
Abstract
Objectives:
Increasing childhood health literacy (HL) is a crucial means of improving health outcomes and reducing preventable deaths globally. Understanding how to best support children’s HL development in schools is essential. However, identifying pedagogical strategies that develop children’s HL relies on a fit-for-purpose measure. Currently, no universally accepted approach for measuring HL among children exists. The purpose of this paper was to propose and discuss how a curricular approach to assessing children’s HL could provide a means to overcoming the challenges with existing children HL measures.
Design/Methods:
The discussion is framed by the key components of assessment – outcome of interest, and collection, analysis and interpretation of data – and is underpinned by contemporary HL and educational research.
Setting:
The Australian Curriculum is used to discuss the approach in practice.
Results:
A curricular approach to HL assessment suggests that HL assessment may work best when it is relevant to the child and their context, is integrated with other areas of the curriculum, allows children to demonstrate a wide range of HL skills and contains an element of open-endedness. Measurement could be guided by a rubric (underpinned by a taxonomy), and interpretation of scores consistently aligned with the learning intentions outlined in the curriculum.
Conclusion:
A curricular approach provides a contextually adaptive framework from which HL assessment tools for children can be developed.
Background
Chronic diseases such as heart disease and diabetes are a leading cause of morbidity and mortality internationally (World Health Organization [WHO], 2020), one-third of which can be prevented with early intervention (Australian Institute of Health and Welfare [AIHW], 2016). Improving health literacy (HL) can support individuals to form educated and autonomous health-related decisions across the life-course and improve population health. HL is influenced by social context and comprises the ‘social and cognitive skills required by individuals and community to access, understand, appraise, remember and apply information to promote health and sustain healthy behaviours throughout the life-course’ (WHO, 2014: 9). As many health attitudes and behaviours are formed during childhood (Bröder et al., 2019a) and childhood HL has been shown to predict adult HL (Vamos et al., 2019), supporting children to develop HL can improve their life-course health trajectory. However, there is a paucity of knowledge about how best to support children’s HL development (Otten et al., 2022). Reliable and valid HL assessments are needed to determine which teaching practices produce optimal learning outcomes.
The assessment process refers to ‘the collection, analysis, and interpretation of information related to a particular issue or outcome of interest’ (Secolsky and Denison, 2018: xviii). First, the outcome of interest must be clearly defined (American Educational Research Association [AERA], 2014). Data are then collected using an assessment (e.g. observations, written tasks) and systematically analysed (measurement) (Magno, 2010). Although measurement can analyse objective (e.g. performance-based quiz) or subjective (e.g. grading of artwork) data, the measure (outcome) is usually expressed numerically (Secolsky and Denison, 2018). The inferences made from data are meaningless without interpretation by means of evaluation (Secolsky and Denison, 2018). All four elements of the assessment process (defining the outcome, assessment, measurement, evaluation) are critical for supporting learning and the determination of teaching efficacy.
Many adult HL measures exist; however, children’s HL measurement is understudied (Bollweg and Okan, 2019; Okan et al., 2018). We undertook a systematised search of the literature and found that six generic HL tools/measurement approaches have been developed or adapted specifically for children aged 12 or younger (Table 1). Other HL measurement approaches have been used with children. However, these measure health knowledge as a proxy for HL (Bröder et al., 2019a; Ribeiro et al., 2023), apply tools designed for adults or consider specific elements of HL (e.g. food literacy) rather than HL as an discrete construct (e.g. Reynolds et al., 2012). Two of the six tools included in Table 1 use a multiple-choice quiz, two use self-report, one uses a combination of these two methods and one uses a combination of self-report and multiple-choice/short-answer questions. None of the six tools have been universally accepted as a generic HL measure for children (Bollweg and Okan, 2019; Okan et al., 2018) and issues exist with each tool, as now discussed.
Health literacy measures for children ⩽12 years.
