
Abstract
Objective:
Peer support interventions can be successful in enhancing physical activity (PA) in a variety of health-related contexts. However, the evidence base remains equivocal, and ways to integrate structured peer support within the context of exercise referral schemes (ERSs) remain unexplored. In this regard, few studies consider the prospective acceptability of peer support interventions. Prior qualitative exploration can elicit insight into factors likely to influence peer intervention success, thus maximising the likelihood of developing and implementing effective peer support interventions. This study assessed the prospective acceptability of a peer support intervention for exercise referral.
Design/Setting:
Individual semi-structured interviews were conducted with 14 ERS clients (n = 10) and providers (n = 4) across two ERS sites in the North West of England, UK.
Method:
Interviews covered preferred demographic and personal characteristics of ERS peers and prospective peer roles. Interviews were analysed using thematic analysis.
Results:
A desirable ERS peer was perceived as someone who was positive and empathetic, with good interpersonal skills. ERS peers were considered to present a promising opportunity to enhance the accessibility of emotional, motivational and informational support among ERS clients while alleviating burden on ERS providers.
Conclusion:
Study findings have relevance to the integration of peer support in comparable ERS contexts, highlighting the value of developmental research to refine peer recruitment criteria and to facilitate ownership and support among providers across a variety of health-related contexts.
Introduction
Peer support is a distinct form of social support where the relationship between providers and recipients of peer support is underpinned by recognition of perceived similarity and shared experience (Ginis et al., 2013). Peers are ‘experienced others’ who offer direct and/or indirect motivational support to aid participants in their pursuit of desirable behavioural or health and well-being outcomes (Matz-Costa et al., 2019).
Physical activity (PA) interventions that incorporate peer support can be effective across a variety of contexts (Hulteen et al., 2019), including schools (Owen et al., 2018) and community-based programmes (Beauchamp et al., 2018), although overall the evidence base remains equivocal (Croteau et al., 2014; Gorely et al., 2019). In part, this is due to ambiguity in relation to how peer support PA interventions are designed and implemented, such as how peers are recruited and operationalised (Matz-Costa et al., 2019).
Peer roles, intervention modality and the quality of relationships between peers and intended recipients of peer support are factors influencing the effectiveness of peer support PA interventions (Ginis et al., 2013; Matz-Costa et al., 2019). Therefore, peer support PA interventions are more likely to yield positive outcomes where they (1) recruit peers who are acceptable to participants and providers and (2) develop peer roles that are sufficiently meaningful to peers and participants. Notwithstanding this, there remains a lack of preliminary research to explore whether proposed peer support interventions are considered acceptable by those who will use and deliver them (Yardley et al., 2015).
A case study from exercise referral
Exercise referral schemes (ERSs) are PA interventions for adults (aged ⩾18 years) who are (1) experiencing or recovering from a physical and/or psychological health condition(s) and (2) failing to achieve 150 minutes of moderate-to-vigorous PA per week, or (3) regularly engaging in prolonged bouts of sedentary behaviour (National Institute for Clinical Excellence [NICE], 2014). ERSs traditionally offer 8–12 weeks of free, or discounted, access to a community-based PA environment (i.e. a gym) where participants perform PA under the supervision of a qualified exercise professional (Rowley, 2019).
ERSs typically have poor rates of completion (Pavey et al., 2011) and modest and variable effectiveness for facilitating meaningful health and well-being outcomes (Wade et al., 2020). Nonetheless, they remain popular, internationally widespread PA interventions (Arsenijevic and Groot, 2017), with research continuing to explore strategies to improve ERS completion rates and overall scheme effectiveness (Morgan et al., 2016). To this end, perceived social support is a known facilitator of ERS completion (Morgan et al., 2016). However, there remains a lack of research to document the development and/or implementation of a structured social support intervention for ERSs and limited practical guidance on how to embed greater social support opportunities within ERSs.
ERS participants who receive sufficient social support report greater levels of enjoyment and satisfaction (Vinson and Parker, 2012), relative to those who do not (Hanson et al., 2019). However, perceived social support varies according to the sociodemographic and personal characteristics of ERS participants, such as age and gender (Moore et al., 2013), and social anxiety (Hanson et al., 2019). In this regard, perceived social support is likely to remain low where (1) intended recipients of social support deem themselves to be categorically dissimilar to the individual(s) who are attempting to offer support (Haslam et al., 2012), and (2) individuals possess insufficient confidence and interpersonal skills to instigate social interaction with others. Recruiting and implementing peers who are representative of the ERS context offers a viable means of enhancing the perceived availability and accessibility of social support among ERS participants.
