
Abstract
Objective:
People with latent tuberculosis infection (LTBI) are required to make complex treatment decisions, which require an understanding of personal risk and associated benefits. However, many people with LTBI in the United Kingdom are at risk of low health literacy and can also experience language barriers, which can affect decision making. Patient education resources can support understanding but must meet the needs of the target population. The aim of this study was to evaluate the accessibility, readability and content of LTBI patient education resources.
Design:
Review and descriptive analysis of online LTBI patient education resources.
Setting:
UK-based online patient education resources.
Method:
We searched UK public health and charitable organisations for online LTBI patient education resources. Resources were evaluated in terms of accessibility (availability of translated versions); readability (Flesch–Kincaid Reading Ease [FKE], Flesch–Kincaid Grade Level [FKG] and Simplified Measure of Gobbledygook [SMOG]), theoretical content (Extended Common-Sense Model) and principles of shared decision making.
Results:
Seventeen out of 60 articles identified in the search met the prespecified criteria for inclusion. Translated materials were available for 7 of them. The overall mean ± SD readability scores and corresponding reading ages were FKE 63.51 ± 8.81 (13–15 years), FKG 9.14 ± 8.95 (13–15 years) and SMOG 8.27 ± 1.51 (13–14 years). No resources met Health Education England recommended readability levels for health-related information. Dimensions of cognitive representations of illness and treatment most commonly addressed included treatment control, cause and identity (symptom and label); no resources addressed emotional identity.
Conclusion:
Current and future LTBI patient education resources would benefit from greater consideration of the needs of non-English language speakers, readability and theoretical content to improve patient illness experience and support informed treatment decision making.
Keywords
Introduction
Newly identified cases of tuberculosis (TB) are rapidly falling in England (Public Health England, 2018). However, TB continues to disproportionately affect some people, with the non-UK-born population representing 72.2% of all TB cases notified (Public Health England, 2018). The majority of active TB cases in the United Kingdom result from the reactivation of latent tuberculosis infection (LTBI) (Zenner et al., 2017). As such, the Collaborative Tuberculosis Strategy has aimed to ‘ensure the delivery of a quality assured local programme of new entrant LTBI screening, focused on areas of high TB incidence’ (Public Health England, 2015). The World Health Organisation (WHO) recommends an individual-level approach to LTBI screening and treatment in low-incidence countries such as the United Kingdom (Lönnroth et al., 2015). This means that any intention to screen for LTBI is an intention to treat a positive diagnosis, based on the decision that the benefits of treatment should outweigh any risks (Campbell et al., 2019).
Shared decision making is a key long-term priority of the National Health Service (NHS) (NHS England and NHS Improvement, 2019). National guidelines for the management of LTBI recommend that the risks and potential benefits of each treatment regimen should be explained clearly, and a suitable regimen selected in discussion with the patient should they accept preventive treatment (National Institute for Health and Care Excellence, 2016b). However, discussions with people about LTBI are often challenging. While there are individual benefits to accepting treatment such as reducing personal risk of TB disease, the concept of latency is complex. Given that the individual is asymptomatic, poses no current risk of infection to others and may not progress to active TB (Dobler et al., 2018), a ‘common-sense rationale’ in which the patient is able to make a link between LTBI and treatment may be unclear. Similarly, such consultations do not occur in isolation of the patient’s personal, social and environmental context, as each patient brings pre-existing beliefs about the illness and treatment (Horne et al., 2013). Addressing misconceptions about illness and treatment, as well as communicating both the risks and benefits of preventive treatment is essential to enable the patient to make an informed choice. At the core of shared decision making is the patient and health care professional relationship, wherein patients should be supported to explore their preferences and make decisions (Elwyn et al., 2012).
Psychological theory can be used to better support informed choice, taking into consideration the potential harms and benefits of medicines as well as a range of intrinsic and extrinsic factors that influence treatment decisions (Horne, 2017). The Common-Sense Model of Self-Regulation (CSM) is a widely used theoretical framework that describes how people use ‘common-sense’ to generate representations of health threats and subsequent coping strategies (Leventhal et al., 2016). The CSM depicts five core domains of cognitive illness representation – identity (symptoms and label), timeline (extent to which an illness is perceived as acute or chronic), cause (perceived cause of illness), consequence (extent to which illness is perceived to negatively affect life) and control (extent to which illness is expected to be responsive to treatment) – which are processed in parallel to emotional representations (emotional response to illness). When the coping procedure (strategies used to manage threat) includes a decision about treatment, it is recommended to use the extended CSM (Horne, 2003). This model sees treatment perceptions as linked to illness representations, with an individual not only having to decide if the threat warrants treatment, but whether the treatment is appropriate (Horne, 2003). The extended CSM encapsulates the Necessity-Concerns Framework (NCF), which provides a theoretical basis for understanding how patients make decisions about treatment, outlining two categories: (1) perceptions of personal need for treatment and (2) concerns about a range of potential adverse consequences (Horne et al., 2013).
