
Abstract
Objective:
Partnering with patients and staff to develop and evaluate falls prevention education could better enable patient learning and engagement. This study aimed to create a revised version of the Safe Recovery falls prevention education programme in partnership with older patients and hospital staff, to improve patient engagement in undertaking falls preventive strategies in hospital.
Design:
Two-phase sequential mixed methods participatory design.
Setting:
Hospital rehabilitation wards in Western Australia.
Method:
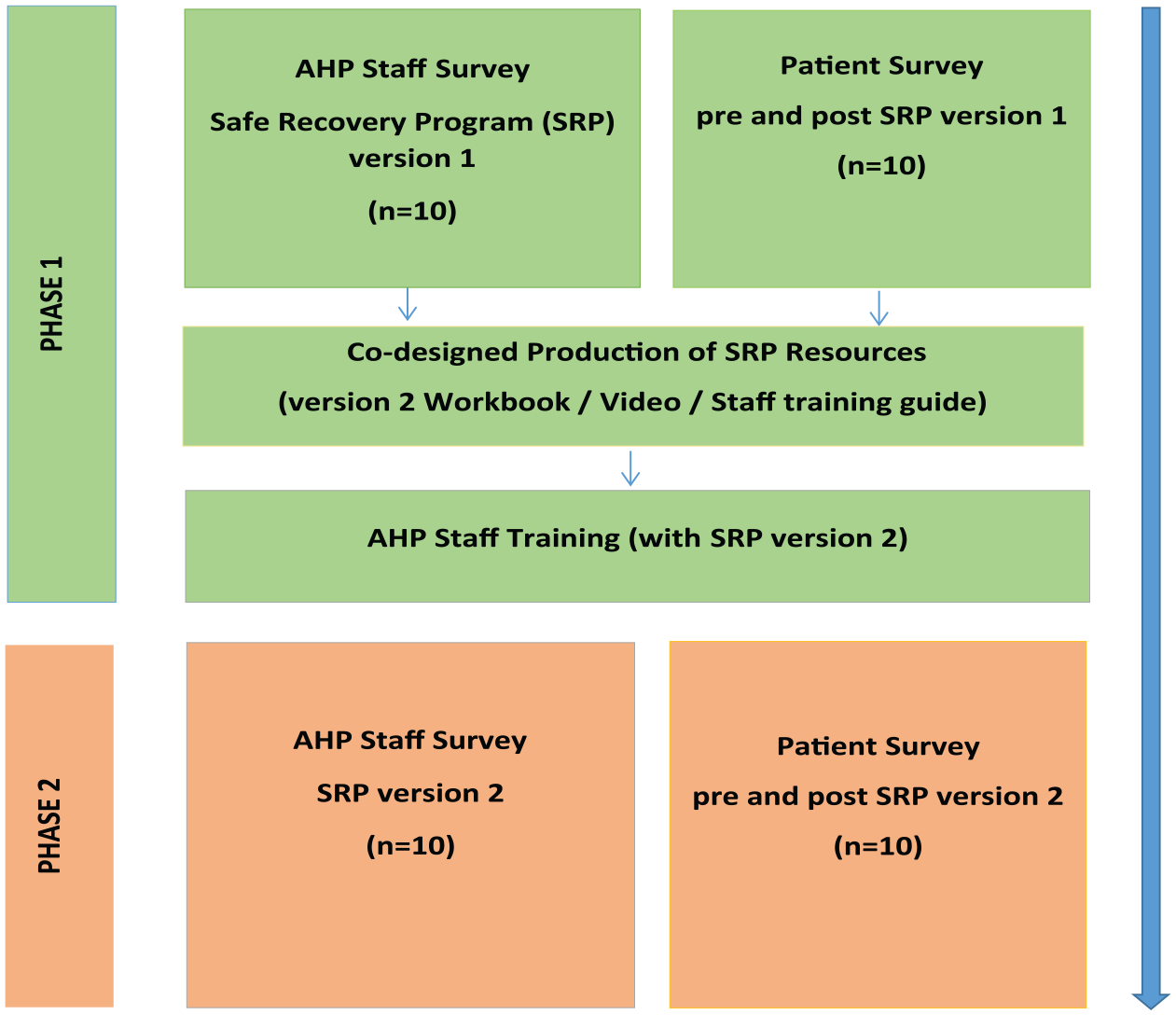
Phase 1: older patients (n = 10) and staff (n = 10) were surveyed before and after original programme delivery to ascertain their reaction and learning. Consumer-focused discussions were undertaken with staff and patients online to inform programme revision. A patient video and workbook were co-produced, and staff were trained to deliver the revised programme. Phase 2: older patients (n = 10) and staff (n = 10) were surveyed before and after receiving the revised programme to gain reactions and learning. Deductive content analysis and Wilcoxon signed-rank tests were used to analyse the qualitative and quantitative data.
Results:
Patients and staff perceived the original programme to be outdated and expressed low levels of satisfaction with the original resources. In contrast, both patients and staff were highly satisfied with the revised programme. Both original and revised Safe Recovery programme patient groups demonstrated significant improvements in knowledge and awareness to reduce their risk of falling after receiving the education (p = .008, p = .005, respectively). However, patients receiving the revised programme were significantly more likely to intend to take action (p = .024) and have a clear action plan (p = .010). Staff perceived that the revised resources showed significant improvements in aesthetic appeal (p = .007) and ability to engage patients in learning (p = .007).
Conclusion:
Patients and staff contributed to successfully revising the Safe Recovery programme with positive reactions to the co-produced resources. Participating in falls education significantly improved older patients’ knowledge and attitudes regarding falls prevention.
