
Abstract
Objective:
This study aimed to compare the knowledge levels of mothers who received education on home accidents and prevention for children aged 0–6, delivered either face-to-face or via social media, and to evaluate the effectiveness of this education.
Design:
Quasi-experimental study with a pre-test/post-test control group design.
Method:
Mothers of children aged 0–6 attending an outpatient clinic, who consented to participate in the study, were assigned to three groups (face-to-face education, social media, control) based on days of the week they attended, with 60 participants per group, totaling 180. All mothers completed a personal information form and the Identification of Safety Precautions for Home Accidents Scale for children aged 0–6. Face-to-face sessions were held in groups of five; social media education was shared on Instagram over 21 days, with no intervention for the control group. After 21 days, mothers completed the scale again.
Results:
The post-test scale scores of the face-to-face and social media education participants were higher than those of the control group. Among those receiving face-to-face education, the mean post-test scale scores were higher than those of the social media group.
Conclusion:
In this study, education provided to mothers on home accidents and preventive measures, both face-to-face and via social media, showed efficacy. Diverse methods can be employed to provide mothers with education about home accidents and home accident prevention. Future studies may find the use of social media particularly suitable for engaging larger groups.
Introduction
Home accidents are unintentional injuries that occur in and around the home and represent a significant cause of serious health problems (Conk et al., 2013). According to the World Health Organization (WHO, 2024), of the 4.4 million deaths attributed to injuries worldwide, approximately 3.16 million are the result of unintentional injuries. In the 5–29 age group, three of the five leading causes of death are injury-related. According to the Turkish Statistical Institute (TÜİK, 2022), external injuries and poisonings were the leading causes of death among children aged 1–17 in 2022, with 1,275 fatalities reported. The high risk of home accidents in early childhood can be attributed to ongoing neuro-motor, physical, sensory, cognitive and psychosocial development, which may limit children’s ability to recognise dangers and protect themselves (Conk et al., 2013; Karatepe and Ekerbiçer, 2017).
Due to spending the majority of their time at home, a lack of awareness of dangers and their natural curiosity, children aged 0–6 are at high risk of home accidents (Çiçek et al., 2022; Silva et al., 2016). Common home accidents involving children include falls, drowning, burns, cuts and poisoning (Törüner and Büyükgönenç, 2012). In Türkiye, Celep and Yardımcı (2021) reported that 70.5% of home accidents occurred in the presence of the mother. Other studies indicate that home accidents often happen even when children are not alone, frequently due to inattention, lack of supervision or inadequate safety precautions (Gündüz and Aytekin, 2015; Şekerci and İnal, 2016). Research highlights that some mothers lack awareness of home accident risks, emphasising the importance of guidance in creating safe home environments and the potential value of nurse-led education programmes (Akça et al., 2017; Çapık and Gürol, 2014).
In the published literature, numerous studies have addressed safety precautions for home accidents, first aid practices and associated risk factors. However, research specifically focusing on educational interventions aimed at preventing home accidents remains limited. In a randomised controlled trial conducted in Croatia, Tokalić et al. (2023) compared face-to-face and web-based (asynchronous) educational methods. Participants in the face-to-face group received instruction on evidence-based decision-making through interactive presentations and practical exercises in a classroom setting. The web-based group received the same content through asynchronous interactive modules on an online platform, allowing them to manage their own learning pace. Significant improvements in post-test scores were observed in both groups, and no statistically significant difference was found between the groups in terms of learning outcomes. Similarly, a study in Japan by Ichikura et al. (2024) involving nursing students found comparable results between online video-based education and face-to-face training about patient communication. They found that both interventions positively affected key parameters in understanding and confidence in communicating with patients. These findings suggest that digital education methods can serve as effective alternatives to face-to-face approaches, particularly for conveying theoretical knowledge.
Barriers such as the limited number of available healthcare professionals and nurses, as well as constraints of time, space and instructional materials, hinder the consistent and widespread delivery of in-person training. However, increasing access to mobile devices in today’s society has made digital and online education a promising alternative to traditional face-to-face methods in home accident prevention. Rad et al. (2022) conducted a randomised educational intervention study in Iran comparing face-to-face and virtual training methods. In the face-to-face group, participants received 6 hours of training using slides, lectures and mannequins. The virtual group received the same content via a video on CD, which included a detailed explanation of the project objectives. Following training, both groups demonstrated significant improvements in four skill domains (p ⩽ .005); however, skill levels in the face-to-face group were higher. These results indicate that both approaches can be effective in improving skills, yet face-to-face education may offer superior performance in certain critical areas. Thus, e-learning methods can be considered effective alternatives or complements to more traditional forms of education.
