
Abstract
Objective:
To examine experiences of anti-Indigenous racism in a Canadian medical school and inform the development of critical and action-oriented Indigenous health education necessary to pave the way for reconciliation within health systems.
Design:
A qualitative study conducted within a constructivist paradigm which involved (1) semi-structured interviews with students, faculty and staff at a Canadian medical school and (2) consensus-building/collaborative analytical sessions with an Indigenous advisory group and a non-Indigenous working group.
Setting:
Twenty-three semi-structured interviews were completed with students, staff and faculty working across a Canadian medical school.
Results:
Inductive coding generated 211 codes that were grouped into seven overarching thematic domains. By engaging in an iterative dialogue with the advisory and working groups, we deductively aligned the thematic analysis with faculty-level and institution-level Indigenous education strategies to ensure local relevance. Self-reflective statements were developed with the advisory group to guide areas for action and resulted in 18 statements with five-point Likert-type-style response options.
Conclusion:
The results of this study suggest that promoting self-reflexivity in health professional education can prompts educators to engage with Indigenous health curriculum and pedagogy; mentorship and role modelling; and accountability. Critically evaluating systemic injustices at an individual level enables educators to resist systemic oppression and create change in the spaces where they work.
Introduction
Anti-Indigenous racism is one of the insidious effects of colonisation (Crowshoe et al., 2019). The 2015 Truth and Reconciliation Commission of Canada: Calls to Action (TRC; Truth Reconciliation Commission of Canada [TRCC], 2015) acknowledges that the health disparities experienced by Indigenous peoples are due to colonisation and government policy. The resulting gaps in health outcomes between Indigenous and non-Indigenous populations are a product of intertwined structures, power imbalances that reinforce social vulnerabilities, unfair distribution of economic and political goods and refusal to recognise or challenge the mechanisms and ideologies that target Indigenous peoples (Czyzewski, 2011). Moreover, research has evidenced that anti-Indigenous racism within Canadian healthcare systems is operationalised between and across multiple levels (Allan and Smylie, 2015; McLane et al., 2022; Roach et al., 2022, 2023; Turpel-Lafond, 2021). Repeatedly, health service providers overlook, deny or disregard the distal determinants of health of Indigenous people as well as the structural barriers they endure (Czyzewski, 2011). Health professionals uphold the legacy of colonisation through active (mistreatment, racism, negligence), passive (social contexts and structural barriers lack of recognition) or combined practices (historical context contempt and traditional culture discouragement; Crowshoe et al., 2019). These systemic, institutional and personally mediated/interpersonal (Jones, 2000) manifestations of racism damage the relationship between Indigenous people and health care systems, exacerbate mistrust, deter Indigenous patients from seeking care and negatively impact Indigenous patient satisfaction with treatment (Ben et al., 2017).
Many public sector local, provincial and federal systems across Canadian society (e.g. health, education, child and family services) have recently made initial statements and attempts to confront and mend the atrocities Indigenous people have faced as a result of colonialism (Department of Justice Canada, 2018; Government of Manitoba, 2022). Critical and action-oriented education on Indigenous health is necessary to pave the way for reconciliation within health systems. The TRC Calls to Action numbers 23 and 24 (TRCC, 2015), and the National Inquiry on Missing and Murdered Indigenous Women and Girls (MMIWG, 2019) Call for Justice 7.6 provide important guidance on how to implement critical Indigenous health education. These calls demand that education on Indigenous health is focused on closing health gaps, tackling inequity, and ensuring Indigenous people’s holistic well-being to address the effects of intergenerational trauma and colonisation.
The work we describe in this paper, in conjunction with other ongoing Indigenous-led initiatives, actively strives to construct and maintain ethical space for engagement in reconciliation (Ermine, 2007) and to embed structural competency within health education (Metzl and Hansen, 2014). The aim of the work was to identify and understand the experience with Indigenous heath education within a medical school; as well as to identify action-oriented strategies in medical educational contexts to push forward systems-level change for Indigenous health.
Methods
Design and recruitment
This Qualitative Consensus (Chatwood et al., 2015) study was undertaken using a constructivist paradigm (Lincoln and Guba, 1985). It had two main components: (1) semi-structured interviews with students, faculty and staff at the Cumming School of Medicine (CSM) in Calgary, Alberta, Canada, and (2) consensus building/collaborative analytical sessions with an Indigenous advisory group and a non-Indigenous working group – two groups that met both independently and together.