Another factor which may impact on shared decision making is patient health literacy, defined as the ‘cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’ (Nutbeam, 1998: 357). A recent report highlighted how the diversification of cultural backgrounds and health profiles within the European Union presents unique challenges in terms of how to reduce systemic inequalities in health care delivery (Matlin et al., 2018). Poor health literacy, language barriers, and different cultural or religious beliefs are associated with lower medication adherence in people with LTBI (Butcher et al., 2013). Ensuring suitable levels of readability and accessibility of patient materials in different languages may be a first step to reducing these inequalities (Kalengayi et al., 2012).
Against this background, the aim of this study was to evaluate how LTBI patient resources in the United Kingdom support understanding and informed choices about treatment. Specifically, we investigated the accessibility and readability of the resources; and evaluated the content in terms of its potential for encouraging and supporting shared decision making and understanding of LTBI and treatment as mapped to the extended CSM.
Methods
Data collection
We conducted a rapid review of online UK-based patient education resources. Searches were performed on targeted specialist public health websites including the NHS (https://www.nhs.uk/), gov.uk (https://www.gov.uk/), the National Institute for Health Care Excellence (https://www.nice.org.uk/) and Google (www.google.com) between November and January 2020. Websites were searched using variations of the term LTBI, pages were then navigated by clicking on relevant links related to diagnosis, patient information and treatment. Where a search function was not available, we manually searched the website and relevant links to identify resources.
Selection criteria
Searches identified relatively few resources (materials designed to support patient education) that were LTBI specific as indicated by title. Flow of data through the different phases of the study is shown in Figure 1. Resources were screened initially by title, with any potentially relevant resources selected for full review against the inclusion/exclusion criteria. During the screening process, we expanded our criteria to include patient resources that targeted either TB or LTBI, so long as the resource included relevant information specific to LTBI.
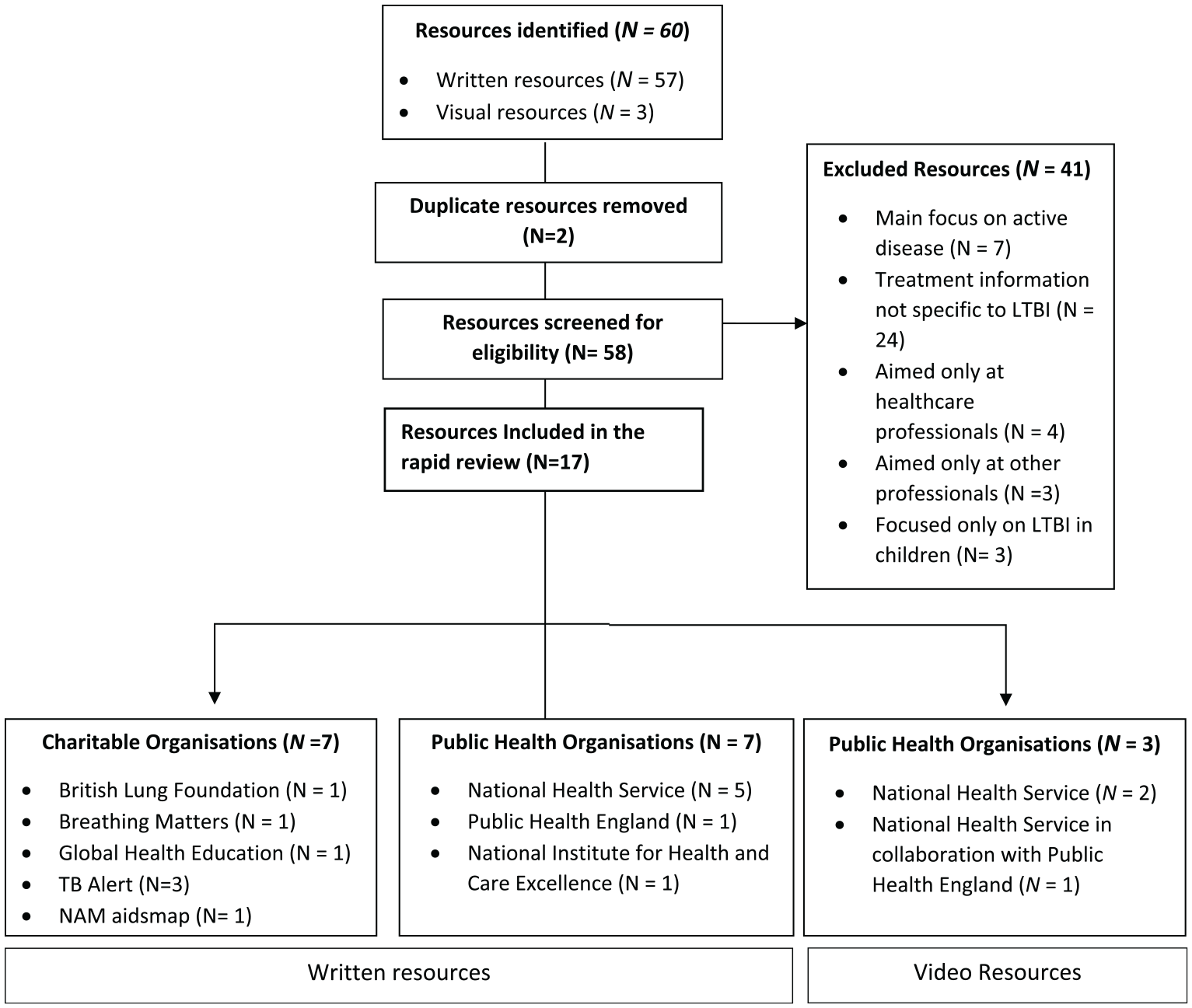
Flow of data through the different phases of the study.