Despite the widespread use of social media platforms such as Instagram by parents, studies evaluating the effectiveness of health education delivered via social media and its comparability to face-to-face education remain scarce. Given this gap, Instagram may serve as a valuable tool for delivering health education content. In this context, comparing the effectiveness of Instagram-based education with traditional face-to-face methods may offer a useful approach to increasing awareness of home accident prevention. Therefore, the aim of the present study was to compare the effects of home accident education, designed for parents of preschool-aged children, when delivered face-to-face versus via Instagram, on levels of parental knowledge.
Methods
The study was designed as a pre-test/post-test, control group quasi-experimental investigation and was conducted between 30 September 2023 and 3 December 2023, at the paediatric outpatient clinic of Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital in Ankara, the capital city of Türkiye. Although the hospital primarily specialises in oncology, outpatient clinics also provide general paediatric care services. Specifically, the two paediatric outpatient units where the study was carried out serve the general population and are not limited to children with oncological conditions.
The study population comprised mothers who visited the hospital’s general paediatric outpatient clinics between 30 September and 20 October 2023, and who had children aged 0–6 years.
To determine the sample size, a power analysis was conducted using the G*Power 3.1.9.7 software. In studies where the expected mean difference between groups is unknown, an effect size of .80 is commonly accepted as appropriate (Joseph et al., 2019). Based on the parameters of α = .05 (Type I error), β = .20 (Type II error) and an effect size of .25, the minimum required sample size was calculated to be 53 participants per group, totaling at least 159 participants. To strengthen the design, 60 mothers were included in each group: face-to-face education, social media education and control, bringing the total sample to 180 mothers.
The inclusion criteria for the study were as follows: mothers who presented to the paediatric outpatient clinic of the study hospital, had children aged 0–6 years, were literate in Turkish, who used the relevant social media platform (Instagram) and who voluntarily agreed to participate. For the face-to-face education group, an additional criterion was the presence of a caregiver (e.g. a father, grandmother, grandfather, etc.) who could look after the child during the educational session. Having someone to care for the child while she received the face-to-face education allowed the mother to focus on the education provided.
Exclusion criteria included mothers withdrawing at any stage of the study, being unreachable by phone for the post-test, failure to follow or unfollow the study account in the social media group and failure to complete the face-to-face education session in the relevant group.
The researcher attended the outpatient clinic on 30 September 2023 and continued data collection until the target sample size was achieved. To prevent potential cross-contamination between groups, randomisation was not undertaken. Instead, convenience sampling was used, with group allocation being based on the day of the week participants visited the clinic: mothers visiting on Mondays and Tuesdays were assigned to the face-to-face education group; those visiting on Wednesdays and Thursdays were assigned to the social media (Instagram) group and those visiting on Fridays were assigned to the control group.
Data collection
Instruments
Personal information form
Developed from a review of the literature (Celep and Yardımcı, 2021; Çiçek et al., 2022; Gündüz and Aytekin, 2015; Şekerci and İnal, 2016), this form included 12 questions on topics such as the mother’s age, employment, age at first motherhood and prior experiences of home accidents. The first 10 questions were asked during the initial interview, while two additional questions (on the incidence of home accidents and preventive measures taken) were asked 21 days post training.
Identification of safety precautions for home accidents scale for mothers of children aged 0–6
The scale’s reliability and validity were confirmed by with a Cronbach’s alpha of .82. Positive items are scored from 1 (never) to 5 (always), while negative items (6, 9, 23, 26, 30 and 40) are reverse-scored. Scores range from 40 to 200, with higher scores indicating greater precaution levels. Completion takes approximately 15–20 minutes (cited in Özmen et al., 2007).
Educational content
The educational content was developed by the researchers based on the relevant literature and the Safety Precautions Scale (Çalışkan and Balcı, 2018; Celep and Yardımcı, 2021; Çiçekler et al., 2012). The content and accompanying visuals were reviewed by three experts in paediatric nursing and one expert in public health nursing. Revisions were made in line with the expert feedback received, resulting in a Content Validity Index (CVI) of .81. The same content was used to create educational plans and materials for both methods of delivery.
