
Abstract
Background:
Condom education campaigns that aim to prevent early and unintended pregnancies can be undermined by local gender norms, religious edicts and ineffective sexuality education policies. In some schools in Ghana, both condom education and abstinence only education run concurrently.
Methods:
This study explored community attitudes towards condom education in a context of competing messages about sexuality education. The study adopted a qualitative case study approach involving three schools in the Komenda-Edina-Eguafo-Abrem Municipality of the Central Region of Ghana. Data were collected from in-depth interviews with pupils and educators. They were analysed by (1) template analysis and (2) using the Health Promoting Schools framework, which emphasises links between schools and communities in sexuality education programming.
Findings:
In the case study schools, condom education was implemented alongside abstinence education through partnerships between schools and the local community. Attitudes varied in the community – with some members rejecting condom education, while others encouraged their daughters into consensual relationships and contraception. The (Methodist) church locally also rejected condom education. The interplay between poverty and gender power relations puts young women at a disadvantage in decision-making about sex, including condom use. Simultaneously, cultural taboos and religious norms limit condom use and place 11- to 15-year-olds at risk of early and unintended pregnancy.
Conclusion:
Future policy must account for local gender norms, poverty and gender power relations, alongside prevailing religious beliefs that affect sexual health interventions. Unlike the current fragmented picture, a coherent sexuality education framework could effectively address these local factors, leading to better outcomes for sexuality and condom education programmes, with health and educational benefits for young people.
Introduction
UNAIDS and the World Health Organization (WHO) have stressed the importance of modern contraception, particularly condom use, as part of health education programmes to prevent early and unintended pregnancies among young people aged 10–19 (Lohan and Gomez, 2022; UNAIDS, 2004). Condoms are the focus because they are the most effective and affordable way to simultaneously reduce new HIV infections and prevent early and unintended pregnancies (Oppong Asante et al., 2024). Condom education in low- and middle-income countries (LMIC) has focused on young people in particular (Evans et al., 2020). In Ghana, this has been accompanied by efforts to tackle sexist norms, such as the expectation that young women should not have sex before or outside of marriage (Gyan, 2018).
Despite international success in promoting condom use, gender power relations and economic factors significantly impact young people’s sexual behaviours, particularly hindering young women’s ability to use condoms (Closson et al., 2018). In some contexts, economic constraints encourage women into transactional sexual relationships, creating substantial barriers to negotiating condom use with sexual partners. However, young men in transactional relationships for sexual pleasure may not see condom use as a priority (Closson et al., 2018). These challenges highlight the complexities surrounding sexual health among young women in sub-Saharan Africa (SSA) and underscore the need for targeted interventions to address both economic and social factors in promoting safer sex.
In Ghana, the prevalence of condom use among sexually active youth remains low. The Ghana Demographic and Health Survey (Ghana Statistical Service and ICF, 2023) surveyed 2,682 girls and 1,424 boys (aged 15–19 years) and found that only 3.3% and 4.2%, respectively, regularly used a condom. This figure highlights a critical gap in sexual health practice in this population (Oppong Asante et al., 2024). As in other findings from SSA (e.g. Closson et al., 2018), research in the Eastern Region of Ghana reveals that pleasure motivates young men in transactional relationships, whereas young women often engage primarily for economic reasons (Teye-Kwadjo et al., 2017). This dynamic can give young men more power over condom-use decisions than young women. Unfortunately, social norms make parents uncomfortable about, and therefore limit discussion of, condom use by young people (Biddlecom et al., 2009). Gender differences in motivation for condom use granting men greater decision-making power, and negative social norms hindering discussions about condoms between parents and young people, impede the effectiveness of condom education and use, contributing to the high rates of early and unintended pregnancies in Ghana where 10.9% of 15- to 19-year-olds have already given birth (Ghana Statistical Service and ICF, 2023), bringing with them the increased risk of adverse health and social consequences for the mother and her newborn’ (UNESCO, 2017). It has been estimated that 99% of maternal and neonatal deaths among young people in SSA occur due to the physiological unpreparedness of teenage mothers for pregnancy (WHO, 2020).