Purposive and snowball sampling was used to recruit participants for semi-structured interviews via departmental newsletters and emails. The same approach was used to contact, screen and recruit the advisory and working group members. The inclusion criteria for the semi-structured interviews were fluency in English and affiliation to any programme within the medical school. The working group inclusion criteria were similar, but individuals also had to have familiarity with Indigenous health or anti-racism education. The advisory group inclusion criteria were to self-identify as Indigenous and have an interest in education.
All interview and advisory group participants were compensated with honoraria; working group participants received a gift card for a coffee shop as a thank you for their time. Interviews were completed virtually using Zoom. Interview recordings and verbatim transcriptions (transcribed by AR) were stored on a secure institutional shared drive. NVivo software was used to manage the interview data. Field notes from the interviews and the group meetings were recorded in a reflexive journal and shared with the study team during peer debriefing sessions.
The project was approved by the University of Calgary Conjoint Health Research Ethics Board (REB20-0244). We adhered to Tri-Council guidelines for research involving First Nations, Inuit and Métis participants, and the project also had Indigenous and allied non-Indigenous leadership.
Data collection
Interview participants included medical school faculty, staff and students from departments including health sciences research and education. Semi-structured interviews were used to explore specific domains while identifying emerging themes and engaging participants in a dialogue that facilitated in-depth understanding of their experiences (Truong et al., 2016).
The interview guide was constructed by incorporating empirical and theoretical insights from the study team and Indigenous health experts. It included five critical areas to be explored: (1) participant’s context, identity and role or position within CSM; (2) perceptions of Indigenous education available within the CSM; (3) knowledge or experiences of engaging with anti-racism at CSM; (4) witnessing or encountering racism; and (5) experiences of Indigenous health education.
Chronologically, we alternated advisory and working group sessions with the explicit goal that the advisory group guided the work so as to ground it in Indigenous community priorities and Ways of Knowing. The working group discussed the implementation of the advice received from the advisory group in a medical school context. Individually, the advisory and working group sessions utilised a discussion group approach (Doria et al., 2018), whereas the joint session between them followed caucus guidelines (Watson et al., 2020).
Data analysis
Reflexive thematic analysis was used to analyse the qualitative interview data (Braun and Clarke, 2019). This approach utilises a six-step process beginning with data familiarisation and the use of a deductive and inductive approach to predict and understand findings (Fereday and Muir-Cochrane, 2006). Initial codes or thematic units were generated by an inductive process, allowing for in-depth understanding of participants’ knowledge, perceptions and experiences in relation to Indigenous health, racism, colonisation and oppression with the educational context. Through an iterative process, researchers searched for, reviewed and defined themes (Braun and Clarke, 2019). This process informed the development of a final codebook. A deductive approach then entailed exploration of the data set using these codes (Neuendorf, 2017). Coding and analysis were led by AR with verification and double coding undertaken by PR. Discrepancies were brought to the wider research team for discussion and resolution. Memos were created throughout the analytical process, which involved regular peer debriefing, confirmation and discussion with the advisory and working groups as described above. The advisory and working group sessions were community-led processes of data analysis and knowledge translation with continuous member checking. We shared the results of our analysis with both groups and their insights guided subsequent analyses. Group feedback and recommendations were incorporated in distinct ways: (1) we created codes for identifying specific concerns or content; (2) we attached analytical memos to specific content to further explore nuances in the data; and (3) we used annotations to map our findings onto the directives, policies or reports that the groups recommended (Henderson et al., 2023; MMIWG, 2019; University of Calgary, 2017). In the joint advisory/working group session, both groups assessed the output of the overall analysis.
Findings
Participation and involvement
Twenty-three semi-structured interviews took place between August 2020 to February 2021; interviews ranged from 45 minutes to 1.5 hour in length. One interview took place over two meetings, the remainder were all completed in one session. See Table 1 for a description of participant demographics.
Semi-structured interview participant demographics.