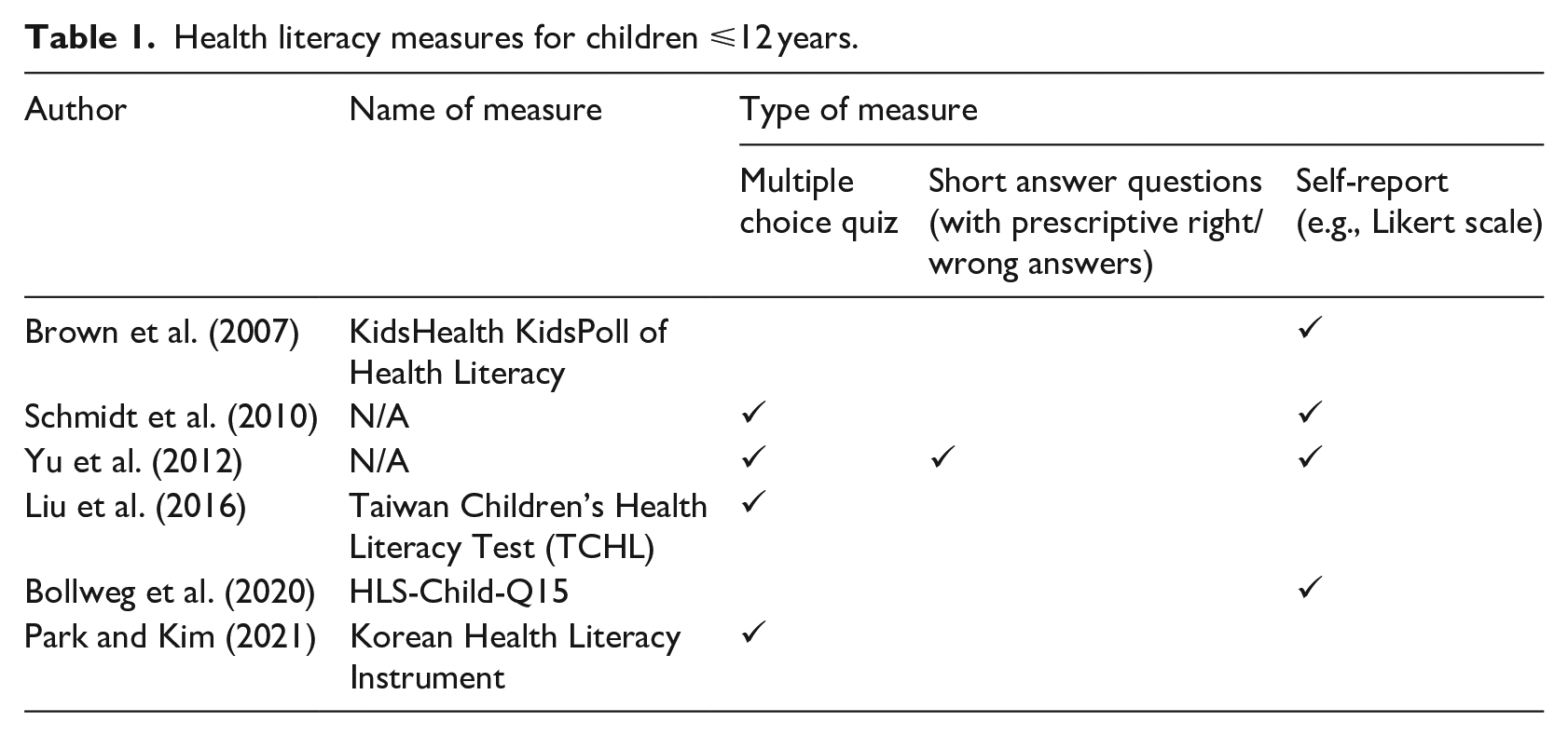
The concept of ‘health’ is socially constructed and subjective: a range of factors such as developmental stage, age, cultural preferences and values all impact what it means to be healthy (Baum, 2015). The skills required to be health literate also differ between individuals and depend on context and the range of interwoven factors affecting health. Short-answer questions and multiple-choice quizzes that are designed as one-size-fits-all measures cannot account for differences across multiple contexts and are not suited to measure individual differences in HL (Osborne et al., 2022; WHO, 2022). Self-report measures allow the individual to define their HL as perceived within their own context; this may explain why the most broadly accepted adult HL measures use this approach (e.g. the Health Literacy Questionnaire) (Osborne et al., 2013).
While self-report has been recognised as a viable solution to overcoming many of the challenges associated with measuring HL, there are problems with this method, particularly among children. Self-report can be associated with informational bias through the inaccurate or false recollection of abilities, beliefs and knowledge (Shephard, 2003). Furthermore, it has been suggested that many children do not begin to develop abstract reasoning skills or the ability to think critically until about the age of 12 years (Marini and Case, 1994). As HL relates to a range of skills (rather than concrete health behaviours) (WHO, 2014), it could be argued that children below the age of 12 lack the cognitive capacity to accurately reflect their HL through self-report.