Training plans
Instructional design is a systematic process that integrates teaching principles, materials, activities, resources and assessments into a cohesive plan (Dooley and Lindner, 2005). The literature describes numerous instructional models, with the Dick, Carey and Carey (DCC) model being recognised for its incorporation of behavioural, cognitive and constructivist approaches, although it is primarily behavioural in its foundations (Dick et al., 2001; Gustafson and Branch, 2007; Kıyak et al., 2020; Kara, 2022). In this study, the DCC model was selected as the basis for developing the educational plans.
Face-to-face educational plan
Expected behaviours: Increase mothers’ knowledge about home accidents and precautions and encourage preventive measures at home.
Determine initial behaviours: Assess willingness to learn about home accidents.
Environment: Nurse’s office.
Set learning objectives: Increase knowledge, awareness and application of safety measures.
Assessment tools: Use the ‘Identification of Safety Precautions for Home Accidents Scale’.
Teaching methods: Face-to-face group instruction, lecture, question and answer.
Materials: PowerPoint slides, brochure.
Develop assessments: Personal information form and safety scale.
Review design: Participants – volunteer mothers on Monday/Tuesday; duration – 40 minutes.
Social media educational plan
Expected behaviours: Increase knowledge of home accidents, encourage preventive actions at home.
Determine initial behaviours: Willingness to learn about home accidents.
Environment: Instagram.
Set learning objectives: Enhance knowledge, awareness and application of safety measures.
Assessment tools: Use the ‘Identification of Safety Precautions for Home Accidents Scale’.
Teaching methods: Online education via social media, narration, question and answer.
Materials: Posts and stories.
Develop assessments: Personal information form and safety scale.
Review design: Participants – volunteer mothers on Wednesday/Thursday; duration – 21 days with daily posts (five posts per day); ● Week 1: Introduction to home accidents, importance and prevention of falls. ● Week 2: Prevention of burns, drowning and poisoning. ● Week 3: Prevention of injuries from sharp objects and electrical accidents.
Training materials
Following expert feedback, the educational content was finalised, and a PowerPoint (ppt) presentation, along with a brochure, was prepared for the face-to-face sessions. The presentation comprised 42 slides, while the brochure provided a concise summary of key information. To reinforce understanding and learning, question-and-answer technique was employed during the face-to-face presentations. For the social media education, the same content in the ppt presentation and brochure was adapted into Instagram posts and Instagram stories. This resulted in a total of 74 posts and nine stories shared through the study Instagram account. To ensure interaction between members of the social media group, question-and-answer technique (in the form of interactive polls) was also used in Instagram stories.
The content of the visual materials was evaluated by three experts in the field (one public health expert and two child health nursing faculty members). The suitability of the visuals was assessed by an expert in computer and instructional technology.
Implementation of training
Face-to-face education group
Mothers included in the study signed an informed consent form and received a copy. They first completed 10 items on the Personal Information Form and the Safety Precautions Scale. When four participants were ready, a 30-minute interactive training session was held in the nurse’s room using a ppt presentation followed by discussion. During the session, children were supervised by a second caregiver. At the end, support brochures were provided. After 21 days, the scale was re-administered by phone. After data collection was completed, the Instagram account was shared with members of the face-to-face education group.
Social media education group
Mothers included in the study signed an informed consent form and then completed the first 10 items of the Personal Information Form and the Safety Precautions Scale. They were introduced to the Instagram account (@ev_kazalari) where the educational content was shared and were encouraged to follow it. Between 25 October and 8 November 2023, daily posts and stories were shared according to the training plan. Participation was monitored through interactive polls shared via Instagram Stories; however, whether the posts were read or not was not tracked, and mothers who did not participate in the polls were not excluded from the study. Between 29 November and 3 December 2023, mothers were contacted again to re-administer the Safety Precautions Scale and complete the final two items of the personal information form, concluding the process.
Control group
Mothers who signed the informed consent form completed the first 10 items of the Personal Information Form and the Safety Precautions Scale after receiving the necessary instructions. No training was provided to members of this group. After 21 days, mothers were contacted again to re-administer the Safety Precautions Scale and complete the final two items of the personal information form. The process concluded with the sharing of the social media account with the control group.
