
Abstract
Objective:
Low mental well-being is increasingly reported among vocational education and training (VET) students. Changing moderate-to-vigorous physical activity (MVPA) and sedentary behaviour (SB) may be beneficial for student mental well-being (SMW). Therefore, the effect of an existing physical activity (PA)-based lifestyle intervention on MVPA, SB and consequently the SMW of VET students was investigated.
Design:
Quasi-experimental study
Setting:
VET schools in the Netherlands.
Method:
A total of 126 VET students participated in either education with an integrated 20-week PA-based lifestyle intervention or in a control group that received education without an integrated lifestyle intervention. PA and SMW were measured at baseline and after 20 weeks. The International Physical Activity Questionnaire was used to assess SB and MVPA. The Centre for Epidemiologic Studies Depression scale and Rosenberg self-esteem scale were used to assess depressive symptoms and self-esteem.
Results:
Repeated measures analysis of variance (ANOVA) revealed a significant time*group effect (F(1, 93) = 7.53, p = .007, η2 = .08) for SB: SB decreased in the experimental group compared to the control group. MVPA did not change over time in both groups. No effect of the intervention on self-esteem or depressive symptoms was found.
Conclusion:
The intervention was successful in decreasing SB. However, the intervention did not seem to increase MVPA, and the decrease in SB did not seem to influence self-esteem and depressive symptoms, future research should investigate whether a more intensive PA-based lifestyle intervention is more effective in increasing MVPA and SMW.
Keywords
Awareness of the importance of a healthy lifestyle and mental well-being is growing (Cunningham et al., 2024; Hautekiet et al., 2022). Significant mental well-being issues impact approximately 13% of the adolescents globally, with higher rates in some regions (UNICEF, 2021). Within the school context, mental well-being facilitates academic success (Douwes et al., 2023). Student mental well-being (SMW) encompasses positive emotions, relationships, resilience, self-optimisation, and satisfaction with educational experiences, along with low depressive symptoms and high self-esteem (Noble et al., 2008). This study focused on the latter two aspects among vocational education and training (VET) students.
VET students represent a diverse group ranging in age (i.e. approximately 16–22 years old) and cultural background (Van Engen et al., 2021). Their education is based on learning practical skills in combination with back-to-back classes (e.g. in hairdressing, nursing, carer education), which differs from higher education students, whose study typically focuses on more theoretical work, and who have a more flexible school attendance schedule (Ministerie van Onderwijs, Cultuur en Wetenschap, 2024). VET students often face heightened risks of poor SMW, due to often coming from low socioeconomic status (SES) households and are therefore more susceptible to negative life events and stressors (Hjorth et al., 2016; Kennisplatform onderwijs, 2018).
Poor SMW can potentially lead to lower academic success and higher dropout rates, unemployment, and social exclusion (Amholt et al., 2020; Andrews and Wilding, 2004; European Commission, 2020). Since VET students are known to have unhealthy sedentary lifestyles (Rijpstra and Bernaards, 2011) and changing one’s lifestyle can play a role in SMW, the number of lifestyle programmes delivered in the VET setting is increasing (Slot-Heijs et al., 2021). In the Dutch VET system, schools are not required to provide students with physical education. However, the government advises them to dedicate 5% of the education time to student health and physical activity (PA). For this reason, schools often develop interventions to adhere to these guidelines (Ministerie van Binnenlandse Zaken, 2023). Therefore, we investigated the influence of an existing PA-based lifestyle intervention on the SMW of VET students.
PA is defined by Caspersen et al. (1985) as ‘any bodily movement produced by skeletal muscles that results in energy expenditure’ (p. 126). Research often focusses on moderate-to-vigorous physical activity (MVPA) and sedentary behaviour (SB). MVPA includes activities from brisk walking and light effort to competitive sports and running (Haskell et al., 2007), while SB refers to low-energy expenditure activities like sitting, reclining, or lying (Tremblay et al., 2017). Evidence from studies suggest that more MVPA is significantly associated with fewer depressive symptoms and greater self-esteem (Biddle et al., 2019; Booth et al., 2023; Jensen et al., 2022; Koch et al., 2020), with interventions showing moderate to large effects in reducing depressive symptoms and potentially increasing self-esteem in youth (Biddle et al., 2019; Pascoe et al., 2020). According to the only study involving a Danish VET-population, students who spent more minutes on MVPA scored higher on mental well-being scores (Jensen et al., 2022).
Research findings indicate that reducing SB can decrease depressive symptoms among university and secondary school students (Lee and Kim, 2019; Wang and Peiper, 2022). Specifically within the VET population, a significant association between low SB and high self-esteem has been identified (Kirschner et al., 2022). Given the unhealthy sedentary lifestyle common among VET-students (Rijpstra and Bernaards, 2011), promoting PA and reducing SB through school-based interventions could lead to a significant increase in SMW. Evidence from systematic reviews suggests that PA interventions can effectively alter MVPA and SB behaviours in VET-students, though SB-specific interventions are less documented (Grüne et al., 2020). Moreover, such interventions are often primarily implemented to achieve improvements in MVPA and SB, and their effects regarding SMW are not assessed. Thus, additional research on the effects of PA and SB interventions on SMW is warranted.