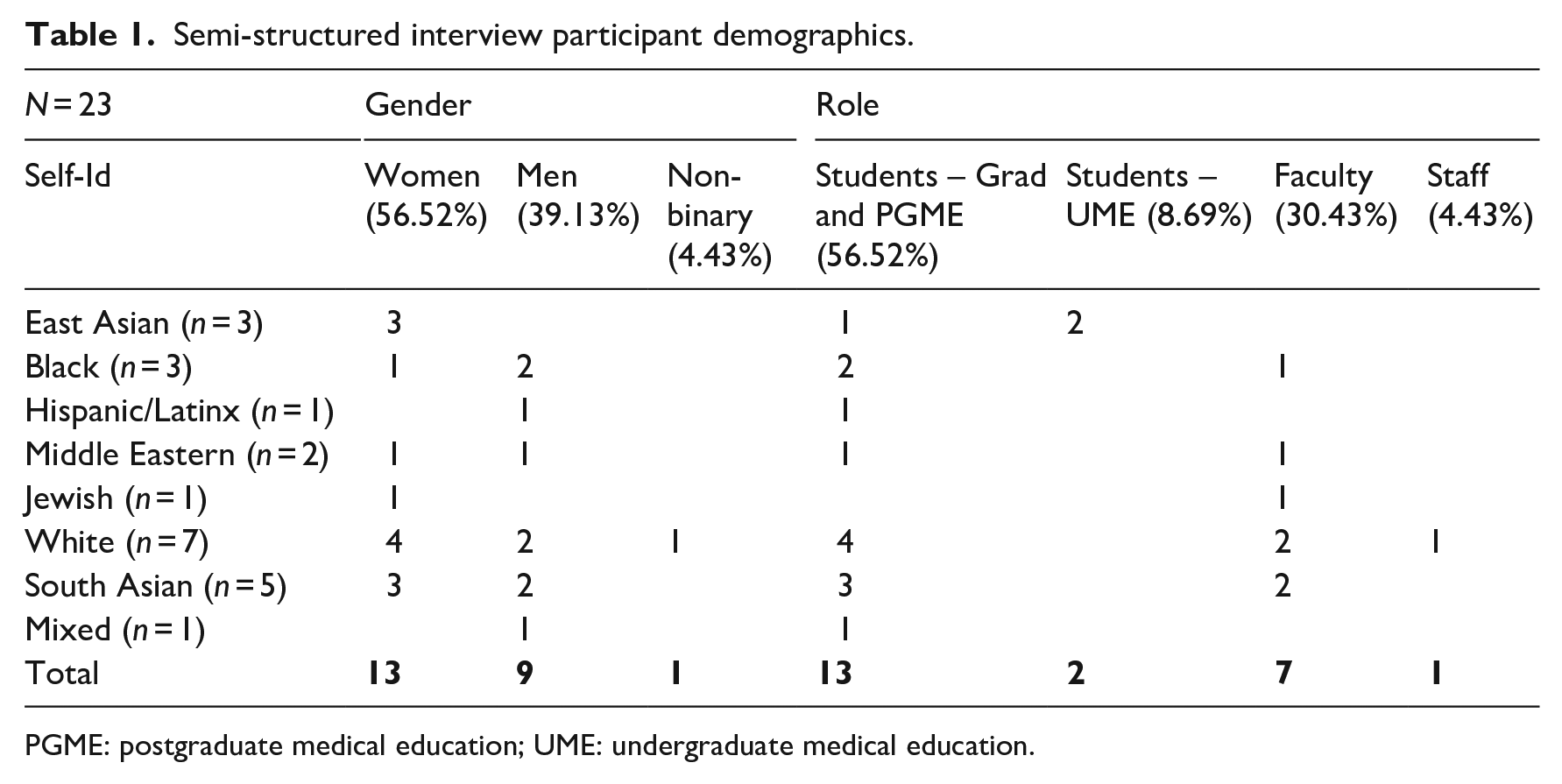
PGME: postgraduate medical education; UME: undergraduate medical education.
The advisory group included six Indigenous community members: one Elder, one health professional, two students and two community educators/activists. The working group included four members of medical school faculty, one student and one staff member. We held two sessions with each group and one joint session with both groups. In the first advisory group session, we presented the preliminary findings and analysis from the semi-structured interviews. The members shared their insights and signalled relevant themes including directions to continue exploring in the analysis. Figure 1 provides an outline of the study flow and process.