Introduction
Falls and injuries from falls remain the most frequently reported safety incidents in hospital inpatient settings. Approximately 30%–50% of falls in hospital result in physical injury including fractures (1%–3%) and head injuries, with negative psychological consequences and delayed functional recovery (Melin, 2018; Morello et al., 2015; Morris and O’Riordan, 2017; Zhao et al., 2019). This can increase patient length of stay and subsequently escalate hospital costs (Morello et al, 2015), therefore, preventing falls and injurious falls is a priority for all hospitals.
Falls epidemiology suggests that a discrepancy between a patient’s perceived personal falls risk and their actual level of risk contributes to patient falls in hospital (Haines et al., 2015; Hill et al., 2015a; Lee et al., 2013). Patients who misperceive their current level of function and capability as being adequate for mobilising independently, despite having impaired mobility, may undertake activities without seeking necessary staff assistance (Haines et al., 2015; Hill et al., 2015a). Older adults have also been found to possess a false sense of security when in hospital, that may lead some of them to think they are not at risk of falls (Lee et al., 2013). Some patients may also have limited understanding of how hospital falls occur and relevant falls risk factors that they should address, such as using a gait aid to compensate for poor balance (Gettens et al., 2018; Heng et al., 2021; McMahon et al., 2011). Any of these factors may result in patients engaging in mobility tasks that they are unable to complete safely, resulting in a fall (Haines et al., 2015; Hill et al., 2015a, 2016a). Unassisted falls (where patients are alone when they fall) may be preventable if patients are provided with, and adhere to, falls prevention advice. Up to 80% of falls occur when patients are alone; therefore, patient-initiated actions are a critical component of falls prevention (Staggs et al, 2014).
World falls guidelines have recently recommended that falls prevention patient education should be provided for older patients to specifically target deficits in patient awareness and comprehension of personal falls risk and provide strategies to help prevent falls in hospital (Montero-Odasso et al., 2022). A recent systematic review of interventions to reduce falls in hospitals identified that evidence-based patient education was the only intervention, from a range of common strategies examined, that was effective at reducing patient falls incidence (Morris et al., 2022). A review of falls prevention education programmes found that programmes informed by educational and behavioural change theory, which involve active learning designs, and combinations of education delivery modes are more likely to produce successful outcomes (Heng et al., 2020). In addition, new insights for developing education for older adults stress the importance of attending to human information processing, such as minimising cognitive load, to deliver effective learning outcomes (Goodman and Lambert, 2023).
The Safe Recovery programme, a hospital patient falls prevention education programme developed in Australia, has demonstrated effectiveness in reducing falls rates by 40% and falls-related injuries by 35% in a randomised controlled trial (RCT) conducted in hospital rehabilitation units (Hill et al., 2015b). Briefly, the Safe Recovery programme outlines hospital falls epidemiology, when, where, why and how falls happen, such as time of day, location, personal falls risk factors and mitigation. The programme is constructed around three simple steps to prevent falls in hospital: know if you need help, ask for help and wait for help to arrive (Haines et al., 2011). The Safe Recovery programme is delivered by trained allied health professionals, most usually physiotherapists and occupational therapists. Such staff engage in personalised discussion sessions with patients, including active learning (personalised goal setting), supported using multimedia resources (digital video disc and paper patient workbook) (Haines et al., 2011). Patients watch the video around the time of the first patient-staff discussion; the workbook is used at each session and left at the bedside for ongoing patient reference. The Safe Recovery programme is designed to be delivered in two to four individual patient sessions of between 5 and 10 minutes each, although staff are instructed to vary the interaction time according to patient needs. The Safe Recovery programme was developed through three RCTs that evaluated the efficacy of the programme in reducing falls (Haines et al., 2004, 2011; Hill et al., 2015b), with the most recent trial using a clustered ward-level approach to deliver the Safe Recovery programme alongside training and feedback to staff (Hill et al., 2015b). This meant that while physiotherapists delivered the Safe Recovery programme, nursing staff in participating wards were informed of the programme and asked to provide support for patients to undertake their planned prevention strategies (Hill et al., 2015b).
The programme resources (video and patient workbook) created in 2009 were based on findings from an initial trial which evaluated the efficacy of a multifactorial programme in reducing falls in rehabilitation wards (Haines et al., 2004). The programme significantly reduced the incidence of falls, and subgroup analysis indicated that there could be benefits for patients living with cognitive impairment, as well as for those with no cognitive impairment (Haines et al., 2004, 2006). The original Safe Recovery programme was deliberately designed to cater for people living with cognitive impairment and included very slow voice-over in the video and simple graphics in the written materials. Findings from a second Safe Recovery programme trial that evaluated the efficacy of the Safe Recovery programme for reducing falls in hospitals indicated that while there was benefit for patients living with mild levels of cognitive impairment, the programme was not effective for patients living with moderate or severe cognitive impairment (Haines et al., 2011). As a result, the later cluster trial delivered the Safe Recovery programme to patients with no or mild cognitive impairment (Hill et al., 2015b). The ward-level delivery of the Safe Recovery programme significantly reduced falls among patients in participating wards compared to control wards. Importantly, in participating wards, patients living with cognitive impairment who did not directly receive education benefitted from the reduced falls rates. This was most likely because the ward delivery impacted the safety culture, including through adaptations to the environment and changes in staff practice (Hill et al., 2015a, 2016b).
