
Abstract
Introduction
In Australian hospitals, medication errors are frequent and may result in adverse events.1,2 Errors are defined as failures in the medication treatment process and occur in all hospital areas at any point from prescription to administration.1,3 They are reportedly detected in up to 1 in 10 medication administration events.2,4 Common error types include omission, overdose, wrong medicine, underdose, incorrect route, and incorrect frequency.5,6 Morbidity and mortality arising from medication errors can be significant,1,2,5,7 and reportedly costs approximately AUD$660 million per year in Australia.5,7
Most interventions to reduce in-hospital medication prescription errors have involved either expansion of the clinical pharmacist role,8-14 or the introduction of technological aids.13,15-18 Emergency department (ED) based research has largely focused on prescription and administration of drugs being used for the initial management of acute conditions.19-21 However, with the introduction of ED Short Stay Units (SSUs) over the past 15 years, the need to correctly deliver patients’ regular medications has become more important. Patients cared for in SSUs remain in the ED for longer, are older, have more co-morbidities, and are more likely to take multiple regular medications than the general hospital population. 22 All these factors are known to be associated with increased medication errors.1,2,22,23 Limited ED-based research reports higher medication error rates in the ED SSU than in the acute ED. 21
In response to repeated reports of regular medication omissions in the Dandenong Hospital ED SSU, a multi-disciplinary response team (The Regular Medications in ED SSU team, a.k.a the ReMedIES team) was formed. Included were 1 junior and 2 senior ED doctors, one senior ED nurse and 2 ED-based clinical pharmacists. Their task was to introduce ED process changes to reduce non-prescription of SSU patients’ regular medications, but with no additional financing or resources. This observational study evaluates the effectiveness of the implemented multifaceted intervention.
Methods
Study Design, Setting and Period
A pre- and post-intervention observational study was conducted at Dandenong Hospital, Monash Health, Melbourne, Australia. The 37-bed acute ED (2021 annual census of 68 950 patients) is supported by an adjacently located 20-bed SSU (2296 admissions in 2021). The pre- and post-intervention periods comprised 10 selected days between 1 January and 11 February 2021, and between 27 December 2021 and 12 January 2022 respectively. Study conduct was approved as a quality improvement project by the Monash Health Human Research Ethics Committee (RES-21-0000-720Q-79444). The study complied with the STROBE guidelines for observational studies. 24
Study Outcomes
The primary outcome was a between-period comparison of the percentage of eligible patients with non-prescription of one or more clinically significant medications (CSM) which they regularly took at the defined medication administration times of 08:00 or 20:00. Secondary outcomes included between-period comparisons of the total number and types of non-prescribed regular CSMs and non-CSMs. Related adverse events were noted.
Study Population
Eligible patients were all those in the ED SSU on the selected study days (see shift selection section), who usually took medications at the hospital’s scheduled regular medication round times of 08:00 or 20:00. Stratified selection of patients between study periods for variables such as age, sex, and comorbid conditions was not considered relevant, as the primary concern was the receipt or not of a regular medication. For this purpose, for example, an elderly woman on antihypertensive medications and a young man on anticoagulants for recurrent thromboembolism were considered equivalent.
The Hospital Electronic Prescribing System and Choice of the 08:00 and 20:00 Administration Times
At Monash Health medications are prescribed electronically, via the hospital electronic medical record system (EMR, Cerner Corporation, North Kansas City, Missouri, USA). This contains a medication database with common dosing regimens available for selection. The medication lists of previously admitted patients are stored in the system, enabling immediate re-prescription of unchanged medications. Any administration time may be entered, but the defaults for “morning” and “night” are 08:00 and 20:00. Almost all 2-, 3-, 4- or 5-times daily medication regimens include one or both default times. For this reason, it was felt that the additional effort of screening for omission of the small number of medications taken in isolation at other times was not warranted.
Following prescription on EMR, the names of all medications, expected administration times and the prescriber’s identity are recorded and readily located in the Orders section of EMR. The same details also appear in the Medication Administration Record section of EMR, where the time of medication delivery is recorded by the administering clinician.
