
Abstract
Objectives:
Community sites, including schools, are important settings for interventions to promote children and young people’s mental health and wellbeing. A central provision to support mental health in the UK is school- and community-based counselling services. However, the evidence-base for school counselling services is limited by weak evaluation designs, lack of understanding of different counselling approaches in use, and a failure to conceptualise counselling services as part of a wider complex system. To address the last point, this article takes a complex system-focused perspective to explore how a ‘system disruption’, that is counselling service implementation, can be optimised in the Welsh education system.
Design:
The approach used in this study is a mixed-method qualitative design.
Setting:
Participants were recruited from school and community settings. They included children and young people, parents, carers, school staff, counsellors and stakeholders from health and education.
Method:
Consultations, key system stakeholder interviews and school case studies were conducted. All stakeholders were asked about their experiences of local authority-funded school- and community-based counselling services in Wales. Interview and consultation data were analysed using a thematic analysis approach.
Results:
Data converged into three main themes focusing on the specifics of counselling sessions, counselling services as part of universal mental health provision and a whole education system approach. These three themes are brought together into a complex systems-focused model of an optimised school- and community-based counselling service.
Conclusion:
The model offers an opportunity to address issues with current counselling services in Wales and improve outcomes and sustainability by increasing the likelihood they will become embedded in the whole education system.
Introduction
The mental health and wellbeing of children and young people are an issue of concern in the UK and globally (Patalay and Gage, 2019; Polanczyk et al., 2015). The COVID-19 pandemic has exacerbated mental ill health and low wellbeing in this population (Moore et al., 2022; Racine et al., 2021). Poor mental health is associated with adverse educational and employment outcomes, including school attendance, low attainment and being ‘not in education, employment or training’ in young adulthood (Hale and Viner, 2018; Wickersham et al., 2021). Government policy in the UK promotes children and young people’s mental health and prioritises schools and other community settings, such as youth centres, as sites for mental health promotion and intervention (Department of Health, 2021; Healthier Scotland, 2017; National Assembly for Wales, 2018; NHS, 2019).
One type of school-based provision to support mental health policies in the UK is school- and community-based counselling services (Department for Education, 2016; Education Authority, 2020; Scottish Government, 2020; Welsh Government, 2013). In Wales, for example, Local Authorities must provide an independent counselling service for 11- to 18-year-olds and pupils in their final year of primary school, and may also provide a service at other community locations. Any child can be referred to a counselling service and is then assessed to ensure that counselling is an appropriate intervention for them (Welsh Government, 2013, 2020). Referrals can be made by education and health professionals, parents and self-referral, and pupils receive an initial episode of counselling, usually six sessions, although this varies by local authority. Counsellors must have a recognised counselling qualification, but different therapeutic approaches are used, depending on the pupil’s needs and the local Authority’s service (Copeland et al., 2024; Welsh Government, 2020). Despite widespread implementation of school counselling services, the evidence-base for their effectiveness and their implementation in school systems in the UK has a number of limitations.
The effectiveness evidence-base is dominated by small pilot randomised controlled trials (RCTs), alongside weaker pre-post experimental and non-experimental designs, which draw on routine data and client and staff perceptions of change (Cooper, 2006; Copeland et al., 2024; Hill et al., 2011). Using the criteria specified in the Joanna Briggs Institute critical appraisal tool for RCTs (Tufanaru et al., 2020), to date there has been only one high-quality RCT which found positive impacts at 6 months, but with additional economic cost (Cooper et al., 2021). Reviewing this evidence-base as a whole highlights a key challenge in that widely different types of counselling (e.g. school-based humanistic counselling, cognitive behavioural therapy, play therapy), and forms of delivery (e.g. group, individual), have been evaluated together. ‘School counselling’ is therefore not a clearly bounded, single intervention, which complicates drawing conclusions about the effectiveness of school counselling services.
Alongside mixed evidence of effectiveness, a UK-based implementation literature has identified individual-, school- and service-level issues that are perceived to impede counselling service delivery in school settings (Copeland et al., 2024). These include lack of awareness and understanding of counselling services among pupils, pupils’ feeling stigma around accessing mental health support, insufficient communication between counsellors and school pastoral staff, school staff not understanding the role and benefits of counselling and its confidential nature, and demand for counselling exceeding supply (Cooper, 2006; Fox and Butler, 2007; Hamilton-Roberts, 2012; Hill et al., 2011; Prior, 2012). None of these studies, however, have explored how counselling services integrate with other education policies and mental health provision in schools to determine whether they are mutually supportive or unintentionally disrupt each other. Such an understanding of school, health and wider education system influences is needed to optimise counselling service implementation.