There are several theories that explain why a PA intervention could be beneficial for SMW. Neurobiological theory suggests that PA positively impacts SMW by increasing the release of mood regulation hormones such as norepinephrine, serotonin and dopamine (Bazzari and Bazzari, 2022; Lin and Huang, 2020; Portugal et al., 2013). Psychosocial theory emphasises that increased PA leads to improved physical fitness, which in turn boosts self-esteem, and an increased sense of accomplishment thereby contributing to enhanced SMW (Lubans et al., 2016). Finally, behavioural theories suggest that reducing SB and engaging in PA results in higher energy expenditure, which promotes tiredness, reduces stress, and improves mood and sleep quality, all of which are associated with improved SMW (Alnawwar et al., 2023; Sampasa-Kanyinga et al., 2020).
Therefore, the aim of this study was to investigate the effects of an already-existing PA-based lifestyle intervention on SB and MVPA and whether it also had an impact on SMW (i.e. depressive symptoms and self-esteem) in VET students. It was expected that students who followed the PA-based lifestyle intervention had significantly higher levels of MVPA and lower levels of SB after the intervention and in consequence scored significantly higher on SMW than the control group.
Method
Study design
This quasi-experimental study was part of the larger ‘PHysical activity InTerventions to enhance LEARNing in vocational education and training’ (PHIT2LEARN) study. The effect of an in-school PA-based lifestyle intervention on MVPA, SB, and SMW was investigated. MVPA, SB and SMW were measured at baseline and after the 20-week intervention period. The study was approved as an addendum (U2017/00519/FRO) to the PHIT2LEARN study (registered in the Dutch Trial Register (NTR6358) which connects to clinicaltrials.gov), and by the Open University of the Netherlands Research Ethics Committee (cETO).
Participants
Participants were recruited in the Netherlands using purposive sampling. The intervention school was chosen due to an existing PA-based lifestyle programme in its curriculum, while the two control schools were selected for their similarity to the intervention school (Ritchie et al., 2013). A total of 133 first-year VET students training to become childcare workers, specialised pedagogical workers, and teacher assistants participated. The school that implemented the PA-based lifestyle intervention formed the experimental group. For the control group, similar students (i.e. students studying pedagogic work) who received education without integrated lifestyle intervention were recruited.
For the sample size calculation, a power analysis for an ANOVA repeated measures within-between interaction was performed using G*Power (Faul et al., 2007). We used an effect size f of 0.25, based on a reviews by Biddle et al. (2019), who report a moderate effect size between PA and mental well-being. An alpha of .05 for 2 groups (i.e. control and experimental group) and 2 measurements (i.e. baseline and follow-up); a correlation between repeated measures of 0.5’ and a nonsphericity correction of 1, were applied. With 27 participants in the control group, and 27 participants in the experimental group (total N = 54), there was a 95% chance of correctly rejecting the null hypothesis of there being no significant effect of the intervention.
Procedure
Data were collected at baseline and 20 weeks later. The PA-based lifestyle intervention took place between September 2021 and March 2022. Students were asked during class if they wanted to participate in the study.
Before baseline, students received a presentation highlighting the study’s voluntary nature, the option to withdraw from the study, and the anonymity of data collected. Students also received an information letter and consent form. The law in the Netherlands allows minors (16–18 year) to inform their parents but decide on participation themselves, while those aged 18+ make their own decision (National Ethics Council for Social and Behavioural Science, 2018).
Students willing to participate submitted their informed consent a week later at the start of the intervention. Thereafter, participants completed an online baseline questionnaire which collected data on their demographics, MVPA, SB and SMW using Limesurvey (Limesurvey GmbH, n.d.). The experimental group then started the PA-based lifestyle intervention, whereas the control group received education as usual. At 20 weeks follow-up, students again filled out the MVPA, SB and SMW questionnaires.
Intervention
The experimental group engaged in a 20-week PA-based lifestyle intervention, beginning with a social introduction week without lifestyle classes. From week 2 onwards, the programme was tailored to students’ preferences, allowing them to choose between six themes for theory modules (see below). An important goal of the intervention was to increase students’ MVPA by making them aware of the health benefits of increasing PA and implementing extra PA classes.
The first PA class of the intervention was dedicated to assessing the fitness level of the students. Students were asked to complete an online ‘test je leefstijl’ (test your lifestyle) test during a designated session. The outcomes of this test provided students with a clearer picture of their own lifestyle in relation to various factors (e.g. smoking, PA, screen time, fitness). Students also received personalised tips on how they could maintain or improve their lifestyle. In addition, students received 8 extra PA classes of 1 hour each. Four lifestyle days focused on PA and teamwork (e.g. dodgeball, a self-defence class, etc.). Finally, students followed four different theory modules, based on what they felt might be valuable in inducing attitude change. Students could choose from six different themes: ergonomics, healthy diet, addiction, BRAVO (i.e. a Dutch language acronym for PA, smoking, alcohol, diet, relaxation), sleep and stress, and resilience.