Data analysis
The effectiveness of the training provided to mothers was assessed by any increase in scores on the Identification of Safety Precautions for Home Accidents Scale. Statistical analyses were conducted using IBM SPSS for Windows, version 26. Kolmogorov-Smirnov and Skewness-Kurtosis tests confirmed that the data followed a normal distribution. Descriptive statistics included means, standard deviations, minimums, maximums, frequencies and percentages. All variables in the dataset had Skewness and Kurtosis values within the range of −1.5 to +1.5. One-Way ANOVA was used for group comparisons, followed by the Duncan test for multiple comparisons, and paired t-tests assessed pre-test and post-test score changes, with statistical significance set at p < .05.
Ethical approval
Ethical approval was received from the ethics committee at the Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital. Before starting the study, mothers were informed about the research and training, any questions were answered and informed consent was obtained from those willing to participate, with a copy of the information and the completed informed consent form being provided to them. Permission for its use was obtained from the developer of the Safety Precautions Scale used in the study.
Results
There was no statistically significant difference in descriptive characteristics between the face-to-face education group, the social media education group and the control group (p > .05) (Table 1).
Participants’ characteristics.
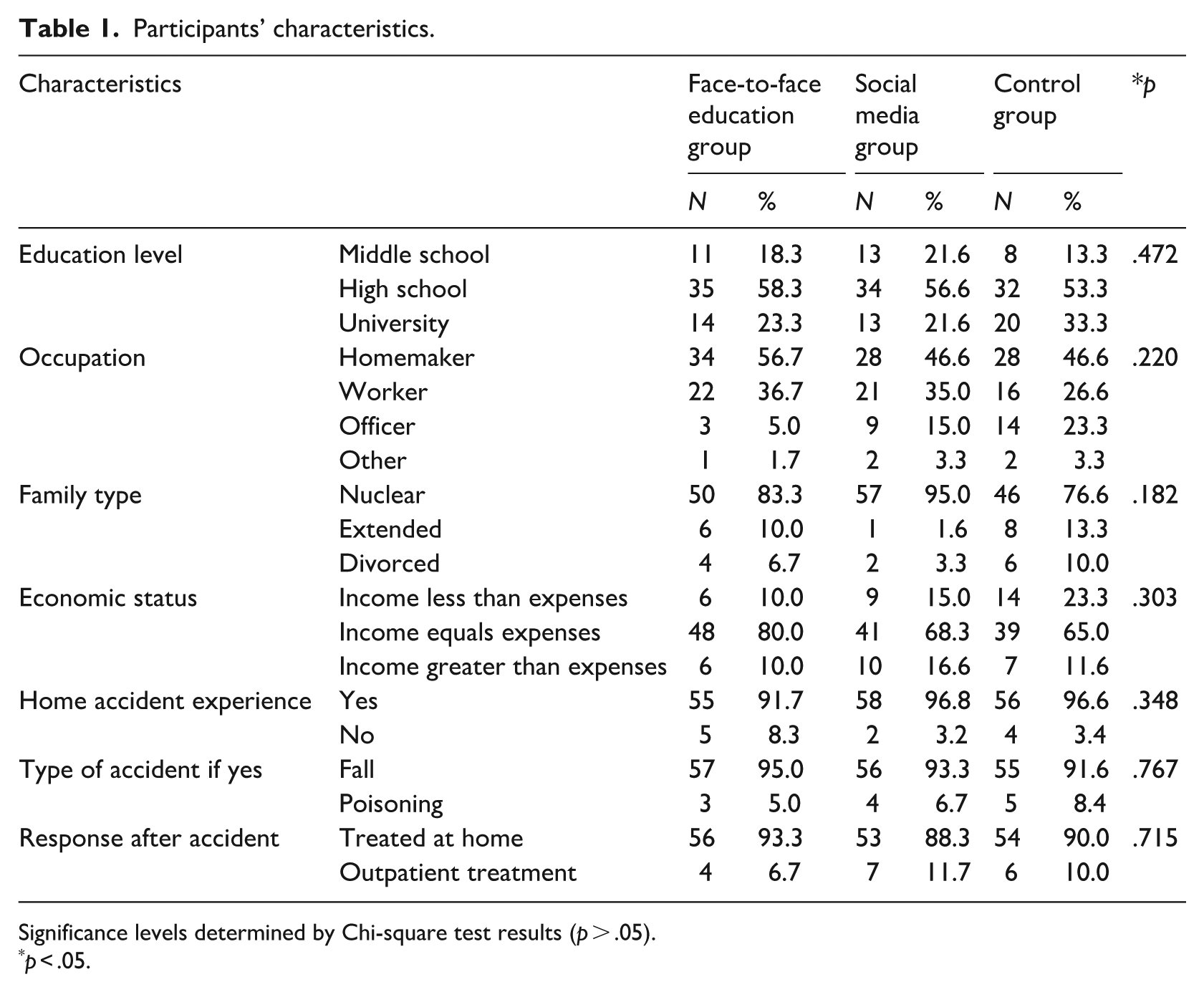
Significance levels determined by Chi-square test results (p > .05).