Study Definitions
Regular medications were classified as either a CSM or a non-CSM. A CSM was defined as a medication with the potential, if omitted, to have an acute (within 24 hours) clinical or physiological effect, which could require acute correctional management. A literature search did not yield any medication lists which met this definition for stable patients having a <24-hour admission to an ED SSU. In general, hospital-based medication error literature focused on medications which could lead to serious morbidity or mortality.7,23 The most widely known classification is the “APINCH” medications (Anti-infectives, Potassium & other electrolytes, Insulins, Narcotics & other sedatives, Chemotherapeutic agents, and Heparin & anticoagulants). 25 While prescribing omission of these medications for SSU patients is clearly important, this list was not felt broad enough for our purposes. Consequently, a modified Delphi method 26 was used to construct a final list of CSMs. A steering group (ML, RM, ABJ) developed an initial list which was circulated to the full author group on 2 occasions, following which consensus was reached. The final list of CSMs and examples of the most common non-CSMS is shown in Table 1. Adverse event occurrence from prescription omission was not required. For example, non-prescription of antihypertensive or hypoglycemic medications might lead to detection of high blood pressure or blood sugar levels requiring remedial action despite being asymptomatic. Non-prescription of some long-term analgesic or anticonvulsant medications may or may not precipitate treatment-requiring withdrawal symptoms or seizure activity. Omission of a combination CSM was recorded as a single non-prescription in 1 clinical category.
Medications Requiring Prescribing in ED SSU: Category, Family, Common Examples, and Exclusions.
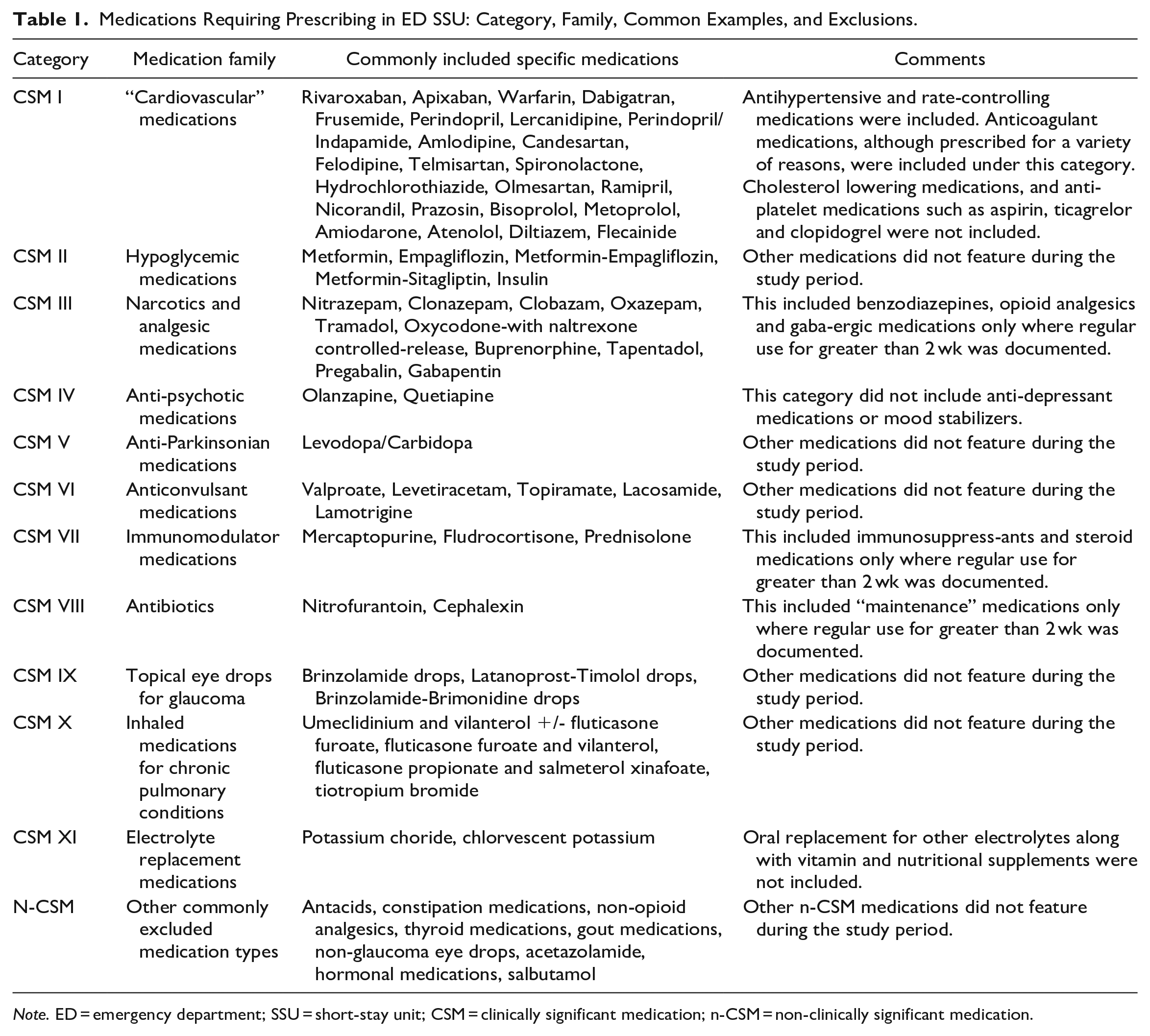
Note. ED = emergency department; SSU = short-stay unit; CSM = clinically significant medication; n-CSM = non-clinically significant medication.