While the Safe Recovery programme was effective, technology for producing and delivering patient education has progressed and continues to evolve. Integral to this evolution is a participatory approach that engages stakeholders and consumers in the revision and evaluation of a programme (Blumenthal et al., 2013; Goodman and Lambert, 2023; Vaughn and Jacquez, 2020). This ensures the changing views and preferences of the intended beneficiaries of the programme are taken into account (Blumenthal et al., 2013; Vaughn and Jacquez, 2020). For example, a scoping review of the preferences of older adults for patient education materials reported that signposted information, logical layouts, relatable peer images and chunking information into clusters were important design elements for better accessibility, engagement and understanding. These design features can reduce demand on working memory (Goodman and Lambert, 2023) and influence patients’ learning experiences and outcomes (Kirkpatrick and Kirkpatrick, 2016). For this revision, staff with experience in delivering the Safe Recovery programme were viewed as important stakeholders, as they would be able to report their reactions to the current programme. In this study, their perspectives were sought alongside those of older patients with no or mild cognitive impairment, who were the relevant consumer group. Therefore, the aims of the study were to:
Create a revised version of the resources for the Safe Recovery falls prevention education programme with staff and patients, informed by their reactions to, and learning from, the original programme.
Evaluate staff and patient reactions to, and learning from, the revised version of the Safe Recovery programme.
Methods
Design
An exploratory sequential mixed method study (Creswell and Plano Clark, 2007) using a participatory approach was conducted in two phases between May 2021 and July 2022 (see Figure 1). Participatory approaches engendered the core philosophy of ‘inclusion’, meaning stakeholders and consumers affected by the issue being researched had valued engagement in the research process in partnership with the research team (Blumenthal et al., 2013; Cargo and Mercer, 2008). This approach has benefits for education programme design as it can help identify barriers to learning and engagement for the target population, incorporate a relevant variety of perspectives and experiences for programme tailoring, and enable iterative real-world testing and feedback for programme refinement (Cargo and Mercer, 2008; Vaughn and Jacquez, 2020).
Sequential mixed methods design.
Ethical considerations
Ethical approval for the study was received from the Human Research Ethics Committees of Ramsay Health and the University of Western Australia. All participants provided written informed consent to participate in the study.
Participants and setting
The study was conducted at a 31-bed hospital in Western Australia. The hospital provided inpatient rehabilitation services for post-surgical and general medical patients following discharge from acute care settings. Patients received the Safe Recovery programme (original version) delivered by trained Allied Health professional staff as part of usual care.
Participants were allied health professional staff and patients. Eligibility criteria for staff were being employed in an allied health professional role and the ability to communicate in English with a minimum of 3 months experience in delivering the Safe Recovery programme. In the hospital setting, the eligible allied health professionals were all either qualified physiotherapists or occupational therapists. Eligibility criteria for patients were being aged 18 years and above, being admitted for rehabilitation, and having the ability to read and communicate in English. The allied health professional manager used the hospital electronic records to obtain a purposive pilot sample that represented the age range, gender and ethnicity of the hospital population.
Phase 1 procedure
All allied health professional staff undertaking the role of Safe Recovery programme patient educators completed an online survey seeking their reactions to the Safe Recovery programme. The survey elicited staff views on patients’ engagement with the programme, how relevant the resources were for patients and patients’ learning experience (see also Table 2). Concurrently, patient participants completed a pre-programme survey to ascertain their perceptions and baseline knowledge of falls prevention in hospitals (see Online Supplemental File 1 and Table 1). All patient surveys were conducted face-to-face by a trained research assistant who recorded responses verbatim on a laptop computer.
Comparison of patients’ falls epidemiological knowledge pre and post the Safe Recovery programme.
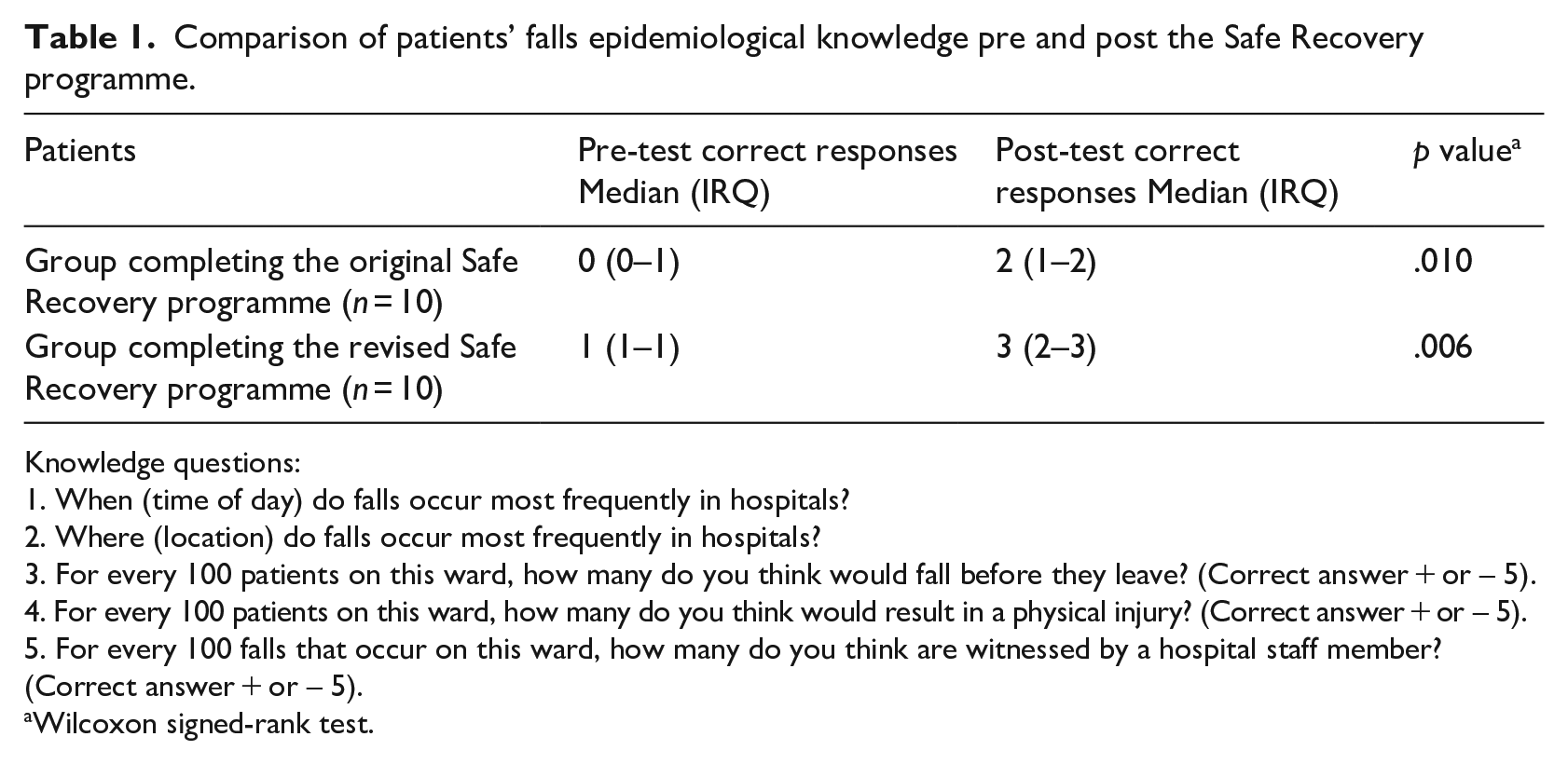
Knowledge questions:
1. When (time of day) do falls occur most frequently in hospitals?
2. Where (location) do falls occur most frequently in hospitals?
