
Abstract
Objective:
The aim of this study was to describe the strategies used by Canadian healthcare providers to assist men in strengthening their intimate partner relationships.
Design:
Qualitative research study.
Method:
Data were collected through semi-structured individual interviews. Using interpretive descriptive methods, secondary analysis inductively identified the strategies used by 10 Canadian-based healthcare providers. Participants comprised six counsellors, one registered psychologist, one associate certified coach, one father support supervisor and one programme facilitator.
Result:
Three thematic findings were developed: (1) equipping men with lifelong relationship skills; (2) knowing and transforming masculinities; and (3) understanding men’s experiences using trauma-informed care approaches. Theme 1 stressed the importance of attentively listening for cues, establishing dialogue and expressing emotions to meet men’s needs. Emphasised was the need to create safe spaces and respect men’s disclosures about previous intimate partner experiences. Theme 2 highlighted the significance of knowing and transforming masculinities to promote pro-social values by identifying and mobilising men’s strengths and assets. Providers explored attitudes about masculinity and created opportunities for men to model transformative approaches towards equitable relationships. Theme 3 emphasised the need to better understand men’s trauma in order to situate and progress their intimate partner relationships. By acknowledging men’s trauma, providers aimed to undo harmful patterns of emotional suppression and facilitate progress towards healing.
Conclusion:
This study identities strategies for working with men to promote emotional reflexivity, pro-social behaviour and help-seeking in intimate partner relationships.
Introduction
Male suicide is a leading health concern worldwide (Lovero et al., 2023) and experiencing a distressed and/or disrupted intimate partner relationship can increase men’s suicide risk (Oliffe et al., 2022). When a relationship ends, contributing factors include high stress, loss of social support, and disrupted masculine protector roles and provider identities (Oliffe et al., 2022). However, professional services focused on men’s relationships are predominantly downstream (by virtue of being mandated, corrective and often inaccessible to non-mandated men) (Oliffe et al., 2021). In order to promote men’s mental health and prevent suicide, upstream programmes are needed which provide men with the skills and confidence to build healthy relationships and/or amicably end an intimate partnership. In contrast to downstream interventions, upstream programmes use strengths-based strategies to promote voluntary behaviour change, individual agency and gender equity through wider social change (McMahon, 2022), and to support men to build better relationships and reduce conflict and violence in intimate partner relationships (Sharp et al., 2023). There is much to be learned from the providers of men’s relationship services, and how they might offer upstream strengths-based mental health promotion to coach men to build better intimate partner relationships.
Background
Masculinities, help-seeking and men’s relationship services
Hegemonic masculinities are socially constructed practices and performativities associated with men’s dominant position in society (Connell, 2005). Characteristics, including self-reliance, strength and stoicism, have alignments with control and power, and have long been key performance indicators of masculinity (Connell, 2005). Given these characteristics, men who closely align with hegemonic masculinities are often reticent to seek professional help for fear that needing and receiving help will render them weak (Oliffe et al., 2022). Among men who do seek professional help, dropout rates are high, and negative experiences with healthcare services significantly reduce the likelihood of accessing further support in the future (McKenzie et al., 2022; Seidler et al., 2021). Implicated are the services themselves and, as a result, research has focused on developing tailored approaches to engage men in treatment to promote their mental health – most prominently psychotherapy (Kealy et al., 2021). In the specific context of men’s relationships, studies indicate that many providers in the counselling and therapy sector lack the skills and competencies to effectively work with men (Morrison et al., 2016; Seidler et al., 2018).
Hegemonic masculinities also comprise power orientations that position men as dominant over women (and other men) (Connell and Messerschmidt, 2005). Such control is often relational, and many men are complicit in sustaining the dominance of hegemonic masculinities in gender relations (Messerschmidt, 2019). In the context of men’s intimate partner relationships, the most often-told story in research is one of men’s masculine control over intimate partners wherein intimate partner violence (IPV) and domestic violence (DV) feature (Jewkes et al., 2015; Oliffe et al., 2021). In contrast, there is evidence that men draw significant mental health benefits from equitable intimate partner relationships in which decision-making and agency are fairly and justly operationalised (Oliffe et al., 2023). Contemporary shifts in gender relations and masculinities have stressed the importance of strengths-based and asset-building programmes (Jewkes et al., 2015; Oliffe et al., 2021; Osborne et al., 2018) inclusive of trauma-informed practices to aid men in building better intimate partner relationships (McKenzie et al., 2022).