This paper discusses how a curricular approach could provide a framework for HL assessment that can be adapted to different contexts to provide appropriate, meaningful and useful data for decision-making about strategies for improving children’s HL. While an objective curriculum and performance-based HL measurement instrument has been developed to assess ninth graders (aged 15–16) in Finland (Summanen et al., 2022), there is currently no universally accepted approach to HL measurement for children under the age of 12 (Bröder et al., 2017; Guo et al., 2018; Okan et al., 2018; Otten et al., 2022). This paper’s discussion is framed by the key components of assessment: the outcome of interest, and the collection, analysis and interpretation of data.
Developing a framework for children’s HL assessment
Outcome of interest
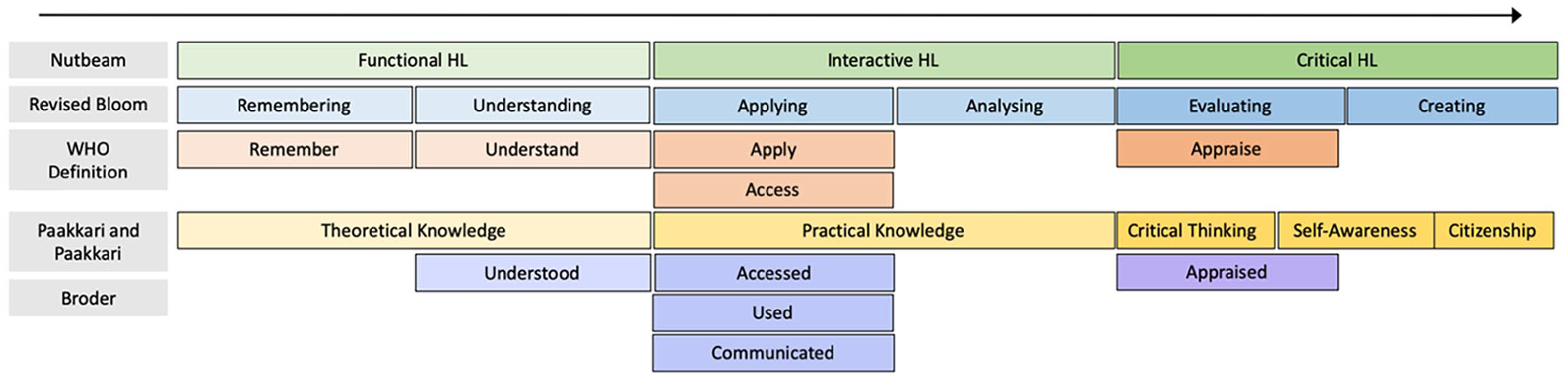
Prior to developing a framework for children’s HL assessment, the concept of HL should be clearly specified to promote clarity in the construct measured. A range of models exist highlighting the crucial knowledge/skills required for an individual to develop HL in their environment. Key models relevant to children include Paakkari and Paakkari’s (2012) core components of HL, the World Health Organization’s (2014) definition of HL and Bröder et al.’s (2019b) Children Youth Target-Group-Centred Definition (see online supplemental file 1). While each model differs, their constituent elements (i.e. HL knowledge/skills) can be hierarchically categorised and related to Nutbeam’s (2000) levels of HL and Bloom’s Revised Taxonomy (Krathwohl et al., 2001) (Figure 1).
Health literacy models compared.
A taxonomy in relation to education is a hierarchical way of categorising learning according to level of complexity; such taxonomies are useful in demonstrating learning progression (Krathwohl et al., 2001). Therefore, viewing HL skills through a taxonomical lens may aid in understanding the order in which HL knowledge and skills are likely to develop. It is a well-established idea that Bloom’s Revised Taxonomy of Educational Objectives and Nutbeam’s levels of HL taxonomy align with one another (Finn and O’Fallon, 2017; Kilstadius and Gericke, 2017). Nutbeam’s three levels of HL are operationalised by the Health Literacy Questionnaire (Osborne et al., 2013). Furthermore, Paakkari and Paakkari have discussed the hierarchical nature of their core components of HL in relation to Nutbeam’s (2000) theory. However, to our knowledge, the relationship between the previously mentioned five models has not yet been discussed. Understanding how each theory relates to the others is important in understanding HL as the outcome of interest.
Nutbeam’s (2000) functional HL refers to the skills required to find and comprehend basic health information. Consequently, it involves lower order thinking tasks such as remembering and understanding. This level of HL can be aligned with Paakkari and Paakkari’s (2012) core component, ‘theoretical knowledge’. Paakkari and Paakkari (2012) acknowledge that theoretical knowledge alone is not likely to be enough to support individuals to make health promoting choices.