According to Ghanaian social norms, premarital sex is prohibited, so serious stigma surrounds adolescent pregnancies. Surveys conducted between 1998 and 2017 indicate that nearly one in five adolescent pregnancies resulted in induced abortions, with almost 30% of girls and young women using non-medical or unsupervised methods (UNICEF, 2022, p. 10). In 2013, abortions accounted for 17% of deaths among young women aged 15–19 according to Ghanaian demography and health surveys (Ghana Statistical Service, 2014).
The economic consequences of pregnancies for young people are far-reaching. The stigma surrounding EUP can lead families to neglect their financial responsibilities for pregnant young mothers, even when they have the means to support both mother and child (Crooks et al., 2022). EUP-related school dropouts in Ghana leave young women with literacy and numeracy gaps, fitting them for unskilled labour which leads to poverty cycles and struggling economies (Britwum et al., 2017). Correct and consistent condom use is the surest way to prevent EUP and stem the negative health, social and economic consequences for young people, with 98% effectivity when used correctly for avoiding early and unintended pregnancies (Marfatia et al., 2015; WHO, 2018), yet incorrect and inconsistent use of condoms compounds low usage among Ghanaian adolescents (Oppong Asante et al., 2024).
Education about condom use is a key component of comprehensive sexuality education (CSE). 1 In Ghana, cultural norms conflict with condom education, leading to a rejection of condom use (Adda-Balinia et al., 2016), and lack of gender equity has been documented as contributes to high teenage pregnancy rates in Elmina and Cape Coast (Ahinkorah et al., 2019). The present study investigated how conflicting ideas about sex, marriage and condoms affect condom education and therefore condom use in Komenda-Edina-Eguafo-Abrem (KEEA) Municipality where the study took place.
Ghanaian schools context
The Ghanaian school system comprises kindergarten (2 years), primary school (6 years) and junior high school (3 years) provision. Although CSE has been promoted as an internationally relevant model for sexuality education (Haberland and Rogow, 2015), its introduction has triggered controversy in Ghana since 2019 (Amo-Adjei, 2024). The country’s School Health Education Programme currently promotes sexual abstinence (Ghana Education Service, 2012), while health policies for schools and communities have targets for condom use (Ministry of Health, 2007). This produces a ‘duality’ of sexuality education programmes and interventions: with the promotion of condom use taking place alongside a curriculum that seeks to promote sexual abstinence. This mixed messaging raises important questions which are explored in our study of three schools with different curricula. The focus is on heterosexual condom use, due to the relatively inexpensive and effective protection it offers against STIs and pregnancy.
Since 2012, the Ghana Education Service has had a School Health Education Programme (SHEP) in place under which sexuality education falls. Under the SHEP programme, the government, in collaboration with UNICEF, introduced an abstinence-based sexuality education curriculum called the Enhanced-School Health Education Programme (e-SHEP) to address sexual health issues among young people at junior high school level. The KEEA Municipality of the Central Region of Ghana implements the e-SHEP programme, positioning it as a crucial means of engaging with community attitudes towards condom use. Importantly, the KEEA municipality accounts for most school-related early and unintended pregnancies in the Central Region of the country. It has been argued that, within the municipality, ‘irresponsible parenting’ and poverty push young women into early but consensual relationships (Ahinkorah et al., 2019). Alongside poverty, the high incidence of teenage pregnancy should also be understood within the context of the dual modes of sexuality education prevalent locally.
Earlier findings suggested that HIV prevention among young people in Ghanaian junior high schools has been undermined by sociocultural factors impacting youth intentions to use condoms (Ocran et al., 2022), Anti-condom use norms have limited the effectiveness of prevention programmes, with teachers often delivering abstinence-only education informed by personal attitudes and beliefs. While some educators have recognised the need for condom use for at-risk youth, this had led to moral exceptionalism and stigma directed against particular young people. It also resulted in a failure to engage with gender dynamics and power relations. Misinformation also circulates, such as the belief that condoms break during intercourse. As a result, an abstinence-based, morally-focused sexuality education curriculum persists, with conversations about contraception within the family being difficult due to norms labelling pregnancy outside of marriage as ‘bad’ and ‘shameful’ (Berhe et al., 2024, pp. 6, 7).