At the end of the 20-week period, each student had participated in eight additional PA classes and four PA lifestyle days, completed four theory modules, and engaged in a comprehensive lifestyle evaluation. To ensure full participation, students who missed any PA class were obliged to make up for the absence by joining a similar activity in another class, embarking on a 6-km global positioning system (GPS)-tracked walk, or taking part in a run. The control group received education as usual, with measurements taken at baseline and at 20 weeks follow-up.
Measurements
MVPA and SB
To measure PA and SB, participants completed the International Physical Activity Questionnaire Long Form (IPAQ-LF), designed for individuals aged 15–69. The IPAQ-LF has a Pooled Spearman r test re-test reliability for MVPA of (95% confidence interval [CI]) = .81 (.79; .82) (Craig et al., 2003), and a test re-test reliability for SB of >.75 (Rosenberg et al., 2008). It has a moderate validity (r = .20.35, p < .01) for overall PA (Skender et al., 2016), and captures PA across four domains: leisure time PA, domestic and gardening activities, job-related PA, and transportation-related PA. These domains differentiate between walking (moderate PA), other moderate-intensity, and vigorous-intensity activities.
Participants reported the number of days and the duration (hours and minutes) of certain activities. An example question is: ‘During the last 7 days, on how many days did you do vigorous physical activities like heavy lifting, chopping wood, shovelling snow, or digging in the garden or yard?’. Subsequently, students had to report the duration of vigorous activities around the house. Regarding SB, students had to answer questions on how many hours and minutes per day they spent sedentary. An example question is: ‘During the last 7 days, how much time did you usually spend sitting on a weekday?’
IPAQ-LF scores were converted to weekly minutes:
SMW
SMW was defined as the absence of depressive symptoms and the presence of self-esteem. A Dutch version of the Centre for Epidemiologic studies Depression Scale (CES-D) (Radloff, 1977) was used to measure the absence of depressive symptoms, with 20 items on a 4-point Likert-type scale with options ranging from ‘rarely or never’ to ‘all the time’. Four positively worded items were scored reversely. Summed scores ranged from 0 (not depressed/absence of depressive symptoms) to 60 (depressed/high number of depressive symptoms), where ⩾16 suggested clinical depression (Beekman et al., 1997), and ⩾22 indicated severe to major clinical depression (Cuijpers et al., 2008). In this study, scores were treated as continuous. The CES-D has very good internal consistency (Cronbach’s alpha = .85), satisfactory test–retest reliability (r = .51.67 over 2- to 8-week period, r = .32–.54 over 3–12 months), and good convergent and construct validity (Radloff, 1977).
A Dutch version of the Rosenberg self-esteem scale (RSE) (Rosenberg, 1979) was used to measure self-esteem, with 10 items on a 4-point Likert-type scale from ‘strongly agree’ to ‘strongly disagree’. Five positive items were scored reversely. Summed scores ranged from 0 to 30, with higher scores indicating greater global self-esteem. The scale has been reported to have a satisfactory reliability of .72–.88 (Gray-Little et al., 1997).
Other variables
Students provided information on possible covariates. Their body mass index (BMI) was calculated using an online BMI calculator (BMI Berekenen/Voedingscentrum, n.d.). SES was determined by the highest education level of their parents and/or caregivers. Smoking and alcohol intake were quantified by weekly cigarette consumption, and frequency and average units of alcohol consumed on drinking days. Furthermore, students were asked if they had been diagnosed with a condition or disability that could influence their PA; thereafter, students were asked what the disability was, and who diagnosed it.
Statistical analyses
Before analysis, an assumption check for a repeated measures ANOVA confirmed compliance with all assumptions. The choice of covariates in the repeated measures ANOVA was informed by the results of chi-square tests for dichotomous variables (i.e. gender, SES, smoking, alcohol, physical disability), Mann–Whitney U tests for non-normally distributed variables (i.e. age), and t-tests for normally distributed variables (i.e. BMI). These covariates were taken into account since previous research has shown that they are associated with PA and SMW (Costigan et al., 2019; Eddolls et al., 2018; Tamminen et al., 2020).
Descriptive statistics were calculated using means and standard deviations (SD) for continuous variables and numbers (N) and percentages for categorical variables. Included and excluded groups were compared with ANOVA for BMI, age, RSE, CES-D, SB minutes/week, and MVPA minutes/week and with chi-square tests for gender, smoking, alcohol consumption, SES, and physical disability differences.
The efficacy of the intervention was evaluated using repeated measures ANOVA with time as a within-subjects factor and intervention condition as a between-subjects factor. For PA, behaviour analyses were conducted with pre- and post-IPAQ-LF scores for SB and MVPA. For SMW, analyses were conducted with the pre- and post-scores on the CES-D and RSE. This resulted in a total of four repeated measures ANOVAs. Interpretation of the effect size η², as calculated with each ANOVA, was as follows: η² smaller than 0.01 = negligible, η² between .01 and .05 = small, η² between .06 and .13 = medium, and η² of .14 or more is considered large (Cohen, 1988). Thus, a higher η² indicating a larger effect. Significance level was set at p < .05, and calculations performed using SPSS version 26 (SPSS Inc., Chicago, IL, US).
Results
Participants
A total of 133 VET students were asked to participate in the study, of whom 126 provided informed consent (60 in the experimental group and 66 in the control group). Dropouts due to educational programme changes, absence, or withdrawal left 49 students in the experimental group and 46 in the control group.