3. For every 100 patients on this ward, how many do you think would fall before they leave? (Correct answer + or – 5).
4. For every 100 patients on this ward, how many do you think would result in a physical injury? (Correct answer + or – 5).
5. For every 100 falls that occur on this ward, how many do you think are witnessed by a hospital staff member? (Correct answer + or – 5).
Wilcoxon signed-rank test.
Allied health professional staff then delivered the Safe Recovery programme to patients face-to-face within 24 hours of their admission. The original Safe Recovery programme comprised a 15-minute video played on a portable DVD player and an A4-sized paper patient workbook (in large font size, outlining hospital falls epidemiology, falls risk factors and falls prevention strategies). The content was designed to meet grade six reading level as per recommended guidelines for patient education materials (Rooney et al., 2021).
Patients were asked to review and reflect on the Safe Recovery programme before writing their personal goals in the workbook. Allied health professional staff then returned the next day to discuss goals and proposed strategies to prevent falls while in the hospital with the patient. Three to four days after receiving the Safe Recovery programme, the research assistant returned to conduct the post-programme survey to gain patients’ reactions to and learning from the programme.
Participatory approach to revise the Safe Recovery programme
A transcript of findings from the allied health professional staff and patient surveys was provided electronically to phase 1 participants for comment. All stakeholders, including two allied health professional managers, ten staff, one professional videographer, three patient actors and seven members of the research team, met iteratively, both on-site (during filming) and online using the Microsoft Teams platform (version 1.5.00.9163) during the programme revision process. This involved watching edited versions of the video and providing comments, then reading through edits of the workbook and providing comments. A subgroup of three allied health professional staff and two patients volunteered to participate in a final review of proposed Safe Recovery programme revisions, together with the research team, in which all programme resources were checked by consumers prior to production.
Allied health professional staff delivering the revised Safe Recovery programme attended a one-hour face-to-face training workshop conducted by the lead researcher (J.F.-C.). The training included the latest evidence on hospital falls prevention and instruction on how to deliver the revised Safe Recovery programme using the new resources.
Phase 2 procedure
Following the delivery of the revised Safe Recovery programme, participating allied health professional staff completed an online survey seeking their reactions to the revised programme. A second group of patients was recruited as described in phase 1 to evaluate the revised Safe Recovery programme. Those consenting completed the pre-programme survey as described in phase 1. Allied health professional staff delivered the revised Safe Recovery programme as described in phase 1 but using the new video played on a tablet and the new patient workbook. Three to four days after receiving the revised Safe Recovery programme, the research assistant returned to conduct the post-programme survey to document patients’ reactions to, and learning from, the revised programme.
Outcomes measured in phases 1 and 2
The theoretical underpinning for the evaluation was based on the first two levels of the New World Kirkpatrick Model for evaluating training programmes, which seeks to evaluate learners’ reactions to, and learning from, the training (Kirkpatrick and Kirkpatrick, 2016). The Kirkpatrick model has been used as a systematic framework to appraise training in different fields including simulation-based training (Kirkpatrick and Kirkpatrick, 2016) and medical education (Moreau, 2017). The framework together with instruments utilised in prior evaluations of the Safe Recovery programme (Haines et al., 2004, 2011; Hill et al., 2015b) guided the development of staff and patient survey instruments. Participants’ (allied health professional staff and patients) responses to both the original and the revised versions of the Safe Recovery programme were evaluated using surveys that included a mix of closed, open-ended and Likert-type scale questions. Two key outcomes were measured ‘reaction’ to the Safe Recovery programme and ‘learning’ from the Safe Recovery programme. ‘Reaction’ explored the extent to which participants reacted favourably to the programme. This included patients’ views on the programme’s ability to engage them in its content, its perceived relevance, and satisfaction with programme delivery and learning resources. ‘Learning’ on the other hand explored patients’ development of falls knowledge and perceived level of risk for falls along with levels of awareness, confidence, motivation and commitment to undertake falls prevention strategies.