To address this gap, counselling service research needs to adopt a complex systems lens to theorise (and understand) how elements of the wider system influence and interact with counselling service functioning, in order to design counselling services that will integrate sustainably with existing systems. Understanding intervention settings as complex systems is increasingly advocated in public health research (Moore et al., 2019; Rutter et al., 2017). Through a complex systems lens, organisations such as schools are characterised by particular patterns of behaviour and social networks. These are dynamic and self-organising but constrained by the larger systems that they are nested within, for example, the local authority education system (Hawe et al., 2009). Complex systems thinking is reflected in the increasing emphasis on whole-school approaches, including in Wales, where a whole-school approach to emotional and mental wellbeing has been identified as the key framework for all schools to use (Public Health England, 2021; Welsh Government, 2021). Whole-school approaches address schools’ physical and social environments to promote the health and wellbeing of pupils and staff. Activities therefore focus on multiple elements, including school relationships with external health service providers, such as counselling services (WHO & UNESCO, 2021).
In the light of the limitations of the counselling evidence-base described above and the implementation issues identified in previous research, this study sought to take a different approach and adopt a complex system-focused perspective to answer two research questions:
How are local authority counselling services currently functioning in the complex Welsh education system?
How can these counselling services be optimised to enhance their responsiveness to wider system conditions?
Methods
This study drew on qualitative data collected in 2021 for a mixed-methods review of local authority-funded school- and community-based counselling services in Wales (Copeland et al., 2024). Three approaches to research data collection were used to ensure that both a breadth (consultations) and depth (key system stakeholder interviews and school case studies) of perspectives were captured. The study was approved by Cardiff University’s School of Social Sciences Research Ethics Committee (Reference 4056) and study participants provided written informed consent.
Consultations
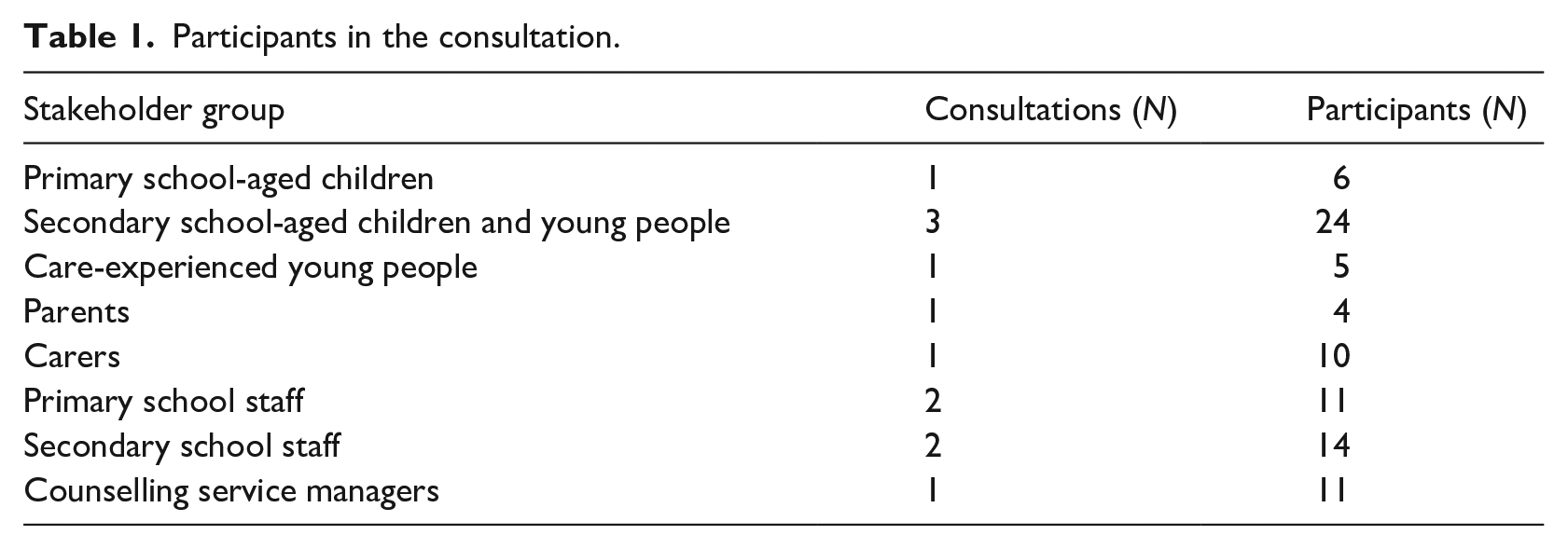
Twelve online consultations were held with different groups (Table 1). Organisations working with children and young people, parents and carers recruited participants and hosted the consultations with these groups. Schools were sampled according to language medium (Welsh, English or bilingual), local authority and level of free school meal entitlement. Invitations were extended to one representative from each school, who could be teaching or pastoral staff, a senior manager or a governor. Participants discussed their experiences and opinions of counselling services and ideas for optimisation. Thematic summaries were made of the discussions.
