
Abstract
Objective:
To design and evaluate an education and training programme for community homecare workers to deliver falls prevention programmes to older homecare clients.
Design:
Mixed methods design.
Setting:
Community homecare organisation.
Method:
A series of role-based training workshops using a Train the Trainer model were designed using a blended learning approach and conducted with allied health professional, community therapy assistant and support worker staff groups. Training was systematically evaluated using the New World Kirkpatrick model Levels 1 to 3 which measured staff reactions to training, training impact on staff learning, and learning translation into workplace practice. Staff surveys, performance-based assessment in the workplace, email/meeting records and field notes were utilised. Quantitative data were analysed using descriptive statistics and Wilcoxon signed-rank tests; qualitative data were subjected to deductive content analysis.
Results:
Five allied health professionals, 14 therapy assistants and five support workers rated the training workshops as engaging and relevant. Allied health professionals felt confident and motivated to train therapy assistant and support worker groups. Therapy assistants and support workers made significant self-rated falls knowledge gains (p ⩽ 0.01), and more than half achieved competency in performing seven of the nine critical behaviours identified for delivering the 12-week falls prevention programmes in the workplace, such as coaching, correct exercise delivery and educating clients on safety at Week 6. The introduction of workplace support visits was a key driver for facilitating competency and ongoing learning. Areas identified for improvement included consolidating skills to motivate client participation, strengthening the ability to link clients’ programmes to clients’ goals and fostering a more proactive culture of problem-solving and feedback.
Conclusion:
Evaluation showed education and training for community homecare workers to deliver falls prevention programmes to homecare clients was relevant, acceptable and improved self-rated knowledge. Learning was translated to the workplace and skills for improvement were identified for future training workshops.
Introduction
Older, frail people receiving care support in the home are at high risk of falls injuries that can lead to functional decline and costly admissions to hospital and residential aged care (Burton et al., 2018b; Tricco et al., 2017). Falls prevention programmes can assist older people to mitigate their falls risks but accessing such programmes can be challenging (van der Velde et al., 2022). A recent Australian government initiative has called for homecare services to do more to provide community dwelling older people with innovative high-quality programmes, such as falls prevention, to remain independent and safe at home (Australian Government Department of Health and Aged Care, 2022).
In Australia, community homecare refers to a range of government-subsidised services available to older people with more complex care needs living at home to maintain their independence and wellbeing. Services can include nursing care, therapy, domestic assistance and social support (Australian Government Department of Health and Aged Care, 2023). Falls prevention programmes are not routinely available but can be integrated within existing homecare services. Community homecare organisations currently employ a range of staff to deliver programmes to older people at home. Allied health professionals (AHPs), such as physiotherapists and occupational therapists are university qualified practitioners who provide the therapy services including assessment, treatment and evaluation of homecare clients and the supervision of community therapy assistants (CTAs, in community settings), known also as therapy assistants or allied health assistants (Government of Western Australia North Metropolitan Health Service, 2022). CTA staff assist clients with clinical and therapeutic programme-related activities such as exercises and gait practice, within their employer organisation’s guidelines under the supervision of an AHP (Lizarondo et al., 2010). Community support workers (CSWs), also known as certified assistants or support workers, assist clients with activities of daily living, domestic assistance and social support within their employer organisation’s guidelines under the supervision of nonclinical service co-ordinators with access to registered nurses as required (Burton et al., 2018a).
Most CTA and CSW have vocational-level training qualifications, that usually do not mandate falls prevention management (South Metropolitan TAFE, 2025a, 2025b) which is strongly advocated for all older adults. The feasibility for appropriately trained CTA staff to deliver falls prevention education programmes (Francis-Coad et al., 2023) and CSW staff to safely deliver falls prevention exercise programmes (Burton et al., 2018a; Walsh et al., 2023) to homecare clients has been demonstrated. Therefore, if the appropriate training was provided these staff will be better positioned to deliver high-quality, evidence-based falls prevention programmes combining tailored education and exercise.
Staff training should incorporate adult learning principles and be sustainable for homecare organisations to deliver, in the context of regulatory requirements and high staff turnover (Gandhi et al., 2021). A Train the Trainer (TTT) model has the potential to deliver a time-saving sustainable training option. This model describes training in which key staff in a workplace receive training on a specified programme and instruction on how to train, supervise and monitor other staff in delivering such a programme to the intended recipients (Pearce et al., 2012). TTT models have been used in the dissemination of information to health care workers, with the best outcomes achieved when designed and implemented using a blended learning approach. This approach integrates multiple instructional methods, including interactive face-to-face sessions and supplementary electronic or written learning resources (Pearce et al., 2012). Importantly, the effectiveness and efficiency of such training must be systematically evaluated to ensure its impact and potential for sustainability.
