
Abstract
Background:
School-based sleep education programmes can promote the importance of sleep health and may improve adolescent sleep. To date, only limited research has examined the feasibility of integrating sleep programmes into the school curriculum.
Objectives:
This study evaluated the feasibility, acceptability and preliminary efficacy of the Strathclyde intervention to encourage good sleep health in teenagers (SIESTA).
Methods:
A total 171 students (12–15 years, 53% women) from secondary schools in Scotland participated in the study. Recruitment and retention, data collection and design procedures were assessed to establish feasibility. Qualitative feedback on acceptability was collected via focus group discussions. Outcome measures assessing insomnia symptoms, sleep hygiene, depression, anxiety and stress were completed at baseline and post-intervention to explore the preliminary effects of SIESTA.
Results:
All schools that were approached consented to participate, and most students completed assessments at both time points (171) with a dropout rate of 5%. Assessment measures provided sufficient data to compare baseline and post-intervention values. Training and delivery manuals ensured successful delivery of the programme. Qualitative feedback indicated SIESTA was acceptable, and students spoke favourably about the content, delivery and techniques. Students reported that SIESTA was age-appropriate, relevant and the techniques were beneficial. There were significant improvements in insomnia and stress, but no improvements were noted for sleep hygiene, depression or anxiety.
Conclusion:
The findings suggest that SIESTA is feasible and acceptable for delivery via the school curriculum. The results indicate that a controlled trial is required to further investigate the efficacy of SIESTA implemented in an educational context.
Introduction
Guidelines recommend that young people aged 14–17 years sleep for 8–10 hours per night for optimal functioning (Hirshkowitz et al., 2015). However, research demonstrates that less than half achieve at least 8 hours (Hysing et al., 2013; Jakobsson et al., 2019) and consequently, the majority of adolescents may be chronically sleep deprived (Alfonsi et al., 2020). Research has suggested that up to 40% of adolescents experience symptoms of insomnia (including difficulties with sleep onset/maintenance and dissatisfaction with sleep quality) and more than 20% meet diagnostic criteria (Chung et al., 2014; Espie and Kyle, 2012; Hysing et al., 2013). The Perfect Storm Model proposed by Carskadon (2011; Crowley et al., 2018) illustrates how biological and psychosocial changes during adolescence affect sleep. Specifically, a delay in sleep timing (by around 1–3 hours) results from Circadian rhythm alterations, slower accumulation of sleep pressure, increased autonomy over bedtimes, social pressure and academic demands (Carskadon, 2011; Crowley et al., 2018; LeBourgeois et al., 2017). These factors combined with early school start times, create a Perfect Storm for adolescent sleep deprivation (Carskadon, 2011).
Insufficient, poor-quality sleep during adolescence has been associated with increased emotional reactivity, mental and physical ill health, poorer cognitive functioning and impaired academic performance (Beebe et al., 2010; Goldstein and Walker, 2014; McGlinchey et al., 2017; Mitchell et al., 2013; Titova et al., 2015). Adolescence is a key developmental stage for establishing health-related habits (Pound and Campbell, 2015; WHO, 2022), so is an opportune stage to initiate sleep health interventions that may also improve mental health and academic performance (Chung et al., 2017; Rydzkowski et al., 2015). A study conducted in Hong Kong by Chung and colleagues (2014) reported that 22% of adolescents with insomnia symptoms sought help from family and friends, although formal help-seeking behaviours were limited. The authors suggested that school-based programmes could increase knowledge of sleep problems and awareness of treatment options.
In recent years, a universal approach to improving adolescent sleep, via school-based sleep education programmes, has received notable attention among sleep researchers (Chung et al., 2017; Rigney et al., 2021). School-based programmes are useful for disseminating evidence-based programmes to large groups in a systematic way via the school curriculum (Chung et al., 2017). The advantages of school-based sleep education programmes can be twofold, by universally promoting the maintenance of good sleep health and by improving disordered sleep in those who report problems (Bauducco et al., 2020; Gruber, 2013).
Commonly, school-based programmes utilise sleep education information combined with cognitive-behavioural strategies to encourage behaviour change (Cassoff et al., 2013; Egbegi et al., 2021). Cognitive-behavioural therapy for insomnia (CBT-I) is a multi-component approach comprising sleep hygiene, stimulus control, sleep restriction, cognitive techniques and relaxation training, and is the recommended treatment for insomnia disorder (American Academy of Sleep Medicine, 2014), including in adolescents (Dewald-Kaufmann et al., 2019). Research has demonstrated that cognitive-behavioural techniques can significantly improve adolescent sleep (Blake et al., 2017, 2018), while good sleep hygiene serves as a protective factor (Bartel et al., 2015). Therefore, this dual approach can be beneficial for individuals who are already experiencing poor sleep, by delivering evidence-based tools that can be implemented to improve sleep. In addition, the preventive elements can educate and encourage the maintenance of lifelong healthy sleep practices.