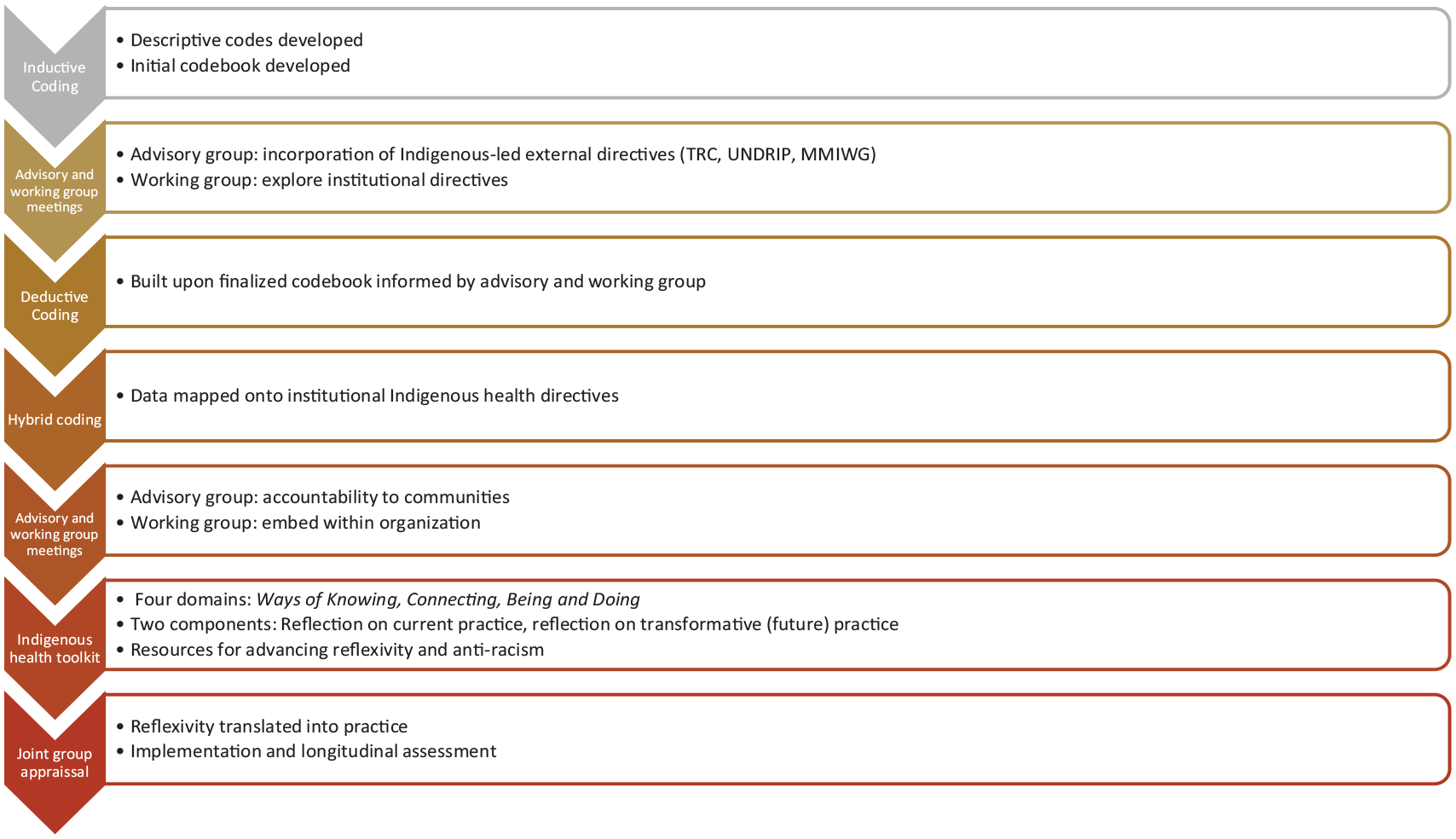
Study flow and process.
Coding and theme development
Initial inductive coding produced 211 codes. These codes were grouped into seven overarching thematic domains: (1) barriers and challenges to implementing anti-racism education; (2) characterising Indigenous health equity within health sciences education; (3) envisioning anti-racism: implementation and institutional considerations; (4) experiencing or witnessing racism, oppression and discrimination; (5) Indigenous health education: gaps and challenges; (6) understandings of Indigenous contexts, health and history; and (7) understandings of race and racism. The inductive analysis identified contexts, mechanisms and nuances in the data set and identified affinities, concerns and specificities between participants both individually and within groups.
We brought the inductive codes to the first advisory group meeting for feedback where the group directed the team to look to Indigenous-led recommendations (MMIWG, 2019; TRCC, 2015). After incorporating the advisory group recommendations, we then held the first session with the working group. During this session, the members reflected on the analysis up to that point. In the second advisory group session, members focused on actionable and accountable ways of implementing Indigenous-specific anti-racism education, including critically needed ways for educators to gain the skills they need to effectively engage with teaching Indigenous health curricular content when their own education had not prepared them to do so.
The second session with the working group focused on the implementation of Indigenous health education within the medical school. Group members identified potential spaces and mechanisms in which to implement actionable and skills-based education for Indigenous health. Following advisory and working group recommendations, we explored existing initiatives and scholarly work on Indigenous health and anti-racism. Internal directives and strategies for Indigenous health together with the University of Calgary’s Indigenous strategy ii’taa’poh’to’p (University of Calgary, 2017) provided context and specific strategic goals and actions for local implementation.
