specific numbers for use in the medical domain. When Benford’s law does not apply, it often means that the numbers are not from a natural sample but are created by humans. However, when we compared the infusion pump terminal digits with the study from Wen et al. (1993), we did not see a similar pattern. The terminating-digit pattern is not as well documented and verified as the leading-digit pattern, so we cannot say with the same level of confidence, but it appears as though these numbers were not generated from human biases alone. This data set represents a new and novel digit distribution that has yet been undocumented.
There are, however, noticeable similarities on a whole-number scale between this research and the work of Dehaene and Mehler (1992), who documented the distributions of number words occurring in large text corpuses, particularly, the unexpected “spikes” in frequency for the numbers 10, 20, and 100, which appear in the top 10 numbers used for rate and VTBI. However, the number word analysis does not account for other common numbers used in infusion, such as the most common rate values, 200, 125, and 999. Again, it seems that there is no existing analysis of digit or number distribution that accurately predicts the digits and numbers used in infusion pump programming.
Information about the abundance of the digit 9, and the frequency of the number 999 for the rate, suggests that entering the maximum possible value is very important particularly, it seems, in the surgical and oncology wards. This finding should be considered when designing number entry interfaces for infusion devices. It is important that the user is able to enter in this maximum rate quickly.
The top three most common values for VTBI were used in almost half of all infusions (100, 1,000, and 50). It is therefore important that interfaces allow users to access these values as easily as possible. It might also be possible that shortcuts to these frequent values be considered on interfaces.
The results of this study have two possible applications. First, studies focusing on the testing of infusion pump interfaces can now make use of more realistic data rather than using random numbers, which do not represent the true distribution of numbers being typed (Oladimeji et al., 2011; Wiseman et al., 2011). Second, these results need to be considered in terms of the current interfaces being used on infusion pumps. The following study addresses these issues and makes recommendations for the design of number entry interfaces on infusion pumps that could save time and potentially prevent errors from occurring.
Study 2: Application to Device Design
Infusion pumps currently allow a variety of methods for the entry of numbers. In the previous study, the logs were taken from an infusion pump with a serial number entry keypad, but other infusion pumps use interfaces, such as incremental chevrons or a five-key cursor-controlled input. These three designs are discussed in more detail here.
Number pad interface. This interface comprises 12 keys: 10 keys for the numbers 0 through 9, 1 key for a decimal place, and 1 key for clearing entered numbers from the display (Figure 4). This interface is used to enter the numbers serially, one digit at a time. The interface can be laid out in one of two ways: as a calculator with the numbers 7, 8, and 9 in the top row or as a telephone with the numbers 1, 2, and 3 in the top row. Current guidelines suggest that number keypads on infusion pumps should make use of the telephone layout (National Patient Safety Agency, 2010).
Chevron interface. This interface allows the user to increment or decrement a number displayed on a screen (Figure 5). The double chevrons make larger increments and decrements, for instance, by adding or subtracting a whole number (e.g., from 1.0 to 2.0). The single chevron makes smaller increments and decrements, for instance, by adding or subtracting a decimal point (e.g., from 1.0 to 1.1).
Five-key interface. This interface allows users to move an on-screen cursor in the left-right and up-down directions (Figure 6). The user edits one digit at a time, selecting it by moving the on-screen cursor left or right along the number. At the desired digit, the user presses up or down to change the value of that digit up or down by one integer. This interface can be configured in different ways to allow a wraparound from 9 to 0 if required.
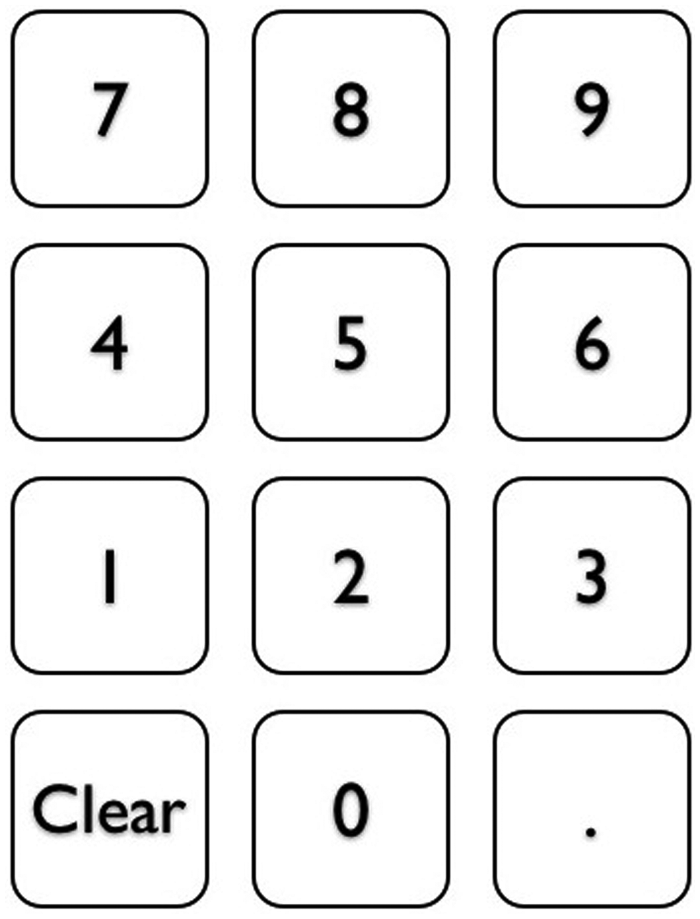
A number pad interface (calculator layout).