The New World Kirkpatrick Model provides a comprehensive framework to systematically evaluate training including participants’ reaction to training, learning from training, translation of learning into the workplace, and workplace outcomes (Liao and Hsu, 2019). To our knowledge no training for community homecare staff delivering falls prevention programmes to homecare clients have been comprehensively evaluated. Therefore, the aim of the study was to design and evaluate education and training for community homecare staff to deliver falls prevention programmes to older homecare clients.
Methods
Study design
Mixed methods design using surveys, online emails/meetings, performance-based assessment and field notes (Creswell and Plano Clark, 2017). This study reports on phase one (staff training) of a two-phase effectiveness-implementation trial (TrEdEx project) that partnered university researchers with a community homecare organisation to enable older adults to remain safe and mobile at home (Francis-Coad et al., 2024). The study was reported in accordance with the quality of mixed methods studies in health services research (O’Cathain et al., 2008) (see online Supplementary file 1a).
Ethical considerations
Ethical approval for the study was received from the University of Western Australia Human Research Ethics Committee (2023/ET000763) and the participating organisation’s executive directorate. All participants provided written informed consent to participate in the study.
Participants and setting
AHP, CTA and CSW staff from a large not-for-profit homecare organisation in metropolitan Perth, Western Australia participated in training. Eligibility criteria for staff were aged 18 years and above; able to communicate in English; and employed by the organisation for a minimum of 1 month. The organisation concerned provides services including home support (e.g. personal care and cleaning), clinical support (Nursing, Allied health), and social support (companionship, shopping, transport). All training took place at the organisation’s central training centre, which included a home simulation area, during April and May 2024. Participating staff were allocated additional paid time to participate in the training and to deliver the falls prevention programme to clients.
Training design
Three discipline-specific (AHP, CTA and CSW) training workshops were designed by the university research team addressing best practice in health care based on prior work (Francis-Coad et al., 2022, 2023), the current World Guidelines for Falls Prevention and Management for Older Adults (Montero-Odasso et al., 2022) and adult learning principles (Merriam et al., 2006). Adult learning opportunities in this context need to be applicable to current roles (staff) and personal situation (clients) and acknowledge their life experiences and knowledge. Our learning design incorporated relevant real-life applications and shared experiences though interactive discussions, role-play and case-based simulations to increase staff engagement, understanding and retention and foster knowledge application with clients (Merriam et al., 2006). A TTT model embedding a blended learning approach was utilised and topics included (Pearce et al., 2012):
Adult learning principles.
Preparation for training delivery.
Facilitating training.
Falls and fall prevention.
Goal setting and action planning.
Role-play and simulation.
Coaching and motivation skills.
Evidence-based falls risk factor awareness and prevention management.
Exercise delivery.
Problem-solving.
Evaluation and review.
All workshops comprised modelling of skills and formative feedback by the master trainers who were qualified (⩾20 years) gerontological physiotherapists, falls prevention researchers and university academic/clinical educators. This experiential profile meant they were well suited to designing and delivering falls prevention training for adult learners working with older clients. Older adult volunteers recruited by telephone from the organisation’s pool of consumer representatives within their retirement village acted as model clients. A descriptive overview of a training workshop is provided in online Supplementary file 1b. Custom training resources were designed to support learning and included a short video and support materials in paper and electronic format.
Data collection and procedure
The application of the TTT model is presented in Figure 1. The organisation designated AHP staff to be trained as programme trainers based on role capacity. The training was delivered as a 3-hour in-person workshop by the master trainers. Subsequently, CTA and CSW staff (trainees) nominated by the organisation were invited to participate based on role capacity. CTA trainees received a 3-hour in-person workshop and CSW staff received a 4-hour in-person workshop. CSW trainees had an additional hour for learning therapeutic skills, that is, assisting clients with a specific range of strength and balance exercises that were new to their role. All trainees had undertaken prior training in identifying safety risks and reporting changes in their client’s condition as part of the organisation’s induction policy. All trainee workshops included education on understanding the scope of their role, clear pathways for reporting any concerns regarding client safety, deterioration or improvement requiring programme review (see online Supplementary file 1b). For the duration of the study, all CSW trainees were under the supervision of an AHP while assisting with delegated falls prevention programmes.