Participants in the consultation.
Key system stakeholder interviews
Individual semi-structured interviews were conducted with stakeholders from the health and education sectors who were involved in, or interacted with, counselling services at a national or regional level. Fifteen stakeholders were identified by the study funder and steering group and nine took part. They represented the education and training inspectorate, youth services, a national children and young people’s programme, mental health organisations, a national public health organisation and educated other than at school services. Interviews were held online and audio-recorded.
School case studies
Stratified random sampling was used to select case study schools. Strata incorporated language medium, geography and level of free school meal entitlement (primary and secondary schools), level of counselling service provision (secondary schools) and extent of primary school counselling offered by the local authority counselling service (primary schools). Six schools were recruited. However, due to the COVID-19 pandemic, one primary school withdrew, and one secondary school only completed one interview (Table 2).
Case study schools and participants.
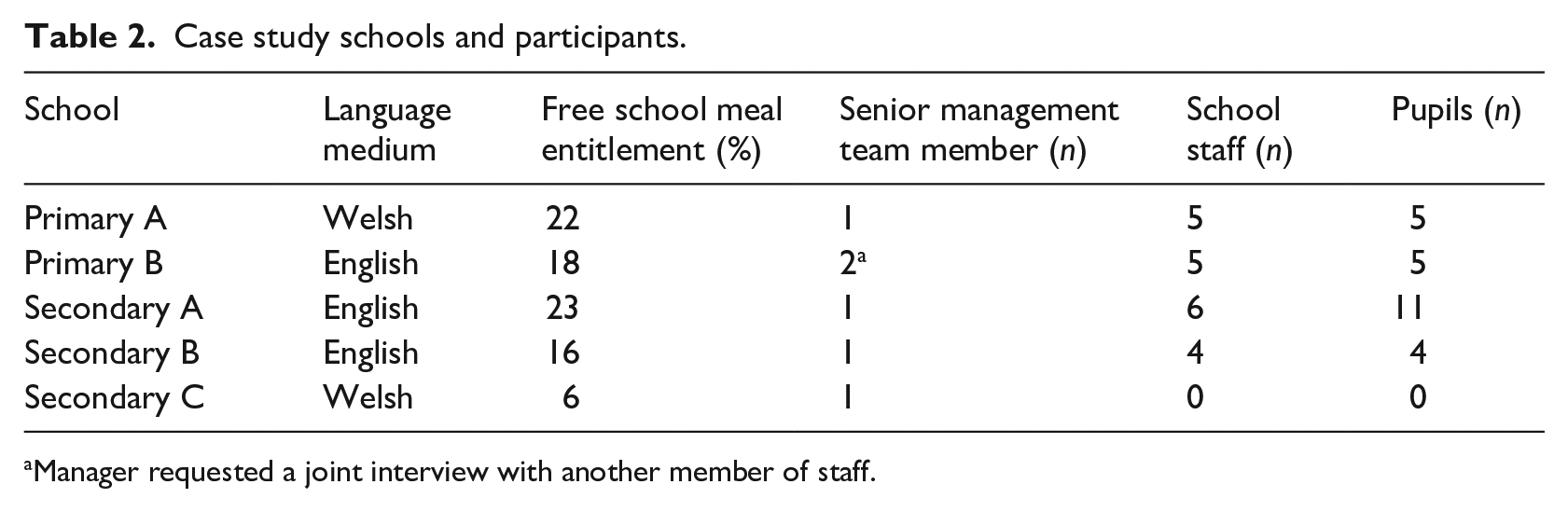
Manager requested a joint interview with another member of staff.
In each school, data collection included an individual semi-structured interview with a senior management team member, a focus group with teaching and pastoral staff and small group interviews with pupils in years 4 to 6 (primary schools) and years 8 and 10 (secondary schools; Table 2). Interviews were conducted online and audio-recorded.
Data analysis
Interviews were transcribed verbatim by a professional transcription company and Welsh-medium transcripts translated into English. Transcripts were checked for accuracy and anonymised.
Interview transcripts and consultation notes were analysed using thematic analysis (Braun and Clarke, 2022). An initial coding framework was devised with a priori codes derived from the study research questions. Two key system stakeholder interview transcripts were then double-coded to refine the framework and assure consistency of coding. The refined framework was then applied to all key system stakeholder interviews. Transcripts from one case study school were then double-coded using the refined framework, with additional codes being added where needed. All remaining school case study transcripts were then coded. Finally, the coding framework was used to organise the consultation notes. All coding was undertaken by four members of the study team and any inconsistencies in coding identified in the double-coding stages were resolved through discussion.