Notwithstanding this, ERSs have unique characteristics that may complicate the peer recruitment and implementation process. For instance, school (Owen et al., 2018) and community-based (Beauchamp et al., 2018) peer interventions typically recruit age- and/or gender-matched peers to promote perceived similarity. In contrast, the use of a similar peer recruitment strategy may be inappropriate within ERSs due to the extent to which participants vary by age and health condition. Moreover, ERSs are delivered by qualified exercise referral specialists with knowledge of an array of physical and psychological health conditions. Accordingly, this may make it less feasible for peers to assume ERS delivery roles relative to other PA settings, such as walking groups that routinely utilise peer walk leaders (Kritz et al., 2020). Thus, it is currently unknown what roles peers may perform to support ERS delivery.
This study documents a qualitative exploration of the prospective acceptability of a peer support intervention for ERSs from the perspectives of ERS participants and providers. Specifically, the aims of this study were (1) to elicit ERS participant and provider views on salient demographic and personal peer characteristics and (2) to identify contextually relevant peer roles.
Method
The exercise referral scheme context
Adults (18+ years) with long-term health conditions were referred by a general practitioner (GP) or self-referred to take part in a 12-week gym-based ERS in North West England. All ERS clients received a bespoke training programme of aerobic and/or anaerobic exercise following a 30-minute health assessment with an exercise referral scheme officer (ERO). Training programmes regularly recommended low to moderate intensity use of cardiovascular endurance machines, such as treadmills or exercise bikes, and/or weight resistance machines relative to participants’ health status. EROs supervised the PA behaviour of ERS clients who attended drop-in sessions within the gym. EROs allocated their supervision time variably according to several factors, such as (1) how many ERS clients accessed each drop-in session, (2) ERS client’s status as an experienced or inexperienced gym user and (3) the severity of ERS client’s reported health condition(s). As such, ERS provision was neither strictly one-to-one nor group-based, nor could ERS clients become accustomed to receiving a guaranteed amount of ERO supervision each week. Drop-in sessions were available throughout the week at varying times, for example, Monday and Thursday, 2– 4 p.m., Wednesday 11:30–1:30 p.m., and were also accessible to non-ERS community gym members. Participants completed a follow-up health assessment at week 12, signifying conclusion of their scheme involvement.
Study background
Details of this study’s conceptualisation and data collection and analysis procedures are presented in accordance with the Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines (Tong et al., 2007). The first author conducted all the interviews and had sufficient prior experience of undertaking qualitative research. Data collection for this study formed part of the first author’s doctoral research, comprising an evaluation and intervention co-development of the ERS. As such, the decision to recruit and implement ERS peer volunteers preceded data collection for this study, and the interviewer had a pre-existing professional relationship with ERS providers. The interviewer was introduced to ERS clients as an independent evaluator working in collaboration with ERS organisers.
Study design
The study adopted an ethnographic approach to identify desirable characteristics of ERS peers and to explore what roles peers can perform to support ERS delivery.
Participants
Institutional ethical approval was obtained prior to data collection (Edge Hill University, Ref: SPA-REC-2017-008). Convenience sampling was used to recruit 14 participants (7 women) between May and August 2019 who were either previous (n = 4) or current (n = 6) ERS clients, or responsible for ERS provision (n = 4). All participants identified as White British.
The age of ERS clients ranged from 56 to 88 years (70.4 ± 8.2 years). Key demographic characteristics of ERS clients are presented below (Table 1). ERS providers comprised three EROs and the operational manager who oversaw the scheme. The age of EROs ranged from 36 to 48 years (42 ± 4.9 years), with 10.5–25 years of professional experience delivering ERSs.
Demographic characteristics of exercise referral scheme clients.