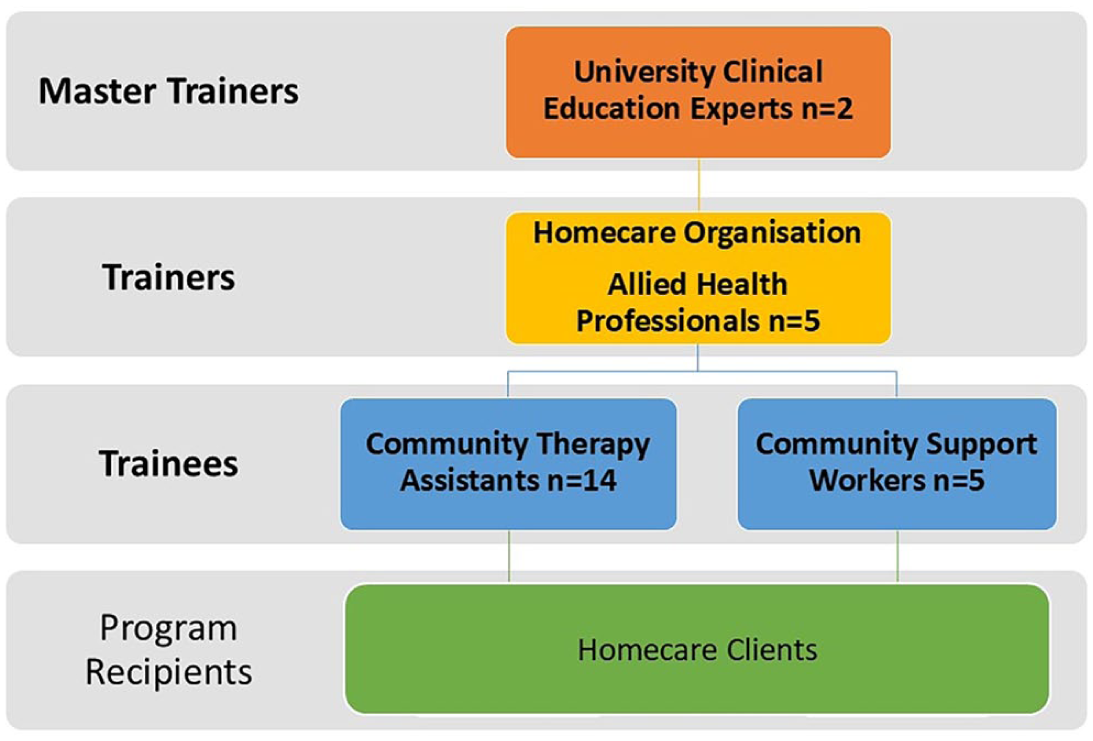
Train the trainer model.
The New World Kirkpatrick framework Levels 1 to 3 were used to evaluate training. Level 1 rated staff’ reactions to the training provided; Level 2 measured the impact of training on staff’ learning; and Level 3 evaluated whether learning from training was translated into workplace practice (Heydari et al., 2019). Training workshops were evaluated using a survey containing closed-response items measured with a Likert-type scale (Hartley, 2014) that included self-assessment and open-responses (see online Supplementary file 1c). We also chose self-assessment as it is used to develop the skills of reflective practice and self-monitoring. These skills are required in the homecare context as CTA and CSW staff are visiting clients in their homes without direct supervision from AHP staff and thus need to be aware of their own limits and learning requirements.
Demographic information was collected at baseline. Self-rated trainer (AHP) knowledge on learning design, coaching and motivation, promoting learner engagement and skills was measured pre- and posttraining. Self-rated trainee (CTA/CSW) knowledge on falls and falls prevention management and coaching and motivation was measured pre- and post-training. On completion of the training workshop staff rated their satisfaction, motivation and confidence with training (Level 1). Perceived barriers and enablers to training and delivering the falls prevention programme effectively were explored by means of open-ended survey items. All trainers and trainees were provided with support materials for learning (see online Supplementary file 1b). The self-assessment of trainee knowledge directly following the training workshops (Level 2) provided the trainers with information as to where gaps in learning remained and trainees could be guided towards revising this knowledge from the learning resources provided.
Briefly, the falls prevention programme was a new 12-week service offered to the organisation’s existing homecare client list meeting the selection criteria (aged 65 years, able to communicate in English and provide informed consent), which was implemented in addition to their usual care. The programme consisted of education on intrinsic (e.g. visual impairment) and extrinsic (e.g. hazards in the home) falls risk factors and strategies for mitigation, combined with lower limb strength and balance exercises. CTA/CSW trainees were allocated to clients based on their role capacity and geographical region of work. The CTA and CSW trainees then delivered the falls prevention programmes weekly (for 12 weeks) to homecare clients. During this period, the master trainers provided workplace support visits, which included an initial (Week 1) support visit and two additional support visits for CSW staff to facilitate programme fidelity and safety, with a single support visit for CTA staff. Master trainers made field notes on their reflections post visit. The trainers provided weekly support emails to the trainees to which they could respond with any learning or programme-related queries. The master trainers also provided online monthly support meetings, weekly emails or video calls for the trainers to problem solve any issues that might arise from trainees when delivering the programme to clients.
The master trainers observed and assessed all CTA and CSW trainees in the workplace at Week 6 to determine if learning from the training had been translated into practice (Level 3). Performance-based assessment was chosen as this type of evaluation focusses on the practical application of knowledge and skills in a real-world context (Myers, 2021). The performance-based assessment tool was developed from previous published work (Francis-Coad et al., 2022; Francis-Coad and Hill, 2014) and identified critical behaviours for delivering the falls prevention programme to homecare clients mapped to topics presented in training. For example, the topic of client programme ‘evaluation and review’ was assessed by observing if the trainee provided feedback to the client on the performance of their exercises and notified trainers, if required, whether the programme should be progressed or regressed. Trainee performance of critical behaviours for delivering the programme to clients was deemed ‘competent’ if ⩽2 prompts were required to achieve the behaviour, or ‘moving towards competency’ if >2 prompts were required.