Research approach
The three schools selected for case studies were junior high schools in the KEEA Municipality. In each case study school, strengths, weaknesses, opportunities and threats were identified and a model developed to suggest improvements in the sexuality education being delivered. The model sought to engage with local sociocultural, religious and gender-based views about condom use and community attitudes towards condom education. Specific research questions explored were as follows:
Research Question 1 (RQ1). What methods are used for (a) condom education in schools and (b) sharing information about condoms within communities?
Research Question 2 (RQ2). What local sociocultural norms and religious factors shape attitudes towards young people’s condom use?
The Health Promoting Schools (HPS) framework (WHO, 1998), was used to identify the factors shaping community attitudes towards condom education by schools.
Methods
Authors’ positionality
This research described here was undertaken by the first author (BO) as part of a Master’s degree thesis and the findings informed subsequent doctoral research of which the second author (PA) was supervisor. BO knows the region well and previously worked as a teacher in the KEEA Municipality. The positionalities of the authors differed with respect to insider-outsider status: the first author, as a local person, was able to win the trust of participants, conduct the interviews in Fante and gained what seemed like authentic accounts from them. As a former sexual health educator in the Municipality, he also had access to high status participants such as senior teachers and headteachers. His familiarity with the region’s culture and language allowed for a contextual interpretation of participants’ comments. The second author, a cultural outsider but with expertise in sexuality research, critically reviewed the identified quotations and themes, offering an outsider’s interpretation. Together, the insider and outsider statuses of the authors played distinct and complementary roles in relation to the research conducted.
Schools
In the KEEA Municipal Education Directorate, three contrasting junior high schools were assessed (from a total of 65 schools) in relation to the curricula they offered, and the number of sexuality education programmes implemented. The choice of schools was the result of both theoretical intention and negotiation with gatekeepers.
The first author first assessed the level to which sexuality education was incorporated into the curriculum from teachers’ lesson plans for the most recent two terms provided by the headteacher. The assessment ranked schools on the amount and quality of health education activities using the HIV Alert Tool and consultations with the Municipal SHEP Coordinator and school-based health education coordinators.
The three schools selected were the highest, lowest and middle-ranked in terms of how much sexuality education their lesson plans, classroom posters and time-tables revealed. Hereafter, the three schools are labelled High (H), Medium (M) and Low (L) in order of ranking with the criteria applied.
Study participants
Data were collected from the KEEA Municipal School Health Education Coordinator, three school-based coordinators and students who had been trained as peer educators as part of the Enhanced School Health Education programme (e-SHEP), a school-based health education programme supported by UNICEF in partnership with the Ministry of Education.
The Municipal School Health Education Coordinator and the school-based coordinators were invited to participate in the study in their role as coordinators of school-community health sexuality education programmes. Their participation was crucial to ensure that perspectives on condom education reflected programmes both in school and the community.
Six students (one girl and one boy per school) were recruited. The inclusion criteria specified that they should be peer educators aged between 15 and 19 who had been trained to facilitate school health clubs as part of the e-SHEP programme for basic schools. All 13 key informants identified as Christian.
The municipal and school-based coordinators, as well as students, were asked to share their perspectives on condom education as part of school-based sexuality education programmes, and to reflect on community attitudes towards them. Five of the six students were living with their parents and shared their views of parental perspectives on condom education and contraception (Table 1).
Sociodemographic characteristics of interviewees in Komenda Edina Eguafo Abrem Municipality, Ghana (N = 13) (Ocran, 2016).