Through an iterative dialogue between the advisory and working groups informed by the reflexive thematic analysis, we deductively mapped findings from the thematic analysis on to the Indigenous Health Dialogue at faculty level (Henderson et al., 2023) and ii’taa’poh’to’p at institution level to ensure that this work was aligned with institutional actions to address the TRC Calls to Action. The Indigenous Health Dialogue was a process in which extensive community engagement created an understanding of how the Truth and Reconciliation Calls to Actions could be operationalised within the CSM. Undertaking this mapping ensured our data connected to four domains of the Indigenous Health Dialogue relevant to teaching and pedagogy: namely, (1) recognising Indigenous Health as a distinct discipline, (2) promoting and supporting Indigenous inclusion, (3) innovating in Indigenous health education, and (4) and addressing institutional barriers to advancing Indigenous health and reconciliation (Henderson et al., 2023).
Indigenous Health Dialogue Domain: recognising Indigenous health as a distinct discipline
Thematic domains:
Characterising Indigenous health equity and anti-racism within health sciences education
Understandings of Indigenous contexts, health and history
Indigenous peoples’ determinants of health are historically, culturally and politically unique and it is fundamental to understand the distinct drivers of Indigenous health (Czyzewski, 2011). Participants stated that learning about Indigenous health requires unlearning racism and other legacies of colonisation. One interview participant shared that it is necessary to continue ‘exploring, unpacking and sort of learning and unlearning some of the racism that we harbour . . . because a lot of it is because for generations, we’ve taken classes to get citizenship. So, we learn all the wrong things there’ (Graduate Student A-11). Interview participants acknowledged that as non-Indigenous individuals, they could not define what or how Indigenous health as a discipline should be structured, and recognised the need for Indigenous self-determination. They also acknowledged that non-Indigenous students and faculty need to centre accountability and not ‘share their experience or share their thoughts if we do not have a purpose for sharing those’ (Undergraduate student A-2). Most importantly, participants suggested that educational programmes and institutions ought to engage in action-oriented process and mechanisms to nurture institutional, interpersonal and individual accountability to create and contribute to safe, anti-racist spaces.
Indigenous health dialogue domain: promoting and supporting indigenous inclusion
Thematic domains:
Envisioning anti-racism: implementation and institutional considerations
Current lack of Indigenous health curricular content across all programmes in the medical school was commented on in all of the interviews. While some departments had implemented Indigenous-led courses or Indigenous health-specific lectures, most reported anti-oppressive education was self-directed and individually sourced. Some student interview participants described how health equity, and social or structural determinants of Indigenous health were topics that many of their peers were resistant to. A member of faculty reported hearing students say, ‘You’re just forcing your leftist, social justice views on me. And that’s not the view that I have’ (Faculty A-1). A graduate student identified how ‘with white fragility, sometimes being confronted with content that isn’t implicitly focused on white people can feel like a threat in itself’ (Graduate student A-9).
These findings imply that for privileged groups within medicine, de-centring their voices may be perceived as ‘oppression’, since they have never experienced intersectional discrimination. Participants also stated that greater Indigenous representation within academic leadership was necessary, highlighting the urgent need to address barriers to admission for Indigenous students and trainees and barriers to hiring for Indigenous members of faculty. Faculty members expressed that Indigenous-specific anti-racism education should be ‘integrated and part of a curriculum so that people come out with clear understanding, with tools on how to manage and deal with it and clear pathways on how to call it out when it is happening’ (Faculty A-2). Throughout the medical school, lack of Indigenous engagement at a curriculum-design level has resulted in white-centred and limited Indigenous health narratives that portray Indigenous people primarily as a historical population without consideration of modern contributions and inclusion.
Indigenous health dialogue domain: addressing institutional barriers
Thematic domains:
Experiencing or witnessing racism, oppression and discrimination
Barriers and challenges for implementing anti-racism education
Interconnecting initiatives at institutional and community levels amplify the voices of anti-racism educators, provide role-modelling opportunities for Indigenous and non-Indigenous students, promote safety networks for marginalised groups and demonstrate institutional commitment to Indigenous health and health equity.
According to one member of faculty, genuine commitment was defined as being ‘...able to support this minority group to make sure they thrive, succeed and honestly saying that we don’t tolerate racism, so it is not just somebody in power saying it . . . to raise it as a faculty and say, this comes before anything else.’ (Faculty A-3)
Indigenous health education in medical schools has the dual task of addressing educational gaps and challenging colonial systems, bias and stereotypes. Participants felt the role of non-Indigenous students and faculty begins with amplifying Indigenous voices. Non-Indigenous participants emphasised that amplification of Indigenous voices includes ‘. . . making sure that Indigenous voices are heard, making sure every department has at least a minimum number of Indigenous people’ (Graduate Student A-10).