Data analysis
Quantitative
Quantitative survey data (levels of knowledge pre- and posttraining workshop, confidence, motivation post-training workshop) and 6-week performance-based assessment findings were entered into Microsoft Excel spreadsheets (Microsoft 365) and analysed using SPSS version 29 statistical software package (IBM SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarise the main quantitative findings. Differences in staff knowledge pre- and postreceiving training were examined using a nonparametric alternative Wilcoxon signed-srank test as the data were not normally distributed. Statistical significance was set at p < 0.05 for all analyses (two-sided).
Qualitative
Qualitative responses from open text items in the staff surveys, emails/meeting minutes and field notes were managed using NVivo software (QSR International Pty Ltd., Version 12, 2018) and read multiple times by the researchers (JFC, JAH) for familiarity. Deductive content analysis was chosen as the analysis was structured around pre-defined categories that were previously known (Elo and Kyngäs, 2008). Staff responses to training were mapped to the New World Kirkpatrick Model by constructing a category matrix using the criteria describing ‘Reaction to’, and ‘Learning from’ training (Heydari et al., 2019; Kirkpatrick and Kirkpatrick, 2016). Master trainer field notes were mapped to critical behaviours (specific programme actions performed consistently on the job that will impact client outcomes) and required drivers (processes that monitor and encourage performance of critical behaviours on the job) (Kirkpatrick and Kirkpatrick, 2016).
Results
Staff characteristics
Twenty-four staff were trained using the TTT model (see online Supplementary file 1d). Briefly, four physiotherapists and one occupational therapist (median age 31 years, and 8 years of experience working with homecare clients) were trained to become ‘trainers’. Fourteen CTA and five CSW (trainees) were trained to deliver the falls prevention programme to participating homecare clients. The median age of the CTA trainee was 31.5 years and the CSW trainee 38.0 years, with the median number of years experienced working with homecare clients being 1 year (CTA) and 2 and a quarter years (CSW), respectively.
What were the staff’ reactions to training? (Kirkpatrick Level 1)
Survey results showed that all AHP trainers, CTA and CSW trainees reported high levels of satisfaction with the training venue, resources, presenters, and overall quality of training (see Supplementary file 1e). The majority found the information presented engaging and relevant to their needs, with AHP (100%) trainers and CSW (100%) trainees being very satisfied, while CTA trainees expressed either satisfaction (28.6%) or high satisfaction (71.4%). Step-by-step guidance, practical demonstrations (by master trainers) and role-playing real-world case scenarios with older adult models were particularly appreciated for aiding in programme delivery, learning motivational interview (MI) techniques (collaborative conversation style for strengthening a client’s own motivation and commitment to change their behaviour to benefit their health) (Rollnick et al., 2022) and actioning falls prevention strategies. Participants also valued receiving clear instructions, videos, and take-home resources for reinforcing learning. Across all groups, training duration was rated appropriate.
Did training impact staff’ learning? (Kirkpatrick Level 2)
AHP trainers felt their self-rated knowledge in designing training, promoting learner engagement and skill acquisition had improved following training, however, only coaching and motivating health behaviour change showed significant improvement (p = 0.038) (see online Supplementary file 1f). Trainer confidence (Agree n = 4, Strongly Agree n = 1) and motivation (Agree n = 2, Strongly Agree n = 3) to deliver falls prevention training to CTA and CSW trainees were rated highly following training (see online Supplementary file 1e).
Trainees (CTA/CSW) reported significant self-rated knowledge gains on all aspects of falls risks and falls prevention strategies following training (Table 1). Motivational interviewing (MI) and delivering education were identified as new learning concepts; trainees reflected that learning was facilitated by having different options to assist them when role-playing client case-studies. For example, two levels of motivational interview scripts were offered during practice that had either more or fewer conversational prompts. Having annotated copies of the safety message cards and MI tips resource to refer to was viewed as an enabler for delivering the education part of the programme to clients. CSW trainees also felt they had benefitted from learning how to correctly teach exercise techniques from both a personal and client-related perspective. The detailed weekly guide resource explaining sequential actions for delivering the programme was noted as a learning facilitator, noting that it was easy to read and follow. A noteworthy barrier reported was not having more opportunity to practise new skills, with trainees suggesting refresher training sessions to help consolidate learning. All trainees either agreed (n = 8, 42.1%) or strongly agreed (n = 11, 57.9%) they felt confident to deliver the falls prevention programme to homecare clients, and either agreed (n = 5, 26.3%) or strongly agreed (n = 14, 73.7%) they felt motivated to deliver the falls prevention programme to homecare clients following training. However, all were reassured knowing that master trainer support visits would be scheduled at regular intervals.