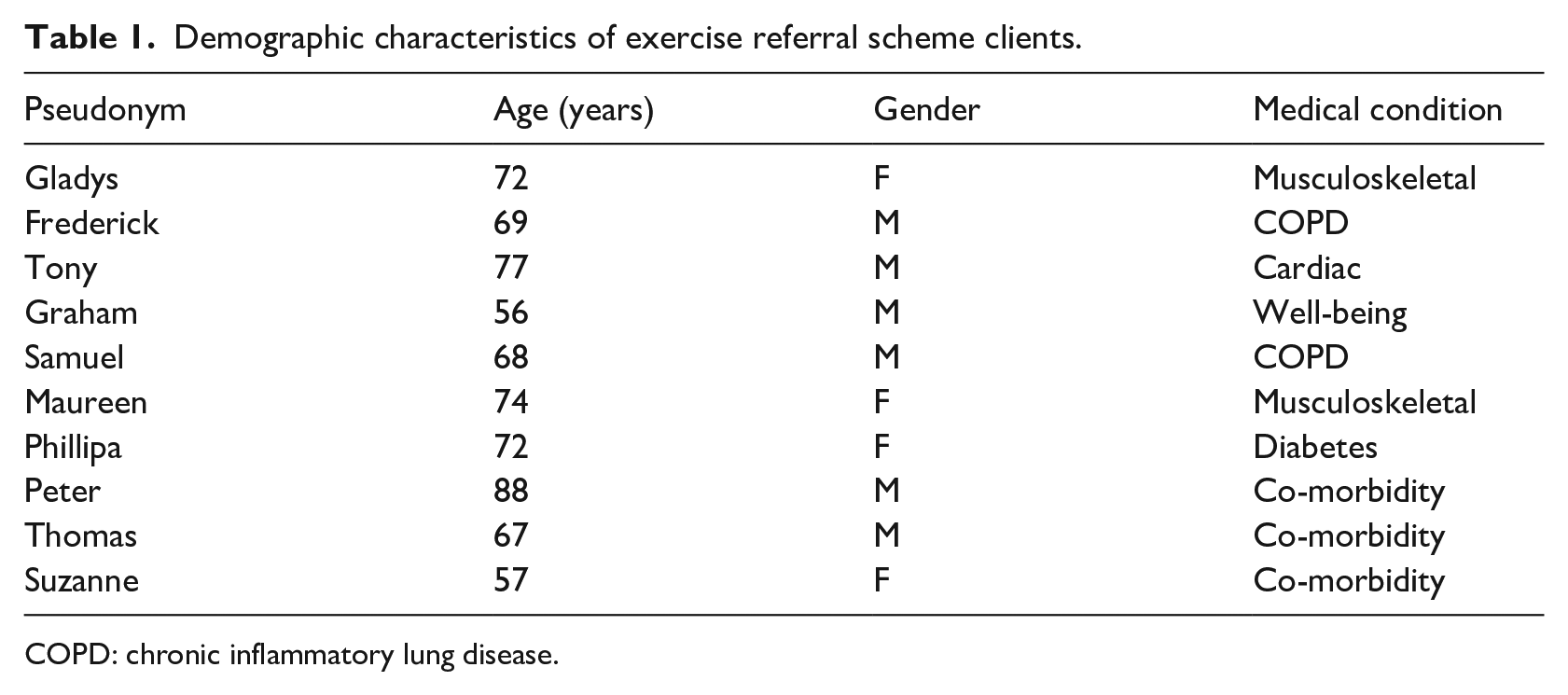
COPD: chronic inflammatory lung disease.
All interviews were arranged in consultation with EROs, who acted as gatekeepers (Turner and Almack, 2017). EROs approached ERS clients during face-to-face drop-in sessions to schedule interviews with the first author. Interview guides contained questions pertaining to demographic and personal characteristics of peers, as well as prospective roles. Interviews were conducted in a private room of the facility where the participant either attended or delivered drop-in ERS sessions. The interview with the ERS operational manager took place within a private room on the university campus. All interviews were one-to-one, except for one ERS client who opted to be interviewed in the presence of an ERO. All participants were given study information sheets and provided written and verbal consent prior to interview.
Interviews with clients and EROs ranged from 23 to 66 minutes (mean duration = 37 minutes) and 32 to 48 minutes (mean duration = 43 minutes), respectively. The interview with the operational manager lasted for 53 minutes. Participants were debriefed following the interview and given the opportunity to ask any further questions. Participants received no financial or material imbursement. All interviews were digitally recorded and transcribed verbatim. During transcription, all identifying information pertaining to the participants themselves or other ERS clients or providers mentioned in the interviews was replaced by pseudonyms to ensure participant anonymity. Transcripts were not directly returned to clients, although member reflections were sought from ERS providers to affirm, or challenge, interpretations of analysed data (Tracy, 2010).