Inclusion criteria
Provides specific information about LTBI treatment
Aimed at patients or the public
Published by a UK organisation
Available to view, download or stream online
Available in the English language
Exclusion criteria
Focused only on active TB disease
Focused only on LTBI in children
Aimed at supporting health care professionals, or those working with people with LTBI only, as opposed to patients
Content analysis of patient education resources
Patient accessibility
We assessed the accessibility of resources, both in terms of format (e.g. streamed, viewed online or downloaded) and the availability (or otherwise) of translated resources for non-English speakers.
Readability
Readability was assessed using a free online readability test tool (https://www.webfx.com/tools/read-able/). The main text from each written resource was imported directly into the tool. Health Education England (HEE) recommends that patient resources be written at a level suitable for comprehension by an average 11-year-old. Mean ± SD readability scores were calculated for the Flesch–Kincaid Reading Ease (FKE), Flesch–Kincaid Grade Level (FKG) and Simplified Measure of Gobbledygook (SMOG) as recommended by HEE (2018). Scores can be converted into UK reading ages – see Supplementary Material 1.
Theoretical content
We developed a coding framework to assess the following theoretical principles: cognitive and emotional representations of illness (identity, timeline, cause, consequences, control/cure [subcategories personal control and treatment control] and emotion) as specified in the CSM (Leventhal et al., 2016) and treatment perceptions (necessity beliefs and treatment concerns) as specified in the NCF (extended CSM) (Horne, 2003) (Table 1). Domains were discussed in terms of definition and relevance to LTBI. Communication was included as an additional domain to assess the extent to which resources encouraged discussion with health care professionals, an important component of shared decision making. An initial classification-coding table was developed based on published definitions for each domain. Key criteria for each domain, along with the classification system were iteratively refined using a constant comparison approach following familiarisation and indexing of the resources. We developed a three-level coding system (fully addressed, somewhat addressed and failed to address) to demonstrate sensitivity regarding the extent to which each resource addressed each of the theoretical domains.
Theoretical domain classification criteria.