Trainee changes in pre- and posttraining falls knowledge.
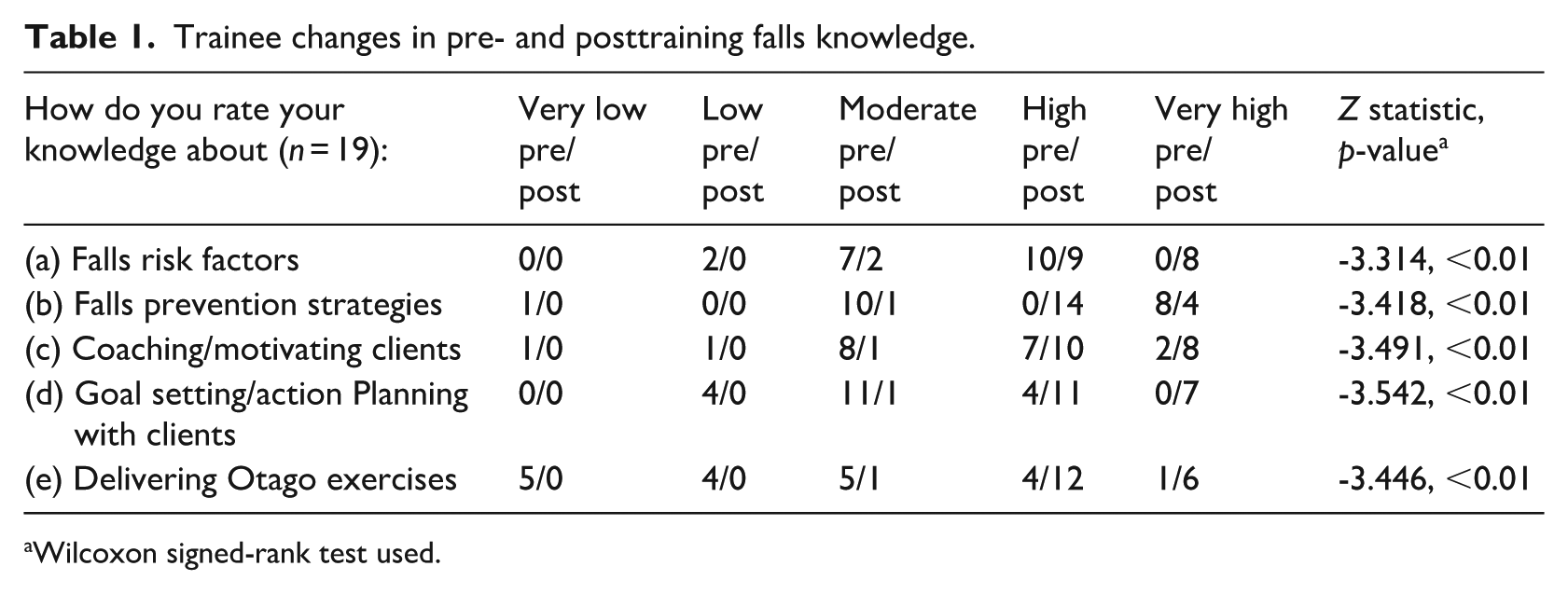
Wilcoxon signed-rank test used.
AHP trainers’ perspectives on training CTA and CSW staff
The AHP trainers perceived that there was a diverse range of knowledge, experience and skills among the CTA and CSW trainees. A potential barrier to programme delivery raised by AHP trainers was the fact that new concepts, such as CSW trainees delivering prescribed exercises to clients, might need further consolidation. To mitigate this, the master trainers implemented additional workplace support sessions (up to three per trainee) for CSW trainees to consolidate newly learned skills. In contrast, prior certified vocational education and training and work experience delivering exercise programmes to clients was seen as an enabler for CTA trainees in delivering the programme to clients.
Was training translated into practice? (Kirkpatrick Level 3)
Master trainers’ support visit observations and workplace assessment
Master trainers provided 31 support visits to CTA (one visit per trainee) and CSW (three visits per trainee) trainees in the workplace corroborated by 20 support emails from AHP trainers. All CSW and most CTA trainees commented that the support visits were helpful to acknowledge and validate what they were doing well, provide encouragement and reinforce their performance of the critical behaviours covered in training, but email support was underutilised. Master trainer formative feedback on what skills could be improved motivated trainees to apply what they had reviewed in the support visit and take responsibility for their continued learning. Sixteen trainees completed a workplace assessment at Week 6, as three trainees had ceased employment with the organisation (see Table 2).
Evaluation of CTA and CSW trainees’ critical behaviours for delivering the falls prevention programme to clients.