With the growing popularity of school-based sleep education programmes, several reviews have been conducted exploring the effectiveness of such programmes (Blake et al., 2017; Blunden et al., 2012; Chung et al., 2017). Outcomes suggest that sleep-education programmes are effective for improving sleep knowledge but have shown limited sustained improvements on sleep behaviour (Blunden et al., 2012; Chung et al., 2017; Gruber, 2013; Rigney et al., 2021). However, some research has reported improvements to sleep were maintained up to 1 year following a school-based sleep (Rey et al., 2020; Wolfson et al., 2015). Furthermore, Bauducco et al. (2020) investigated the long-term preventive effects of a school-based sleep programme in Sweden and found that adolescents who completed the intervention were less likely to report insufficient sleep (<7 hours) 1 year later, compared to controls.
There has been limited research, however, investigating how to integrate school-based sleep education programmes into the existing health and wellbeing school curriculum as a universal approach (Davis et al., 2022). Instead, many programmes implemented as stand-alone or targeted interventions for those already experiencing poor sleep (Bei et al., 2013; Egbegi et al., 2021; MacLeod and Taylor, 2013). Cassoff et al. (2013) highlighted that feasibility research is key for integrating programmes into the curriculum to ensure interventions are acceptable and feasible for delivery to adolescents. In Scotland, health and wellbeing is a key target area within the Curriculum for Excellence, delivered within the Personal and Social Education (PSE) curriculum (Scottish Government, 2019). Despite the significant detrimental consequences of insufficient sleep in adolescence, sleep is entirely absent from the PSE curriculum. There has been no systematic delivery and/or investigation of an evidence-based sleep education programme in Scottish schools. Therefore, the aim of this study was to investigate the feasibility, acceptability and preliminary efficacy of delivering Strathclyde Intervention to Encourage good Sleep health in TeenAgers (SIESTA) in Scottish Schools as part of the PSE curriculum. The findings of this study will inform future decisions about the wider dissemination and evaluation of SIESTA.
Methodology
Participants
Secondary school pupils from four schools in Scotland were recruited to participate in the study between January 2020 and January 2021. Schools were located in four local authority areas, representing varied socio-economic status backgrounds. Teachers identified classes within the S1–S3 year groups (age 12–15 years) to participate in the study, based on timetabling constraints and convenience. As this was a feasibility study, we did not conduct a priori sample size calculation (Julious, 2005).
Design
To determine feasibility, recruitment and retention, data collection and design procedures were assessed. Qualitative feedback was used to assess acceptability and primary (insomnia symptoms) and secondary outcomes (sleep hygiene, screen use, symptoms of stress, anxiety and depression) were collected at baseline and post-intervention.
Materials
Intervention
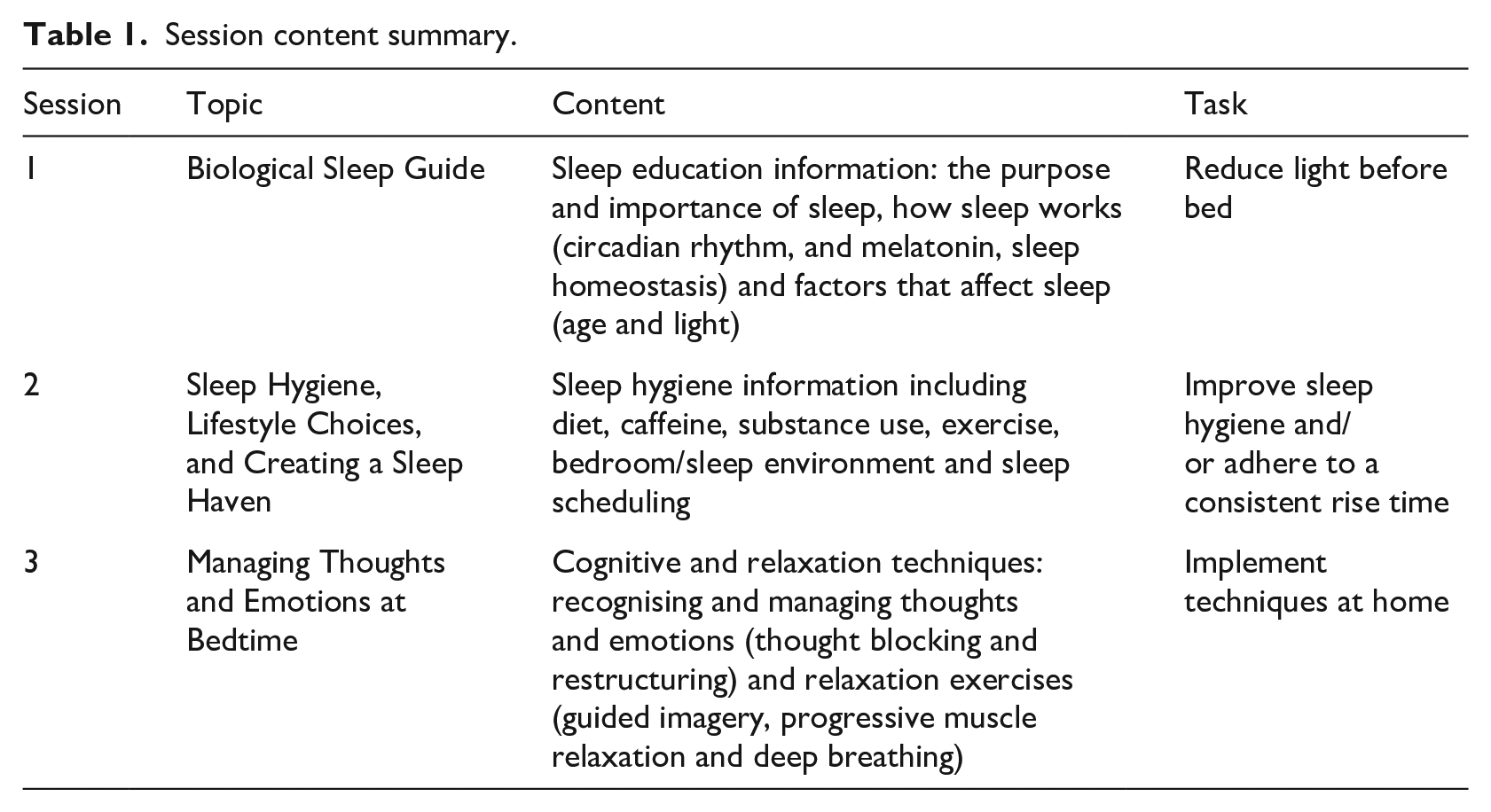
SIESTA is a sleep psycho-education programme, which integrates cognitive and behavioural techniques. The aim of SIESTA is to improve adolescents’ sleep knowledge and teach behaviour-change techniques that will facilitate sleep improvement. SIESTA comprises three lessons and was developed as a holistic approach, adopting both a preventive and intervention approach. SIESTA combines formal teaching and activities via three PowerPoint lessons, pupil workbooks and intervention practice via at-home tasks (see Table 1 for session summaries). At the beginning of the second and third lesson, students are encouraged to participate in a class discussion about their experience of implementing the at-home tasks. A delivery manual has been designed to ensure consistent delivery. In this study, sessions were delivered by the researchers in collaboration with class teachers.