Key to programmatic ideals for upstream work with men’s gendered practices and emergent discourses about relational masculinities are service providers’ speciality skills. While research indicates that men will seek professional help if counselling or therapy services are accessible and engaging (Hussain et al., 2020; Seidler et al., 2018), there is also evidence to suggest that clients who align with hegemonic masculinities can challenge clinicians and counsellors (McKenzie et al., 2022). Help-seeking resistance can reflect self-stigma and the fear of appearing weak in seeking mental health support services (Hussain et al., 2020; McKenzie et al., 2018). Shame can also be a root cause of men’s violence and resistance to professional help both in the context of relationship distress and disruption and mental health challenges (Hussain et al., 2020; Vickery, 2021; Vogel et al., 2011). It is important to note that although men who adhere to these norms are less likely to engage with help-seeking services and may have negative attitudes towards help-seeking, researchers are clear that masculinities are not ubiquitously damaging, and may be leveraged as supportive in treatment (Caddick et al., 2015; Lin et al., 2021). Caddick et al. (2015) for example indicated that strength can serve as a protective factor and predict positive treatment outcomes for men enrolled in post-traumatic stress disorder treatment, while Lin et al. (2021) reported masculinity as a protective factor for depression.
It is noteworthy that current psychological treatments are also inadequately organised and structured for many men (Hussain et al., 2020; Osborne et al., 2018; Seidler et al., 2018). Men are more likely engaged and motivated by programmes if they have an active role in their health management and this underscores the need for action-oriented and strengths-based programmes for men to build better relationships (Hussain et al., 2020; Kealy et al., 2021; Seidler et al., 2018). Gender-transformative programmes that focus on equipping men to explore and engage with their emotions, experiences, and symptom management are favoured by help-seeking men as tailored healthcare services (Hussain et al., 2020; Kealy et al., 2021). Predictive factors of successful providers of outpatient mental health services are therapeutic alliances and supportive counselling styles (Aliga, 2023; Hussain et al., 2020; Kealy et al., 2021). Healthcare providers can help men build relationships by recognising their client’s strengths and preparing for challenges while actively building therapeutic alliances with clients through interactive participatory methods (Hussain et al., 2020; Kealy et al., 2021; Storey et al., 2022). Addressing the knowledge gap about impactful strategies that can inform future training programmes to equip service providers to meaningfully engage men on relationship issues, the current study sought to answer the research question, what are the strategies used by Canadian providers to help men build better intimate partner relationships?
Methods
A secondary analysis (Heaton, 2008) was used to identify the strategies used by Canadian service providers who had experience helping men with intimate partner relationships. This included reviewing existing data to develop and address an inductively derived research question (Hinds et al., 1997). With ethics approval from UBC Behavioural Research Ethics Board, individual qualitative interviews were conducted with Australian and Canadian-based healthcare providers as part of a larger study conducted in 2020 and 2021, with the primary aim to understand healthcare providers’ perspectives about working with men in the relationships space. The senior author (J.L.O.) contributed to the data collection, orientating the lead author (C.G.Y.C.) to the interviews, and the current secondary analysis of a cohort of 10 Canadian-based healthcare providers. The analyses were led by the first author (C.G.Y.C.) by reading the interview data to inductively derive and answer the research question.