According to Nutbeam (2000), interactive HL extends functional HL skills to include cognitive, literacy and social skills that contribute to people’s ability to interact and apply health information. This level of HL aligns with the concepts of ‘applying and analysing’ in Bloom’s revised taxonomy, the WHO’s (2014) concepts of ‘applying and accessing’ and Bröder et al.’s (2019b) concepts of ‘accessing, using, and communicating’ health information. Interactive HL aligns with Paakkari and Paakkari’s (2012) idea of practical knowledge, which relates to the procedural knowledge or skills that allow individuals to apply their theoretical health knowledge to contextualised situations.
Critical HL extends interactive HL skills to include advanced cognitive and social skills that enable people to critically interpret and analyse health information, and to use what they learn ‘to exert greater control over life events and situations’ (Nutbeam, 2000: 264). Therefore, it can be related to higher-order thinking skills such as evaluation, appraisal and creation. The final three elements of Paakkari and Paakkari’s (2012) core components of HL (critical thinking, self-awareness, and citizenship) align with this category due to the complex thinking required to possess each component. Each component could be placed in a hierarchy with critical thinking as a prerequisite for self-awareness, and self-awareness as a prerequisite for citizenship (Paakkari and Paakkari, 2012). The relationships between these HL models are shown in Figure 1.
While Nutbeam’s (2017) levels of HL (including its associated components) remain constant across settings, the specific knowledge and skills required to reach each of the levels varies substantially between individuals and populations, and across different contexts. Consequently, it is difficult to universally describe how HL skills are manifested across settings. To capture HL differences between individuals in different contexts, a tailored approach to HL measurement is required.
School health education (HE) curricula could be used to help define and describe the social and cognitive skills required for children to develop HL, relevant to their age and to the context in which they live. While HL and HE are different, the two concepts are linked. Most health curricula outline the competencies required for an individual to make educated and autonomous health-related decisions in the context in which the curriculum is intended to be enacted. As Paakkari and Paakkari (2012) and Nutbeam (2009) have suggested, HL can be viewed as a learning outcome in schools. Their viewpoints suggest that HL is an outcome of HE, rather than a learning area, or sub-component. Consequently, it can be suggested that HE is what is taught, and that HL relates to the knowledge and capabilities that are learned as a direct result (Gugglberger, 2019). Thus, assessing a child’s progress against the achievement standards in a curriculum could serve to provide an assessment of their HL.
The Australian Curriculum, for example, is a nationally implemented curriculum that comprises different learning areas, one of which is Health and Physical Education (Australian Curriculum Assessment and Reporting Authority [ACARA], 2022). Health and Physical Education is divided into two strands: (1) Personal, Social, and Community Health, and (2) Movement and Physical Activity (ACARA, 2022). In Australia, a concern for Personal, Social and Community Health is commonly known as Health Education. This strand is further broken down into sub-strands, content descriptors, and elaborations that outline the skills and knowledge related to health that a child should learn/develop from kindergarten through to year 10 (ages 5–16 years) to meet a range of achievement standards. The HL of a child in year 5 or 6 (ages 10–12 years) who attends school in Australia could be determined through a variety of assessments linked to the year 5/6 (ages 10-12) achievement standards in the relevant Health and Physical Activity strand of the Australian Curriculum.
While many curricula indicate achievement standards and guide the concepts taught relating to HE, learning experiences and forms of assessment are often selected at the discretion of the teacher or school. For example, students in years 5 to 6 in Australia learn to ‘investigate different sources and types of health information and how these apply to their own and others’ health choices’ (AC9HP6P09) (content descriptor) by ‘analysing nutritional information of different foods’ (elaboration) to develop their ability to ‘analyse health information to refine strategies to enhance their own and others’ health, safety, relationships and wellbeing’ (achievement standard) (ACARA, 2022). Although all year 5 and 6 children should learn these skills, the way children are taught and learn to investigate sources will vary according to the lessons provided by each individual teacher (Alfrey and Brown, 2013). This flexibility is a key component of assessing HL using a curricular approach because it means that each child receives a tailored teaching, learning and assessment experience relevant to their own context and age.
Collection of student HL data
A child’s HL may be most comprehensively assessed through a range of assessment tasks mapped to HE curricula, targeting different components of HL. Key characteristics that are recommended for each individual HL assessment include the following: (1) relevant to the child and their context (Fairbrother et al., 2016; Jang, 2008); (2) integrated with other areas of the curriculum (Fazriyah et al., 2017); (3) allow children to demonstrate a wide range of HL levels (Secolsky and Denison, 2018); and (4) contain an element of open-endedness (Fan et al., 2022).