Session content summary.
Feasibility
Feasibility of recruitment and retention was assessed via the number of schools approached who consented to participate, the return of opt-out consent forms, and participant dropout rate (number of students who did not complete baseline and post-intervention measures). The number of completed questionnaires and the number of missing items were used to assess the feasibility of data collection procedures. Suitability of training and programme delivery as intended was used to assess the feasibility of the design procedures.
Acceptability
Acceptability was measured using qualitative feedback collected from focus groups. Materials included a semi-structured topic guide with open-ended questions covering topics such as intervention content, usefulness of materials, delivery method, areas for improvement and implementation. Focus groups were audio-recorded to enable transcription.
Demographic measures
Demographic information was collected including participant age, gender and year group.
Sleep measures
Symptoms of insomnia were assessed with the sleep condition indicator (SCI, Espie et al., 2014). The SCI is an eight-item standardised measure, each item is scored on a 5-point scale (0–4) with scores ranging between 0 and 32 (higher scores indicative of better sleep). The SCI includes recommended cut-off scores indicative of probable insomnia (⩽16). The SCI has been used with adolescents (Illingworth et al., 2020), and is a valid and reliable measure with good internal consistency (α = .86). Sleep hygiene was measured using the 28-item Adolescent Sleep Hygiene Scale (ASHS, LeBourgeois et al., 2005), which assesses sleep-facilitating and sleep-inhibiting behaviours. Each item is rated on a 6-point scale with higher scores indicating better sleep hygiene. The measure had good internal consistency (α = .8).
Additional outcome measures
Screen use was measured using the Screen-Based Media Use Scale (SBMS, Houghton et al., 2015), which is an 11-item measure that assesses device type as well as duration of use and has been validated for use with adolescents. Symptoms of depression, anxiety and stress were measured using the short-form Depression, Anxiety and Stress Scale (DASS-21, Lovibond and Lovibond, 1995). DASS incorporates three sub-scales assessing symptoms of depression, anxiety and stress. Five categories of severity exist for each sub-scale and include normal, mild, moderate, severe and extremely severe: depression (⩽9, 10–13, 14–20, 21–27 and ⩾ 28), anxiety (⩽ 7, 8–9, 10–14, 15–19 and ⩾ 20), and stress (⩽ 14 15–18, 19–25, 26–33 and ⩾ 34). Each item is scored on a four-point scale (0–3) and ranged from 0 to 42 (higher scores indicate increased symptom severity). The DASS-21 is valid and reliable for use with adolescents aged 12+ years (α = .94).
Procedure
Ethical approval for the study was granted by the University of Strathclyde Ethics Committee. The study was initially designed for the face-to-face delivery of SIESTA and data were collected for 115 students using this method. Due to COVID-19 pandemic restrictions at the time of the study, a live online delivery (via Zoom) method was selected for the remaining 56 students. Study researchers and teachers had completed a 2-day CBT-I training workshop delivered by behavioural sleep medicine experts prior to the delivery of SIESTA and attended ongoing supervision.
Schools disseminated information sheets and opt-out consent forms to parents/carers prior to the onset of data collection (all students participated in the SIESTA programme, but could opt-out of having their data included in the data analysis). Verbal consent was gained from students prior to the completion of assessments conducted 1 week prior to the first session, during a scheduled PSE class. A unique ID code (10 digits comprised birth month and year and six digits of a telephone number) was created by students to maintain anonymity and to link assessments. A master copy of the ID codes was retained by each school, stored securely and separate from the data.