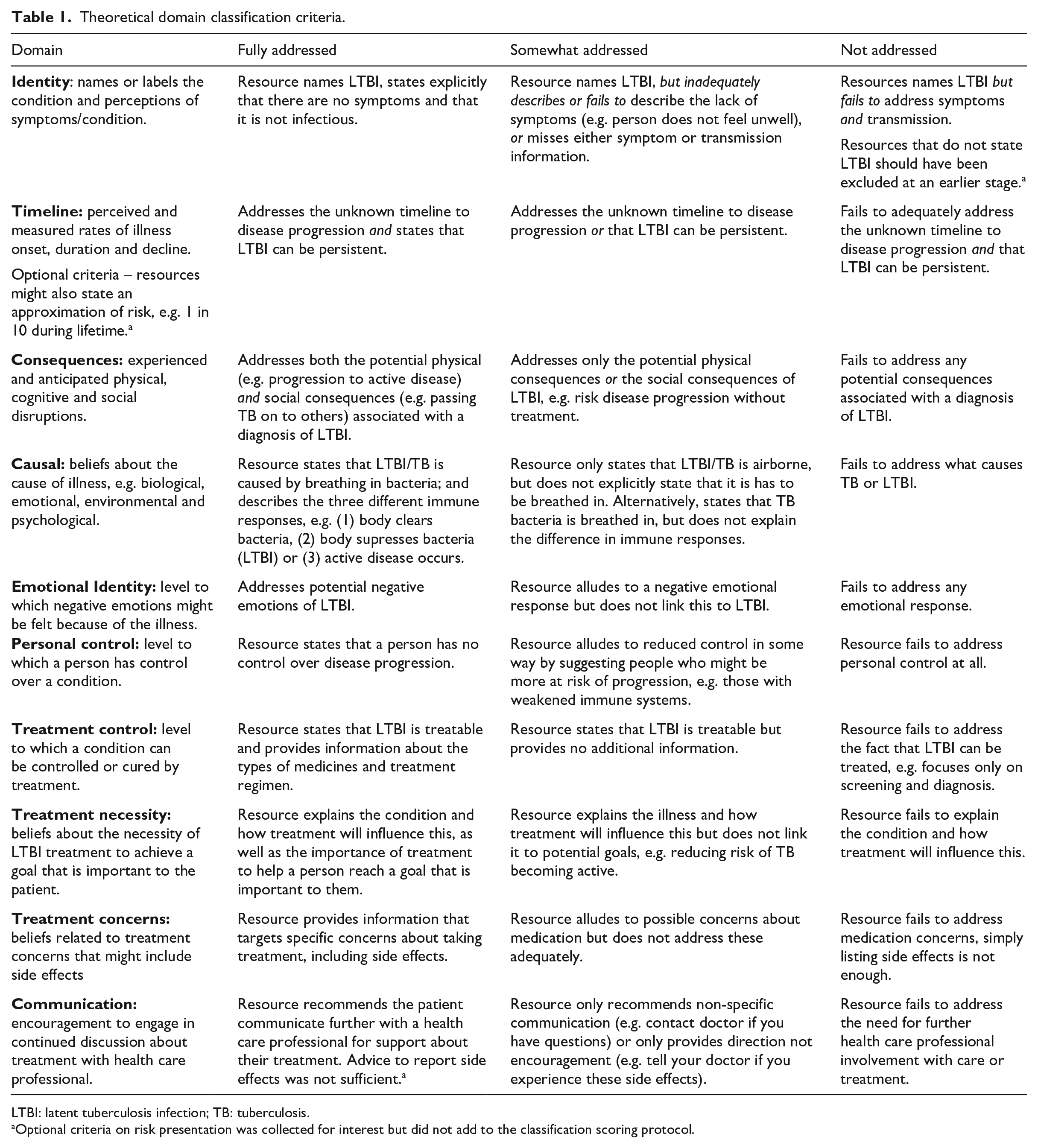
LTBI: latent tuberculosis infection; TB: tuberculosis.
Optional criteria on risk presentation was collected for interest but did not add to the classification scoring protocol.
Content analysis
Data analysis was guided by the principles of a deductive content analysis (Elo and Kyngäs, 2008) in which resources were coded against the predefined theoretical framework (Table 1). The authors A.L.C., T.S. and A.S.K.J. individually coded the resources; codes were combined and any inconsistences resolved through discussion.
Readability data were analysed using SPSS (version 26) and are presented as means ± SD.
Results
Our search identified 60 resources of which 17 resources met the inclusion criteria (Table 2). The publication dates of included resources ranged from 2007 to 2020. Of the included resources, nine were LTBI specific and eight focused on TB disease but included relevant LTBI information.
Description of LTBI resources (N = 17) and level of accessibility.