After excluding outliers, based on the IPAQ-LF guidelines, 37 students from each group were included for MVPA analysis, as shown in Figure 1. Participant characteristics shown in Table 1 revealed there were no significant differences between both groups. Therefore, no covariates were added to the repeated measures ANOVA. In addition, the group of students included in the data analysis did not differ significantly from the group excluded from the data analysis due to dropout (results not shown).
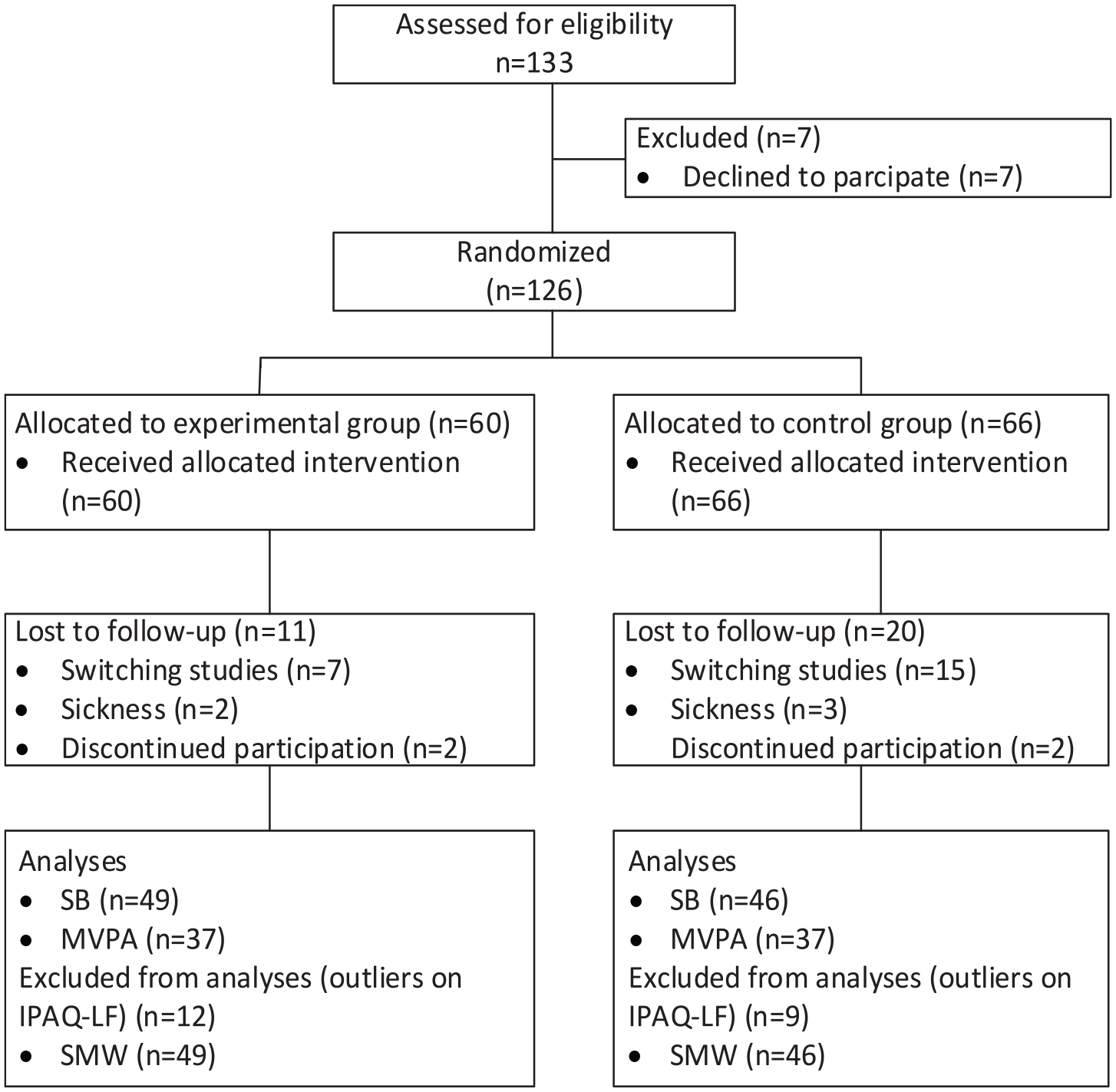
Flowchart detailing participant selection.
Participant characteristics at baseline.