SIESTA was delivered over 3 weeks during time-tabled classes. Each class comprised up to 32 students and lasted 45–60 minutes. One week following the final session, teachers distributed the post-intervention assessments and students completed them in class. Two weeks following the final session, pupils identified by the teachers, were invited to participate in focus groups conducted by researchers. Focus groups varied in length and were conducted during a scheduled lesson. Three focus groups were conducted, one per year group and comprised 19 students.
Data preparation and analysis
Questionnaire data were first inspected for missing values, and questionnaires met inclusion criteria if there were less than three items missing per questionnaire (data from 11 participants were removed). All remaining missing values (N = 31) were replaced using individual mean imputation method. This technique was selected as it is a validated technique (Shrive et al., 2006), was recommended in the DASS manual (Lovibond and Lovibond, 1995) and was selected to maintain consistency across measures.
Quantitative analyses were conducted using the Statistical Package for the Social Sciences (IBM SPSS Statistics Version 26) and focused mainly on pre/post-intervention changes. Summary data for each measure were calculated, descriptive and frequency analysis was conducted for all variables. Inspection of the distribution of data using histograms, Q–Q plots and Kolmogorov–Smirnov tests highlighted a non-normal distribution for the SCI and DASS. Therefore, non-parametric tests were selected as the most appropriate for the analysis. Wilcoxon signed-rank tests were conducted to investigate pre- to post-intervention changes. Using the recommended cut-off scores for the SCI, students were categorised as ‘good sleepers’ (scored ⩾ 17) or ‘poor sleepers’ (scored ⩽ 16). To investigate category shift from pre- to post- insomnia, a McNemar analysis was conducted on the SCI. Sensitivity analyses were conducted to investigate the effects of the delivery method (face-to-face delivery vs remote delivery) on the primary outcome. An alpha level of .05 was set for all statistical tests.
Focus group data were transcribed by an online transcription service using orthographic transcription. Data were analysed using Braun and Clarke (2006) steps for thematic analysis (TA) and conducted by four researchers.
Results
Feasibility – participant recruitment and retention
There were excellent rates of recruitment and retention in this study as all the schools approached to participate in the study agreed to do so. The opt-out consent process appeared feasible and acceptable as 369 students consented to participate in the data collection, and no students/parents/carers opted out. Therefore, the recruitment and consent procedures adopted were deemed successful. Unexpected school closures due to COVID-19 pandemic, meant that 142 students could not complete the SIESTA programme and/or post-intervention assessments and were therefore excluded from the final sample (see Figure 1). A follow-up debrief email was sent to schools to disseminate to parents of affected students, which detailed that the student’s data would not be included in the analysis. Excluding those students who could not complete SIESTA due to the pandemic (142), only 5% (11/227) of the sample dropped out and did not complete both baseline and post-intervention measures. Therefore, there was successful retention of participants in this study.
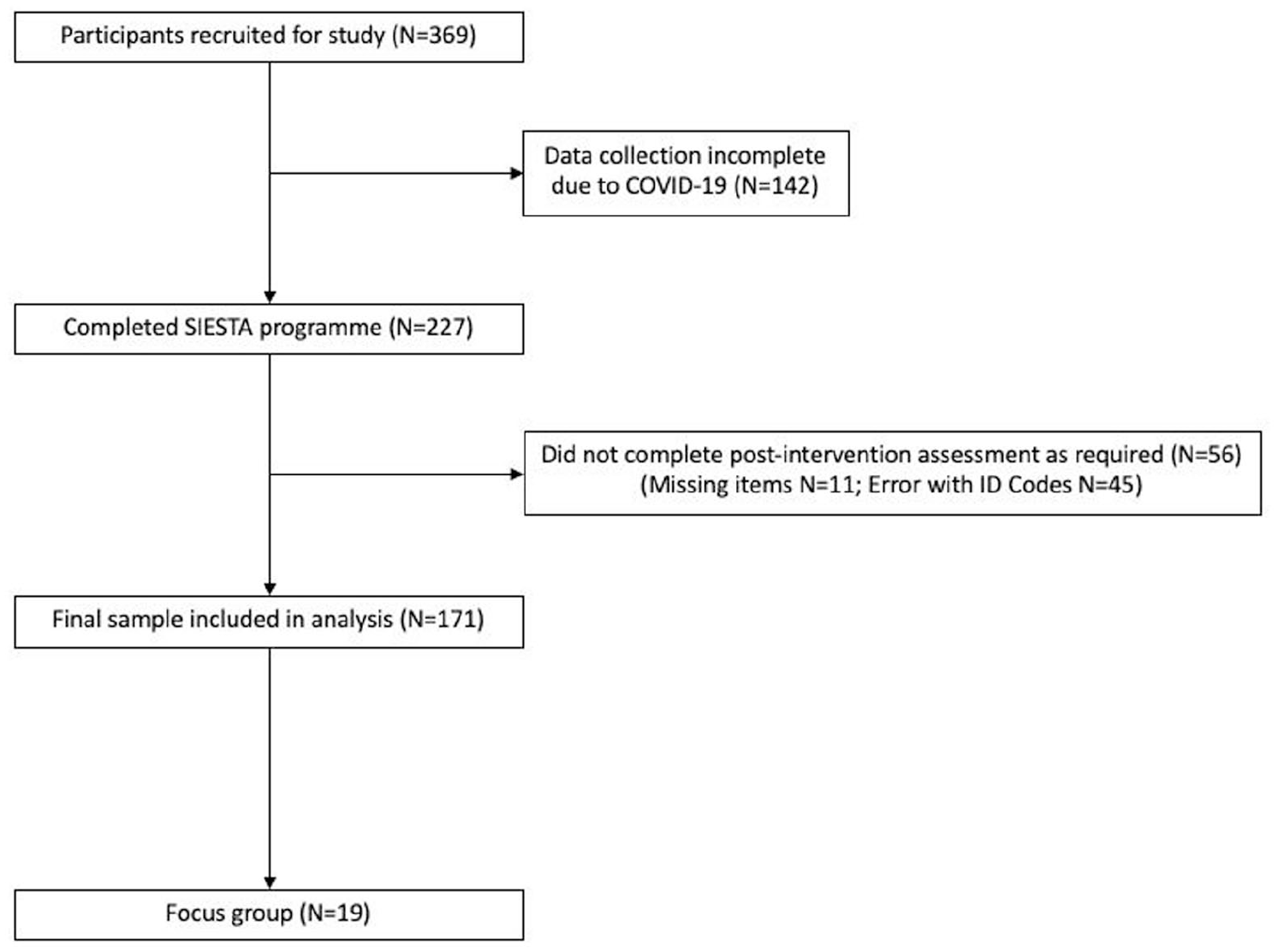
Flowchart of participants.