p < .05.
In the face-to-face and social media education groups, the post-training scale score averages increased within the groups (p = .001). No significant change was observed in the control group (p > .05) (Table 2).
Test and post-test scale scores on the identification of safety precautions for home accidents scale for mothers of children aged 0–6.
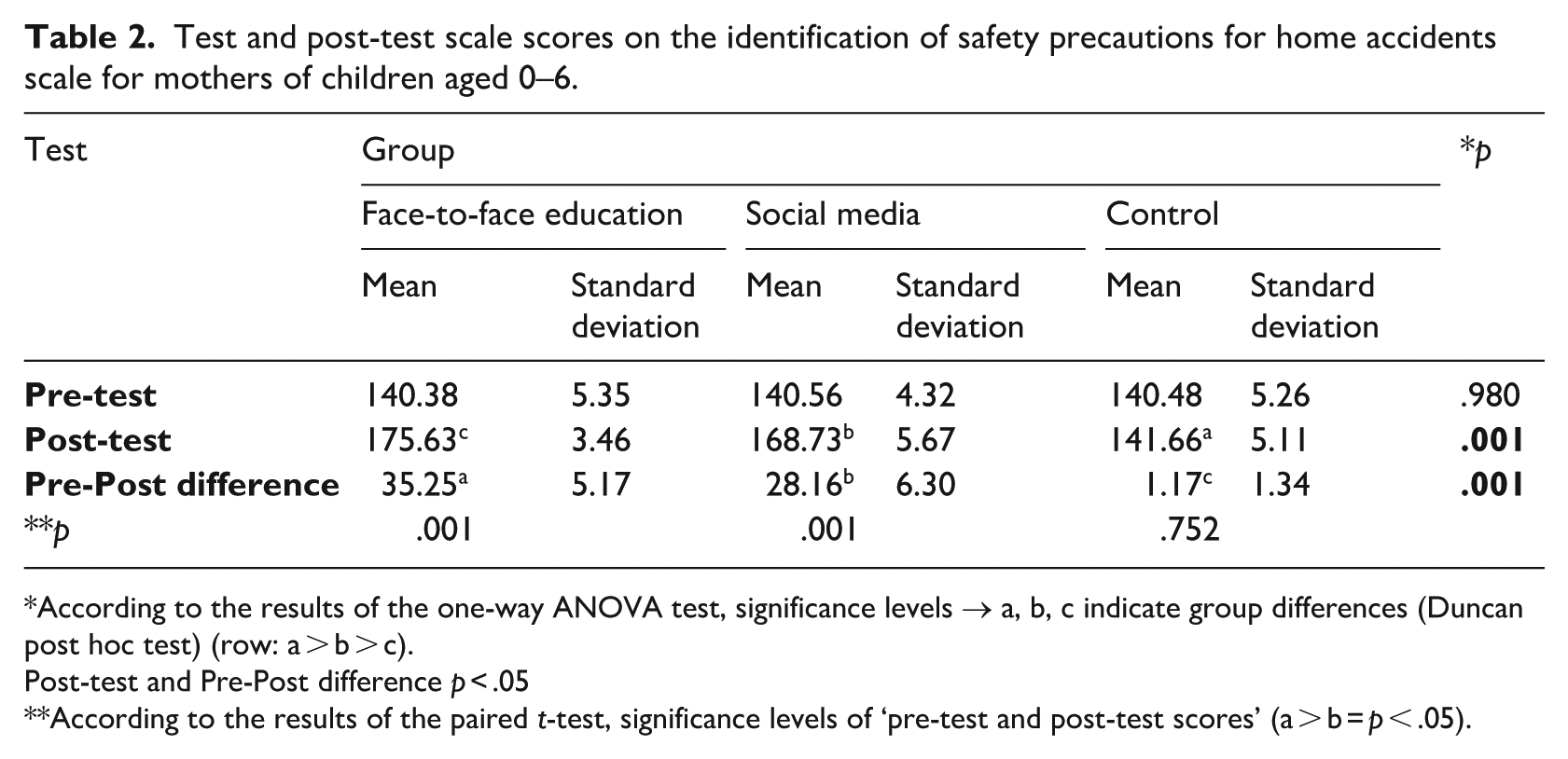
According to the results of the one-way ANOVA test, significance levels → a, b, c indicate group differences (Duncan post hoc test) (row: a > b > c).