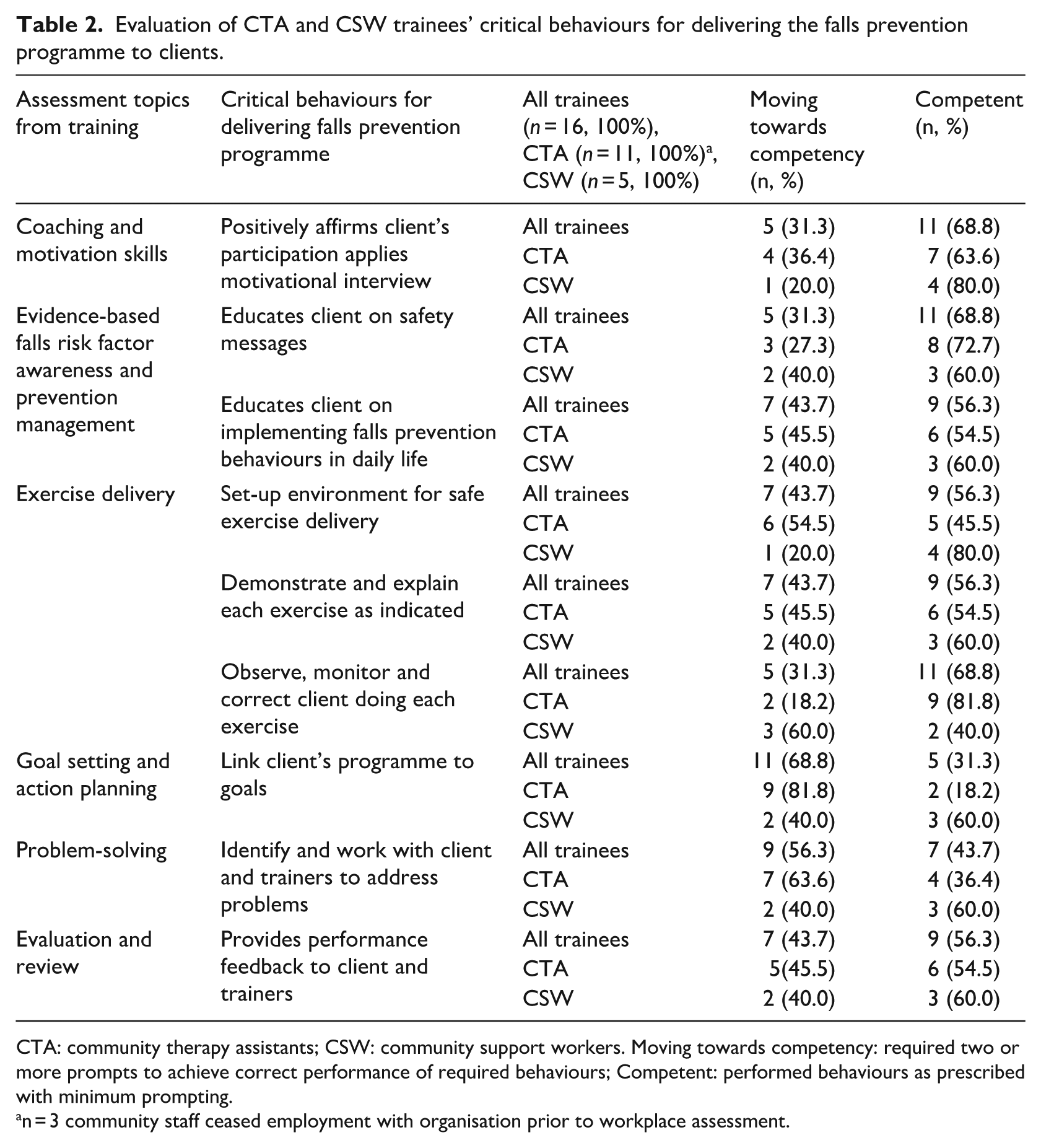
CTA: community therapy assistants; CSW: community support workers. Moving towards competency: required two or more prompts to achieve correct performance of required behaviours; Competent: performed behaviours as prescribed with minimum prompting.
n = 3 community staff ceased employment with organisation prior to workplace assessment.
Coaches and motivates client
Eleven (68.8%) trainees achieved competence in coaching and motivating clients to support and encourage programme participation, with coaching particularly well executed. For example, one CSW provided positive reinforcement to their client after needing to correct their balance exercise technique, and a CTA provided reassurance to their client when coaching their leg exercises by explaining that performing the exercises would help reduce his osteoarthritic knee pain. However, Master trainers identified an area of challenge in trainee ability to motivate clients to overcome exercise participation barriers, noting there were missed opportunities to apply MI skills covered in training. Trainees tended to use didactic delivery approaches, that is, talking at the client, which was often ineffective in overcoming client barriers to participation, rather than engaging with the client in conversation to understand and support them in making a positive change.
Educates client on evidence-based falls risk factor awareness and prevention management
Delivering falls prevention education using prescribed safety messages to raise awareness of personal falls risk was performed competently by 11 (68.8%) trainees and educating clients on implementing their prescribed falls prevention strategies in daily life was competently accomplished by nine (56.3%) trainees. An exemplary performance by one CSW trainee utilised the annotated safety message cards during the client education session. The trainee checked for client understanding of dehydration risk and barriers and enablers for improving their hydration, resulting in an agreed action plan of having a water bottle to hand while seated in the lounge room, which was actioned immediately.