Feasibility – Data collection procedures
The remaining students completed both assessments and the SIESTA programme. However, 45 students incorrectly entered their ID codes meaning that their baseline and post-intervention assessments could not be matched. This highlighted that the method adopted to create ID codes may have been too complex for this population. Therefore, our final sample comprised 171 students (mean age = 12.93 (.91); 53% women; S1 = 43%, S2 = 29%, S3 = 28%).
Most questionnaires were completed accurately with some missing items (n = 31 missing items). However, the SBMS may have been too onerous for students, and majority were not completed fully/accurately. Therefore, the decision was made to exclude the SBMS from the data analysis. However, the other measures provided sufficient data to assess the preliminary efficacy of SIESTA.
Feasibility – Delivery procedures
Outcome measures were collected 1 week prior and 1 week following the delivery of SIESTA during a scheduled PSE lesson, which enabled students to ask questions/seek guidance from the researchers/teachers. No extended follow-up assessment was conducted. The researcher/teacher training, accompanied by ongoing supervision, and delivery manuals enabled the researchers to successfully deliver the programme as intended. Therefore, this was a feasible method of delivery with sufficient training and guidance to deliver the programme.
Acceptability
The students spoke favourably about the method of delivery, and many expressed their preference for SIESTA to be delivered by the researchers, as they perceived them to have increased knowledge and expertise. However, students expressed that they would still prefer teachers to deliver the programme, as opposed to self-help or older students. SIESTA was appropriate for delivery within the context of the PSE curriculum as one teacher commented ‘As a teacher, you know, mental health’s a huge issue in school just now and I think sleep’s really, really tied into that’.
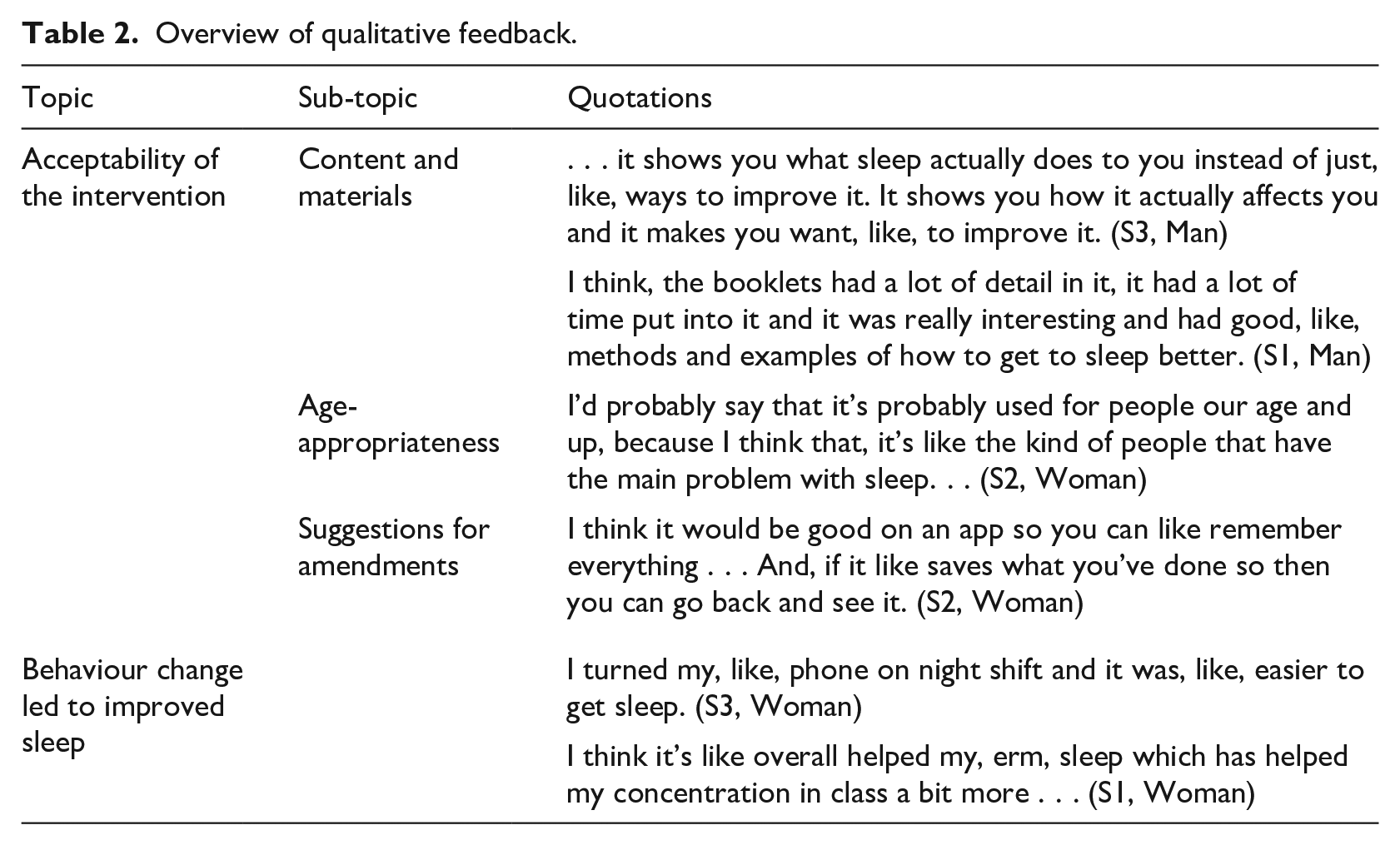