Relevant to the child and their context
As the skills required to be health literate differ between individuals and contexts (McKenna et al., 2017), an HL assessment would need to be flexible and adaptable to the context of the individual whose HL is being measured. While the approach to measurement could remain consistent, the assessment activities themselves would likely differ.
Relevant assessment activities are also critically important in supporting learning development. A positive relationship has been shown to exist between students’ perceived relevance of a learning activity and their motivation and engagement with education (Fairbrother et al., 2016; Jang, 2008). Furthermore, it has been suggested that improved engagement with education produces positive learning outcomes (Ko et al., 2016). Choosing assessment tasks that are relevant to students in different contexts may develop their HL during the assessment process while supporting a contextually appropriate measure. A one-size-fits-all set of assessment activities designed to universally measure HL would not be appropriate for national or global dissemination.
Integrated with other areas of the curriculum
Integrating learning and assessment experiences with other areas of the curriculum is one approach to contextualising and making learning relevant to students. While many teachers feel comfortable organising learning into discrete subjects (e.g. Mathematics, English), integrating curriculum areas has been shown to improve a variety of learning outcomes (Fazriyah et al., 2017). Integrated learning is more relevant and indicative of ‘real-world’ experiences than subjects taught in isolation (Hieu and Nam, 2019). The integration of activities requires systems that support teachers to use this approach.
Health learning experiences and assessment often include engagement with sensitive topics (Brown and Wissow, 2009). Learning experiences may be most effective when tailored to individuals and integrated with other areas of the curriculum (Otten et al., 2022). Thus, HL assessments are best when conducted by someone who knows the student well and has the capacity to integrate learning experiences (e.g. generalist classroom teachers). It should be noted, however, that many primary generalist teachers report lacking the confidence and competence to develop HL in their students (Otten et al., 2023), and therefore, would likely require support from specialist teachers and professional development.
Capable of demonstrating a wide range of HL levels
To accommodate the various learning levels in the one classroom, HL assessment tasks need to provide students with the opportunity to demonstrate a wide range of HL levels. Primary schools provide a unique setting to develop functional, interactive and critical HL. In Kindergarten/Foundation and year 1 (age 5–6 years), students begin to process information independently, including health information, which means that they can develop functional HL (Yin, 2020). By the end of primary school (at 12 years of age), most students have achieved skills associated with interactive HL, have become capable of abstract reasoning and are able to develop critical HL (Marini and Case, 1994). Critical HL includes critical thinking as well as ‘empowerment, social and political action, and the existence of the concept at both an individual and population level’ (Sykes et al., 2013: 1). Supporting critical HL in primary school settings has previously proved to be challenging, but is not impossible (Fage-Butler, 2018). Some students have the potential to become critical thinkers (and hence may be capable of developing critical HL extending to citizenship) earlier than age 12, while others may never reach this milestone (Van Gelder, 2005). It is, consequently, important that teaching and assessment is differentiated to support the needs of all learners. Furthermore, for an HL assessment to be appropriate, meaningful and useful, children need to be able to demonstrate their full range of capabilities.
Contain an element of open-endedness
HL assessments would benefit from an element of open-endedness. Open-ended tasks allow students to demonstrate understanding and creativity (Fan et al., 2022) and develop children’s critical thinking skills (Sarwanto et al., 2021). Open-ended tasks are unstructured tasks that have no predefined steps or goals that can be precisely defined in advance (Pehkonen, 1995). Open-ended tasks allow children to demonstrate their understanding in a manner that is contextually and developmentally appropriate for them.
Example assessment
An example of an assessment task that adheres to the above characteristics for year 5 and 6 students (aged 10–12 years) in Australia is to ask children to design a healthy pizza recipe and compare it to a pizza from a local shop. Students are required to specifically consider differences in nutritional value using a range of reputable sources (including the Australian Dietary Guidelines) to support their suggestions. This assessment has a variety of links to the Australian year 5/6 curriculum (see online supplemental file 2). The activity is also relevant to the child and their context, can be integrated with other areas of the curriculum, allows students to demonstrate a wide range of HL levels and has elements of open-endedness. Online supplemental file 3 provides an example student artefact in response to this task.
Analysis – Assessing sub-components of HL using the health curriculum
When learning is best indicated by performance (i.e. things students make, do, say or write), rubrics have been shown to be the most effective approach to assess learning outcomes (Brookhart, 2013). As HL specifically relates to social and cognitive skills (i.e. something that would be demonstrated through performance) (WHO, 2014), a rubric may provide an appropriate tool to measure HL development. Rubrics indicate ‘a coherent set of criteria for students’ work that includes descriptions of levels of performance quality’ (Brookhart, 2013: 4) while providing structure to observations.