Data analysis
Qualitative data
Qualitative responses from open text items in the patient and allied health professional staff surveys were read multiple times by the researchers (J.F.-C., T.W. and A.-M.H.) for familiarity and analysed with the aid of NVivo software (QSR International Pty Ltd., Version 12, 2018). Deductive content analysis was used to evaluate the Safe Recovery programme as while there existed prior knowledge regarding the research topic, a revised version of the programme was now being evaluated (Elo and Kyngäs, 2008). Allied Health professional staff and patient responses appraising the original and revised versions of the Safe Recovery programme were mapped to the New World Kirkpatrick Model by constructing a category matrix using the criteria describing ‘reaction’ to, and ‘learning’ from the programme (Kirkpatrick and Kirkpatrick, 2016). The confirmability of the qualitative findings was ensured by using verbatim participant quotes (Polit and Beck, 2013).
Quantitative data
Quantitative survey data were entered into Microsoft Excel (Microsoft Office 2019) and analysed using SPSS version 27 (IBM SPSS Inc., Chicago, IL, USA). Descriptive statistics in the form of frequencies and percentages were used to present participant demographics, patients’ responses to falls knowledge questions and Likert-type scale responses (Strongly Disagree, Disagree, Undecided, Agree and Strongly Agree). Differences between allied health professional staff reactions to the original and revised versions of the Safe Recovery programme were assessed using the Wilcoxon signed-rank test (Portney and Watkins, 2009). Differences between phase 1 patient learning before and after participation in the original Safe Recovery programme and differences between phase 2 patient learning before and after participation in the revised Safe Recovery programme were also assessed using Wilcoxon signed-rank tests (Portney and Watkins, 2009). Content from all data sources was combined in a content cloud, a type of visualisation tool for comparing and summarising information, to clarify key findings (Cidell, 2010). The study was reported on using the Guidance for Reporting Involvement of Patients and the Public (GRIPP) guidelines for reporting patient and public involvement in health and social care research (Staniszewska et al., 2017) (see Online Supplemental File 1).
Results
Participant characteristics
Allied health professional staff
Ten allied health staff undertaking the role of Safe Recovery programme educator participated. Eight of the ten participants were female, with a mean age of 31.2 years (SD ± 7.8 years). Six of the ten participants were physiotherapists, and four of the ten were occupational therapists. Six of the ten participants had 5 or more years’ professional experience, and eight of the ten had been Safe Recovery programme educators for more than 1 year.
Patients
Twenty patients participated in two independent groups of ten, the first group in phase 1 and the second group in phase 2 of the work. The key reason for patients’ admissions was rehabilitation following surgery (n = 17), with 15 having experienced one or more falls in the past 6 months. Additional patient characteristics are shown in Supplemental Table S1 (see Online Supplemental File 2).
Phase 1
Reactions to the Safe Recovery programme (original version)
Allied health professional staff
Overall, staff were somewhat dissatisfied with the original Safe Recovery programme, in particular the video and workbook resources, with one (S1) summing them up as ‘a bit basic and slightly outdated’. Primarily, staff attributed low levels of patient engagement with the video to the predominantly still photography slide format, the low-resolution images and poor audio quality. Staff also reported that the video was less engaging for patients with higher levels of cognition and normal hearing as its pace was deemed too slow (S3) ‘They [the patients] don’t feel like it relates to them at their level of function . . . they can find it quite frustrating to sit through the full-length video’. Low engagement with the workbook was attributed to the language level used. One member of allied health professional staff (S2) commented ‘the language in the video/book needs re-writing as it can seem a bit childish’.
Staff felt the idea of the Safe Recovery programme educating patients to prevent falls while in hospital was relevant, as in their experience, few patients had received personalised falls prevention education prior to admission. One reflected (S4), ‘Some patients find it very educational’. Another (S7) added that the Safe Recovery programme messages were ‘on the mark’ as they ‘encourage the patient to pro-actively reduce their risk of falling’.
Patients
Patients (P1–10) expressed low levels of satisfaction with the original Safe Recovery programme resources, particularly the video, one (P6) said ‘it was childishly done’. The slow pace and length of the video limited engagement also elicited criticism, with one patient (P2) stating ‘I think a lot of people would get half-way through this and not bother with the rest’. Delivery of the video on a small DVD player screen also inhibited engagement as it was challenging for some older people with lower levels of vision to view. One patient (P1) commented, ‘it was a small dark video . . . must be 20 years old or more, no one would be engaged by this’.
Some patients thought the A4 sized workbook was (P4) ‘too big’ to handle comfortably and one (P7) pointed out ‘there was a lot of white space’ and consequently too many pages. This reduced their desire to engage in reading in full, with one patient (P4) saying he ‘wasn’t enthused’ by it. Questions concerning programme relevance generated a mixed response. Some patients acknowledged they were at risk of falling. P9 said, ‘it did accentuate the problem of falls’. However, others did not identify with being ‘at risk’. One patient (P2) added, ‘it was informative, but it doesn’t apply to me’.