Overall, the students spoke favourably about the SIESTA programme and reported that the content was engaging, informative, clear, and well organised (see Table 2 for an overview of key topics and sample quotations). The majority of students expressed that SIESTA was age-appropriate and relevant for early adolescents before insufficient sleep becomes a more prominent issue in late adolescence (e.g. stress of examinations impacting sleep). Some students made suggestions for amendments to improve the lessons in future (e.g. use of a mobile app to support with at-home activities/strategies). Students reported that they had attempted the techniques including reducing screen use/activating blue light-limiting function, improving their sleep environment, cognitive and relaxation techniques. Some students reported an improvement in daily functioning after the intervention, specifically, in their ability to concentrate in class.
Overview of qualitative feedback.
Preliminary efficacy
In the total sample, there was a significant improvement in symptoms of insomnia (SCI) from baseline to post-intervention (Z = 4.986, p =< .001, r = .38). Descriptive analysis of baseline data (see Table 3) showed that 18.2% of the total sample were categorised as poor sleepers (⩽16 on the SCI), and this reduced to 14.6% post-intervention. Examination of baseline sub-groups revealed that there was a significant improvement in symptoms of insomnia for both those with poor sleep (Z = −2.75, p =< .005, r = .3) and those with good sleep (Z = −4.26, p =< .001, r = .17). A McNemar’s test revealed there were no significant category shifts (p = .118) between the groups. Sensitivity analysis showed that insomnia symptoms improved significantly in those who received face-to-face delivery (N = 115, Z = −4.67, p =< .001, r = .02) and live remote delivery (N = 56, Z = −2.02, p =< .05, r = .02). See Table 3 for an overview of descriptive statistics. There were no significant improvements in sleep hygiene behaviours from baseline to post-intervention (Z = −1.42, p = 1.55). There were significant improvements in symptoms of stress (Z = −2.67, p =< .05, r = −.2), but not for depression (Z = −1.12, p =< .26) or anxiety (Z = −1.34, p = 2.57).
Descriptive statistics for primary and secondary outcomes.