To integrate the data from the interviews and consultations, coded data from each were re-read and organised into themes. Themes from each of the three data sources were then compared, simultaneously drawing in findings from a rapid evidence review (Copeland et al., 2024) to generate study-level themes and sub-themes. The study-level themes and sub-themes were then organised into a complex system model of an optimised counselling service. Findings from the study-level themes were reviewed again to refine the model and strengthen its conceptual coherency. This included consideration of feedback on the model from the study steering group.
Results
The data converged to enable the identification of three main study-level themes.
Theme 1: Counselling sessions: the specifics of their approach and delivery
Theme 2: Universal mental health and wellbeing provision: counselling services’ position within this provision
Theme 3: Whole education system approach: 1 the context for universal mental health provision with integrated counselling services
Each theme and its sub-themes are presented below, and together they describe our understanding of participants’ experiences of current counselling service functioning, and their suggestions for how counselling services could be optimised. The themes and sub-themes are then organised into a model of an optimised school- and community-based counselling service that takes into account our understanding of counselling services within the wider education system.
Theme 1: Counselling sessions
This theme identified specific aspects of counselling sessions that determined how children and young people experienced them, and how they could be optimised within the school and wider systems. It included three sub-themes: principles, delivery and capacity and capability.
Principles
Principles referred to the underpinning ethos of counselling sessions, which participants suggested should be a child-centred approach that offered choice, tailoring and flexibility. Lack of choice was a key issue, with some services being described as having a ‘one size fits all’ approach. Participants had experienced lack of choice in a number of areas, for example, choice of counsellor or choice of language. Some services allocated counsellors to schools, thereby reducing pupil choice. However, school staff and some counsellors favoured this approach as it meant they could strengthen their working relationships. This potentially optimised the functioning of these relationships, that is, the social networks within the complex system of the school.
Choice also arose in relation to setting. Counselling services in Wales are encouraged to offer provision in community settings as well as schools, so children and young people can attend counselling where they feel most comfortable. Community provision is patchy, however, and awareness of it is low. Although young people acknowledged that accessing counselling sessions was easiest at school, they thought it important to have a choice:
I think that’s very important that they have the choice of whether they want to do it in school or out of school because I just feel it is more control over the situation. (Pupil, secondary school A)
The challenge of offering choice for younger children who may be less able to request or refuse counselling was acknowledged. One primary school senior leader advocated choice be balanced with professional input for younger children:
The word we use in this school is ‘child negotiated’ rather than ‘child-led’ [. . .] The counsellor is professional and gives therapy, so they are the people who are going to know, but in discussion with the child and the family, rather than just the child leading the way they want. (Senior leader, primary school A)
Related to choice was the principle of tailoring and flexibility in counselling sessions, meaning sessions being adapted to meet the needs of individual children and young people. There were negative and positive accounts of tailoring and flexibility, related to services’ responses to changing demand, critical incidents and missed sessions, restricted number of sessions and timing of sessions in the school day, as the following teacher explained:
But that, for that pupil, is a really valid reason why he doesn’t want to go to counselling anymore, because he was taken out of, twice in two weeks, he’s been taken out of a lesson that he really enjoys. (Staff member, secondary school B)
Delivery
This sub-theme included practical aspects of counselling sessions. These included referral routes, co-occurring drop-in and appointment systems, offering different therapeutic approaches, having appropriate spaces for counselling and mode of delivery.
Counselling services offered multiple referral routes, including self-referral. Self-referral was viewed positively, particularly for older young people, as it conferred autonomy on them and prevented school staff acting as service gatekeepers. Some school staff, however, perceived self-referral as a ‘double-edged sword’, as it compromised their capacity to offer complementary pastoral support.
The location of counselling sessions in schools was also important. Counsellors stressed the need for a consistent, appropriate space that they could tailor to their needs. School staff, however, said their capacity to provide such spaces was sometimes limited.