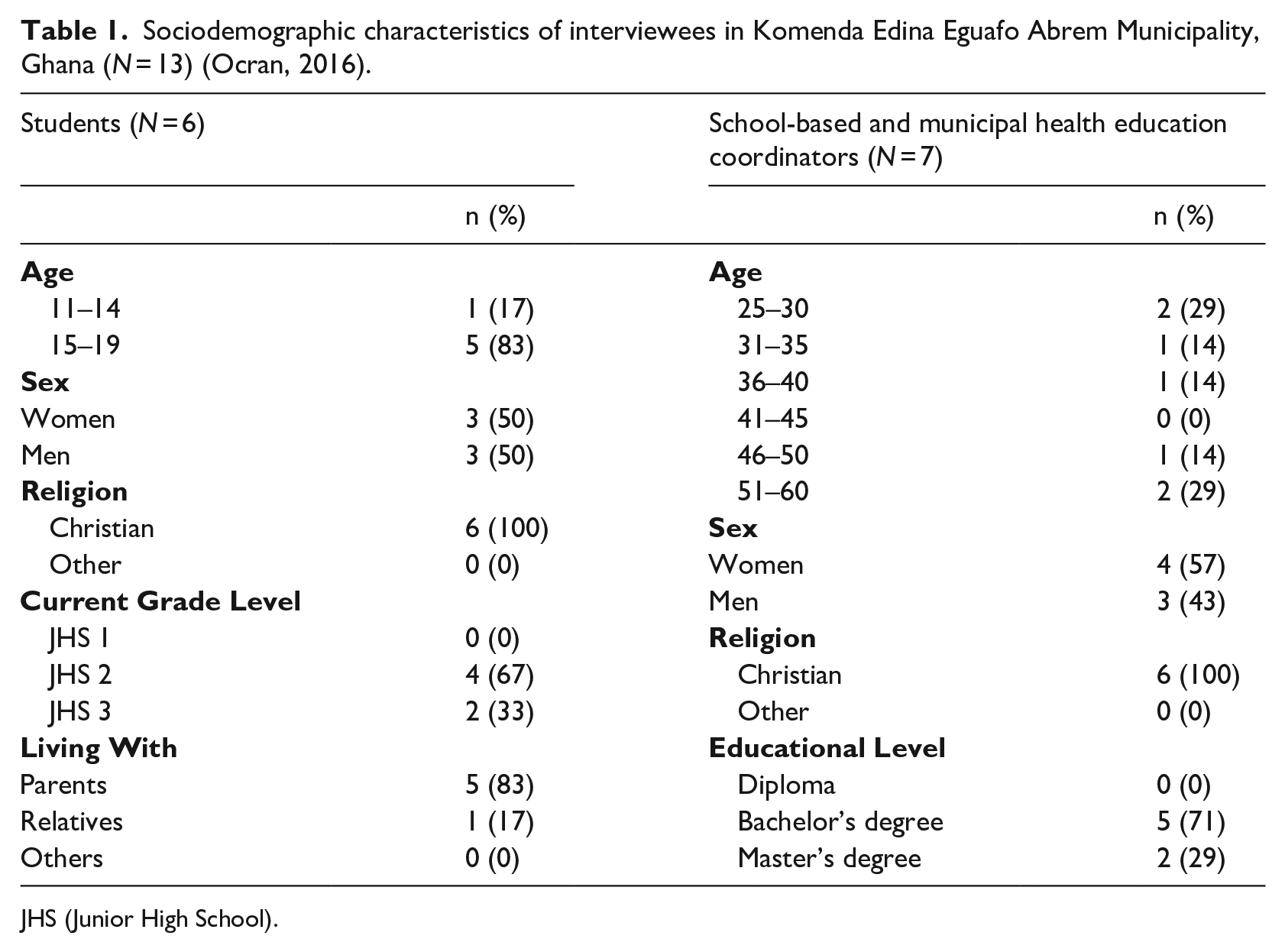
JHS (Junior High School).
Data collection and analysis
Semi-structured interviews were conducted in classrooms in each of the three schools outside of lesson times. Interview guides were used to elicit participants’ views on topics such as love, sex and relationships. In addition, information about sexuality education in school (including condom education), community engagement in school programmes, local factors influencing attitudes towards condoms and suggestions for improving sexuality education delivery were collected. Data were analysed using King’s (2004) template format to identify recurrent themes. Template analysis was chosen over other qualitative methods for its ease in facilitating a systematic exploration of perspectives from the different groups of participants involved in the study.
The analysis centred on factors influencing community attitudes and condom use. With a focus on informant statements relating to the research questions, manual coding took place to identify recurrent themes (King, 2004). The two authors then worked together to revisit each of these themes as reported here.