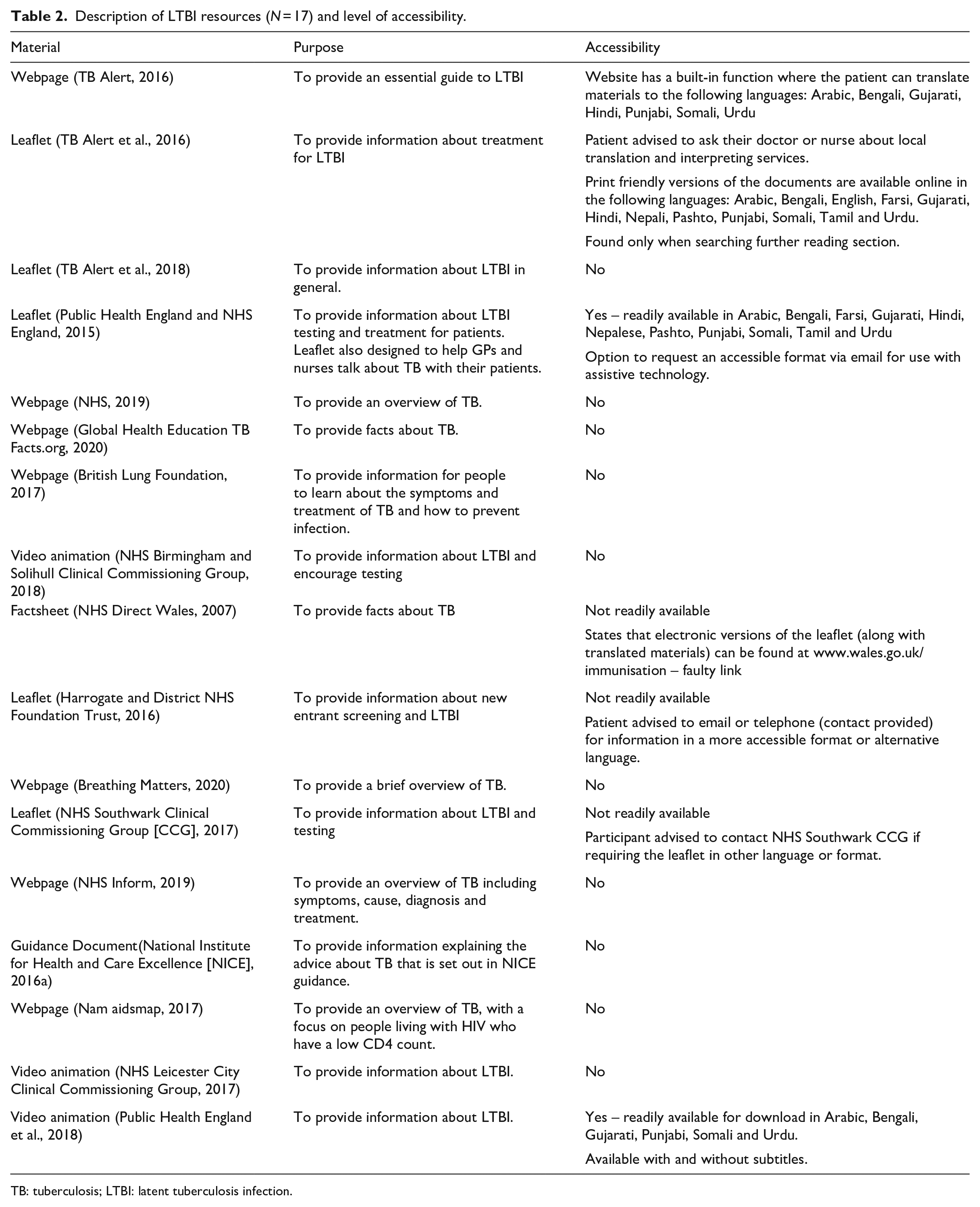
TB: tuberculosis; LTBI: latent tuberculosis infection.
Format and accessibility
Table 2 details the accessibility of the resources. Patient resources were available in various formats including leaflets, booklets, websites, guidelines and video animations. All resources were accessible online. Alternative formats for increased accessibility were available for three resources, including the addition of subtitles (animation video), larger text or versions compatible with assistive technology. Translated materials were reported as available for seven resources, but only three translations were available for immediate viewing. For the remaining resources, access to translated materials were either only available on request (e.g. by contacting a request telephone line or health care professional), were not easily located on the site or unavailable due to a broken hyperlink.
Readability Statistics
Of the included resources, 14 were in a written format and evaluated for readability. The remaining 3 resources were video animations. The overall mean ± SD readability scores and corresponding reading ages were FKE 63.51 ± 8.81 (13–15 years), FKG 9.14 ± 8.95 (13–15 years) and SMOG 8.27 ± 1.51 (13–14 years). None of the resources met HEE recommendations for readability across all three tests. The resource with the lowest reading age score was a leaflet authored by Public Health England: FKE 74.10 (reading age 12–13 years), FKG 6.20 (reading age 11–12 years), SMOG 6.50 (reading age 11–13 years).