ED Medical Rostering and Study Shift Selection
From 07:30 to 24:00, the SSU is covered by an intern who is based within the SSU, working under the remote supervision of an emergency physician based in the acute ED. From 23:00 to 08:00, the SSU is covered by a resident medical officer (RMO, post-graduate year 2-4) who is based within the SSU, working under the remote supervision of an emergency medicine registrar. The ED is staffed at any one time by about 20 emergency physicians, 14 emergency medicine registrars, 5 RMOs and 9 interns. Doctors, other than the permanent emergency physicians, work in the ED for 12-week rotations. Each shift is staffed by a balance of senior and junior doctors in each of the acute ED, Fast Track and the SSU. Individual doctors are usually rostered on the same shift (day, evening or overnight) in the same clinical area for 3 to 7 consecutive days.
Given this rostering pattern and the number of study days required (see sample size section), selection of consecutive days would have limited the number of different doctors present on the included days. Consequently, the detected prescribing practices may have been systematically influenced by over- or under-representation of those with more rigorous prescribing habits. To maximize representativeness, the first 10 days from 1 January 2021 (pre-intervention period) and 27 December 2022 (post-intervention period) on which different medical staff were present in the different ED areas (acute ED, Fast Track, SSU) were selected as the study days. These conditions were met by 11 February 2021 and 12 January 2022 respectively for each study period. This also ensured that each period fell within a single 12-week junior medical staff rotation.
Pre-Intervention Prescribing
Prior to SSU admission, the initial treating acute ED doctor is responsible for prescribing all medications, including regular home medications. The initial admitting acute ED nurse is expected to note patients’ regular home medications. The nurse may alert the attending doctor to a prescribing omission but has no formal responsibility in checking medication prescription. Patients remaining in the SSU at shift completion time are handed over to the junior SSU doctor who continues or completes the management plan. SSU nurses or the junior SSU doctor might detect and rectify a regular medication omission but are not expected to double-check prescription completeness. The ED pharmacist (07:30 to 16:30) performs medication reconciliation for acute ED patients awaiting an inpatient bed, sources required non-stocked medications and dispenses discharge medications. The ED pharmacist has no role in SSU admission medication reconciliation.
The Intervention and Post-Intervention Prescribing
The ReMedIES team developed a 4-part intervention. (1) The initially treating acute ED doctor’s prescribing responsibility, and the value of the initially treating nurse monitoring this, was repeatedly reinforced at doctor and nurse communication huddles. (2) Prescribing questions were included in the formal SSU handover checklist. The junior SSU doctor was to ask: “Are the patient’s regular medications prescribed?” and “If not, who is doing this?” (3) An overnight meeting (approximately 02:00) between the SSU nurse team leader and the junior SSU doctor was instituted at which presence of regular medication prescription was to be checked for all patients. (4) At 07:30 the overnight junior SSU doctor and/or the SSU nurse team leader, delivered a list of patients still needing medication reconciliation to the ED pharmacist for completion by 08:00. This was an additional duty for the ED pharmacist. A 2-week period of education preceded introduction of the intervention in November 2021. No additional staff or resources were made available.
Study Procedure
Lists of patients present in the SSU at either 08:00 or 20:00 on the selected days were generated from the EMR. All records were screened by ML. Those on documented regular home medications were retained for analysis. Presence or not of a prescription for the regular medication at 08:00 or 20:00 was then checked in the Orders section of the EMR and its administration cross-checked in the Medication Administration Record section. Prescription omission, including medication name and type were recorded by ML and ABJ into Microsoft Excel™ worksheets (Microsoft Corporation, Redmond, Washington, USA). Occurrence of adverse events was checked for in EMR notes and in the hospital-wide Riskman incident reporting system (Riskman International, Southbank, Victoria, Australia).