Inclusion criteria
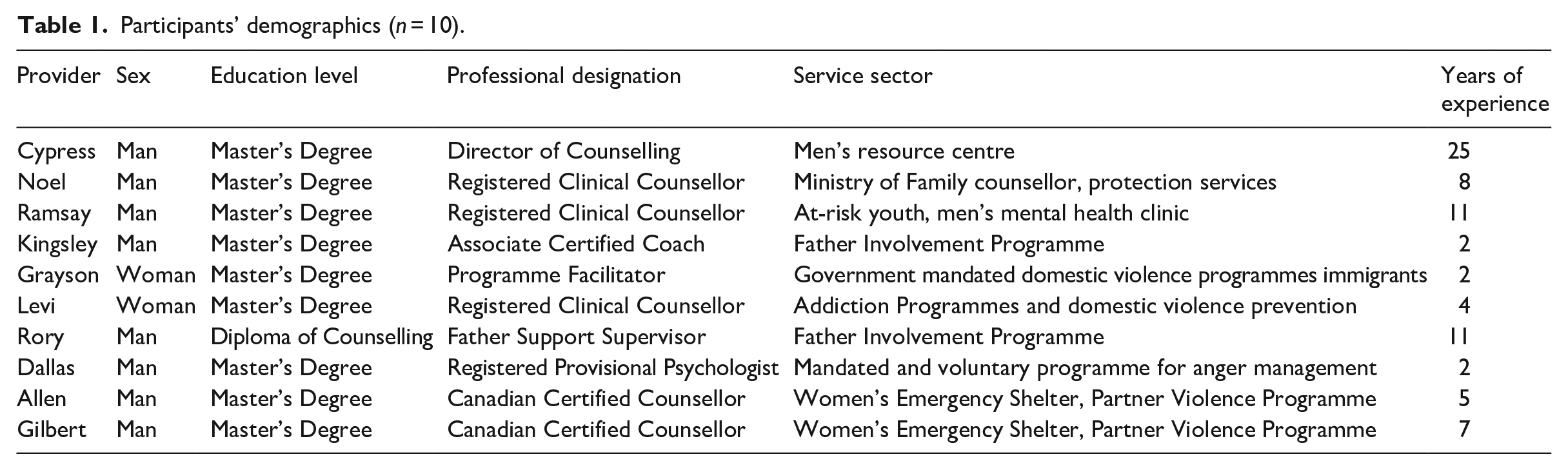
Credentialled Canadian healthcare providers were recruited via social media and targeted emails. The 10 Canadian-based providers (8 men and 2 women) included in the study had an average of 8 years experience working with men and had diverse clinical backgrounds including 6 counsellors, 1 registered psychologist, 1 associate certified coach, 1 father support supervisor and 1 programme facilitator (Table 1). ‘Credentialled’ in this context was defined as an individual who had received formal education at a post-secondary institution and completed a certificate, diploma, bachelor’s, and/or master’s degree in counselling. Nine of the 10 participants had a master’s degree and 1 participant had a diploma in counselling. All participants completed individual Zoom interviews lasting 60 to 90 minutes and were provided with a $100 gift card honorarium.
Participants’ demographics (n = 10).
Data collection and analysis
During interview, participants were asked to share their perspectives of working with men who accessed services and what they needed regarding intimate partner relationship challenges. Of particular interest were participants’ insights to men’s pathways and barriers to services along with specific strategies for working with men. Interviews concluded by inviting participants to share things that might not have been explicitly asked about in the interview.
The recorded interviews were transcribed verbatim and checked for accuracy. Interview transcripts were read one by one by the first author to determine the secondary research questions to be addressed (Hinds et al., 1997). This process was key to distilling a subset of data with adequate depth and detail to feasibly complete a secondary analysis. Thematic analysis involved the six steps outlined by Braun and Clarke (2006). The interview data were first reviewed by the authors (C.G.Y.C. and J.L.O.) in search of meanings and patterns of meaning, in and across the transcripts. This was followed by the development of a preliminary coding schedule. Interview transcripts were then coded focusing on distinct and unique ideas pertinent to each of them while noting repeated and patterned perspectives across participants. Ideas that differed from those of most participants were coded as ‘outliers’ in the initial analysis (Braun and Clarke, 2006), noting their context with respect to the overall findings drawn from across the analysis.
As the analysis progressed, codes were subsumed iteratively into themes. The validity of each preliminary theme was considered within the data set (Braun and Clarke, 2006), to confirm and weight themes as representative of the data in answering the research question. For each theme, illustrative quotes were identified and attached to participants’ demographics and pseudonyms. Participant quotes were selected to capture core findings and reflect efforts to follow the 15-point checklist for thematic analysis suggested by Braun and Clarke (2006). Codes and themes were iteratively discussed by the research team, seeking input on interpretation errors, biases and key findings (Polit and Beck, 2021). Connell’s (2005) work on masculinities, especially the concepts of hegemonic masculinity and plurality of masculinities, was used to guide the analysis and conceptually advance the thematic findings.