Theoretical content analysis
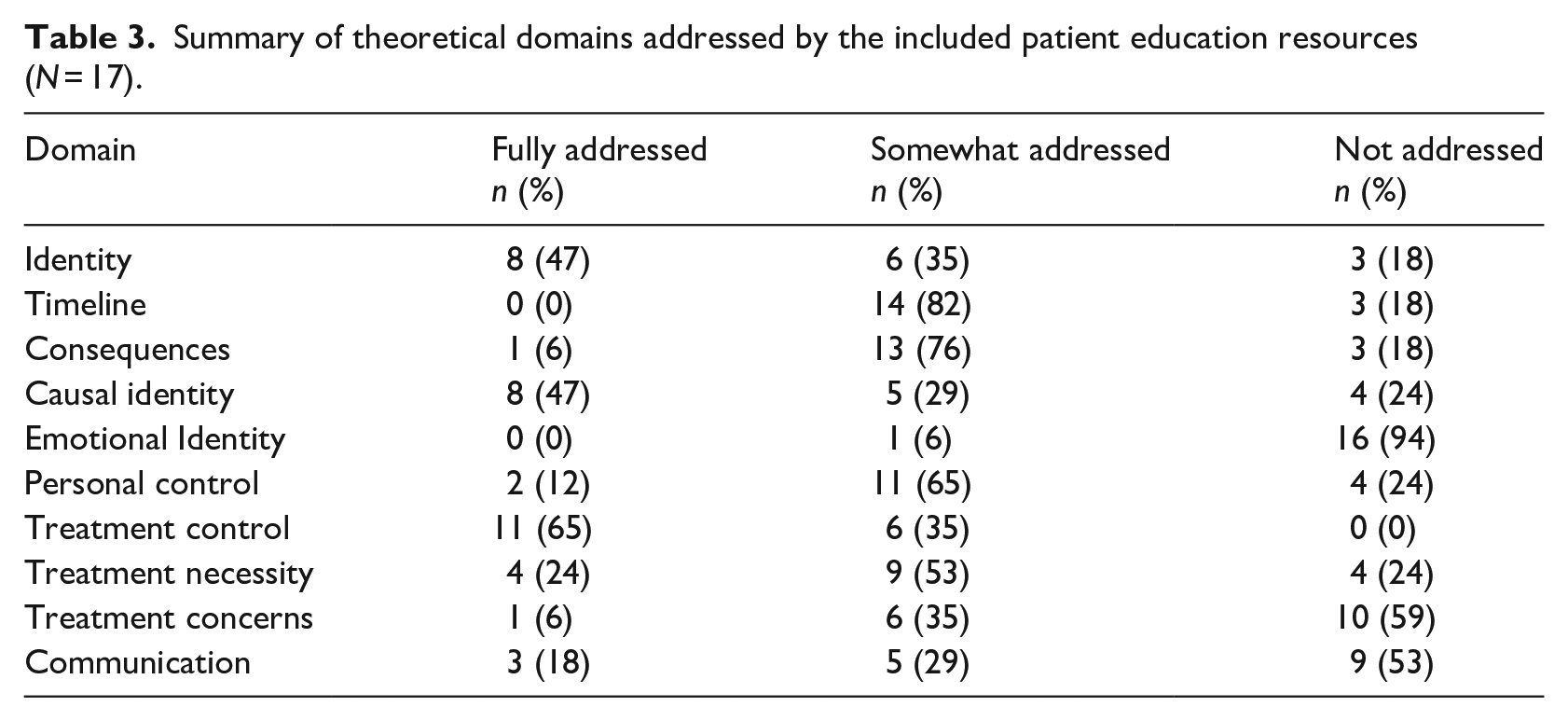
Coding criteria and domain glossary are shown in Table 1, and a summary of the number of resources adequately addressing each theoretical construct of interest is shown in Table 3. A further breakdown of the individual resources mapped to the theoretical domains is contained in Online Supplemental Material.
Summary of theoretical domains addressed by the included patient education resources (N = 17).
Illness perceptions
All resources named LTBI. However, identity was fully addressed by only 47% of resources. Resources that did not fully address the identity domain tended to provide vague statements related to the asymptomatic nature of the condition, such as ‘LTBI does not make you feel unwell’.
The majority (65%) of resources fully addressed treatment control by providing information about the curability of LTBI and additional information about treatment type and duration. In contrast, only 12% of resources fully addressed personal control by explicitly stating that there is no way of knowing whose infection will progress from LTBI to active TB.