The COVID-19 pandemic saw counselling sessions move to online and telephone delivery. Some young people preferred these delivery modes, and they potentially increased counsellor availability by reducing their travelling time. However, there was a consensus that they were not appropriate for all young people. Issues included difficulty in establishing a therapeutic relationship and lack of privacy or suitable technology at home. It was therefore recommended that counselling sessions be flexible in their delivery mode:
Well, as with everything, one size doesn’t fit all, and there are some children who are going to feel more comfortable behind a screen. And perhaps the relationship can be developed – starting from behind a screen, then a meeting, and then one-to-ones. (Senior leader, secondary school C)
Capacity and capability
The sub-theme ‘capacity and capability’ referred to workforce issues that impacted on counselling sessions. Lack of capacity was a key concern and participants described long waiting lists for counselling. They expressed concerns that problems would worsen while young people waited and that they might change their mind or feel disillusioned at having to wait:
. . . you’ve kind of got to say, ‘But unfortunately, you’re not going to get that for three months’. And it’s a very deflating thing, then, for our pupils, thinking, ‘Well yeah, he’s trying to help me but, obviously, he can’t’. (Staff member, secondary school B)
Two examples of wider system constraints characteristic of complex systems were discussed in this sub-theme. Counselling workforce diversity was raised as problematic, as work was perceived to be dominated by white, middle class women, due to counsellors having to fund their own training. Service managers also highlighted recruitment and retention challenges, which they felt were compounded by the annual grant funding model they relied on restricting the length of employment contract they could offer.
While some young people who participated in the consultations said they would like to see teachers trained as counsellors, as they knew and trusted them, there was a wider consensus that counselling should be delivered by trained, accredited professionals. Furthermore, there was a desire for counsellors to have wider skillsets, for example, working with care-experienced young people.
Theme 2: Universal mental health provision
This theme related to participants’ experiences and views of counselling service integration into universal mental health provision, and the need for that provision to raise awareness of counselling and deliver complementary, wraparound support in order to optimise counselling services.
Participants thought counselling should be a targeted service, integrated into universal mental health support in schools. This included all staff being able to discuss mental health and signpost pupils to support, and schools offering a range of support to meet pupil needs and preferences. This would mean pupils would be supported until they felt ready for counselling:
I had a child earlier for example where she’s really struggling, and she didn’t want to be referred for counselling and that’s fine. I said, right come in and check in with me every week and then we’ll see once you’ve done that, if you need to talk to someone, then you can try counselling. (Staff member, secondary school A)
However, awareness of school counselling services was low, as was knowledge of the purpose of counselling and what counselling sessions might entail. This was considered problematic because there was a perception that children and young people should understand all the mental health interventions available to them, to enable them to make an informed choice about the support they engage with.
Improving counsellor visibility was considered to familiarise pupils with the counsellor, thereby diminishing the mystery surrounding counselling and helping pupils build trust with the counsellor. This was seen to be particularly important for younger pupils:
. . . someone like you’ve met before, and someone that you trust, and you’ve spoken to them before. And you need to make sure that you can actually speak to them without being worried or scared or anything like that. (Pupil, primary school B)
School pastoral staff wanted to work more closely with counsellors to help them support pupils after counselling. They were frustrated by counsellors’ unwillingness to offer a ‘handover’ and found counsellors’ commitment to pupil confidentiality unnecessarily strict:
. . . a good thing would be to share any information. Even if it’s just, you know, through a feedback form or some advice for what the school could offer, [. . .] some suggestions for the future going forward. (Staff member, secondary school B)
This, together with pre-counselling support for pupils, would mean schools could provide wraparound support for counselling services.
Integrating counselling into schools’ universal mental health provision was not, however, perceived to be without risk. While there was a desire from schools to adapt their processes to integrate counselling services, some participants highlighted the importance of pupils seeing the counsellor as someone not ‘of the school’, so that they could talk to them freely:
It’s really important to get the balance between, we’re not part of the school, so the counsellors are not the teachers, they don’t need to be referred to as ‘Miss’ or ‘Mrs’. First names; using mobile phones; using whatever language they want to use, including swearing. (School case-study counsellor)
Theme 3: Whole education system approach
This theme focused on participants’ experiences of aspects of the school and wider systems that impacted counselling services, and how attention to those aspects could potentially facilitate the integration of counselling services, embedded within universal mental health provision, into a whole education system approach. Five sub-themes included benefits of the approach, capacity, culture, the multi-agency relationships the approach requires and its challenges and risks.
Benefits of the approach
A whole education system approach was perceived to offer a supportive framework for delivering counselling services for several reasons. Under the Welsh Government’s Whole-School Approach Framework, schools support mental health through addressing it positively in all areas of school life, including the curriculum, and through universal and targeted provision. Participants thought the approach would therefore lead to early identification of mental health issues, thereby preventing them from escalating and reducing demand on counselling services. Furthermore, the approach would normalise mental health and reduce stigma, thereby creating an environment where pupils could discuss their feelings and not be concerned about being seen to use counselling services.
There were three sub-themes related to successful implementation of a whole education system approach to mental health. The first of these was capacity.
Capacity
School staff felt ill-equipped to support pupil mental health, suggesting a lack of capacity in the school workforce to implement a whole education system approach to mental health. They described ‘muddling through’ and expressed a desire for training to build their skills and confidence. Participants wanted all school staff to be able to respond compassionately and knowledgeably to pupils and for staff to be able to support pupils while they waited for counselling. Training about counselling itself was also important, to address limited staff knowledge of counselling’s aims and benefits.