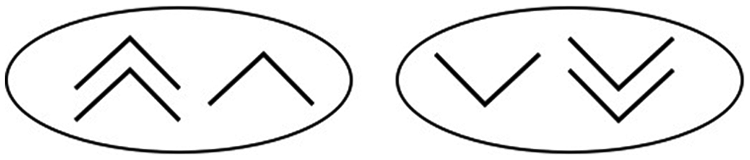
A Chevron interface.
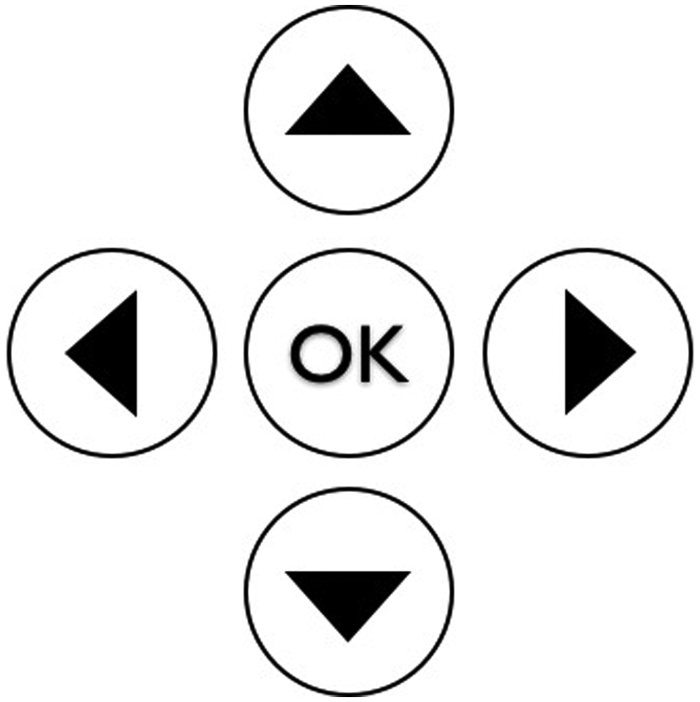
A five-key interface.
Evaluation of Interface Design With Consideration of Digit and Number Distribution
The results of the first study on the distribution of digits and numbers used in the hospitals suggest a set of heuristics that can be used to guide the design of number entry interfaces in infusion devices. These four guidelines are listed next, and each of the three possible current interfaces is evaluated against them.
Number entry heuristics
Heuristic 1: As 0 is the most common digit, entering a string of zeros should involve no more than one key press per digit.
Heuristic 2: Decimal points are used very infrequently, so entering a decimal point should require the user to request that functionality to prevent accidental slips.
Heuristic 3: Entering the value 999 should be possible with, at most, three key presses.
Heuristic 4: The numbers 1,000, 100, and 50 are used in nearly half of all infusions and should have dedicated buttons.
Number pad
Heuristic 1: ✓ The number pad allows for quick entry of multiple zeros. Each zero requires a single key press.
Heuristic 2: ✖ There is a dedicated decimal point button on this interface, meaning that accidental entry of an unwanted decimal point is very possible (especially with poor number pad design; Wiseman et al., 2011). The decimal button should be controlled by asking users to confirm that they wish to use the decimal key.
Heuristic 3: ✓ The number 999 can be easily entered with only three key presses.
Heuristic 4: ✖ There are no dedicated buttons for these common values on this interface. The user must type the whole number each time.
Chevron
Heuristic 1: ✖ It is not possible to enter strings of zeros on this interface with a single key press per zero. The user must cycle through values before getting the number he or she wishes to enter.