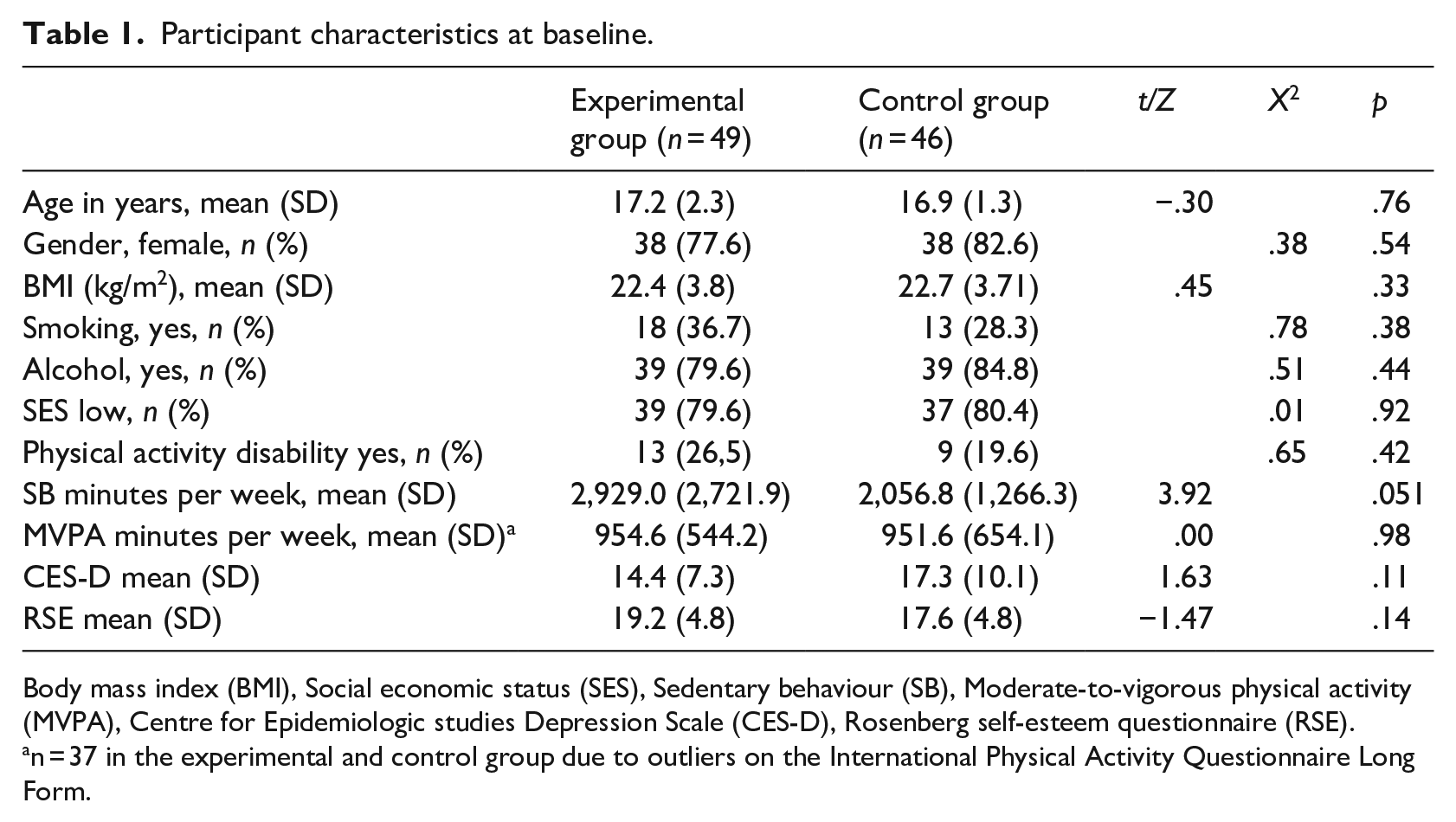
Body mass index (BMI), Social economic status (SES), Sedentary behaviour (SB), Moderate-to-vigorous physical activity (MVPA), Centre for Epidemiologic studies Depression Scale (CES-D), Rosenberg self-esteem questionnaire (RSE).
n = 37 in the experimental and control group due to outliers on the International Physical Activity Questionnaire Long Form.
Effects on SB and MVPA
SB
A repeated measures ANOVA (Table 2) indicated that there was a significant interaction effect of time*group for SB (F(1, 93) = 7.53, p = .007, η2 = .08). The time spent sedentary significantly decreased in the experimental group compared to the control group (Figure 2). The interaction effect had a medium effect size, meaning that 8% of the variance could be explained by the intervention. There was no statistically significant within-subjects effect (F(1, 93) = 3.74, p = .06, η2 = .04), nor a significant between-subjects effect (F(1, 93) = 0.66, p = .42, η2 = .007).
Descriptive statistics and repeated measures ANOVA results of physical activity behaviour variables, pre-test versus post-test for the Experimental group (EG) and the Control Group (CG).