Statistical Analysis and Sample Size
Variables are presented as median with interquartile range (IQR) or number and percentage. Between-period comparison of prescribing omissions used the chi square test. Analyses were performed by RM and ABJ using Stata statistical software (Version 17, StataCorp, College Station, Texas, USA). A limited local audit suggested 40% of SSU patients might have regular medication prescribing omissions. The ReMedIES team considered that initially halving the omission rate to 20% would be worthwhile. If this was achieved, a sample of 110 patients per group was required to demonstrate statistical significance (α = .05, β = .90).
Results
On the 10 pre- and post-intervention study days, 110 and 106 eligible patients were identified. Baseline patient characteristics were generally similar. Median patient age pre- and post-intervention was 72 (IQR: 58-84) and 70 (IQR: 55-77) years respectively (difference 2 years [95% CI: −10 to 4]). Of the total, female patients comprised 62% (95% CI: 52-71) and 56% (95% CI: 46-65) respectively (difference 6% [95% CI: −7 to 19]). Patient flow is detailed in Figure 1.
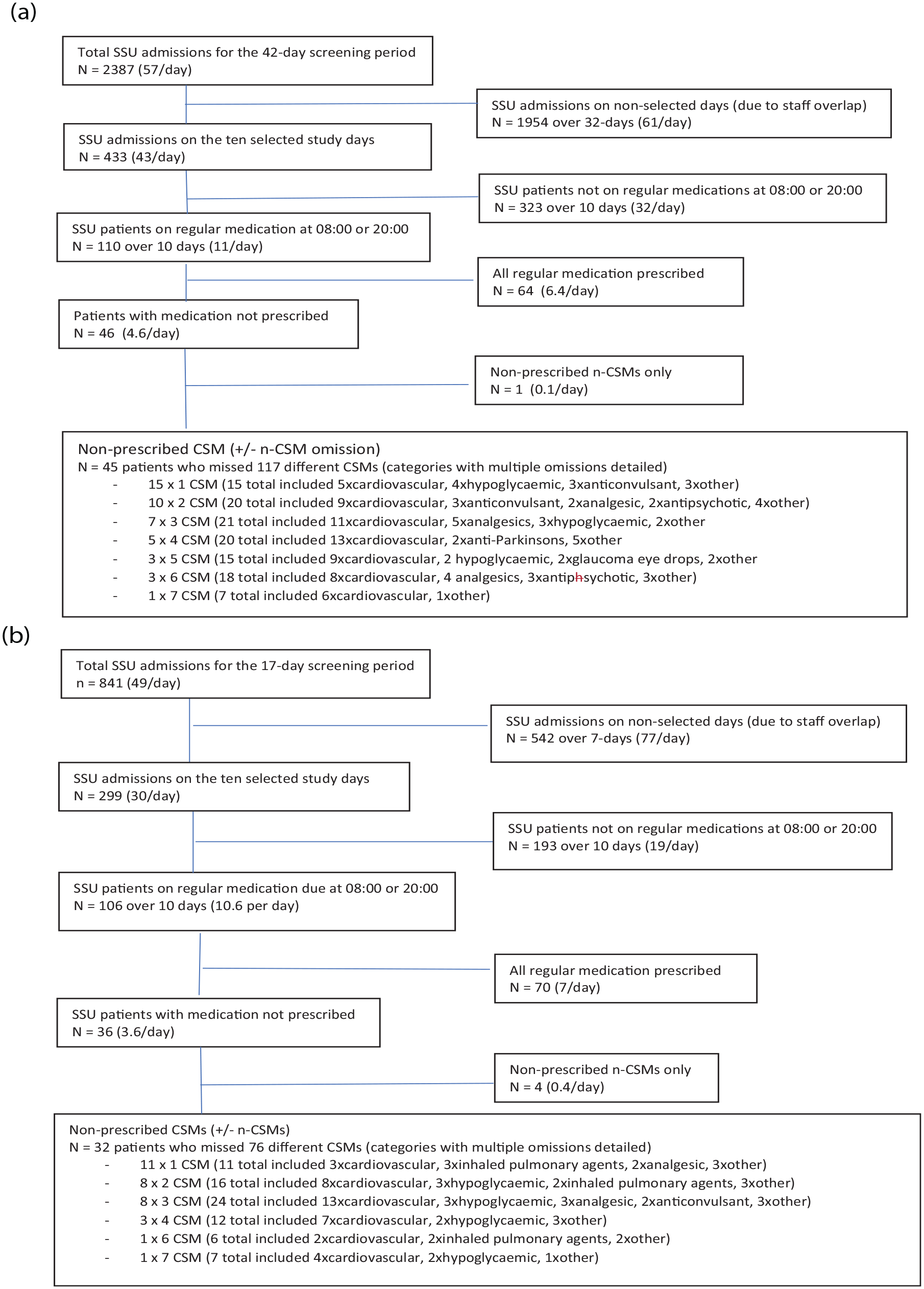
(a) Pre-intervention patient flow regarding medication prescription and (b) post-intervention patient flow regarding medication prescription.