Heuristic 2: ✖ There is no dedicated decimal point button on this interface, which means a decimal is less likely to be entered by accident. However, it is still possible if the user pressed the down chevron multiple times. This error can be guarded against by asking users to confirm that they want to enter a decimal place.
Heuristic 3: ✖ Entering the maximum value 999 takes far more than three button presses. This interface requires a maximum-rate button. This interface should require users to confirm that they wish to press this button to guard against accidental use.
Heuristic 4: ✖ There are no dedicated buttons for these values. Shortcut buttons should be provided, or the increments could be tailored so that each time the double chevron button is pressed, the display could show the next most common number, rather than simply adding 10 to what was displayed on screen. This function, however, may not be as predictable to the user, and so the increment values could be made larger to help users navigate to the large, common values more quickly.
Five-key
Heuristic 1: ✓ All digits default to zero so the only button press necessary is to move the cursor left or right, away from that zero. This interface is well designed for multiple zeros.
Heuristic 2: ✖ There is no dedicated decimal point button, so entering a decimal by accident is less likely. However, it is still possible to enter numbers after a decimal place by pressing the right key too often; therefore, users should be prompted to confirm that they wish to enter a decimal.
Heuristic 3: ✖ Entering 999 can take 5 key presses or 29, depending on how this pump is set up. Pressing the down arrow while the cursor is on a 0 can either cause that digit to change to a 9 (if wraparound is enabled) or remain as a 0 (if wraparound is not enabled). Allowing wraparound means the user can type 999 much faster than without. This feature could be implemented without having to make hardware changes. However, this interface may still require a maximum button, as 5 key presses still does not meet the guideline.
Heuristic 4: ✖ There are no dedicated buttons for these values. Shortcut buttons should be provided.
Alternative Interface
Although none of the interfaces evaluated is ideally suited to entering the most common numbers used in infusion tasks, the number pad interface adheres to more of the guidelines than the other two interfaces and is the best suited of this set. However, it is also possible that alternative interfaces may better suit this task. More affordable touch-screen hardware may enable more novel number entry interfaces to be used in the design of infusion devices. Entering numbers on a touch-screen scroll wheel (as is common on many smartphones and tablets) has many benefits (Figure 7). This design would allow the user to control each digit independently by either scrolling on the wheel or tapping on the desired number. The decimal portion of the number would be grayed out and would not be usable until the user tapped and confirmed that he or she wished to select it. The default for the display would have every wheel set to 0. By assessing this design against the heuristics, we can see it performs very well.
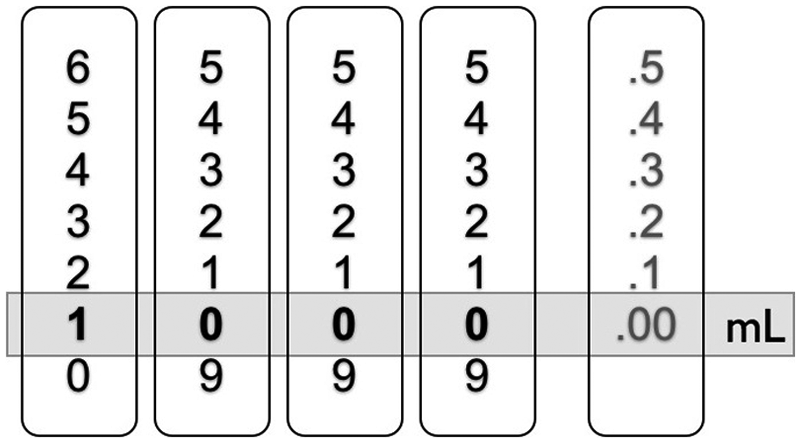
Potential scroll wheel interface for entering numbers on an infusion pump.
Touchpad scroll wheel
Heuristic 1: ✓ All scroll wheels default to zero, meaning no interaction is needed to enter multiple zeros.
Heuristic 2: ✓ Entering a decimal point requires that the user interacts specifically with the decimal wheel. The user would have to confirm this intention before the wheel turned, making it harder to enter a decimal by accident.
Heuristic 3: ✓ Entering 999 takes three presses; the 9s are on screen so simply need to be tapped by the user.
Heuristic 4: ✓ The most common VTBI numbers can be entered by tapping one section on the desired wheel. For instance, 1,000 is entered by tapping the 1 on the first wheel, 500 by tapping the 5 on the second wheel, and 50 by tapping the 5 on the third wheel.