Unlike holistic rubrics that assess all criteria together, analytic rubrics assess each criterion separately and may prove useful for assessing the multidimensional construct of HL (Brookhart, 2018). Although holistic rubrics are quicker to implement, analytic rubrics have been shown to be better for teacher instruction, formative assessment and clear communication to students about their areas of strengths and areas for improvement (Sadler, 2009). Important elements within each HL analytic rubric would be rating scales, criteria and performance descriptors.
Rating scales
Rating scales for an HL assessment need to relate to the level of HL achieved, remain constant across all HL assessments and be underpinned by a taxonomy. Taxonomies can facilitate assessment of open-ended tasks (Krathwohl et al., 2001). Two taxonomies previously discussed are Bloom’s Revised Taxonomy of Educational Objectives (Krathwohl et al., 2001) and Nutbeam’s (2000) levels of HL (Figure 1). These two taxonomies could be combined to form rating scales in an HL assessment. Combining Bloom’s and Nutbeam’s taxonomies when creating rating scales is useful for several reasons. First, doing so allows for a wide range of levels, facilitating a more precise measure because individuals are classified in groups specific to and indicative of their capabilities. Second, the amount of research done on Bloom’s taxonomy is significant and there are examples available that can be used to support the development of the performance descriptors (Eber and Parker, 2007). Third, unlike HL concepts (Otten et al., 2023), Bloom’s taxonomy is reasonably well understood in many educational settings (Seaman, 2012). As familiarity and confidence are positively associated (Chang et al., 2021), teachers may be better equipped and more likely to use this rubric if it contains familiar concepts.
Some students may not demonstrate HL skills during HL assessment. For instance, when asked to complete the example assessment about designing a healthy pizza, a student could provide an inappropriate response (e.g. they might draw a picture of a bird instead of a pizza with no explanation). Thus, it could be suggested that they have not demonstrated functional HL skills. Therefore, seven performance ratings could be used in each HL rubric: learning to remember, remembering, understanding, applying, analysing, evaluating and creating.
Assessment criteria
Assessment criteria can be assessed against the performance ratings. Assessment criteria describe expectations for standards of work (Bearman and Ajjawi, 2021). The criteria should be chosen based on the most appropriate components of what is being assessed (Brookhart, 2013). In HL assessments, the criteria would be best constructively aligned to the learning outcomes identified in HE curricula (Biggs and Tang, 2011). As HE curricula differ, the criteria used for HL assessments will also change. There are, however, many key characteristics that should remain common to each criterion. Criteria should be appropriate, definable, observable, distinct from one another (so as to be observed separately), complete (describe all learning outcomes fully when considered together) and able to support descriptions along a continuum of quality (described over a range of performance levels) (Brookhart, 2013). Importantly, each criterion should also describe qualities that demonstrate evidence of learning, rather than the characteristics of the task itself (Bearman and Ajjawi, 2021).
Performance descriptors
Performance descriptors explain each of the rating scale levels for every criterion. The descriptors are most useful when they are explicit and clearly written to describe what could be observed from the work (Brookhart, 2013). Evaluative language should be avoided (e.g. excellent, poor) to decrease the subjectivity of the rating (Brookhart, 2013). Furthermore, to support a strengths-based approach to education (Lopez and Louis, 2009), it is important that descriptors are written using positively framed language. Like criteria, in an HL assessment, performance descriptors will differ depending on the curriculum used to guide assessments, as well as the assessment task created to conduct the assessment. A wide range of verb lists 1 are aligned with Bloom’s taxonomy. These could be aligned with the rating scales in HL rubrics and used to guide the creation of performance descriptors.
Analytic rubrics are appropriate measures to record HL development. Each rubric could contain seven performance ratings (in increasing difficulty from learning to remember, remember, understand, apply, analyse, evaluate, and create) that remain consistent across HL assessments. The criteria and performance descriptors for each assessment may differ according to the assessment task. An example of a rubric that could be used to assess the previously mentioned pizza activity is provided in Figure 2.