Findings
Three themes – equipping men with lifelong relationship skills; knowing and transforming masculinities; and unpacking men’s experiences using trauma-informed care approaches – form the research findings.
Equipping men with lifelong relationship skills
Many providers described coaching with the goal of equipping men with lifelong relationship skills. They looked to assist men in developing skills that could be applied to their current and future relationships. Providers modelled and prioritised the teaching of active listening, open empathetic communication, and fostering emotional competence. Active listening relied on participants providing a safe space for men to speak as little or as much as they wanted. Within this context, the importance of allowing men to lead the conversation in sessions without pressuring them was key. Experiences of sitting in silence with men were offered, suggesting that men should not be rushed or normed as needing to speak – especially early on. The essence of active listening in this regard was being present and ready to listen. Cypress, a counsellor and educator with 25 years experience, shared his experiences as follows:
A lot of the coaching starts off with listening. When I finally come up with a spot where I can see an opportunity to give them good, healthy information, then I can do that. A lot of it is just listening and then looking for an understanding of the situation and then coming up with information that would be useful. They need people to talk to, they need groups. They need to know they’re not alone, and that there are some societal problems.
There is recognition here of the need for pacing, pauses and reflexivity in how Cypress actively listens to and speaks with men. This might be understood as modelling, but is also strategic in helping men feel comfortable about engaging professional help. Underscoring this point, Cypress stressed the importance of men knowing they are not alone in, nor entirely to blame for, the challenges they encountered in building intimate partner relationships.
Providers suggested that teaching men mutual respect was a strategy they employed to help men have better communication with their partners. Levi, a registered clinical counsellor with 4 years of experience facilitating men’s IPV programmes at addiction centres shared his thoughts on the values men needed to develop:
Teaching them that yes, we have disagreements, we have different opinions, but we can still take care of each other. We can still respect each other. We can still sort of see each other, and listen to each other. It’s okay for us to not have the same common ground.
Having mutual respect and effective communication for men to convey their emotions in intimate partner relationships were identified by service providers as key for developing healthier relationships.
Working with men to break silences, participants described the importance of helping men to develop emotional competence. This included coaching men to identify and interpret their emotions before expressing what was felt. Emotional competence was also an important skill for healthcare providers themselves whereby their feelings and vulnerabilities were shared to model and norm that approach. Providers needed to be responsive to men’s individual needs while facilitating a safe environment and cohesion. Noel, a family counsellor with 8 years of experience working with men in family crises, described the importance of validating men’s emotional struggles:
If they’re having relationship struggles, they’re in a vulnerable position and the appropriate response to that – to start with, has to be compassion. Finding a way to be compassionate towards them, regardless of even when they’ve done really shitty things.
Referencing men’s vulnerabilities in receiving professional help, Noel suggested compassion was effective for facilitating the group – and in enabling men to move towards their relationship skills.
Ramsay, a provider with 11 years of experience working with at-risk youth and men in a mental health clinic, discussed how poor communication skills negatively impacted men’s intimate partner relationships:
Emotional suppression, anger, and lack of ability to communicate. Those three things destroy relationships all the time. That’s a product of socialising men that the only acceptable emotions are happiness or anger. We always say that anger is a secondary emotion.
Evident here are the negative effects of men’s emotional suppression, anger and lack of communication in intimate partner relationships. Anger was viewed by Ramsay as a secondary emotion often flowing from an underlying sadness – suggesting this should cue providers to help men (re)connect with, build and share their emotions with others.
Knowing and transforming masculinities
Providers acknowledged the significance of knowing and transforming masculinities to advance men’s intimate partner relationships and pro-social values. Crucial was recognising men’s strengths and values to grow their development and intimate partner relationships. Cypress shared his thoughts:
Masculinity is a challenge. Masculinity is what stops us sometimes from asking for help. I would say that one thing that helps is an understanding that masculinity is all over the place.