There was a non-significant reduction in the percentage of patients with CSM omission between the pre- and post-intervention periods (41% [95% CI: 32-50] to 30% [95% CI: 21-39], difference −11% [95% CI: −23 to 2], P = .10). Between-period difference in the percentage of patients with either n-CSM or any regular medication omission is shown in Table 2.
Pre- Versus Post-Intervention Comparison of Patients With Medication Omissions.
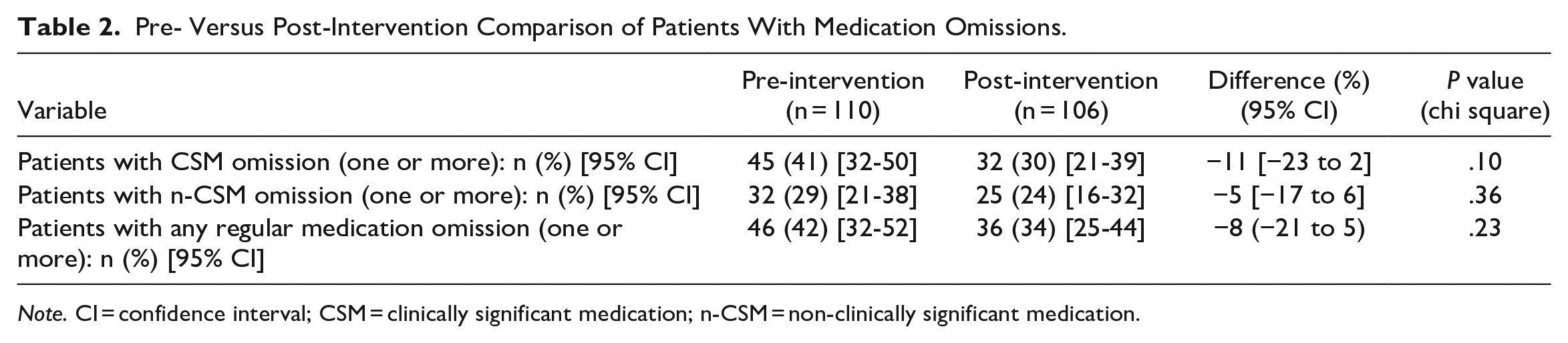
Note. CI = confidence interval; CSM = clinically significant medication; n-CSM = non-clinically significant medication.
The 45 and 32 patients with CSM omissions in the pre- and post-intervention periods were not prescribed a total of 117 and 76 different CSMs respectively. Individual patients were not prescribed between 1 and 7 CSMs. (Figure 2). The most commonly non-prescribed CSMs in both periods were cardiovascular medications. Frequency of missed CSMs by medication category is detailed in Figure 1.