Delivers prescribed client exercises effectively, facilitates client goals and actions
CTA and CSW trainees needed some master trainer assistance to ensure effective exercise delivery. Nine (56.3%) trainees set up for safe exercise delivery and demonstrated and explained each exercise to their client competently. Eleven (68.8%) trainees achieved competence in observing, monitoring and correcting their client’s performance. A CTA provided an exemplary performance in exercise delivery paying great attention to detail setting up a safe exercise environment, educating the client on the correct techniques, demonstrating, correcting and adapting the client’s calf strengthening exercise to include light hand-touch on the bench to assist client stability. However, only five (31.3%) trainees competently demonstrated linking their client’s programme to their client’s goals. For example, a CTA reminded their client that the balance exercises they were performing would help them feel steadier for being able to take their dog for a walk in the park.
Problem solves, evaluates and reviews client participation
Most trainees demonstrated developing competence in this behaviour with only seven (43.8%) actioning working with trainers and clients to address problems to improve programme engagement. For example, one CSW observed their client becoming fatigued during their visit when delivering their programme. Following discussion with their client, the CSW liaised with trainers and the scheduling team to alter the time of their visit, allowing for a recovery break, so that their visit didn’t immediately follow the client’s personal care assistance service. Providing regular performance feedback to clients was competently performed by nine (56.3%) trainees. A CTA determined their client’s improved performance of repetitions and sets with a 1-kg ankle weight, informing the client that their leg strength was improving. This resulted in a discussion with the trainer to have the weight increased to enable further client progress.
Discussion
The TTT model was successful in the short-term for training AHP, CTA and CSW staff to deliver falls prevention programmes to homecare clients, similar to findings reported in Nexø et al. (2024) where TTT programmes targeting nurses, social care and health care assistants proved effective in translating knowledge from trainers to trainees. We chose this model as it enabled the use of a blended learning approach comprising interactive discussion, modelling, coaching, case-based role-play and custom companion learning resources, which has been evidenced in a systematic review as the most effective way of delivering a TTT programme (Pearce et al., 2012). The partner organisation was also keen to explore this model of training as it could potentially be time-saving, encourage a culture of learning and knowledge sharing, and be sustainable in the longer term given high staff turnover in the aged care sector (Australian Government Department of Health and Aged care, 2023).
However, there is mixed evidence for the use of TTT cascade models in the literature as potential pitfalls may include: dilution of fidelity and consistency of training content across trainers and variability in trainer confidence and competence to deliver training effectively (Harper et al., 2024). To address fidelity and content consistency limitations, we incorporated a suite of online and paper-copy training resources for the organisation, while variation in trainer confidence was minimised with ongoing online support emails or video calls. Trainers and trainees were engaged and highly satisfied with the training (Level 1) which was important as engagement is a known driver for learning (Level 2). Consequently, trainees were able to apply what they had learned in the workplace (Level 3) as they perceived the training to be relevant to their needs and felt confident, motivated and committed to delivering the programme to clients (Heydari et al., 2019). High satisfaction ratings can also provide support for organisational-buy-in for the training contributing to long-term sustainability. Well-trained staff are also more likely to feel satisfied in their roles. This can improve job satisfaction and reduce turnover (Kirkpatrick and Kirkpatrick, 2016), which is beneficial for both the staff, the organisation and the clients they serve.
CTA and CSW trainees made greater knowledge gains following training whereas AHP staff, participating as trainers, reported fewer knowledge gains. This was not surprising given the scope of their professional undergraduate degree combined with their current professional role in supervising CTA staff had encompassed many of the trainer skills. All staff groups expressed unfamiliarity with motivational interviewing (MI) techniques which was reflected in the workplace with trainees tending to revert to more directive, less client-centred methods when attempting to influence client behaviour. The limited use of MI skills by trainees may have reflected the brevity of time to learn and practice this skill during training (1 hour), which highlighted a need for enhanced focus. Two studies on teaching MI skills to nurse practitioner students (Nesbitt et al., 2014) and medical students (Daeppen et al., 2012), respectively, both recommended 8 hours of training plus follow-up sessions. Future iterations of the training may benefit from additional practical application of these techniques online as funding the additional training hours face-to-face could prove cost-prohibitive for organisations. Despite these challenges AHP trainers felt that learning MI was particularly beneficial to pass on to CTA and CSW trainees for motivating client behaviour change in an empowering way, as it supports clients to take a more active role in their health and wellbeing (Biddle and Hoover, 2020).