Exploring men’s views of masculinities was emphasised as helping them deconstruct and build better intimate partner relationships. Providers spent time working with men to challenge the restrictive limits of hegemonic masculinities as a means to deconstructing their alignments to unhelpful masculinities. Men were then coached to authentically reflect on and take up pro-social values, including the importance of open communication and reducing power differentials. Dallas, a therapist working with men through mandated and voluntary programmes for anger management, explained the challenges of loosening culturally and socially prescribed masculinities:
A challenge with traditional masculinity is that men are not invited and actively discouraged in some ways from experiencing and expressing the full spectrum of emotions, vulnerability being one of the hardest ones. Men, just like women, have a desire to be connected.
Importantly, hegemonic masculinities could shape men’s stoicism and self-reliance in ways that closed them off from their relationships. Highlighting masculine values and virtues for social connectedness, Dallas suggested that men could be transformed by affirming the benefits of connecting socially.
Because most men accessed relationship services when they were in crisis, participants suggested that working with men’s strengths and values were key. Noel explained,
The point at which many men engage in counselling services and social services generally, it tends to be in a moment of crisis. It tends to be when they’ve done something wrong, and that’s not a great place to start.
While not excusing the harms invoked by some men’s negative relationship behaviours, Noel highlighted the need to undo the shame accompanying men’s help-seeking after a relationship crisis by opening up opportunities to work with men’s strengths. Participants explained that they worked with men to shape a strong sense of identity as a means to purposefully becoming accountable and a better partner. Kingsley, a father’s programme facilitator, explained,
The foundation of anyone’s personhood is rooted in identity . . . when you get rooted in your own identity, you show up differently in a relationship. If somebody comes into a relationship with a strong sense of identity . . . they can generally show up from a healthier whole place for that other person.
Providers also discussed the need for upstream services to de-stigmatise biases towards downstream corrective relationship services for men. Ramsay suggested the following upstream approach to help men recognise their own strengths:
The best thing to do is to teach them functional skills. If things do go badly, they know how to recognise it. They know how to improve it. They know how to function with anxiety, depression, or addiction as early as possible just so that it can be derailed as early as possible.
Other providers also spoke about the value of equipping men with skills for recognising and managing conflict in intimate partner relationships, which encouraged them to self-manage and mitigate or prevent their own mental health challenges. Providers acknowledged the broader health benefits of addressing hegemonic masculinities and the importance of teaching men skills to prioritise their mental health in the early stages of therapy.
Providers’ recognition of men’s strengths and masculine values directed their focus towards men’s gender roles, identities and relations. Here, providers worked to ease men’s rigidities and strengthen their sense of identity towards more gender-equitable partnerships. Dallas shared,
Exploring how current perspectives on masculinity, and what sorts of thoughts, feelings and behaviours are realistically permissible for that person. Exploring the benefits and drawback . . . leaning into the experience of the children is often really motivating for guys.
By recognising the multiplicity of masculinities, providers created space for men to thoughtfully reflect on their masculinity without conforming to gender norms. Providers suggested asking men to reflect on the impact of their behaviours and choices regarding what was fair and just for their partner, and role modelling that equity for their children.
Understanding the impact of hegemonic masculinities on men’s mental health, help-seeking and connection with partners was seen as key to building better intimate partner relationships. Providers’ use of these strategies eased the masculine rigidities some men aligned with, making available possibilities for transformative changes towards more gender-equitable partnerships.
Unpacking men’s experiences using trauma-informed care approaches
Previous experiences (including adverse childhood events) can impact men’s ability to form and sustain intimate partner relationships, and key to success was unpacking men’s experiences using trauma-informed care approaches. A strategy spoken about by many participants was having deep one-on-one conversations with men regarding their childhood experiences to map their mental health and intimate partner relationship behaviours. Kingsley highlighted the importance of this work:
Acknowledging that somebody’s perceptions or experiences or what they’ve gone through are absolutely true. Because that’s that person’s lived experience. Yet trying to step into the world or the experience of that individual, understanding them, empathising with them, acknowledging what that might have been like for them.
Providers said empathy was key to effectively helping men work through possible connections between past trauma and current relationship challenges. By using trauma-informed care, providers were able to contextualise men’s fears and challenges and make plans for empowering them to take some control over their mental health. Trauma-informed care often involved the provider being a coach for men in creating structured, specific session goals, which supported men’s self-management skills and strategies for building better intimate partner relationships.