Ethics
The study adhered to the ethics guidelines of the British Educational Research Association (bera.ac.uk) 2018. It was reviewed and approved by the Research Ethics Committee of the Faculty of Education and Society at the UCL Institute of Education, UK, and by the Education Office in KEEA Municipality. For every student informant, their consent, their parent’s consent and that of the headteacher was obtained. Participants were assured of confidentiality, and all consented to be audio-recorded. Programme managers, including the municipal health education coordinator, headteachers and school-based coordinators have been assigned designations such as PM 1, PM 2, and so on to prevent responses being linked to specific offices or schools. Peer educators are referred to as PE 1, PE 2, etc. In the analysis, participant designations represent the school they were based as ranked H(igh), M (medium) and L(ow), respectively.
Findings
Three main themes were identified as detailed below.
Condom education at school and community levels
Despite official Ministry of Education policy in favour of abstinence education (Ghana Education Service, 2012), condom use can be integrated into teaching and learning activities through integration and infusion. As one programme manager explained,
The Enhanced School Health Education Programme promotes the teaching of sexuality education in the classroom in two forms: integration by which the topic is directly related to the content of the curriculum [. . . .] for infusion, the topic is mentioned but not as the main part of the curriculum. (PM 1)
Nurses from the Ministry of Health may be employed to undertake condom promotion using an infusion approach, which is not part of the mainstream government-approved curriculum.
Moving from the mode of implementation to the content of condom education programmes, the majority of teachers reported that the curriculum focuses primarily on reproductive health and assumes heterosexuality, aiming to educate students about the dangers of premarital (hetero)sex, as the following quotations from a headteacher and a school-based coordinator respectively illustrate:
Sexuality education is being aware of sex in boy-girl relationships and how to protect themselves from consequences such as teenage pregnancy. (L, PM 3) At this point in the students’ lives [age 11 to 14], they should be taught to abstain from premarital sex, and that is why subjects like Science and Religious and Moral Education teach topics such like reproductive health and morality. (L, PM 4)
Other stakeholders, such as the church, were also said to be involved, supporting the stance taken by the Ministry of Education by promoting the abstinence message. A different headteacher explained,
The Methodist Church (also) has in place sexuality education activities that have a special interest in the promotion of sexual abstinence. (M, PM 3)
However, it was evident from some responses that nurses working for the Ministry of Health moved beyond a moralistic stance on abstinence to discuss contraception and condom use even to the point of condom demonstration. This aligned with the overarching policies guiding school health jointly agreed by the Ministries of Education (Ghana Education Service, 2022) and Health (Ministry of Health, 2007). Under these policies, nurses offer technical support to school health programmes. A programme manager distinguished the sexuality education provided by the Ministry of Education from that offered by nurses working for the Ministry of Health:
Ghana Health Service also has school services, it does, so when they go to the school, they teach the inclusive measures such as condom use through demonstration, we (teachers) also teach the abstinence form of it. (PM 1)
A male student in School Two described how nurses were involved in teaching about HIV and teenage pregnancy–stressing condom use as a way of preventing both:
Nurses come around during school hours to talk to us about teenage pregnancy and AIDS. They also teach about how to avoid getting pregnant through the use of condoms. (M, PE 2)
Students had varying opinions regarding the two approaches to sexuality education: abstinence education and nurse-led condom education. A female student defined sexuality education as covering either abstinence or condom education. She described the focus of this work as helping those in sexual relationships remain in school and avoid teenage pregnancy. For her,
Sexuality education helps those who have boyfriends not to get pregnant, and it also helps us not to drop out of school. (H, PE 1)
School dropout is a consequence of teenage pregnancy in KEEA as no childcare is available despite formal policies allowing pregnant teenagers to remain in schools (Morgan et al., 2023).