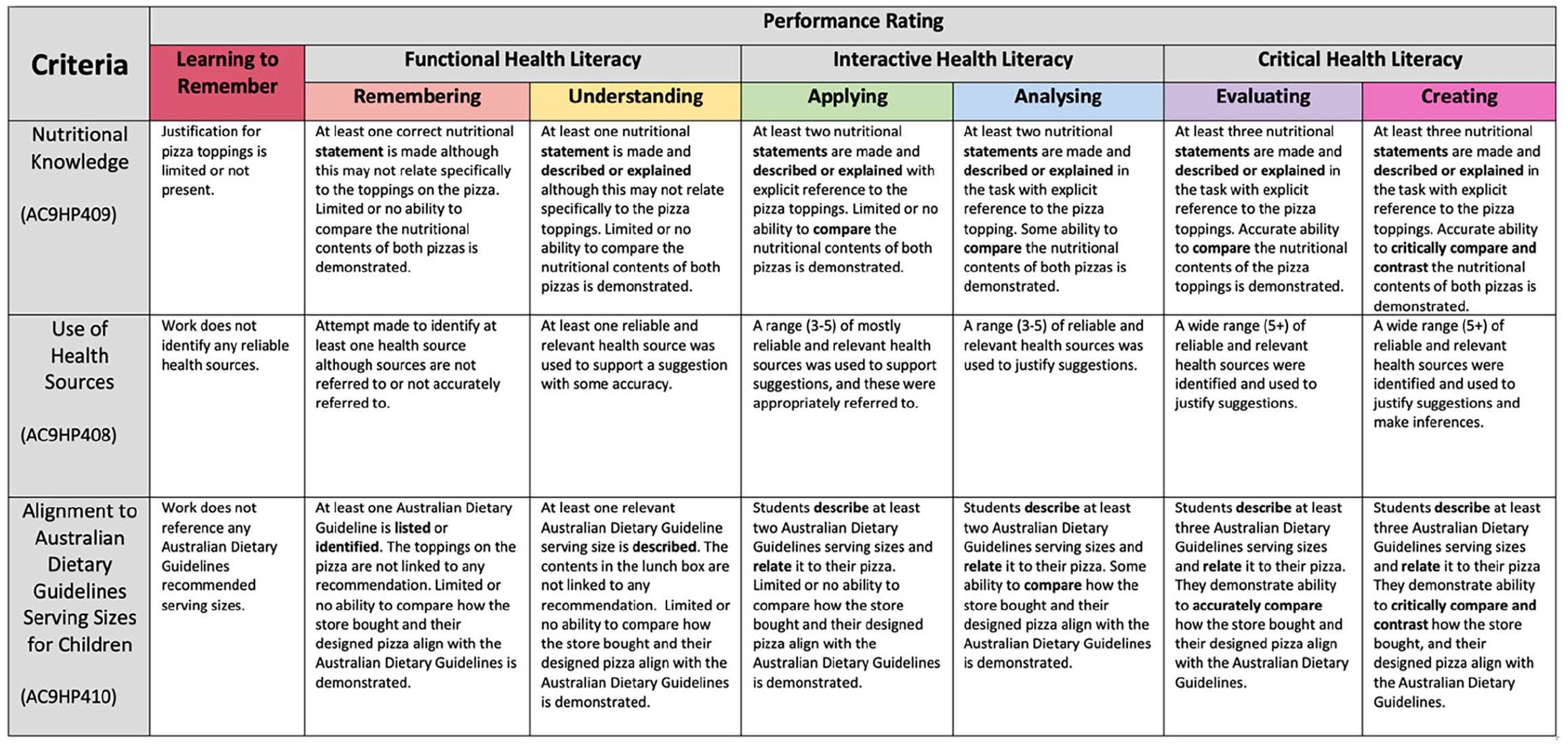
Example rubric: making healthy and safe choices year 5/6.
Analysis – Assessing student achievement against the entire health curriculum to develop an HL profile
HL achievement can be measured by appraising completed HL assessments against taxonomy-derived HL rubrics. An example of how the healthy pizza task might be analysed against the example rubric is provided in online supplemental file 4. Individual tasks can serve as formative assessments and can be used to indicate areas of strength and areas for improvement. However, as discussed previously, due to the multifaceted nature of health (Baum, 2015), one assessment cannot accurately or comprehensively reflect an individual’s HL. A child’s overall HL profile could be determined through several HL assessment tasks linked to a wide range of components of the relevant health curriculum. This facilitates tailored teaching and learning because it allows educators to identify where support and intervention is required by individuals (e.g. in finding and using reliable health sources).