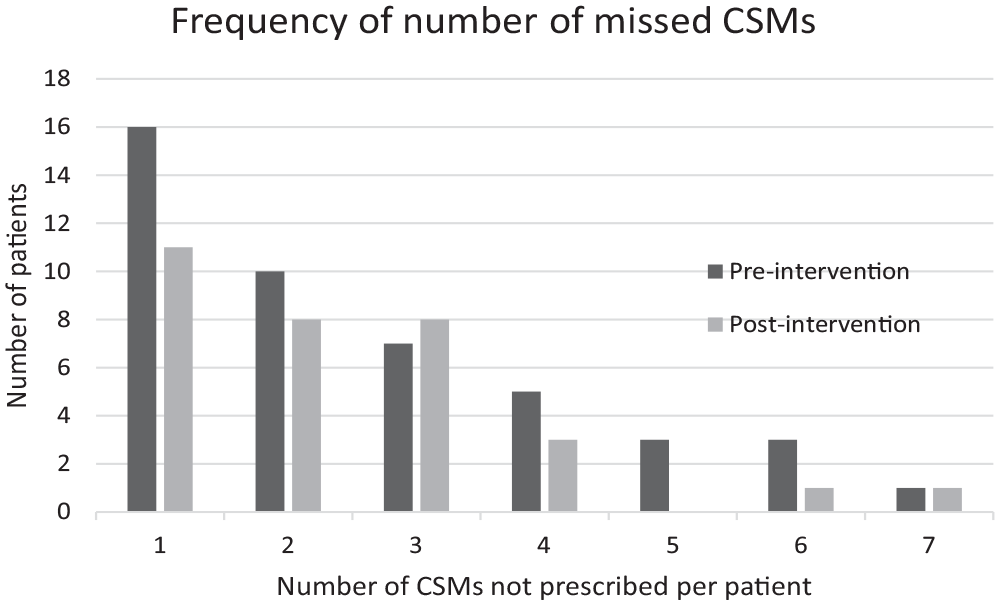
Frequency of number of CSMs not prescribed for individual patients.
For the pre- and post-intervention periods no adverse events related to medication non-prescription were detected in either the patients’ medical notes or in the Riskman system.
Discussion
This study evaluated a multifaceted intervention aimed at reducing CSM prescription omissions for SSU patients without increasing ED expenditure or resources. The resulting improvement from 41% to 30% did not reach our a priori benchmark of halving the CSM omission rate. Consequently, the difference (−11%, 95% CI: −23% to 2%) lacked statistical significance.
Two important differences between this and other studies on medication error rates must be noted. Firstly, the study hospital already uses electronic prescribing, which is proven to significantly reduce errors involving wrong medication, dose, or route.13,27 Secondly, this intervention only addressed CSM non-prescription for SSU patients. Most research has included all types of prescribing and administration errors,1,19-21 and evaluated interventions such as technological aids, teleconsultation, automated drug distribution systems and individualizing patient medication packs.5,13,16,17,27 These interventions, however, rely on presence of an initial prescription. Barriers to accurate prescribing are known to include general workload and interruptions,4,18 but specific preventers of prescription initiation are unknown. This would be of interest but was beyond the scope of this study.
Staff-related interventions to reduce medication error have been described with mixed results. These include junior-senior physician pairing for medication reviews and other types of prescription double-checking,20,28 but their specific impact on prescription omission is unknown. Our intervention did include 2 forms of dual checking, with the addition of prescription-related questions to the SSU handover checklist, and the overnight SSU nurse-doctor meeting. The contribution of these components could not be separately evaluated, but the overall impact of our intervention was non-significant.
The intervention which is consistently reported to have the most significant impact on both prescribing completeness and accuracy is an expanded role of the clinical pharmacist. Improvements have previously been reported in all hospital areas, including medical and surgical wards, ICUs, the acute ED and ED SSUs.8,10-13 Reductions in overall medication errors by over 90% have been reported, from baseline rates over 60% to less than 10%. 14 Described clinical pharmacist roles vary, but usually include admission medication reconciliation.8,10-13,29 Intuitively, provision of this information to the initially attending acute ED doctor should improve the regular medication prescription rate.
Medication reconciliation can be time-consuming, however, so pharmacist availability must match the expected workload. At our hospital, the 1 ED-based pharmacist is instructed to perform medication reconciliation for “sicker” patients awaiting inpatient admission rather than “stable” SSU patients. However, SSU patients are older and have high polypharmacy rates, both factors which contribute to medication errors.1,16,22,23 Regardless, time constraints do not allow 1 ED pharmacist to perform admission medication reconciliations for both patient cohorts. Given this, our intervention could only involve minimal assistance from the ED pharmacist.