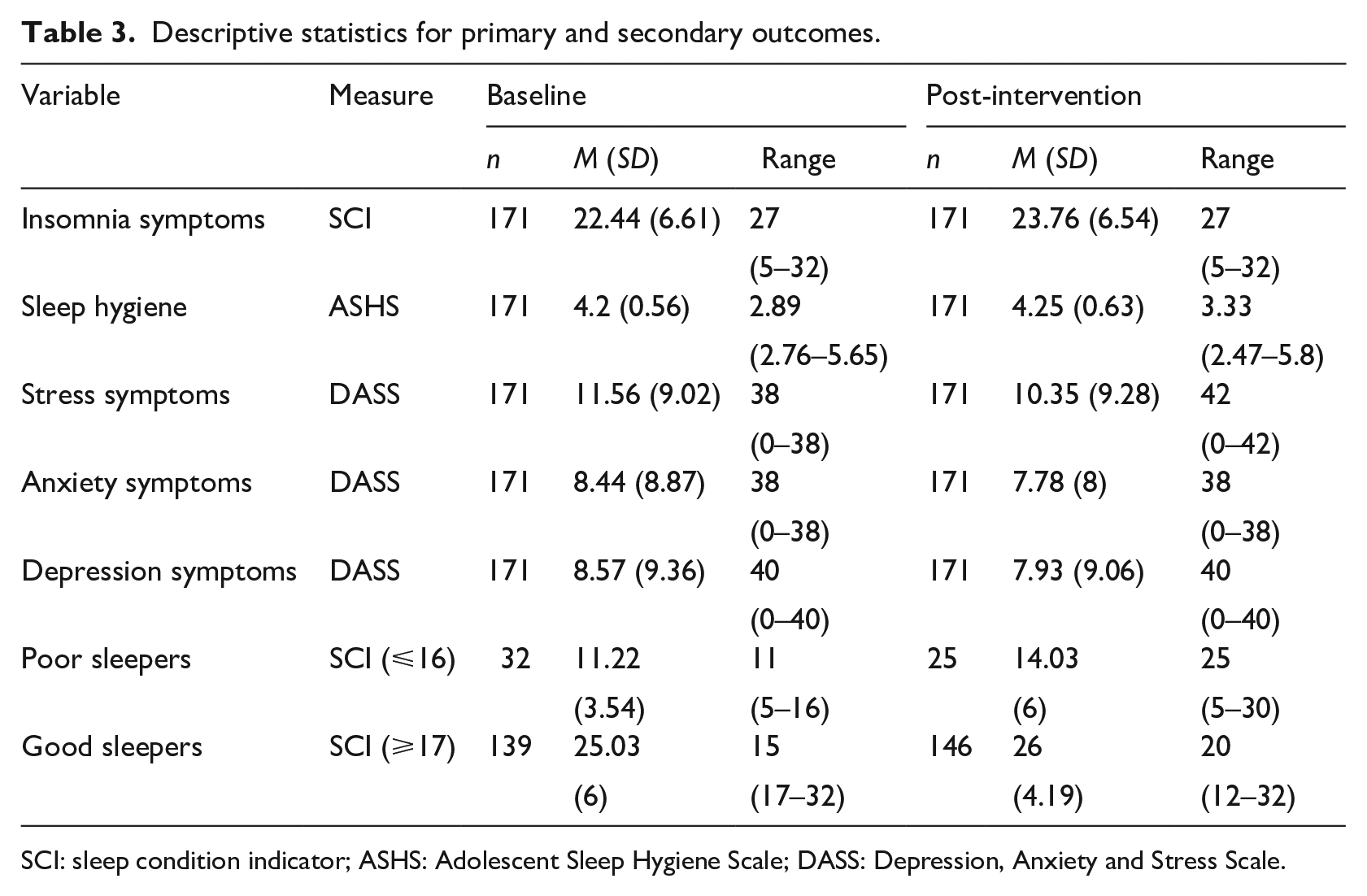
SCI: sleep condition indicator; ASHS: Adolescent Sleep Hygiene Scale; DASS: Depression, Anxiety and Stress Scale.
Discussion
This study investigated the feasibility, acceptability and efficacy of delivering SIESTA via the school curriculum. Overall, the results indicate that SIESTA is a feasible and acceptable programme for delivery within the Scottish Educational context, with preliminary evidence for the efficacy of the programme.
The use of opportunity sampling was a viable method of recruitment as all invited schools participated in the study, no students/parents opted out of data collection and almost all students completed follow-up measures. This may have been due to the relationships that were developed with schools via training and ongoing communication, which is crucial for successful recruitment and retention in school-based studies (Schoeppe et al., 2013). In addition, in Scotland, schools have autonomy over the content of the PSE curriculum; therefore, individual schools/teachers were able to authorise participation in this study, which enabled us to recruit more easily. Furthermore, the data collection procedures involved baseline and post-intervention measures collected during scheduled class time. This was a useful method of collection as students were able to seek advice/guidance if required. However, errors with ID codes meant that 25% of questionnaires could not be matched and were excluded. In future, a simpler method of anonymisation should be adopted, such as an online ID code generator. Overall, the majority of questionnaires were completed fully and accurately, with the exception of the SBMS that had to be excluded from the analysis. This may have been due to the length and/or structure of the questionnaire, which featured a significant amount of text. Questionnaires that feature complex instructions, unclear wording and include too many questions can reduce completion and increase drop-out (Bartell and Spyridakis, 2012).
Regarding the study design, SIESTA was delivered over three consecutive weeks during scheduled classes. This was advantageous as it ensured that all content was delivered without burdening the schools with requirements for increased time and resources, which can be a key barrier to implementation (Cassoff et al., 2013). The training to criterion approach that was adopted was feasible as researchers, in collaboration with class teachers, were able to successfully deliver the programme. However, in future trials, SIESTA will be delivered exclusively by teaching staff (as per the intervention protocol) to enhance the delivery, evaluation and subsequent implementation (Toomey et al., 2020).
To assess the acceptability of SIESTA, qualitative feedback was collected via focus groups. The students spoke positively about SIESTA and many students expressed that the lessons were engaging, informative and relevant. The students discussed the importance of sleep and commented on aspects that they enjoyed, most notably, the physiology of sleep. This finding is echoed in previous research that noted students were keen to have the opportunity to learn about sleep (MacLeod and Taylor, 2013). Overall, the feedback indicated that the content and delivery of SIESTA was acceptable and beneficial for students. This is an important finding as it has been argued that acceptability can impact the efficacy of interventions (Sekhon et al., 2017). Although only limited feedback was collected from teachers, the feedback received was positive and highlighted the importance of sleep for mental health and wellbeing. In future trials, teacher feedback should be sought to enhance our understanding of the acceptability of SIESTA to facilitators.