Interpretation of HL data
Once HL measures have been established, they could be evaluated against expected achievement standards. This process can indicate whether students are functioning below, at or above the expected level of HL for their age and context. Given that HL is a desired outcome of HE (Nutbeam, 2009), one approach to HL evaluation could be to compare student progress to the achievement standards described in different HE curricula. This is practical because health achievement standards are already established in a range of curricula internationally (ACARA, 2022; Education Scotland, 2022; Ministry of Education, 2022). Consequently, they are ready to implement immediately and may be easier to use than an unfamiliar approach (Barwood et al., 2017). The Australian Curriculum, for example, describes the expected health skills for varying year levels in the Health and Physical Education achievement standards (ACARA, 2022). The curriculum also provides work samples that demonstrate differing levels of attainment in relation to achievement standards (e.g. below standard, above standard).
While comparing student achievement to expected achievement standards provides a contextually appropriate way to evaluate HL, the validity of this approach is dependent on the strength of each HE curriculum. For example, curricula that accurately describe the skills needed to be health literate in the environment in which these skills are intended to be enacted may facilitate a comprehensive HL assessment process. However, if HL assessments are undertaken using HE curricula that do not include all the necessary skills to be health literate (e.g. because they exclude skills related to mental health), then the assessments are unlikely to support comprehensive HL profiles of children. Furthermore, in some countries, health may not be a key component of the curriculum, rendering this approach to assessment less relevant. Although assessing different curricula for their ability to support HL development and assessment is beyond the scope of this paper, it is a critically important area for future research.
Study strengths and limitations
A curricular approach is more appropriate than existing approaches to children’s HL measurement for three reasons. First, unlike existing measures, this approach is comprehensive because it measures a broad range of HL skills. Second, it considers the child’s context and their development stage. Finally, it measures HL as demonstrated by children, rather than self-reported or observer-perceived HL. Therefore, a curricular approach is more likely to be a valid indicator of a child’s HL.
However, implementing such an approach does have practical challenges. For instance, as many teachers lack confidence teaching about health (Otten et al., 2023), and find it difficult to provide opportunities for children to develop critical HL, (Peralta et al., 2021), this approach may be difficult for some teachers to implement. Furthermore, the measurement process is only as robust as each HE curriculum, as well as the teacher responsible for its delivery and assessment. Future research is required to consider the barriers and enablers to teachers teaching health and assessing HL, the strategies needed to support the development of critical HL (including citizenship) as well as an examination of the differences between HE curricula internationally.
Conclusion
This paper has outlined the basis of a framework that could be used to measure children’s HL. The framework is built on authoritative educational and HL models and suggests that the knowledge and skills required for children to be health literate within their context can be broadly described by HE curricula. HL assessments are best when they are specific to students’ context and open-ended, when measurement can be guided by a rubric (underpinned by a taxonomy), and when interpretation of the measurement is consistent with the learning intentions outlined in the curriculum from which the assessment was derived. A curricular approach to assessing HL is advanced as a comprehensive and contextually adaptive method of assessing HL in children.
Supplemental Material
sj-docx-1-hej-10.1177_00178969241246172 – Supplemental material for Assessing children’s health literacy: A curricular approach
Supplemental material, sj-docx-1-hej-10.1177_00178969241246172 for Assessing children’s health literacy: A curricular approach by Claire Otten, Nenagh Kemp, Vaughan Cruickshank, Louisa Peralta, Melanie Hawkins and Rose Nash in Health Education Journal
Supplemental Material
sj-docx-2-hej-10.1177_00178969241246172 – Supplemental material for Assessing children’s health literacy: A curricular approach
Supplemental material, sj-docx-2-hej-10.1177_00178969241246172 for Assessing children’s health literacy: A curricular approach by Claire Otten, Nenagh Kemp, Vaughan Cruickshank, Louisa Peralta, Melanie Hawkins and Rose Nash in Health Education Journal
Supplemental Material
sj-docx-3-hej-10.1177_00178969241246172 – Supplemental material for Assessing children’s health literacy: A curricular approach
Supplemental material, sj-docx-3-hej-10.1177_00178969241246172 for Assessing children’s health literacy: A curricular approach by Claire Otten, Nenagh Kemp, Vaughan Cruickshank, Louisa Peralta, Melanie Hawkins and Rose Nash in Health Education Journal
Supplemental Material
sj-docx-4-hej-10.1177_00178969241246172 – Supplemental material for Assessing children’s health literacy: A curricular approach
Supplemental material, sj-docx-4-hej-10.1177_00178969241246172 for Assessing children’s health literacy: A curricular approach by Claire Otten, Nenagh Kemp, Vaughan Cruickshank, Louisa Peralta, Melanie Hawkins and Rose Nash in Health Education Journal
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.O. was supported by an Australian Government Research Training Program (RTP) Scholarship.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.