In addition, participants suggested incorporating mandatory anti-racism education, a minimum expected level of foundational knowledge for students, staff and faculty, and embedding Indigenous-specific ways of knowing and doing throughout every programme at the CSM.
Indigenous health dialogue domain: innovating indigenous health education
Thematic domains:
Indigenous health education: gaps and challenges
Understandings of race and racism
Participants identified that apart from the limited Indigenous health curricular content they were exposed to, the pedagogical approach adopted in the medical school was mostly didactic in nature. Not only was this approach misaligned with Indigenous ways of doing, but it failed to provide the opportunity for participation in the critical engagement and skills-based learning needed to counter cognitive dissonance between what is being taught about and how it is experienced. Participants acknowledged that this approach could be useful for providing baseline knowledge, but multidisciplinary teams, flipped classroom scenarios and role modelling allowed them to learn ‘a lot more on the ground and getting your feet wet and addressing problems as they present themselves, and actually, trying to do things practically’ (Graduate student A-4).
They described that, broadly speaking, the current course content on health equity was like learning definitions from a textbook. The challenge for most participants lay in incorporating this learning into their research and practice. Participants also emphasised the lack of longitudinal assessment or follow-up, and also the fact that the Indigenous health-related education that was available tended to happen in silos (Hartwell et al., 2017).
Participants also felt that any kind of educational strategy, either curricular or extra-curricular, should aim to be transformative and target systems- and policy-level change. They noted that providing education without addressing power imbalances was like doing ‘anti-racist work without going to the root of the problem’ (Graduate Student A-9).
Constructing an action-oriented tool for educators
The mapped analysis was shared with the Indigenous advisory group and the non-Indigenous working group. The advisory group emphasised the need for action-oriented outcomes from this work and the working group highlighted the need for tools that were relevant for use in many different educational contexts. With this encouragement, the research team integrated the elements discussed and drafted a toolkit to promote self-reflexivity, interpersonal action and institutional accountability. To align this work with the larger vision of ii’taa’poh’to’p, work to create action-oriented domains was undertaken using the visionary circles described in this strategy in relation to ways of connecting (through mentorship and role modelling), ways of knowing and doing (in terms of curriculum and pedagogy) and ways of being (in relation to accountability).
The thematic domains produced through the qualitative reflexive thematic analysis were discussed with both groups to reach consensus on the actions that could address each of the areas described above. Self-reflective statements were developed with the advisory group to guide areas for action and presented to the working group to determine their relevance to medical educators and the feasibility of implementation. These consensus-based discussions resulted in 18 statements with a five-point Likert-type style response options, and an individual reflection section to guide improvement and the development of future learning objectives (see Table 2). Six statements were identified within each of the following areas: ways of connecting, ways of knowing and doing, and ways of being that were positively framed and action oriented.
Indigenous health individual reflective tool for educators.