Grayson, a facilitator of individual and group counselling catering to immigrant men seeking support to end relationship violence, shared his use of the Attitude, Skill, and Knowledge (ASK) model (Bakarman, 2011). This model encompasses being aware, providing skills to the client and being knowledgeable while exploring the impacts of earlier trauma on men’s relationships. As an example of such trauma, Dallas described the situation of fathers who shamed their sons for crying, to protect them from being seen as weak or feminine. Boys who grew up in such an environment were encouraged to consider the risks of this form of childhood socialisation in adulthood, and the implications of it for how they engaged as intimate partners:
What really stands out to me is people presenting with overwhelming feelings of isolation and disconnection . . . they don’t have an established history of those kinds of conversations with the supports that they have, which of course my perspective is all wrapped up in a kind of traditional masculinity.
Evident here was Dallas identification of the need for men to deconstruct the origins and learned nature of their behaviours as a first step to moving forward. He later suggested that irrespective of the level of childhood injury or trauma, there were benefits to men from thinking about where their masculinities came from. Providers normed trauma-informed work to get some depth and meaning from events that had happened in men’s lives – not just the relationship distress and/or disruption. Dallas further reflected on the value of a trauma-informed approach that prioritised understanding the often-untold experiences of physical and emotional violence that men had encountered:
Men have experienced usually physical violence, but just as often, emotional violence and intimidation . . . their mom being aggressed upon or experiencing it themselves. The reality is most people who have experienced violence in physical and emotional forms in their childhood choose not to enlist it in the future.
Addressed was the misconception that men who have experienced trauma are destined to perpetuate violence themselves. By recognising the multifaceted nature of trauma, providers could gain a better understanding of the complex relationship between men’s childhood experiences, help-seeking behaviours and gender relations.
Ramsey (introduced earlier) discussed his approach to interpreting and working with men with father–son relationships as an entry point for evaluating trauma:
Look for context as to why the person thinks like that. Father-son relationships are obviously complicated . . . some abuse, neglect and it creates a negative pattern of thinking and functioning that they now use. Emotional suppression almost always comes up.
Emphasised by Ramsey, and some other providers, was the importance of exploring the antecedents of men’s recent and current behaviour. Within father–son relationships, masculinities were understood as being deeply socialised in men. Some providers stressed the potential for emotional suppression as a coping mechanism for trauma, a state that can also manifest (and invoke) men’s efforts to antithetically appearing self-assured and trouble-free. Providers highlighted the need to see past these external presentations, underscoring the importance of helping men to identify and address what may lie below.
Men can find it challenging to open up and express their feelings and experiences. Key to the implementation of trauma-informed work were providers’ strategies for helping men reflect upon the past. Trauma was not excusatory or cause and effect but instead normed the need for men to be retrospective as a requisite for moving forward. The use of strengths-based asset-building approaches demanded men’s accountability for doing this introspective work in and for the betterment of their intimate partner relationships.
Discussion and conclusion
This study’s findings illuminate Canadian providers’ strategies for helping men build better intimate partner relationships. Affirming previous work, our findings support suggestions that culturally idealised and socially constructed masculinities can restrict men’s help-seeking – and limit their ability to seek and benefit from help, especially in treatment (McKenzie et al., 2018, 2022). Evident were participants’ views that men often worry about appearing weak, which transgresses masculine norms of self-reliance, strength and stoicism (Oliffe et al., 2021).
In Theme 1, with its focus on equipping men with lifelong relationship skills, active listening, empathetic communication and emotional competence skills were seen as valuable in beginning work with men. As suggested by others (Kealy et al., 2021; Storey et al., 2022), important to develop trust and rapport men to secure a therapeutic relationship. Dual modelling and teaching were employed as strategies to help men feel comfortable with engaging professional help. In line with the findings from Hussain et al. (2020), by emphasising and jointly working to develop the relational skills men needed, healthcare providers were able to establish therapeutic alliances.