Data collection encompassed all ERS providers responsible for the delivery of drop-in sessions. Data collection for ERS participants ceased following a reflexive consideration of the quality and coverage of collected data and the cost–benefit relationship regarding whether the additional time required to collect and analyse further data would sufficiently enhance the peer recruitment and training processes (Braun and Clarke, 2019).
Data analysis
The study adhered to Braun and Clarke’s (2013) guidance for conducting thematic analysis (TA). TA was performed at a semantic level and primarily adopted a deductive, data-driven approach to identify perceived prototypical characteristics and behaviour (i.e. roles) of desirable peers within an ERS context. The TA also incorporated elements of inductive analysis to explore unifying aspects of an ERS social identity. Specifically, the interviews collected data on desirable, identity-congruent characteristics and behaviours of prospective ERS peers rather than representing a simple aggregation of equally weighted personal preferences.
The first author conducted data analysis in accordance with the following six-step process (Braun and Clarke, 2013): first, data immersion was achieved via conducting interviews, listening to audio files, transcription of audio recordings, and reading and re-reading transcripts. This facilitated intimate data familiarity and contributed towards subsequent sense making and knowledge construction. Second, chunks of the data set were assigned codes in relation to the study aims. The third and fourth steps involved the identification of codes reflecting similar issues and pooling these codes together to construct potential themes. Fifth, potential themes were scrutinised for suitability and consistency to ensure each code was appropriately reflected by its overarching theme. Finally, after establishing a final thematic structure, illustrative quotes were extracted from the data set as supporting evidence.
Results
Participants identified desirable characteristics and behaviour of prospective ERS peers. Participant preferences were subsequently organised into three prominent themes to highlight (1) desirable peer demographic characteristics, that is, what ERS peers should look like and/or what status they should hold, (2) desirable peer personal characteristics, that is, how ERS peers should interact with ERS clients and providers, and (3) peer roles, that is, how peers can support ERS clients towards scheme completion.
Desirable demographic characteristics of ERS peers
This theme explored whether participants considered peers of a particular age, gender or health status to be better suited to ERS peer roles.
Collectively, ERS clients regarded age and gender to be largely inconsequential to an individual’s ability to act as an ERS peer. This was reflected by Samuel’s (client, 68 years) response when asked whether he would prefer to interact with peers of a certain age: ‘They can be 5 years old; they can be 100 years old. Doesn’t matter, does it? Age is only a number’. ERS clients, like Samuel, had no preference for recruiting peers of similar ages to themselves. Equally, ERS clients did not recommend recruiting peers of the same gender as themselves. When asked about his preferences, Tony’s (client, 77 years) response below illustrates his relative ambivalence concerning desirable peer demographic characteristics: I don’t think that [peer age or gender] really matters. I think that the thing is really, they just need to have a positive . . . they have to have been through the experience and they have to be positive about the whole thing.
Here, Tony alludes to a requirement for peers to meet certain criteria to demonstrate their role suitability. However, for him, age and/or gender similarity were of low value. In contrast, other ERS clients, like Phillipa (72 years), highlighted the potential advantages of recruiting peers with similar health conditions to themselves: [Peers with similar health conditions] would know . . . what they’re going through and . . . what issues they’ve faced, or what they’re going to face. And maybe on that . . . they can say maybe, ‘don’t do it this way, do it that way, because it’ll be easier for you.
These ERS clients anticipated peers with similar health conditions to themselves to be able to draw from personal experiences to offer tailored support. However, as articulated by Suzanne (client, 57 years), most clients suggested a more general experience of ‘going through something’ as providing a sufficient basis for demonstrating a shared understanding between peers and ERS clients: ‘Usually, if you’ve gone through something yourself, you’ll have some idea. You can relate to those people because you’ve been there’. Suzanne’s account here may point to a common psychological coping mechanism(s) that binds ERS clients together irrespective of the individual differences related to their specific health-related condition(s).
ERS providers adopted a more pragmatic perspective on desirable demographic characteristics of peers. Sharon (provider, 41 years) had extensive experience of overseeing ERS delivery and suggested peer recruitment strategy should align with the prevailing demographic characteristics of ERS clients: ‘I think someone who’s 50+ (years) . . . more than 50% of our clients are 50+ (years) . . . I think in that sense, the age thing is important because they can then relate more to the clients’. Sharon’s response reflected the views of other ERS providers, believing peers who are demographically similar to the majority of ERS clients will have better acceptability. This was similarly evident when providers discussed peer gender preferences. For instance, Mary (provider, 48 years) suggested no benefit can be gleaned by specifically recruiting male or female ERS peers: ‘I don’t think it matters, male or female . . . I think it’s more of an equal thing now, rather than being predominantly female dominated’. Critically, Sharon and Mary’s responses were specifically tied to recruiting peers who were demographically comparable with the majority of ERS clients as opposed to suggesting peers of a specific age or gender would be better suited because of such characteristics.