Learning from the Safe Recovery Programme (original version)
Patients
Patients’ knowledge about how and when hospital falls occur showed significant improvement following delivery of the original Safe Recovery programme (p = .010), as shown in Table 1. Patients’ awareness of the measures needed to reduce their risk of falling in hospital also showed a significant improvement (p = .008) (see Supplemental Table S2 in Supplemental File 2).
Changes to the Safe Recovery programme
The use of a professional videographer resulted in better quality lighting and images, audio integration and overall execution. The new narrative style using a content presenter in a real life setting provided a more authentic and contemporary experience. The video had been shortened to eight minutes and was delivered by means of a single click on a tablet device. The workbook was reduced to an A5-sized booklet format, and text phrases were shortened and emboldened in colour, reducing repetition and white space. New contemporary photographic images were utilised that mirrored those present in the text and video messaging. The revised workbook also included more overt instructions about goal setting.
Phase 2
Reactions to the Safe Recovery programme revised version
Allied health professional staff
Staff perceived the new resources as more contemporary, engaging and easy for patients to understand. Staff reaction ratings to the revised Safe Recovery programme showed significant improvements in the programme’s ability to utilise multimedia effectively (p = .007); easily access the video (p = .007) and workbook (p = .041); provide instructions and demonstrations that reflected clinical practice (p = .007); and explain how to prevent falls in hospital (p = .011) as shown in Table 2.
Comparison of allied health professional staff reactions to the original and revised versions of the Safe Recovery programme.
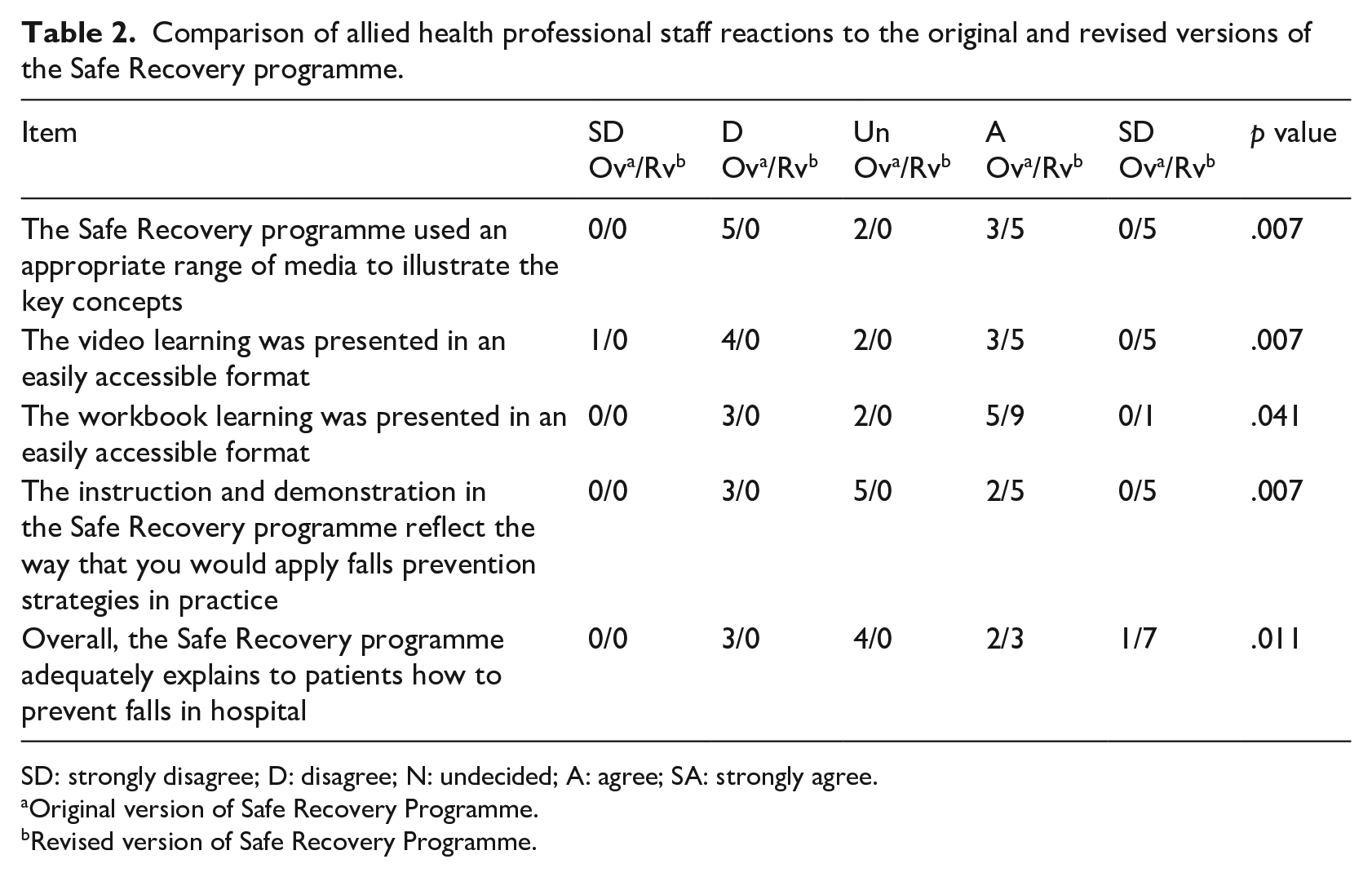
SD: strongly disagree; D: disagree; N: undecided; A: agree; SA: strongly agree.
Original version of Safe Recovery Programme.
Revised version of Safe Recovery Programme.