Culture
The sub-theme of culture focused on the need for a mental health and wellbeing promoting culture in schools to address the significant stress that school staff experienced due to supporting pupil mental health with limited skills:
. . . we feel often that we’re failing the children, because we’re not able to be proactive enough and there is only so much we can do. (Senior leader, primary school B)
They identified school leadership as key to creating and sustaining a wellbeing-focused school ethos that prioritised staff as well as pupil mental health.
Multi-agency relationships
The sub-theme of multi-agency relationships focused on the relationships between the varied stakeholders involved in mental health and counselling service provision. The quality of these relationships – the social networks of the complex system – was important, but variable. School staff and counsellors acknowledged the effort required to build good relationships between themselves and identified several areas of tension, including communication, inconsistency between counsellors, conflicting priorities around confidentiality and counsellors’ space requirements.
Parents and carers were also influential stakeholders. Schools had experienced some parents of primary school-aged children being defensive when the school suggested counselling as they felt that this was a judgement on their parenting. Secondary schools do not inform parents that their child is attending counselling if the pupil wants the information kept confidential, unless a safeguarding issue emerges. This approach was valued by pupils and believed to encourage them to attend counselling. However, it could create tension between parents and school staff if parents found out their child had received counselling without their knowledge.
Multi-agency working between professionals was largely considered to be poor. Primary school staff described being passed back and forth between services like ‘ping-pong’. Multi-agency working was therefore considered important to facilitate counselling services’ integration with other sources of mental health support within a whole education system approach.
Suggestions about how to improve stakeholder relationships included counsellors joining the ‘team around the child’ approach to multi-agency working, counsellors joining school pastoral care team meetings and schools holding wellbeing workshops for parents:
I’d like to see wellbeing workshops, perhaps once a month, [. . .]. [Agency name] would do a parenting course, maybe [the counselling service] could join in on that as well, and just sort of speak to parents and say this is our service, this is what we provide, and this is what the children can access. Maybe they’d feel a bit happier then. (Senior leader, secondary school A)
Challenge and risks
A number of challenges and risks to implementing a whole education system approach were identified and created the final sub-theme. There were concerns that increasing expectations on schools in relation to mental health provision might overload them in the context of other educational reforms and the time burden of additional training might prove too great. Some school staff expressed a fear that academic and mental health priorities would compete, with the former winning out as it is the key parameter on which schools are judged.
Capacity within external agencies was a further concern, and it was suggested it would be futile to try to implement strategies to facilitate multi-agency working, such as multi-agency referral panels, if the services that could be referred to had low capacity.
The risk of harming relationships with parents was raised by primary school staff, who suggested that discussing mental health with parents, particularly if a child’s issue was family related, could damage relationships that had taken a long time to establish:
We might have spent five years building up a reasonable relationship with a really, a family that are having a really difficult time and whose children suffer because of it, and then that one conversation, could really put a stop to that really, and stop them bringing their children to school. (Staff member, primary school B)
An optimised model of a whole education system approach to counselling
To facilitate the use of these findings in the design, delivery and evaluation of counselling services, the three main themes are brought together into a system-focused model of an optimised school- and community-based counselling service (Figure 1). The themes relate to the intervention the counselling service represents, that is the counselling sessions themselves (theme 1), and to two tiers of the complex system within which the service operates (themes 2 and 3). Each part of the model addresses the issues and suggestions identified by the study participants, as described in the previous sections.