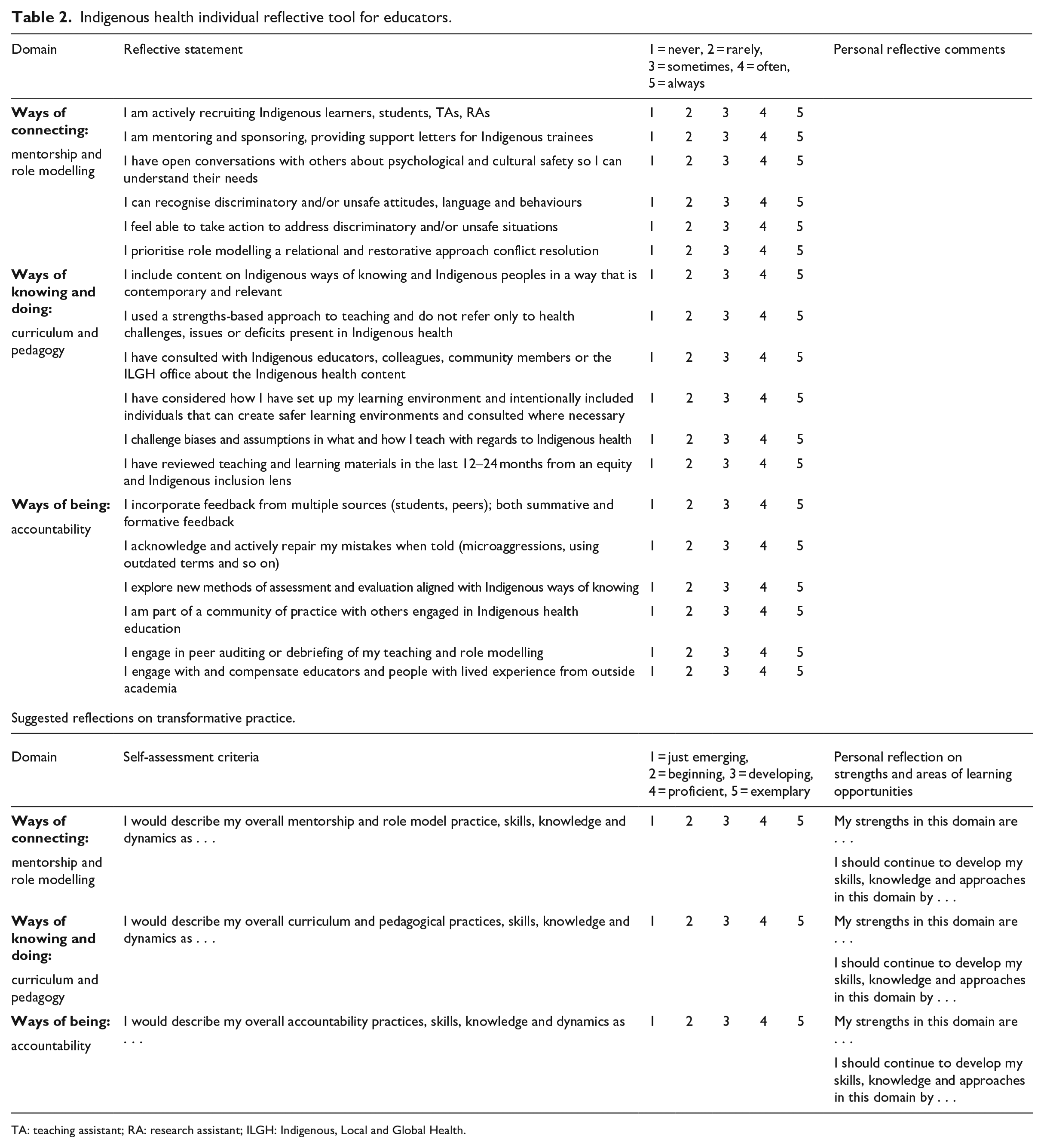
TA: teaching assistant; RA: research assistant; ILGH: Indigenous, Local and Global Health.
Each statement provides individuals with a way of assessing their own perceived competency and skills but accounts for the possibility of unfamiliarity with the vocabulary used in the statements. Change over time can be tracked if the tool is used repeatedly and reflective notes can be made to provide context or explanation for one’s own self rating. A self-rating score is also included on each of the three areas for overall rating of ability to contribute to transformative educational practice. A compiled list of institutional and external educational resources will be made available as a companion document to aid self-directed learning when the tool is published and then implemented into practice. A joint group session between working and advisory group members was held to present and discuss the tool, and to reach consensus on implementation, curricular content and outcome assessment. Members of both groups provided pragmatic, theoretical and operational insights, and agreed on the final version to use for future piloting and implementation.
Discussion
In this study, all participants recalled experiencing or witnessing racism in the medical school, noted a lack of representation of Indigenous staff, students and faculty, and had experienced limited Indigenous health curricular content. Throughout the analysis, it became clear that participants felt that Indigenous-specific anti-racism education must be accountable not only to learners, but also to educators and to the community. Indigenous faculty are under-represented in higher education and are, therefore, at risk of being tokenised and experiencing anti-Indigenous racism in teaching environments. It is critical when implementing anti-racist curriculum and pedagogy to aim at reducing these risks and the potential for such individuals to experience harm. Focusing on safety structures in interpersonal interactions and within learning spaces to create change also needs to be supported and resourced by university leadership (Jones, 2000).
Dismantling bias and confronting the colonial core foundations of Canadian higher education and the health system will come with denial, discomfort and guilt, which if not addressed will likely result in stagnant attitudes, knowledge and behaviours (Snider, 2020). Lack of accountability will continue to enable unsafe (racist, misogynistic, classist and oppressive) faculty by maintaining the priority on white-centred Indigenous health and health equity education (Denis, 2007). This type of education is often deficit-focused, with an emphasis on saviourism, which positions non-Indigenous staff, students and faculty as external to the racist systems that they knowingly or unknowingly perpetuate (Nixon, 2019).
Accountability, as praxis, a theoretical construct, an organisational process and a higher education approach, needs to be integrated into all aspects of the educational setting (Noltemeyer and Grapin, 2021). Thus, it is important we do not compartmentalise our strategies in health professional education but instead take a holistic approach to advancing critical Indigenous health education. The development of a reflective tool that prioritises responsibility, transparency and action fosters the capacity for creating change (Snider, 2020). A shared responsibility for accountability embeds health equity in professional practice and curriculum development. An Indigenous-specific anti-racism tool strengthens the scope of existing initiatives by encouraging reflection. A self-monitoring instrument creates opportunity for self-awareness, helping individuals identify (un)intentional (un)safe behaviours and process discomfort, guilt and fragility in a proactive way (Snider, 2020), rather than a reactive one.