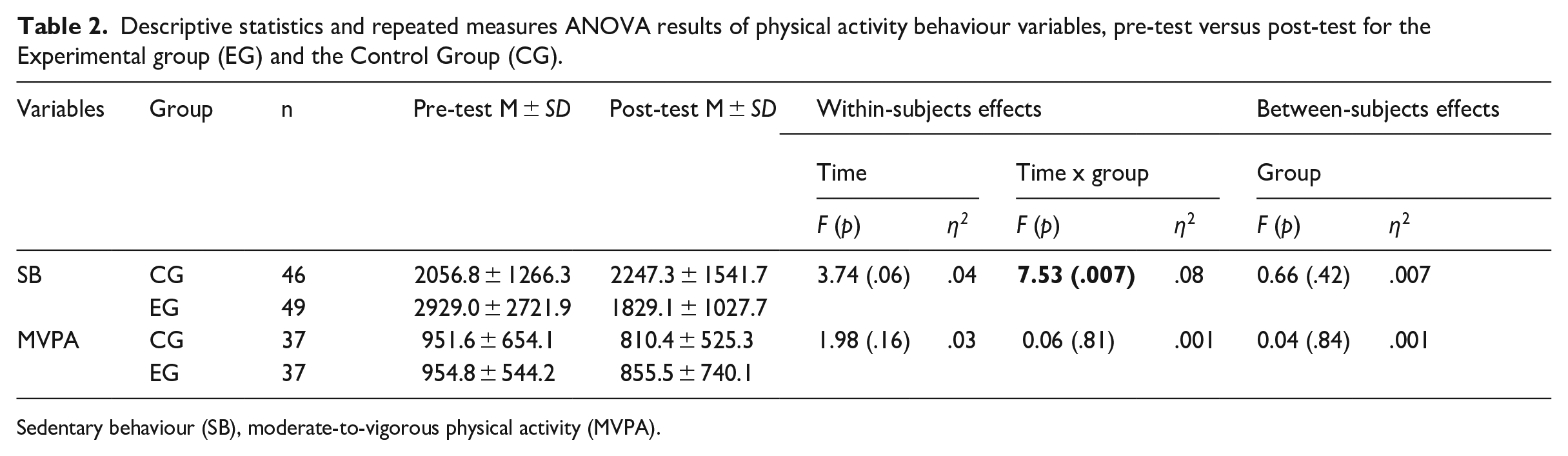
Sedentary behaviour (SB), moderate-to-vigorous physical activity (MVPA).
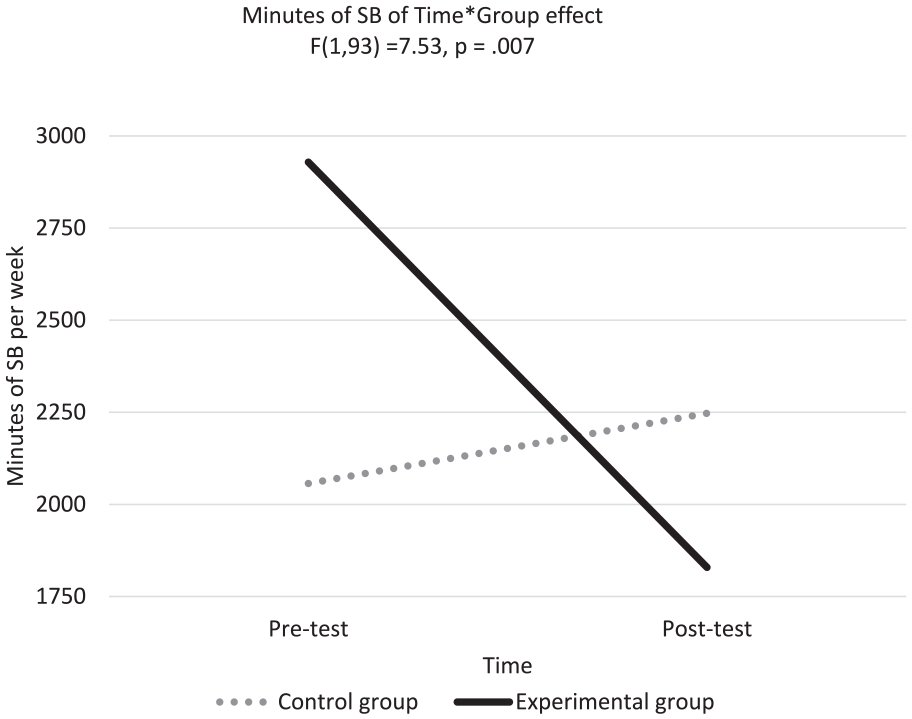
Scores on total minutes of sedentary behaviour (SB) for the experimental and control groups at pre-test and post-test.
MVPA
A repeated measures ANOVA (Table 2) showed no significant interaction effect for time*group for MVPA (F(1, 72) = 0.06, p = .81, η2 = 001), no significant within-subjects effect of time (F(1, 72) = 1.98, p = .16., η2 = 03), and no significant between-subjects effect of group (F(1, 72) = 0.04, p = .84, η2 = 001).
Effects on SMW
Depressive symptoms
A repeated measures ANOVA (Table 3) indicated that there was no significant interaction effect for group*time for scores on the CES-D (F(1, 93) = 0.40, p = .84, η2 = 00), nor a significant within-subjects effect (F(1, 93) = 3.75, p = .06, η2 = 04) or a between-subjects effect (F(1, 93) = 2.68, p = .11, η2 = 03).
Descriptive statistics and repeated measures ANOVA results of student mental well-being variables, pre-test versus post-test for the experimental group (EG) (n = 49) and the control group (CG) (n = 46).