Perceived improved patient engagement with Safe Recovery programme resources was attributed to (S6) ‘clearer messaging’ delivery with ‘more modern content and vibrant audio’ making it more enjoyable for patients. Staff felt the new video had a better narrative structure. One staff member stated (S3) ‘the presenter talks slower but still at a speed that doesn’t make viewers feel demeaned or that their own knowledge and experience are underestimated’. Another added (S4), ‘its timely and not too long, avoiding inattention and distraction’.
The updated workbook was deemed an improvement on the original due to being smaller and less bulky. A member of staff commented (S2) ‘it’s a good size to have on a tray table’. The graphics were also thought to be sharper with good use of supporting text in bold and upper case, with one staff member (S7) validating this by saying, ‘it better emphasised points [Safe Recovery programme messages]’.
Programme relevance too was heightened. S10 said, ‘it’s absolutely appropriate to our patient population as the majority have had falls in the past or are at high risk because they are below their baseline mobility’. S3 added ‘[It has] clear instruction of when they are most at risk is valued information for any vulnerable patient’. Staff perceived patients to feel safer after participating in the revised Safe Recovery programme as they were, as one (S8) reported, ‘more aware of their risks and the strategies they can employ to reduce falls’.
Patients
Patients (P11–20) expressed high levels of satisfaction and enjoyment following participation in the revised Safe Recovery programme, one (P13) reflected, ‘It all made sense, it was easy to follow . . . there was a story there’. The programme made patients feel safer and Safe Recovery programme messages were deemed (P15) ‘sensible . . . and well reinforced using different contexts’, giving them broad appeal.
The video received very positive feedback from patients as they felt it was ‘well put together’. They found the video interesting and easy to watch, the pace was good, and it kept their attention throughout. One patient concluded (P18), ‘. . . [it’s] nice and clear and not too long, otherwise people tend to lose interest’. Patients appreciated the explicit language used in the new version of the programme as it was not overly complicated. Overall, the video received the highest praise, with patients liking the narrative style presentation. One of them (P16) summed it up by saying, ‘the presenter did a great job . . . it was a damn good video!’
Responses to the new patient workbook were also more enthusiastic and positive. Patients believed it to be a valuable resource for anyone in a hospital setting, especially for those who preferred reading something. Patients praised the workbook for its manageable size. One explained (P13), ‘it’s a nice size to hold in your hands’ with ‘clear easy to read print and the use of contrasting bright colours that make the information stand out’. One patient remarked (P12) ‘It has good readable font size and shaded text boxes’, and another affirmed (P17), ‘I can read it easily after my cataract surgery’. The pictures in the book were perceived as helpful in reinforcing the safety messages as they illustrated what was said in the text. One patient stated (P14), ‘the use of graphics and pictures adds interest . . . it reinforces what you should do’. Reinforcement of key messages in written format was perceived as beneficial. One patient explained (P11) how ‘older patients like me may need reinforcement . . . as my generation are not used to treating a screen as a medium for learning’. Patients also reported that the information was presented in a logical order and points were repeated for emphasis. They also liked the concept of setting their own goals and writing them down, as this encouraged involvement in the process of falls prevention.
The Safe Recovery programme was deemed relevant for everyone in a hospital setting. Most patients identified being at risk of falling while recovering in hospital. One pointed out (P14), ‘[the information] was highly relevant because you don’t feel like your usual self’. Another reflected (P20), ‘I could relate to several of those messages . . . my legs are weak, and I’ve been light-headed and dizzy’. The programme also provided reassurance to patients during recovery, with one of them summing it up (P13) as follows, ‘It makes you feel you’re not alone in your predicament’.
Learning from Safe Recovery programme revised version
Patients
Patients receiving the revised Safe Recovery programme showed significant improvements in their falls knowledge (p = .006) (see Table 1). Patients’ perception (p = .046), awareness (p = .005), motivation (p = .020) and intention (p = .024) to undertake strategies to reduce their risk of falling in hospital also significantly improved (see Supplemental Table S3, Supplemental File 2).
The revised Safe Recovery programme provided patients with a clearer plan (p = .010) about how to reduce their risk of falls in hospital. Male patients learned it was acceptable to ask for help. One of them (P19) disclosed, ‘Guys shouldn’t be [too] proud to ask for help’. Another said (P16), ‘Don’t be a hero! particularly us blokes, press the bloody bell and be patient [laughter]’. Patients demonstrated improved risk and strategy awareness, with one of them stating (P20), ‘I didn’t know . . . that if you feel dizzy you should tighten your leg muscles!’ Another concluded (P15), ‘despite what I might think I am at significant risk of a fall . . . but three things, know if I need help, ask for help, and wait for help can ensure I’m safe!’
Discussion
This study used a participatory approach, in which patients, staff and researchers successfully designed a revised version of the Safe Recovery programme. The updated resources were acceptable to patients and staff, particularly the new and more contemporary video resource. The revised Safe Recovery programme adhered to the original programme design of using best practice principles for patient education and adult learning, catering to lower levels of health literacy and using a strong health education framework (Goodman and Lambert, 2023; Kirkpatrick and Kirkpatrick, 2016; Merriam and Bierema, 2014; Rooney et al., 2021). These principles foster improved information accessibility, supportive learning interactions that reduce cognitive load, and better programme outcomes (Goodman and Lambert, 2023; Merriam and Bierema, 2014).
Patient and staff feedback emphasised that it was particularly important to update the video resource. A review of video-based health education demonstrated that videos have superior effectiveness in patient uptake and health literacy over other patient educational methods, when presented in an understandable way (Dahodwala et al., 2018). A previous RCT that piloted the original Safe Recovery programme resources found that older hospital patients who received the video education demonstrated significantly higher levels of awareness about their risk of falls, as well as better motivation and confidence to engage in falls prevention strategies, compared to those who received the workbook alone (Hill et al., 2009). Studies using animated videos or presentations as interventions have found consistent improvement in short-term patient outcomes such as knowledge and comprehension of information provided by the health care team (Dahodwala et al., 2018).