The clinical importance of not delivering patients’ regular CSMs also warrants discussion. We found that CSM omission was common, with most patients having non-prescription of 3 or more regular medications. While the morbidity and mortality associated with errors such as wrong medication, patient, route, or dosage are well described,1,2,5,7 the consequences of CSM non-prescription in an ED SSU have been less examined. Although adverse events may be obvious and severe, such as seizure following regular anticonvulsant omission, most are less prominent. Our most frequently non-prescribed CSMs were cardiovascular and hypoglycemic agents. Given usual SSU admission durations of <24-hours, the seriousness of resultant short-term alterations in coagulation status, blood pressure, or blood sugar could be debated. Opioid or benzodiazepine withdrawal symptoms are easily corrected and have no ongoing effects. Despite this, the correct delivery of regular medications while in hospital is a recognized and important component of patient-centered care which should not be neglected. 30 It is reasonable that our ED patients should expect us to get this right.
In summary, the impact of our multifaceted intervention was not statistically significant. Without an increase in existing resources, we could only reinforce already present expectations, with the addition of some process changes. Acute ED doctors and nurses are busy, and neglecting to ensure prescription of medications for their SSU patients is unlikely to be deliberate. The overnight SSU senior nurse and junior doctor are also busy and protected time to go through patient medication charts is difficult to guarantee. The 1 ED pharmacist was already fully utilized, so adding more than 1 or 2 morning medication reconciliations per day was not possible. In a system where everyone is already trying and working hard, the benefits from asking people to try harder and work harder are limited. It seems unlikely that we could further reduce our CSM omission rate without increasing resources. The related literature supports that the change most likely to reduce our non-prescription rate to <10%, would be the addition of an ED pharmacist to perform SSU admission medication reconciliations.8,10-13,29
This study has several limitations. Firstly, the desire to halve the medication omission rate from the suspected 40% to about 20% was arbitrary. The effect size which equates with “clinical significance” in this setting is debatable. Incomplete medical recording and non-inclusion of the occasional regular medications only taken at times other than 08:00 or 20:00 will likely have resulted in a small underestimation of the true CSM non-prescription rate. Once prescribed, however, the electronic system ensured that medication name, dose, ordering time and administration were all accurate. Base rates of prescribing omissions may vary at different types of EDs, including those without electronic prescribing systems. CSMs were defined by expert consensus within our group, but these could be debated, as could the clinical importance of their omission. Population matching between study periods is always difficult, but ours were in the same season and within a single junior medical staff rotation. The COVID-19 pandemic influenced ED attendance numbers (lower) and acuity (higher) in the first half of 2020, but the ED census and SSU admission rates were similar between study periods, as were the number of eligible patients per day. Due to the retrospective design, detection of adverse events is likely to have been incomplete, however the lack of Riskman reports suggests that no serious morbidity arose. Monitoring the effect of the intervention over time was beyond the scope of this study. Further improvements may have occurred with embedding of the systems, but initial gains following a well-publicized introduction may also not be maintained.
In conclusion, we found that work practice changes within existing resource constraints resulted in a non-significant change in non-prescription of regular CSMs for SSU patients.
Supplemental Material
sj-docx-1-hpx-10.1177_00185787231194999 – Supplemental material for Regular Medications in the Emergency Department Short Stay Unit (ReMedIES): Can Prescribing be Improved Without Increasing Resources?
Supplemental material, sj-docx-1-hpx-10.1177_00185787231194999 for Regular Medications in the Emergency Department Short Stay Unit (ReMedIES): Can Prescribing be Improved Without Increasing Resources? by Aidan B. Jackson, Mark Lewis, Robert Meek, Jeniffer Kim-Blackmore, Irim Khan, Yong Deng, Jaime Vallejo and Diana Egerton-Warburton in Hospital Pharmacy
Footnotes
Acknowledgements
Nil.
Authorship Statement
ML and JKB originally conceived the study with contributions from RM and DEW. All authors contributed to devising the ReMedIES intervention. ML and ABJ were responsible for data acquisition and entry. All authors contributed to study definition derivation and were responsible for clinical outcome allocations. RM and ABJ performed the data analysis. RM has qualifications in basic and advanced biostatistical methods. RM and ABJ drafted the manuscript with ongoing contributions from all authors. RM takes responsibility for the manuscript as a whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no external funding for study conduct. Internal funding covered minor expenses.
Ethics Statement
Study conduct was approved by the Monash Health Human Research Ethics Committee, as detailed in the first paragraph of Methods.
No Patient or Public Contribution
Given the retrospective nature of the study, patient or public contribution was not considered feasible.
Data Availability
Requests for further data should be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.