Regarding condom education programmes in and for the wider community, programme managers leading this aspect of school health education, sought to involve community members in sexuality education (Ghana Education Service, 2014). Some of this work involved partnerships with traditional authorities and non-governmental organisations (NGOs):
It is a strategy (Community directed pillar) that we use because we believe that the children come from the community and since sexuality education is not taught as a subject, we need the parents to support us. So, during Parent Teacher Association and School Management Committee Meetings or whichever forums that bring the parents together, we equip them with necessary skills to impart sexuality education to the children. (PM 1)
The programme manager gave another example of how this work took place:
We also have the Queen Mothers’ Association which has been very, very helpful. . . so we involve them in our activities in the community [. . . .] The Queen Mothers’ [Association] takes an active part in the education of young girls to stay away from premarital sex to safeguard their education for a better future [. . . .] We have lots of NGOs working on sexuality education in the community. So, the children can access some of their services. (PM 1)
Collaboration occurred between the school and the community regarding condom education within the school. The Parent Teacher Association (PTA) and School Management Committee created space for school-based coordinators to talk about the importance of students’ sexual and reproductive health (SRH). One programme manager stated,
During PTA meetings, I am given some time, about 10 to 15 minutes, to talk about important issues about sexual and reproductive health. (H, PM 5)
In addition to discussion about sexuality education at PTA meetings, the Municipal School Health Education Coordinator participated in other community-based programmes and talked about the importance of sexuality education to traditional leaders, the municipal chief executive, and international NGOs working on school health locally.
Community responses to condom education
Teacher reports were used to infer community attitudes towards condom education. Teachers were of the view that parents’ attitudes towards sexuality education and contraception varied. Several said that the community opposed the teaching of sexuality education to students, with educators fearing conflict with parents. One coordinator said,
The community is not prepared to accept what the teachers teach, especially regarding condom education. The community does not accept what the students tell them [about condoms and condom use] and, in the end, [that] influences the students too. . . The community is okay with what society teaches, mainly about staying away from sex before marriage. (L, PM 3)
However, teachers’ reports also suggested that parents had complex, varied and mixed feelings about young people using condoms, showing both support and opposition. For example, while some parents disagreed with condom education, others encouraged their daughters to engage in relationships with older men for financial support. In the latter case, parents might encourage their daughters to use contraception to avoid pregnancy or STIs and HIV. A programme manager reported,
‘Some parents suggest through indirect comments to their daughters to enter intimate relationships with men to satisfy monetary needs and wants’, and some parents encourage their daughters into sexual relationships perhaps in the hope of the financial cost of schooling their daughter becoming shared or becoming unnecessary if the relationship leads to marriage since it is assumed that schooling would end if [their daughter] married. (PM 1)
One of the headteachers recognised this as well, saying,
Parents encourage their daughters into sexual relationships and sometimes contraception to avoid financial commitments to education. (M, PM 3)
Other teachers reported that parents were uncooperative in addressing young people’s risky sexual behaviours, which put girls in particular at risk of STIs including HIV:
We identify certain behaviours of young girls and boys and invite [their] parents over to discuss, but parents adopt a very non-cooperative attitude, including the refusal to honour invitations to discuss identified sex-related problems associated with their children. (L, PM 4)
Implications of resistance/acceptance for young people’s condom use
Teachers and students had different opinions about the sociocultural factors influencing young people’s sexual behaviour, condom-use in particular. Similarly, there were varying views on the factors shaping community and parental attitudes towards condom use among young people. A headteacher, for example, highlighted the impact of poverty on sexuality education:
Poverty renders (sexuality education) efforts useless if girls go back into sexual relationships for money. (L, PM 3)
Economic factors were also identified as contributing to this situation. However, one headteacher emphasised the need to question prevalent ideas about older men and relationships with younger women:
Much education should [take place] about the myth that men solve financial problems, since in the long run the women suffer and work economically more than men. (M, PM 2)
A female student in School H agreed with the headteacher that poverty negatively impacted the effects of sexuality education. Providing for the needs of girls is necessary to prevent consensual relationships with older men he had argued. The student agreed, saying, ‘I think providing markets [i.e. financial support] for girls will prevent them from entering into sexual relationships’ (H, PE 2).
A number of respondents suggested that sexuality education should include discussion of cultural and religious factors because religious considerations impacted hugely on their lives. The headteacher of School M for example mentioned the Methodist church’s more comprehensive approach to sexuality education, which differed from promoting abstinence: ‘If church leaders are made to understand that sexuality education is not only (about) sex being a sin, it will also have a deeper perspective and meaning’ (M, PM 3). And programme managers suggested that parents and community leaders should reconsider the view that sexuality education is ‘wrong’.