Causal identity was fully addressed by 47% of resources. Resources failing to address this domain often stated that TB was airborne but did not explicitly state that TB bacteria are inhaled or describe the different immune responses following exposure to TB bacteria. No resources addressed causal misconceptions commonly held by certain TB patient groups, for example, ‘TB is a family curse or sign of witchcraft’.
One resource fully addressed consequences, stating both the physical (e.g. disease progression) and social (e.g. risk of transmission to friends and family) consequences of not treating LTBI. While most resources addressed the physical consequences, social issues were not addressed beyond the future risk of transmission. Missing concepts included the impact of LTBI diagnosis on social identity or social relations, and experience of stigma.
No resources fully addressed timeline. The majority (82%) referred to the unknown duration of disease progression, yet failed to acknowledge that LTBI can be persistent. Eleven patient resources provided absolute risk estimates for disease progression (optional criterion within the timeline domain) using numerical event rates (e.g. 1 in 10 or 10% chance of disease progression.).
No resources adequately addressed emotional identity, which refers to the extent to which an illness promotes a negative emotional reaction (Hagger et al., 2003). One resource alluded to negative emotions generally, and some resources provided links to support, but these were not specific to addressing negative emotions resulting from LTBI or treatment.
Treatment perceptions
Treatment necessity was only addressed fully by 24% of resources. Resources often failed to link the problem and the treatment. For example, many resources simply stated that treatment can prevent progression to active TB (benefit of treatment), but did not include a common-sense rationale for how treatment might work to help the patient achieve a health goal that is important to them. Only one resource fully addressed treatment concerns, by making reference to common patient concerns throughout the resource such as ‘I don’t feel ill so why should I take treatment for latent TB?’ This same resource also provided a common-sense rationale for treatment necessity (TB and Alert, 2016c).
Communication
Communication was addressed by 18% of resources. Most failed to address communication with a health care professional at all or only identified the need for contact in relation to the experience of side effects. No resources facilitated shared decision making by addressing both illness and treatment perceptions and encouraging communication with a health care professional.
Discussion
This study aimed to evaluate the accessibility, readability and content of online UK LTBI patient education resources. Searches yielded a modest number of patient resources (N = 17), with the majority of these focusing predominately on active TB disease.
All included written resources scored higher than the recommended reading level for patient information, as advised by HEE (2018). This is problematic as non-UK-born individuals disproportionately bear the burden of TB in the United Kingdom (Pareek et al., 2016), may have limited English language proficiency and an increased vulnerability to poor health literacy (Ward et al., 2019). Furthermore, only three resources were readily available in other languages. Translated resources available only on request can add an extra barrier to asserting candidacy (eligibility for medical attention/intervention jointly negotiated between individual and health care system) among the UK migrant population (Potter, 2018). This potentially limits patients’ ability to make informed treatment choices, thus widening the gap for health inequality within the United Kingdom (Salway et al., 2020).
The majority of resources were in written format, but there may be more optimal formats for delivering patient education. The review identified three video animations whereby written or spoken information were supported by graphics. One video animation had high accessibility, being readily available for streaming and download in a number of languages, but the primary focus was LTBI screening (Public Health England et al., 2018). Animations have been shown to improve TB knowledge among low literacy populations (Reeves et al., 2020), suggesting animation as an effective channel of delivery for improving patient knowledge and supporting informed treatment decisions.
Theory-based materials (in the form of the application of a set of concepts and/or standards with specification of how phenomena relate to each other, applied to the development of interventions such as patient education resources) can enhance knowledge and facilitate informed choice about treatment (Bishop et al., 2019; Davis et al., 2015). However, this review highlighted a lack of theoretical content in LTBI patient education resources. No identified resource fully addressed all the theoretical domains in the extended CSM and the additional domain of communication. A website page by the leading UK TB charity, TB Alert, had the most theoretically based content (fully addressing 6 out of 10 domains) (TB and Alert, 2016c); however, it failed to address emotional identity.
A recent mixed-methods cross-sectional study of 108 people with LTBI conducted in Sweden, showed emotional concerns (anxiety and depression) to be prevalent among 27.7% of the sample (Shedrawy et al., 2019). Qualitative work described how lack of clarity about the disease, the future and risk to others had a negative impact on participants’ mental health (Shedrawy et al., 2019). This highlights the importance of acknowledging emotional identity and treatment concerns in LTBI patient education resources, and the need for signposting to appropriate supportive services.