Post-test and Pre-Post difference p < .05
According to the results of the paired t-test, significance levels of ‘pre-test and post-test scores’ (a > b = p < .05).
The post-test scale scores in the face-to-face and social media education groups were higher than those in the control group. The post-test scale score averages in the face-to-face education group were higher than those in the social media group (p < .05) (Table 2).
No statistically significant differences were found between the groups in terms of mothers’ reported preventive measures for home accidents and their children’s history of home accidents after the post-test (p > .05) (Table 3).
Mothers’ preventive measures for home accidents.
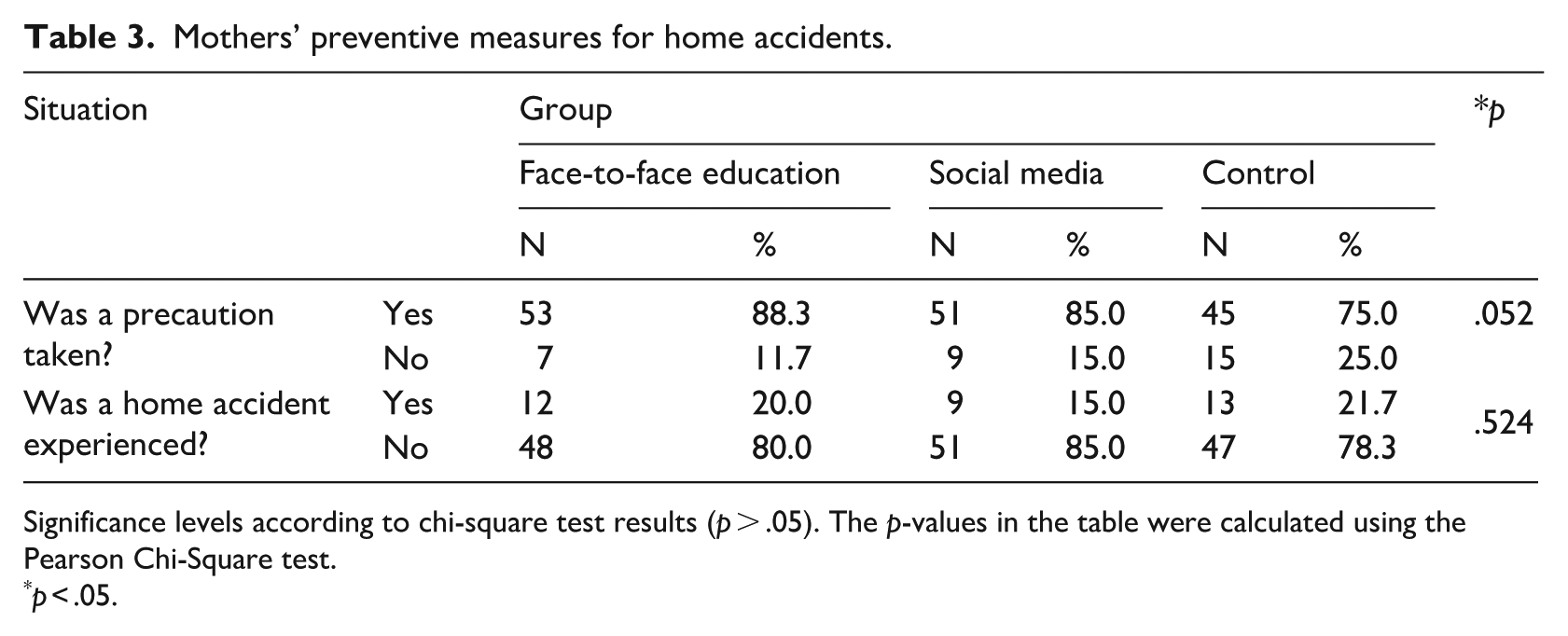
Significance levels according to chi-square test results (p > .05). The p-values in the table were calculated using the Pearson Chi-Square test.
p < .05.