The results demonstrate that there was a significant improvement in symptoms of insomnia in the total sample. This result is consistent with a similar study by Illingworth et al. (2020) who also found significant improvements in insomnia symptoms. This finding is promising as previous reviews have reported significant improvements in sleep knowledge, but mixed findings regarding improvements in sleep quantity and/or quality (Blunden et al., 2012; Gruber, 2013; Rigney et al., 2021). Although, most school-based sleep intervention studies have measured sleep outcome variables such as sleep onset, duration and efficiency (Bartel et al., 2018; Moseley and Gradisar, 2009), but not insomnia symptoms, which limits the comparability of the current findings. In future, a sleep diary should be used to assess additional sleep outcome variables.
Furthermore, the results indicate that SIESTA was beneficial for all adolescents including students who were identified as having poor sleep at baseline, as well as those who were categorised as good sleepers, demonstrated by significant improvements in insomnia symptoms in both groups (although it is important to note that even though these improvements were statistically significant, they were modest, represented by small increases on the SCI). However, examination of subgroup movements revealed that most students remained within the same category (either poor or good sleepers). This contrasts with the findings of a study conducted in the UK by Illingworth et al. (2020) who reported that students with ‘probable insomnia’ at baseline, significantly improved post-intervention, but there were no significant improvements observed for ‘good sleepers’. On the contrary, Bauducco et al. (2020) conducted a study in Sweden and noted that universal school-based programmes are more likely to benefit those without sleep problems, as they provide an opportunity to prevent the development of maladaptive sleep behaviours and subsequent problems.
Regarding secondary outcome variables, there were no significant improvements in sleep hygiene following the intervention. This finding is in line with some (Bauducco et al., 2020; Inhulsen et al., 2022; Rigney et al., 2015), but not all previous research (Illingworth et al., 2020; John et al., 2017). However, the results indicated that there was a significant improvement in symptoms of stress. SIESTA features cognitive and relaxation techniques that are beneficial for managing stress, which may have led to an improvement in stress symptoms (Sweetman et al., 2020). On the contrary, there were no significant improvements on symptoms of anxiety or depression. This finding is also in line with some previous research (Das-Friebel et al., 2019; Moseley and Gradisar, 2009; van Rijn et al., 2020), whereas other studies have reported improvements in depressed mood (Bonnar et al., 2015). One possible explanation is that there were lower levels of depression and anxiety symptoms at baseline, as most students scored within the normal severity range. Also, SIESTA was designed to target and improve adolescent sleep, and this aim was achieved with the improvement in insomnia symptoms. Research has suggested that poor sleep may predate symptoms of depression and anxiety (Goldstein and Walker, 2014; Lovato and Gradisar, 2014). Therefore, it may be possible that the prevention, recovery and subsequent improvements in depression and anxiety also follow a similar trajectory.
Limitations
The findings from this study should be interpreted in the context of some methodological limitations. The absence of a control group has been highlighted as a key methodological limitation of studies investigating school-based sleep education programmes (Blunden and Rigney, 2015). As the purpose of this study was to explore the feasibility of SIESTA, a control group was not required. However, the reporting of preliminary efficacy data should be interpreted cautiously. Furthermore, the programme was delivered to adolescents in January 2020 and 2021, following the Christmas break, at the beginning of a new term. Research has found that adolescents sleep significantly longer during a holiday period (Agostini et al., 2018). Therefore, insomnia symptoms may have been lower at baseline than they would have been if they were assessed later in the school term, after they had accumulated sleep debt. Future research should aim to control for this potential confounding factor. Finally, this study included a post-intervention assessment conducted 1 week following the final lesson, therefore, it is perhaps unsurprising that there were no significant improvements observed in symptoms of depression or anxiety. Future research should aim to include a later follow-up at 6 or 12 months to detect any longitudinal and preventive changes (Bauducco et al., 2020).
Conclusion
This study was the first study to evaluate the systematic delivery of a school-based sleep education programme via the PSE curriculum in Scotland. The findings are encouraging and have demonstrated that delivering SIESTA via the PSE curriculum, to groups of adolescents, is feasible and acceptable. In addition, the results highlight the preliminary efficacy of SIESTA, demonstrated by improvements in symptoms of insomnia and stress. The study provides further evidence for the preventive benefits of school-based programmes as improvements were seen in all students, irrespective of insomnia symptoms severity. The findings suggest that delivery of sleep education can influence improvements in sleep behaviour. This exploratory feasibility study has also highlighted some key methodological issues that will be used to inform future trials and evaluations of SIESTA.
Footnotes
Acknowledgements
We thank the following former students of the University of Strathclyde, who were instrumental in data collection for this study: Astrid Selin, Karolina Kiper, Clare Munro, Emma Brown, Khansa Hussain, Mollie McDermott, Monica Garcie Del Torro, Nicola Doyle. We also thank James Boyle from the University of Strathclyde. We are grateful to the schools and students who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this research was funded by a grant from the Glasgow Children’s Hospital Charity Research Fund (GCHC/SPG/2019/05).