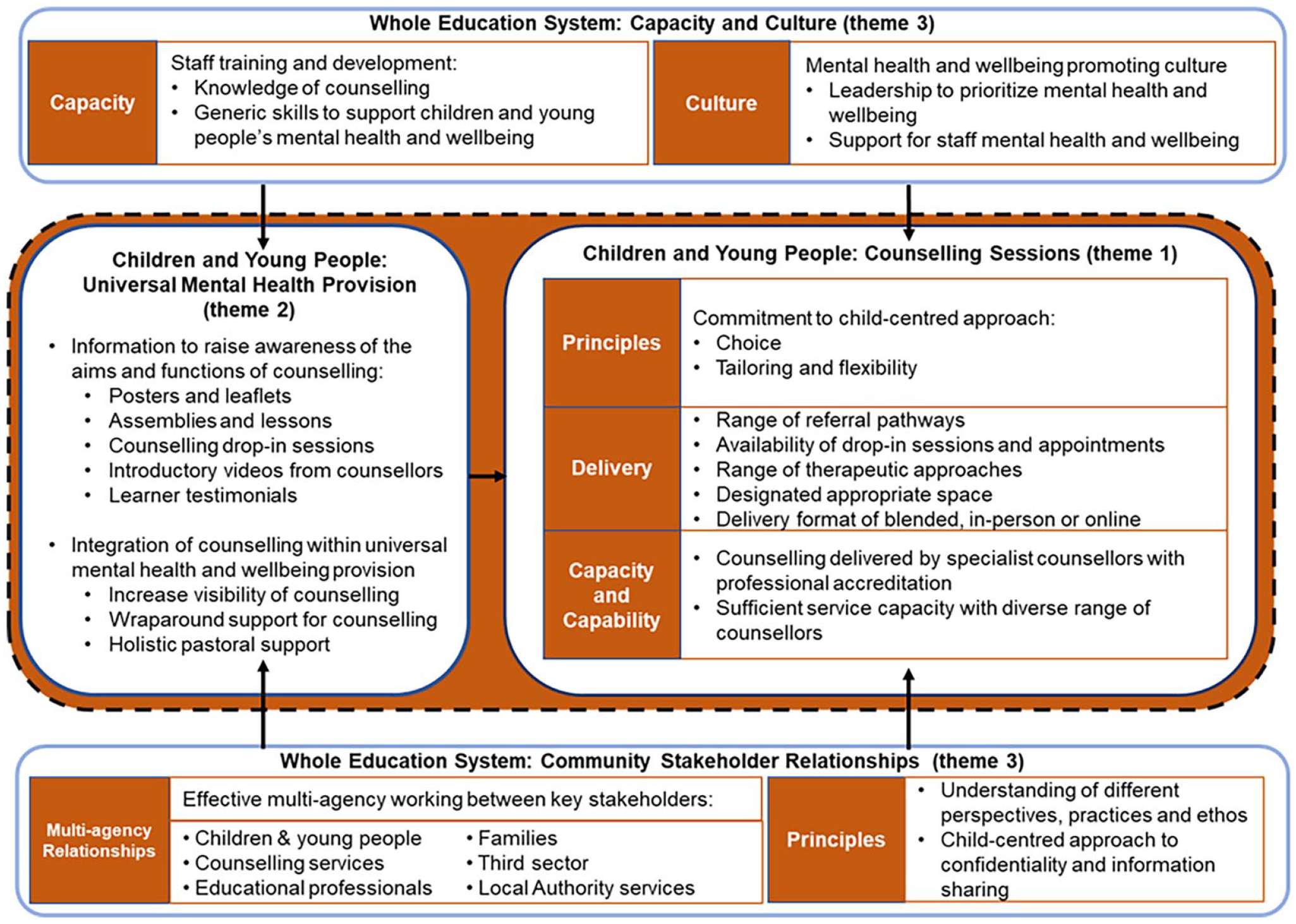
A system-focused model of an optimised school- and community-based counselling service.
To optimise counselling sessions (theme 1), the model proposes a core principle of a commitment to a child-centred approach. This approach can be encapsulated by the notion of ‘the right therapy with the right counsellor at the right time’ and would see service provision offering choices and flexibly adapting to meet need. The model also reflects the elements of counselling session delivery that could help operationalise a child-centred approach, and the ‘capacity and capability’ needed from the counselling workforce. The model posits that sessions should be delivered by professionals with accreditation and that the workforce should have sufficient capacity to meet demand and reflect the diversity of the children and young people it serves.
The model positions counselling sessions as a targeted intervention, supported by universal mental health provision (theme 2). Critical for achieving this in practice is increased awareness of the aims and functioning of counselling and for counselling services to be better integrated into systems of universal mental health provision. The model therefore proposes that targeted interventions such as counselling should be experienced by children and young people holistically, with schools and counselling services working together to provide support before, during and after counselling.
The model situates counselling sessions and universal mental health provision within a whole education system approach (theme 3). Capacity and culture were two core system requirements for delivering high-quality mental health provision within a whole education system approach (top section of model). To create and sustain sufficient capacity within the system, the model includes staff training and development to deliver universal mental health provision. It also includes a mental health promoting culture characterised by leadership that prioritises mental health provision for pupils and staff. To reflect the importance of relationships between professionals, families and children and young people, the model includes reference to the principles that should underpin stakeholder relationships within a whole education system approach (bottom section of model). These include understanding each other’s perspectives and adopting a child-centred approach to confidentiality and information-sharing.
Discussion
This paper has sought to apply a complex systems lens to the implementation of counselling services in school and community settings. The use of complex systems thinking has allowed a novel understanding of the issues of counselling service implementation and a fresh perspective on how to address them (Moore et al., 2019; Rutter et al., 2017).