By adhering to the heuristics, this interface requires fewer presses than the previously analyzed interfaces, thus reducing the potential for error.
Conclusion
The design of number entry interfaces on infusion pumps is not optimized for the tasks that they are being used for. By taking recommendations from the results of Study 1, we can create a series of heuristics that would allow number entry with fewer key presses and would thus reduce the chance for error. The guidelines do not only have to be used as an analytic tool but can also be used as the basis of design. Here we have shown how a touch-screen scroll wheel interface may be designed to meet the needs of the infusion programming task. Designs, such as the touch-screen scroll wheel presented here, need to be tested in laboratory environments before a recommendation can be made for real-world usage. However, this study has shown how results from Study 1 can be used to generate possible improvements in number entry interface design on infusion pumps.
General Discussion and Conclusions
The research reported here has important implications for the design of number entry interfaces in general and, in particular, for those used on infusion pumps in medical settings. It also provides clear evidence that particular distributions of numbers and digits are used in different settings. We now discuss each of these issues in turn.
The Design of Number Entry Interfaces
The consequences of this research for the design of number entry systems can be distilled into a single guideline to be considered when choosing the type of number entry interface to be selected. Designers of such devices should give consideration to the context of use, and in particular, to the distribution of numbers and digits that are most frequent within that context.
Our research demonstrates that in this particular context, leading digits do not follow Benford’s law (Benford, 1938), terminal digits do not follow the pattern indicated by Wen et al. (1993), and the numbers do not wholly follow the pattern found by Dehaene and Mehler (1992). It is therefore important to understand the distribution of both digits and numbers used in a particular context, rather than relying on prior knowledge about other number distributions, before attempting to design a number entry interface.
The Design of Number Entry Interfaces for Infusion Devices
We suggest four clear guidelines for design that should be considered by designers of number entry interfaces on infusion devices. These are as follows:
Zeros should involve no more than one key press per zero.
Entering a decimal point should require the user to request that functionality to prevent accidental slips.
Entering the value 999 should be possible with at most three key presses.
The numbers 1,000, 100, and 50 should have dedicated buttons.
We have demonstrated that these guidelines can be used for evaluating existing designs in considering the extent to which they support the entry of the most frequently occurring digits and numbers. They can also be used to support the design of future number entry interfaces for this range of devices. Making theoretical changes to the interfaces according to the heuristics has shown the reduction in key presses possible.
Application of these guidelines to number pad entry systems would result in the addition of shortcut buttons for the most frequently used VTBIs. Three buttons could be used to allow nearly 50% of VTBIs to be entered, which would greatly reduce the number of key presses and opportunities for error.
Application of the guidelines to chevron entry systems would result in the design of different levels of increment that cycle through the most commonly used numbers, not just incrementing by 10. Alternatively, the increments could better reflect the numbers that are likely to be navigated to, perhaps making the increments 50 each time rather than 10.
Applying the guidelines to the design of five-key entry systems would allow wraparound for the common rate value of 999 to be entered as quickly as possible. This rate value means that the drugs need to be administered as fast as possible, and speeding up the process of entering those numbers would help greatly.
In summary, current designs of number entry interfaces used on infusion pumps do not take into account the digits and numbers being programmed in daily use. We propose four guidelines that can be used to support the design of such interfaces in this context. In the future, researchers should empirically test existing and future interfaces for their suitability for the task to ensure safer and more efficient devices for patients and medical workers.
Key Points
Numbers used to program infusion pumps cannot be predicted by existing research on digit and number distributions.
The numbers used to program infusion pumps are stable and consistent across many years.
This article presents four heuristics based on digit and number distribution analysis that should be followed to reduce the key presses needed when programming infusion pumps. These guidelines reduce the number of chances for error.
Current infusion pump interfaces are not optimized for entering the numbers that are most regularly used when programming infusions.
Footnotes
Acknowledgements
The authors would like to thank the reviewers for their useful comments, which have helped strengthen the article. This work has been supported by the Division of Psychology and Language Sciences, University College London, and the Engineering and Physical Sciences Research Council Grant EP/G059063/1 for CHI+MED.
Sarah Wiseman is a PhD student at University College London (UCL) Interaction Centre. She received her master’s degree in human-centered interaction from University of York, United Kingdom, in 2010.
Anna L. Cox is a senior lecturer at UCL Interaction Centre. She received her PhD in cognitive science from University of Hertfordshire, United Kingdom, in 2002.
Duncan P. Brumby is a senior lecturer at UCL Interaction Centre. He received his PhD in cognitive science from Cardiff University, United Kingdom, in 2005.