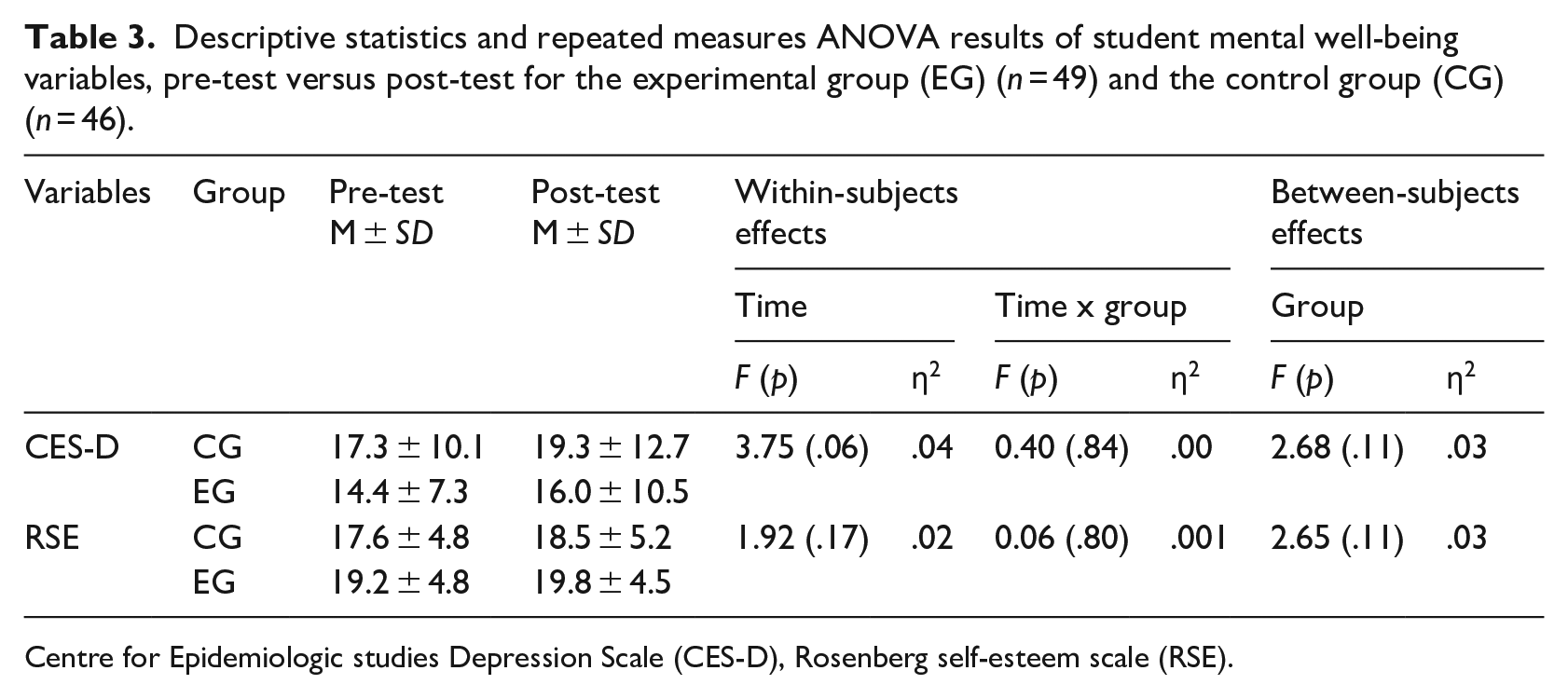
Centre for Epidemiologic studies Depression Scale (CES-D), Rosenberg self-esteem scale (RSE).
Self-esteem
A repeated measures ANOVA (Table 3) indicated that there was no significant interaction effect for group*time for scores on the RSE (F(1, 93) = 0.06, p = .80, η2 = 001), nor a significant within-subjects effect (F(1, 93) = 1.92, p = .17, η2 = 02) or a between-subjects effect (F(1, 93) = 2.65, p = .11, η2 = 03).
Discussion
The purpose of this study was to investigate the efficacy of an existing PA-based lifestyle intervention for VET students in changing MVPA and SB and in changing SMW. Findings revealed that the intervention significantly reduced SB, suggesting that over time, time spent in sedentary activities decreased in the intervention group compared to the control group. The intervention did not change MVPA nor did it change SMW, that is, depressive symptoms or self-esteem.
The significant decrease in SB aligns with findings from other interventions focussing on reducing sedentary time in students (for a review see Hegarty et al., 2016). Elements of our PA-based lifestyle intervention, such as additional PA classes and theoretical lifestyle education, likely contributed to this reduction of SB by enhancing awareness of the health impact of high SB (Fishbein and Yzer, 2003). It was expected that the decrease in SB would be accompanied by an increase in MVPA, but this was not the case. As we did not find a significant increase in MVPA, it is possible that the reduction in SB resulted in an increase in light PA (e.g. standing, walking). However, light PA is not assessed by the IPAQ-LF questionnaire used in this study. Therefore, we cannot draw any conclusion about which type of PA substituted for the educed time spent in SB. In addition, the finding of decreased SB should be interpreted with caution, as the experimental group’s higher baseline levels of SB may have predisposed them to a more likely decrease due to regression to the mean, compared to the control group with its initially lower SB levels.