Participants described mixed experiences of the current counselling service model that highlighted areas where services were not functioning well and were not fully integrated into the wider whole education system. Some of the issues resonate with findings from the implementation literature in the UK, for example, low capacity (Hamilton-Roberts, 2012), low awareness of what counselling entails (Prior, 2012), services needing to be tailored (Westergaard, 2012) and counsellors not integrated into schools (Prior, 2012).
By viewing participants’ experiences and suggestions for service improvements through a complex systems lens, a system-focused model of counselling services has been developed that considers how services could be optimised within the socially complex and dynamic context of schools and the wider education system. The model engages with complex systems thinking by conceptualising counselling sessions as part of a wider system (Moore et al., 2019). This means that counselling and the complex system in which it is embedded need to be seen as interdependent, and system structures, processes and relationships need to be in place from the outset to ensure that counselling functions successfully (Hawe et al., 2009). Without a clear systems approach that essentially treats the wider system as an inextricable part of the counselling model, the implementation issues reported in the evidence-base will likely continue and sustainable delivery will not be achieved (Copeland et al., 2024).
Implications for policy and practice
For the proposed model to have traction in Wales, and the UK more broadly, its implementation needs to be harmonised with existing policy and practice. The widespread advocacy of whole-school approaches to mental health is potentially helpful, as there are shared principles between the complex systems thinking embodied in the optimised model and whole-school approaches to mental health. In Wales, for example, all maintained schools are expected to implement a whole-school approach to mental wellbeing (Welsh Government, 2021). Several elements of the model map directly onto this whole-school approach, including the provision of universal and targeted mental health support, mental health training for all staff, leadership and staff wellbeing. In addition, schools are expected to develop collaborations with external service providers, such as counselling services. This context provides an opportunity for successful implementation of the model.
Implications for future research and evaluation
An evaluation of the proposed model would strengthen the counselling evidence-base. Such an evaluation should follow established methodological guidance on evaluation of complex interventions (Skivington et al., 2021) and would ideally be conducted at two levels. First, at the individual level work should be undertaken to assess the impact of the direct work that a counsellor undertakes. A mixed-method evaluation with a qualitative component could capture children and young people’s experiences of their whole counselling journey and provide rich data to further stakeholders’ understanding of issues such as awareness and stigma (Palinkas et al., 2011). It might also bring to light examples of how to normalise counselling and encourage children and young people to consider it as an option for support.
Second, at the system level, there is a need for an evaluation that assesses the impact of the whole education system counselling service. Such an evaluation is important as it evaluates the model as a whole and would capture the elements of the complex system that influence mental health outcomes, as well as any unintended consequences across the system (Moore et al., 2019; Rutter et al., 2017). A qualitative process evaluation with a system-focused perspective could be important here to capture implementation of the model and the factors that facilitated and impeded implementation (Moore et al., 2015).
Strengths and limitations
This study benefits from the participation of a wide range of stakeholders and staff and pupils. A diversity of perspectives on school- and community-based counselling services was therefore included. However, while children and young people who had experience of counselling participated, not all talked directly about their experiences. This may have been a consequence of the small group interview format or of conducting the interviews online. Developing rapport with interviewees is harder with the online format and for safeguarding and technical support purposes, a member of school pastoral staff was with the pupils. Furthermore, numbers in some of the consultation groups were low, particularly primary school-aged children, care-experienced young people and parents. It is therefore possible that these groups’ experiences and range of views were not fully captured in the data.
One case study primary school withdrew from the study due to the COVID-19 pandemic and one secondary school could only offer one manager interview. This reduced variation in school contexts and meant that no pupils from a Welsh-medium secondary school participated.
Conclusion
This study identified a number of issues with local authority school- and community-based counselling services and ideas for service optimisation. These centred on the approach and delivery of counselling sessions; the integration of counselling services into universal mental health provision; and the complex whole education system as the context for counselling service implementation. The findings have been translated into a complex system-focused model of an optimised counselling service. The model offers an opportunity to improve counselling service outcomes and sustainability by increasing the likelihood they will become sustainably embedded in the whole education system.
Footnotes
Acknowledgements
The authors thank study participants and school staff, together with staff from the children, young people, parent and carer organisations who helped organise data collection. They also extend their thanks to members of the research team: Simone Willis, Helen Morgan, Nick Page, Matt Davies, Peter Gee and Joan Roberts.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by the Welsh Government. The Centre for Development, Evaluation, Complexity and Implementation in Public Health Improvement (DECIPHer) is funded by Welsh Government through Health and Care Research Wales. The study was also supported by the Wolfson Centre for Young People’s Mental Health, established with a grant from the Wolfson Foundation. Both DECIPHer and the Wolfson Centre are based at Cardiff University.