Discussion
This study investigated the effectiveness of two different educational methods in delivering training on home accidents and prevention to mothers of children aged 0–6. The pre- and post-training knowledge levels of the trained groups were compared with those of the control group after 21 days. The findings demonstrated that the increase in knowledge levels among the trained groups was significantly higher than that among those who did not receive training. Enhancing mothers’ knowledge about home accidents and prevention is crucial, as previous studies have reported that, in most cases, children are not alone during accidents, with 70.5% of children being in the presence of their mothers at the time of the incident (Celep and Yardımcı, 2021; Gündüz and Aytekin, 2015). The literature recommends improving mothers’ awareness of home accidents and prevention, guiding them in creating safer home environments and undertaking safety education for their children (Akça et al., 2017 Çapık and Gürol, 2014). Both the educational methods used in this study – face-to-face education and social media training – resulted in increased knowledge levels among mothers, revealing their value in educating mothers about home accident prevention.
Unlike previous studies, which have not compared face-to-face education with social media-based education, this study examined the effectiveness of these two methods side by side. The results revealed that the face-to-face education group experienced a greater increase in knowledge levels than the social media group. Literature suggests that good-quality face-to-face education can foster an interactive learning environment in which shared experiences within the group enhance the retention of information (Eroğlu and Kalaycı, 2020; Karataş, 2003). In this study, the more significant improvement in the face-to-face education group may be attributed to the smaller group sizes, the mothers having children of similar ages and their shared living environments. In contrast, promoting the participation of mothers in the social media training and ensuring their comprehension of the information presented was more challenging. This likely contributed to the relatively smaller increase in knowledge levels in the social media group.
Although focused on different topics, previous studies have demonstrated that education delivered through social media can result in increased knowledge levels post training. The findings from these studies align with the results of our research (Alp and Kaleci, 2018; Koç and Ayık, 2017; Logenthini et al., 2017). Studies highlight that social media-based education has advantages due to its accessibility, its ease of implementation and the absence of constraints such as time, duration and location (Atallah et al., 2023; Güler, 2015; Wang et al., 2022). The increase in knowledge levels achieved through social media training is particularly significant, as it provides a viable alternative when face-to-face education is not possible and enables the education and training to reach larger audiences.
Limitations
This study was conducted with parents of children aged 0–6; therefore, the findings cannot be generalised to the mothers of children of other age groups. Monitoring access to the educational content on social media was limited due to constraints in sample size, time and researcher capacity. The findings from this study may not be relevant to other demographic or socioeconomic contexts.
A key limitation of the study was the lack of a specific plan to measure the extent to which participants in the social media group followed the educational content, making it unclear how much of the education they actually received. Furthermore, the degree to which participants accessed, read and comprehended the content could not be directly monitored.
In addition, the effectiveness of the education was evaluated only in the short term, with no medium- and long-term follow-up. Future studies should include long-term assessments to better understand the lasting impact of the intervention.
Conclusion
This study found that the education and training provided to mothers on home accidents and preventive measures, both face-to-face and via social media, displayed efficacy. A significant increase in mothers’ knowledge levels was noted after the training, demonstrating the effectiveness of both educational programmes. Future studies should explore how the use of social media in home safety and child accident education can be made more efficient. This may require the development of more interactive, comprehensive and longer-term training programmes aimed at preventing child accidents, thereby enhancing the awareness levels of mothers and other family members.
Footnotes
Acknowledgements
This study was conducted as a master’s degree thesis study in the Department of Nursing at the Ankara University Health Sciences Institute.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
AI use
In the preparation of this manuscript, support was received from ![]() version), with respect to text translation and language editing. AI assistance was used solely to enhance translation quality and writing style; the scientific content, analyses and conclusions of the study were entirely developed by the authors. The authors take full responsibility for the content and accuracy of this work.
version), with respect to text translation and language editing. AI assistance was used solely to enhance translation quality and writing style; the scientific content, analyses and conclusions of the study were entirely developed by the authors. The authors take full responsibility for the content and accuracy of this work.