But Indigenous health educational reflective tools, and anti-racism toolkits are not a panacea. Institutional practices including existing initiatives, the funds allocated to Indigenous equity, anti-racism or anti-oppression, and senior leadership engagement or disengagement with the goals of such work influence what is actually achievable (Ricks et al., 2022). The additional complexities of social and geo-political location and the availability of ethical space (Ermine, 2007), accompanied by an accountable and safe faculty, shape the possibilities for equitable environments in higher education. (Denis, 2007; Snider, 2020). The reflective tool we co-designed seeks to promote reflection across each of these spheres. Impact and intentionality, action and inaction, engagement and apathy, and other elements along the justice–injustice continuum influence educational and equity outcomes. Implicit or explicit silences and stances model behaviours, and future professional practice and environments. Integrating an instrument that encourages reflections on ethical Indigenous inclusion within health professional education prompts educators to engage with Indigenous health curriculum and pedagogy (through ways of knowing and doing); mentorship and role modelling (through ways of connecting); and accountability (through ways of being).
Anti-oppression interventions, initiatives or strategies must also take into account the character of specific disciplines and fields; particularly those (such as some forms of ‘hard’ science that assume a disconnect from social issues. Constructing reflective statements that incorporate institutional specific language offers a welcoming and familiar approach with which to engage learners who may be at different places along a learning continuum (Ricks et al., 2022; Snider, 2020). Often the basic sciences and applied sciences, which historically have disguised bias and prejudice as legitimate ‘scientific knowledge’, lack curricula focusing on the relationships that these fields have had with different forms of oppression (Hoberman, 2007). A reflective tool, used in conjunction with anti-racism education and training, offers a transdisciplinary form of engagement. Individuals can reflect on their strengths and present gaps to create a baseline, access resources and engage with Indigenous health education, either individually or collectively. The aim of non-confrontational tools such as this is to reduce reluctance or reactivity that is often directed at Indigenous students, staff and faculty in learning environments (Denis, 2007). Reflective instruments can also serve a secondary purpose by connecting socio-political and historical circumstances to bio-medical understandings of diseases, which may be more effective in creating change in basic and applied science contexts.
Limitations
There are limitations to this study. Most notably, our work provides an in-depth understanding of present and future practice in only one medical school in Canada. There is evidence, however, that the challenges faced in this medical school are present in all Canadian medical schools when it comes to Indigenous representation and inclusion. This situation is not only recognised by the TRC Calls to Action (TRCC, 2015), but also by the creation of the National Consortium for Indigenous Medical Education (NCIME: https://ncime.ca/), which aims to catalyse efforts across Canada to provide guidance and resources to strengthen Indigenous medical education initiatives.
Another limitation to the work stems from the fact that the semi-structured interviews took place with participants who were fluent in English. Given ongoing conversations about racism and oppression, and perception of Indigenous health education, the inclusion of non-English speakers may have added an important lens to the work to expand the understanding of experiences of oppression. Future work will endeavour to be more broadly inclusive and allocate resources for translation facilities.
Finally, although the tool developed in this study was intended for use at an individual level, further work is currently planned to implement and pilot the tool to understand how it may be adapted to a unit/department/faculty context. We recognise that at an individual level the tool may have limits in affecting systems-level change, but given there exist few spaces for reflecting upon Indigenous health and anti-racism skills within higher education, we need to begin somewhere and collective individual level reflection in the short term may lead to systems-level change in the long term.
Conclusion
By creating space to critically evaluate systemic injustices at an individual level and those in our close social and professional environments, we become able to resist the systemic oppression present in the higher education and medical education systems and identify structures through which we can create change in our own spheres of influence. A developmental process such as that described in this paper, followed by the design and preparation of a reflective tool that targets accountability and implementation, can add momentum to integrating longitudinal and skills-based Indigenous health and anti-racism education into the medical school curriculum. Medical schools in Canada have a mandate to train physicians and health leaders to meet the needs of the populations they serve and to do this in an equitable, anti-racist and socially just way. Our work helps contributes to the nascent literature, which provides educators with tools to work towards this shared future of equitable health outcomes for all Indigenous people.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the authors received financial support from the Office of Health & Medical Education Scholarship (OHMES) at the Cumming School of Medicine for the research, authorship and/or publication of this article.