AHP trainers had expressed concerns regarding the ability of the CSW trainees to effectively deliver the exercise component of the falls prevention programme to their clients, given their limited experience. However, CSW trainees performed better across most of the assessed critical behaviours required for delivering the exercise component of the falls prevention programme to clients compared with CTA trainees. The additional workplace support visits taken up by CSW trainees appeared to close the initial skill gap. This master trainer support structure was pivotal in translating training into real-world application, Kirkpatrick and Kirkpatrick (2016) describes this process as a ‘required driver’, that is, a process that reinforced, monitored and encouraged the performance of trainee critical behaviours in delivering the programme to clients. Similar to Walsh et al. (2023), physiotherapist support for CSWs delivering home exercise programmes was key to success. All trainees appreciated the support visits, highlighting their role in validating performance and the targeted feedback not only highlighted trainee strengths but also identified specific skills for improvement, motivating ongoing self-directed learning. This support structure could positively contribute to the organisation’s commitment to ongoing quality improvement, as organisations that reinforce training with follow-up support can achieve up to 85% knowledge translation, compared with 15% with a single event training only (Kirkpatrick and Kirkpatrick, 2016).
Actioning problem-solving strategies, evaluating client progress, and reviewing client performance emerged as developing competencies among trainees. Furthermore, the underutilisation of email-based support from trainers suggests a missed opportunity for guided reflection and skill consolidation between sessions. Opportunities exist to continue to promote feedback and a collaborative culture by the regular use of the weekly AHP trainer support email for trainees to share information about what is working well and what is not. Incorporating the topic of feedback literacy into the training workshops may assist in progressing how trainees engage with feedback so they feel confident in developing their evaluative judgements (Ajjawi et al., 2023).
Overall, the findings suggest that the training workshops led to meaningful behavioural change among CTA and CSW trainees, with the additional support mechanisms playing a crucial role in reinforcing and advancing these changes in the workplace. This has implications for addressing the problem of falls among homecare clients as delivery of evidence-based falls prevention programmes may require sustainable workplace redesign. An Australian study showed that only 27.4% of homecare clients were referred to a falls prevention programme after a fall (Burton et al., 2018b), despite evidence suggesting that individuals who were referred to falls prevention programmes had a 47% reduced likelihood of having another fall. Falls prevention programmes could be delivered to homecare clients by CTA and CSW staff with AHP support, similar to that in hospital settings where supervised allied health assistants have successfully delivered evidence-based falls prevention programmes to patients (Morris et al., 2024). This type of workplace redesign could enable more homecare clients to receive falls prevention programmes through staff cost savings.
Strengths and limitations
A key strength of this study was our evaluation of education and training at three levels, and in particular whether learning from training was translated into the workplace using an objective performance-based assessment (Kirkpatrick and Kirkpatrick, 2016). However, the study did not report on Kirkpatrick Level 4 evaluation ‘results’, in our case outcomes of the recipients of the falls prevention programmes (homecare clients) that could include functional measures, falls rates and injurious falls rates, as these data are currently being collected.
Study limitations include the small sample size (particularly AHP and CSW subgroups) and subjective self-rating assessment of pre- and posttraining knowledge measures, which may have resulted in staff overestimating or underestimating their knowledge, meaning changes in knowledge should be interpreted with caution. The collection of qualitative data during support visits may also have introduced some bias, as trainees could have altered their responses or behaviours in a supported context. This could limit the identification of errors in practice that may occur under usual conditions. However, these visits also fostered trust and openness, allowing for richer insights into real-world practices and areas for improvement.
Although we used a TTT model to deliver the training with the intention of enabling future staff training, it was beyond the scope of this study to measure if using such a model was sustainable for the organisation in the longer term.
Conclusion
Using a TTT model was acceptable in training different community homecare staff groups to deliver a falls prevention programme to older people receiving homecare services. Trainers and trainees described a positive experience; learning from training was translated to the workplace, gaps in learning were identified, and staff were provided with feedback and support to further improve their performance of critical behaviours for enabling client mobility and safety. Findings provide insights into effective training practices for community homecare organisations looking to implement falls prevention programmes.
Supplemental Material
sj-docx-1-hej-10.1177_00178969251371518 – Supplemental material for Training community homecare workers to deliver falls prevention programmes: A mixed methods evaluation
Supplemental material, sj-docx-1-hej-10.1177_00178969251371518 for Training community homecare workers to deliver falls prevention programmes: A mixed methods evaluation by Jacqueline Francis-Coad, Jo-Aine Hang, Vanessa Jessup, Leon Flicker, Christopher Etherton-Beer, Elissa Burton, Bernie Wong, Sharmila Vaz, Dan Xu and Anne-Marie Hill in Health Education Journal
Footnotes
Acknowledgements
We thank the staff and clients at Juniper community homecare who participated in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was funded by a Hospitals Contribution Fund (HCF) Translational Research Grant awarded to Jacqueline Francis-Coad from the HCF Research Trust (2022). Anne-Marie Hill was supported by an Australian National Health and Medical Research Council (NHMRC) (EL2) award (GNT1174179) and by the Royal Perth Hospital Research Foundation. Elissa Burton was supported by an NHMRC Investigator Grant (EL1) award (GNT1174739).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.