Identified patient education resources also commonly neglected certain illness perceptions such as treatment concerns and timeline, despite the likely influence of these beliefs on treatment decision making. A recent study found that ~30% of patients declined participation in a randomised international trial of new LTBI treatment regimens, due to beliefs about LTBI (e.g. no perceived risk of active TB) or treatment perceptions (e.g. negative impact on health) (Hedges et al., 2019). Addressing treatment perceptions may help to support informed treatment decisions; however, only one resource addressed treatment concerns. Listing side effects is not enough to alleviate patient concerns, and may exacerbate anxiety or leave patients with outstanding questions, particularly in the absence of information to weigh up concerns against treatment benefit (Wells and Kaptchuk, 2012).
The majority of resources described the unknown timeline of progression to active TB but failed to indicate that LTBI can be persistent with (albeit to a lesser extent) or without treatment. This is important to communicate, as many younger patients may only have experience of treating acute or self-limiting conditions. Communicating the risk of progression to active TB is further complicated by the differing risk profiles observed across groups (e.g. contacts and migrants) (Abubakar et al., 2018) and the inability of current diagnostic tests to confirm viable dormant TB bacteria and accurately predict progression (Lalvani et al., 2019). Despite this, the majority of resources included generalised risk statements (e.g. 1 in 10 people with LTBI will progress to active TB), which may lead patients to form inaccurate representations around their own risk. Newly developed tools such as the Periskope.TB (http://periskope.org/tb-risk-predictor/), which take into consideration individual demographics and medical characteristics, may help to communicate personal risk to patients (Gupta et al., 2020). However, further research is required to understand how personalised risk estimates influence treatment decisions.
Similarly, the majority of resources inadequately addressed personal control. Previous qualitative work has demonstrated patient beliefs about the use of exercise and nutrition to manage their risk of developing active TB (Gao et al., 2015). Misconceptions concerning personal control can influence perceptions of risk and treatment necessity, affecting the ability to make informed treatment decisions. Personal control needs to be communicated accurately to patients with the limits pointed out. For example, if resources promote the benefits of a healthy lifestyle, they should also clearly state that this is not a substitute for LTBI treatment.
Patient education resources can support patients to make informed choices about their health. However, the difficulties and extent to which this can be achieved within the boundaries of public health agendas and screening programmes to eliminate TB in low-incidence settings should be acknowledged. Systematic programmes offer personal and public health benefits for some, but may disadvantage others through treatment that is potentially harmful, may be of no personal benefit, and which has negative health and social consequences (Degeling et al., 2017; Scandurra et al., 2020). In particular, anticipated or experienced stigma may have a negative influence on the uptake of screening and treatment but was not addressed by the included patient education resources.
The extended CSM is a useful model for addressing commonly asked questions about illness and treatment and can be used to inform future LTBI patient education resources. Similarly, including the views of people with lived experience of LTBI and relevant stakeholders can help to ensure resources are acceptable and sensitive to the priorities and values of the target community (Yardley et al., 2015).
This study analysed online LTBI patient education resources from UK-based organisations. Our search was restricted to Internet-based resources and more local materials may have been missed. Furthermore, while readability tests are useful in gauging how a patient might understand text, they offer little insight into how a patient might engage with a resource, which may be affected by the use of headings, imagery, tables, tone and ease of access.
Conclusion
Our searches found a modest number of UK LTBI patient resources, none of which fully addressed patient perceptions of LTBI and treatment, and promoted shared decision making. The quality of resources identified was variable in terms of accessibility, readability and theoretical content. All written resources failed to meet HEE reading age recommendations for patient materials, and only three were readily available in other languages. This is particularly worrying given the NHS and UK government priority to address health inequalities in UK multi-ethnic and migrant populations (Salway et al., 2020). Video animations may be a promising channel for health information delivery to groups with low literacy or limited English. Further research is now required to develop and test the acceptability and effectiveness of theory-based patient resources to support informed treatment decisions in LTBI.
Supplemental Material
sj-pdf-1-hej-10.1177_0017896921990066 – Supplemental material for Evaluating patient education resources for supporting treatment decisions in latent tuberculosis infection
Supplemental material, sj-pdf-1-hej-10.1177_0017896921990066 for Evaluating patient education resources for supporting treatment decisions in latent tuberculosis infection by Amy L Clarke, Tamilore Sowemimo, Annie SK Jones, Molebogeng X Rangaka and Rob Horne in Health Education Journal
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Given the nature of the study and the fact that all the resources analysed are publicly available, ethical approval was not required for this investigation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.