Discussion
This study explored pupils’ and professionals’ attitudes towards condom education in Ghanaian schools finding contradictory views that reflect the duality of the concurrent educational interventions with a focus on sexual abstinence and condom education. In Ghana, condom education in school and community settings faces sociocultural barriers concerning gender, age and faith. The interrelated nature of these cultural factors is unsurprising, given that the same factors have influence the disjointed sexuality education policies that prevail in Ghana allowing both abstinence only education and condom education to co-exist in schools and communities.
The dual approach to sexuality education in the three schools included in this study may explain the community’s mixed attitudes towards condom use, echoing findings in our earlier study in 10 Ghanaian junior high schools that revealed differing perspectives among teachers, creating a situation that was confusing for students (Ocran et al., 2022). The HPS framework suggests that school health promotion influences the community, indicating that the dual approach to sexuality education may contribute to these contradictory views. The relationship between local cultures and policies is complex and likely not unidirectional, but is clearly plurivocal/multiple and contradictory.
Our analysis highlights how poverty also shapes community responses to condom education, particularly among the parents of daughters involved with older men. Parents often expect self-sufficiency at an early age from their children, occasionally endorsing daughters’ involvement in economically beneficial relationships where contraceptive use is desirable. However, cultural norms heighten the risk of early and unintended pregnancies for young women. While condom use may be seen as empowering (Nguyen et al., 2021), societal expectations limit women’s ability to negotiate its use (Baiden and Rajulton, 2011; Teye-Kwadjo et al., 2017). Research from Accra indicates that diverse masculinities impact sexual negotiation, highlighting gendered power imbalances in seemingly equal relationships (Agbeve et al., 2022). Young women, especially those who may lack gender power, may face challenges in making informed choices about condom use due to conflicting parental messages. Ultimately, the interplay of poverty and gender norms elevates early pregnancy risks, likely contributing to the high unintended pregnancy rates present in KEEA Municipality (Ahinkorah et al., 2019).
Teachers in this study reported that cultural and religious norms lead to community disapproval of condom education, particularly in church-influenced schools, although this is not always the case. In this study there is notable parental and community resistance to discussing young people’s sexual health, reflecting disapproval of taboo topics like love, sex and relationships in Ghana. Despite being sensitive, conversations about condom use are essential for sexually active young women. However, emphasising that sexuality education must fit the local context. Differing values complicate discussions on children, affecting debates about protection versus the right to information (Alldred and David, 2007). Teachers promoting abstinence often overlook young people’s agency, treating them as children rather than recognising their sexuality (Allen, 2005; Ocran et al., 2025).
Implementing condom education within a fragmented sexuality education policy context requires sensitivity to local factors affecting condom use. Experiences from Thailand and Uganda underscore the need to incorporate the sociocultural and religious context into programme design (UNAIDS, 2004). Condom education must address policy inconsistencies and parental attitudes towards contraception, which can create mixed community perceptions. Further research is needed to explore why some parents support early relationships and contraception for daughters while believing that SRH educational needs end with marriage.
Conclusion
By using the HPS framework to analyse the views of health education programme managers and students, this study identified some of the challenges faced by sexuality education and condom education programmes when they do not neatly align local community attitudes towards condom use. In ongoing and future policy discussions about CSE, it is important for policymakers and practitioners to consider sociocultural factors at the community level. This study has highlighted the interplay between poverty, power and gender norms, and the prevailing cultural and religious beliefs, that shape responses to condom education within schools and communities. These factors not only influence the delivery of condom education programmes but also shape community responses to them, impacting the acceptance of these interventions and hence their likely effectiveness.
Footnotes
Acknowledgements
The authors thank the three anonymous reviewers and the editor-in-chief of this journal for their constructive feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the original study in Ghana which this paper draws on received funding from the Commonwealth Scholarship Commission, UK. However this re-analysis, its authorship, and the publication of this article, was not the subject of any additional funding.