MVPA did not significantly increase, even though it was expected that the PA-based intervention would cause a significant increase (Cale and Harris, 2006; Grüne et al., 2020). Seasonal changes could offer a possible explanation for this since the intervention took place from the end of summer to mid-winter, possibly reducing motivation to engage in PA outside of school due to shorter days and colder weather (Turrisi et al., 2021). In addition, the added 8 hours of MVPA over the 20-week intervention period, may have been insufficient to produce a substantial increase in MVPA. MVPA did not change despite efforts to raise awareness about the risks of unhealthy behaviour through theory classes and lifestyle tests.
Understanding health behaviour is one of two critical conditions for behaviour change mentioned by Mäntyselkä et al. (2019); the other is that it is important to have a non-resistant attitude. Given the mandatory nature of our PA-based lifestyle intervention, students did not have the option to choose whether or not to participate in the intervention, which may have triggered a resistant attitude towards participation and therefore hinder an increase in MVPA. Moreover, effective behaviour change often requires autonomous self-regulation, that is, students engaging in PA because they find it personally interesting or important (Teixeira et al., 2012). Thus, the compulsory aspect of the intervention may not have aligned with the students’ personal values, underscoring the need for programmes and interventions that can foster intrinsic motivation for PA to achieve lasting increases in MVPA.
The study also explored if the PA-based lifestyle intervention influenced SMW. One reason why SMW may not have been affected by the intervention is that it started at the beginning of the school year. However, research shows that VET students often experience a decrease in SMW as the school year progresses due to an increase in responsibilities related to apprenticeships, workload and household responsibilities (Dopmeijer et al., 2024). Another reason could be the lack of increase in MVPA since an increase in MVPA possibly increases SMW (Biddle et al., 2019; Booth et al., 2023; Jensen et al., 2022; Koch et al., 2020), and not finding a significant change in SMW is therefore not surprising. Possibly the total of eight classes of PA offered in the 20-week intervention period was not enough to achieve the recommended hour per day for SMW benefits to take place (Janssen and LeBlanc, 2010). Other studies, however, do report that lifestyle interventions focusing on PA show bring about increases in SMW (for a review, see Dale et al., 2014). One possible reason for this discrepancy could be that even though the current intervention took the form of a PA-based lifestyle intervention, it also addressed other lifestyle factors (e.g. drug use, stress, etc.). As explained in the review by Dale et al. (2014), interventions targeting PA are particularly effective in improving mental well-being when they focus solely on PA and mental well-being. If a lifestyle intervention focuses on too many factors, it may be perceived as too burdensome, causing the intervention to be less effective (Dale et al., 2014; Grüne et al., 2020).
Observational as well as experimental studies report a negative association between SB and SMW (Biddle et al., 2019; Jensen et al., 2022; Kirschner et al., 2022; Koch et al., 2020). Not finding a change in SMW while SB decreased significantly could be because the decrease in SB was not associated with an increase in MVPA. MVPA particularly is known to increase blood flow for the release of endorphins and monoamines in different brain regions (Craft and Perna, 2004; deVries, 1981; Portugal et al., 2013; Lubans et al., 2016) which can contribute to better SMW. Furthermore, as noted earlier, this study did not take light PA into account, yet previous studies have shown that higher amounts of light PA are also associated with higher SMW (de Vries et al., 2022; Kirschner et al., 2022). As assessment of light PA is lacking, we were not able to gain full insight in the effects of all PA behaviours (i.e. SB, light PA and MVPA) and SMW.
Strengths and limitations
To our knowledge, this is the first study of the effects of an existing PA-based lifestyle intervention in VET-setting on MVPA and SB. The intervention’s impact on SMW was also investigated. Although we found a decrease in SB, MVPA and SMW did not increase. Future studies with more intensive PA-only interventions are needed. Such interventions should include behaviour change techniques that could contribute to changing PA in school as well as outside the school setting, thereby contributing to a sustained increase in PA. That said, a strength of this study was the fact that it examined an already existing PA-based lifestyle intervention, which contributes to its ecological validity.
A potential limitation of this study is the fact that the IPAQ-LF questionnaire was used to measure MVPA and SB, instead of a more objective instrument like an accelerometer. Although self-reported instruments are prone to over- or under-estimating behaviour due to socially desirability effects (Schilling et al., 2018), they offer a less-invasive manner to measure MVPA and SB. The use of these questionnaires may also have resulted in less dropout than in previous studies using thigh worn accelerometers (Kirschner et al., 2022). Future studies including accelerometers that capture all PA behaviours (i.e. light PA and MVPA) are recommended to get fuller insight into different types of PA behaviours. Another limitation was the study the timeframe. Since the intervention lasted 20 weeks, it covered two seasons. Because of this, seasonal influences may have negatively impacted the PA-findings. However, the duration of the existing PA-intervention was predetermined by the school in which it took place. Future research should consider adopting a longer intervention timeframe with more measurement points and a follow-up measurement at a suitable time point
Conclusion
In this study, a significant decrease in SB of VET students was found after following an existing, predominantly PA-based, multi-component lifestyle intervention. However, this decrease in SB was not associated with a change in SMW. Future research is needed to investigate whether a more intensive intervention solely focussing on SB and PA is more effective in increasing MVPA and SMW, as well as the mediating effect of such an intervention on SMW.
Footnotes
Acknowledgements
The authors thank the directors, coordinators, teachers, and students of the schools participated within this study.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.