Theme 2, knowing and transforming masculinities, highlighted the need to explore different kinds of masculinity in order to promote pro-social values and recognise men’s strengths and values in building relationships. Providers spoke to the socialisation harms of hegemonic masculinities on men’s mental health and its later implications for intimate partner relationships, as has been previously reported (Oliffe et al., 2021). Also consistent with findings of previous research, working with men’s strengths and values to unlearn restrictive masculine norms was seen as critical for men to become better partners (Sharp et al., 2023). The current findings highlight the importance of understanding men’s views on masculinity to address its function in their identity and in intimate partner relationships. Clarifying the plurality of masculinities with men facilitated the validation of their concerns and emotions, and led to norming of men’s social connectedness. As discussed by Aliga (2023), healthcare providers’ alliance with men in transforming masculinities served as an affirmation of men’s help-seeking and provided self-management opportunities for men facing challenges in their intimate partner relationships.
Theme 3, unpacking men’s experiences using trauma-informed care approaches, considered the implications of the past including adverse childhood events on later intimate partner relationships. Aligned with previous work, providers agreed that men who had experienced trauma may experience difficulty with emotional intimacy, trust and communication in intimate partner relationships, leading to increased risk for conflict (McKenzie et al., 2022). Study findings emphasise the importance of helping men recognise how past experiences may influence (but not excuse) later intimate partner relationships. The use of a trauma-informed approach to care can help manage often long-standing feelings of isolation and disconnection.
Finally, in line with Oliffe et al. (2021), the accounts of service providers in this study suggest the potential of using skills-building and strengths-based approaches to increase men’s ability to build resilience from past experiences with benefits for their current-day intimate partner relationships. The use of active coaching methods in conjunction with tailored trauma-informed care approaches was endorsed as an effective strategy for working with men.
Limitations and strengths
The small sample size of 10 participants working in a wide range of service sectors in this study sets serious limits on the generalisation of the research findings. While the research team was consulted on the development of codes and themes, member checking was not utilised in the study to provide additional insight into reliability and validity. While we relied on the providers’ narratives to identify effective strategies for working with men, we did not elicit or have access to client accounts to confirm this appraisal. Despite these limitations, the study is valuable in highlighting gender-transformative approaches and strategies to help men build better intimate partner relationships.
Next steps
There is an urgent need for more service providers in North America to specialise in men’s relationship work (Morrison et al., 2016). In Canada, there is an increased demand for mental health services and providers who are specifically trained to help men with issues related to masculinity are needed (Tulk et al., 2023). Structured education programmes that encourage healthcare professionals to work with men in the counselling space will potentially reduce client dropout and loss to follow-up (Kealy et al., 2021; Oliffe et al., 2021; Seidler et al., 2021).
While no specialist training programme currently exists for providers working with men in Canada, men’s health training programmes tailored for service providers are available, including Men in Mind, a professional training programme developed in Australia (Seidler et al., 2022) and ENGAGE, a national training programme in Ireland (Osborne et al., 2018). With the growing demand for mental health services (Moroz et al., 2020; Tulk et al., 2023), it is important for North American healthcare systems to learn from this experience and finesse training programmes and services for men in the relationship-building space.
From a health education perspective, men’s relationships may be understood as a pathway for improving their health outcomes. Beyond aiding men’s recovery following a distressed relationship, the present study highlights important considerations for working with men to promote emotional reflexivity, pro-social behaviour, and help-seeking. Moreover, a remodelling of hegemonic masculinities may also normalise open communication and shared decision-making to encourage contemporary equitable relationships.
In conclusion, the current study findings reveal strategies for working with men to promote emotional reflexivity, pro-social behaviours and help-seeking in their intimate partner relationships. Applying these insights and working with men to build healthy relationships will benefit from targeted speciality training for providers with the goal of advancing not only men’s health but also the well-being of their partners and families.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Movember funded Men Building Better Relationships grant. C.G.Y.C. is supported by a stipend from the UBC Reducing Male Suicide research cluster, and J.L.O.’s Tier 1 Canada Research Chair in Men’s Health Promotion stipend. J.L.O. is supported by a Tier 1 Canada Research Chair in Men’s Health Promotion. E.J. is supported by a Tier II Canada Research Chair in Population Health Approaches to Mental Health and Substance Use.