Programme improvements also led to greater patient awareness of their own personal risk of falls. This is particularly important for two reasons. First, behaviour change frameworks identify that recognising one’s own personal risk of a health problem is a strong motivator for being willing to take action to mitigate risk (Cane et al., 2012; Michie et al., 2011). Second, when investigating beliefs and knowledge about hospital falls, older patients, even those at high risk of falls, have been consistently shown to have a very low self-perceived risk of falling, as well as low levels of knowledge about falls, and think staff will inform them if they are at risk or required to take action (Heng et al., 2021; Lee et al., 2013).
The Safe Recovery programme has demonstrated efficacy in reducing falls and injuries in two previous RCTs (Haines et al., 2011; Hill et al., 2015b). In both these trials, the efficacy was shown to include older patients living with mild cognitive impairment (measured as having a mini-mental state examination score > 23/30 or a short portable mental status questionnaire score of ⩽ 7/10) (Folstein et al., 1975; Pfeiffer, 1975). In the second of these trials, where a cluster design was used, the Safe Recovery programme significantly reduced falls across participating wards (Hill et al., 2015b). This included those patients living with moderate or severe cognitive impairment who did not directly receive the Safe Recovery programme (Hill et al., 2015b). Process evaluations of this cluster RCT with this mode of delivery demonstrated that patients who received the Safe Recovery programme developed high levels of knowledge, confidence and motivation to engage in personalised falls prevention strategies and staff felt the programme created overall, positive ward-level behaviour change (Hill et al., 2015a, 2016a, 2016b).
Further randomised trials to evaluate staff delivery of the revised Safe Recovery programme for its efficacy in facilitating relevant patient falls prevention behaviour change and reducing falls are now required. In previous trials that evaluated the Safe Recovery programme (Haines et al., 2011; Hill et al., 2015b) staff received dedicated time to deliver the programme, and in the present study staff regularly delivered the programme as part of usual care. Therefore, the new programme resources were able to be substituted in the same time allocation. If a hospital planned to commence Safe Recovery programme delivery as part of their patient care, allied health professionals’ workload allocation would need to be considered.
Strengths and limitations
Study strengths include the inclusive participatory approach adopted in this study, which resulted in the re-design of existing resources and enhanced the credibility of the Safe Recovery programme revision. The mixed methods design enabled triangulation of data, with staff and patients having similar positive reactions to the revised programme, contributing to the trustworthiness of the findings.
The study used two different cohorts of patients for each phase, which was considered a research limitation, as it meant that a direct comparison of the two versions of the education was not made by one cohort. However, this was felt to be necessary and practical by both consumers and staff, as patients needed to be provided with education in real time as part of the safety procedures of the hospital and hospital staff delivered the education as part of usual care.
A further limitation was that culturally and linguistically diverse populations were not included in this study. Partnering with these populations to develop versions of the Safe Recovery programme that are best suited to their needs could further assist in achieving successful outcomes (Goodman and Lambert, 2023). In addition, the revised Safe Recovery programme was only evaluated in one setting in a small rehabilitation hospital. Further trials in other hospitals are required to support these findings.
Finally, allied health professional staff were already experienced in programme delivery, and these results may reflect a training effect.
Conclusion
The new World Falls Guidelines recommend that older patients be provided with falls prevention education when in hospital (Montero-Odasso et al., 2022). Education programmes should be evidence-based and designed using sound andragogical and behavioural change frameworks. In this study, which was conducted in pursuit of these goals, patient and hospital staff participation contributed to the successful revision of the Safe Recovery programme, an effective individualised falls education programme. Both staff and patients showed significant improvements in their reactions to, and learnings from, the revised programme. Patients also demonstrated positive changes in their attitudes towards reducing their risk of falling in hospital. Investigating the impact of the revised Safe Recovery programme on older patients’ engagement in falls prevention strategies and its effectiveness in reducing hospital falls and injuries is warranted.
Supplemental Material
sj-docx-1-hej-10.1177_00178969231204329 – Supplemental material for Revising and evaluating falls prevention education for older adults in hospital
Supplemental material, sj-docx-1-hej-10.1177_00178969231204329 for Revising and evaluating falls prevention education for older adults in hospital by Jacqueline Francis-Coad, Melanie K Farlie, Terry Haines, Linda Black, Tammy Weselman, Philippa Cummings and Anne-Marie Hill in Health Education Journal
Supplemental Material
sj-docx-2-hej-10.1177_00178969231204329 – Supplemental material for Revising and evaluating falls prevention education for older adults in hospital
Supplemental material, sj-docx-2-hej-10.1177_00178969231204329 for Revising and evaluating falls prevention education for older adults in hospital by Jacqueline Francis-Coad, Melanie K Farlie, Terry Haines, Linda Black, Tammy Weselman, Philippa Cummings and Anne-Marie Hill in Health Education Journal
Footnotes
Acknowledgements
The authors sincerely thank the staff and patients of Attadale Rehabilitation Hospital for their kind contribution to this research. The revised Safe Recovery programme materials can be made available for ongoing evaluation upon request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by an Australian National Health and Medical Research Council (NHMRC) Investigator (EL2) grant (GNT1174179) awarded to A.-M.H. A.-M.H. was also supported by a grant from the Royal Perth Hospital Research Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.