Overall, the sole demographic criterion deemed essential by both ERS clients and providers was for peers to have completed an ERS prior to taking on a peer role. This was reflected by the views of another client, Frederick (69 years): ‘I do think that it would be important that they had been through the scheme, yeah. Because otherwise, they’re just another person coming in, aren’t they? You don’t know the ins and outs of it’, and also by Kevin (provider, 36 years): You’re looking for someone who has completed the service, someone who’s done well on the service, because obviously, there’s no point in having a champion if you’ve not done very well. You can’t motivate somebody else to do a good job, when you’ve not put the effort in yourself.
Desirable personal characteristics of ERS peers
Participants cited several personal characteristics as being key to the success of future ERS peers. Principally, ERS peers needed to be ‘positive people’, characterised in terms of the ability to demonstrate an adept conversational style and a general gregariousness. This was reflected by Phillipa’s (client, 72 years) description of desirable peer personal characteristics: ‘I think they’d have to be quite outgoing . . . a very sociable person . . . to be able to talk to anybody,’ and Gladys’ (client, 72 years) description of the same: ‘It’s someone that you can go and speak to and you don’t have to feel daft or stupid . . . someone like that who puts you at ease’. Phillipa’s account indicated a requirement for ERS peers to have sufficient conversational skills to interact with a broad range of clients. This may reflect not only the extent to which ERS clients vary in age, gender and health status, but also the extent to which ERS clients may differ in their communicative style or social anxiety. Gladys’ account reflected clients’ typical lack of experience of community-based gym environments prior to enrolling on an ERS. Because of this, new ERS clients may feel a need to ask further questions or to seek reassurance. Thus, it was important for peers to be friendly and approachable individuals to help new ERS clients feel at ease in unfamiliar surroundings. Gladys went on to describe a particular instance when a fellow ERS client had experienced social anxiety: ‘I wasn’t so bad, but when [her friend] came [to the ERS] for the first time he was absolutely terrified’. As such, peers who exude positivity can help combat new ERS client’s initial trepidations.
Suzanne (client, 57 years) considered empathy to be the most critical peer personal characteristic: ‘If [peers] don’t have empathy, it’s not going to work. Because you’ll find that people that don’t have empathy, tend to get impatient very quickly’. Suzanne’s comment may also speak to the heterogeneity of ERS clients, this time in relation to differences in physical capabilities. Empathy may be especially salient within an ERS context as there are relatively few characteristics that bind clients together. However, as explained by Peter (client, 88 years), there is at least one defining characteristic which ERS clients do share: ‘You had a common cause, you were ill . . . and you were trying to recover. That was it. So, there was no . . . “well, he’s too posh for me,” or, “he’s too scruffy for me”’. Ultimately, desirable ERS peers are those who demonstrate empathetic understanding of the multitude of ways in which ERS clients differ while also appreciating how ERS clients are similar.
In addition, providers highlighted the need for peers to have competent listening and organisational skills. Kevin (provider, 36 years) considered these skills to be critical to ensure peers suitably adhere to their given roles and responsibilities: ‘[A desirable peer] would be someone who is able to follow instruction, to work within the boundaries of what we’re asking them to do and go no further’. This belies a conceptualisation of the ERS peer role as operating under the authority of the existing EROs. Sharon (provider, 41 years) described an example of undesirable peer behaviour: ‘As long as they don’t run away with themselves, giving advice that is, potentially, not professional advice . . . knowing that is not their role within the gym’. Accordingly, ERS peers need sufficient understanding of where they are situated within the ERS delivery framework. Specifically, providers, like Sharon, were steadfastly opposed to the possibility of peers offering clients technical advice related to the dose, intensity or choice of exercise behaviour.
Roles and responsibilities of ERS peers
Participants highlighted several roles peers can perform to provide additional emotional, motivational and informational support to those accessing ERSs. Phillipa (client, 72 years) described how peers can positively influence a client’s mood and attitude towards exercise on ‘bad’ days: ‘Maybe you’ve gotten up and you don’t feel that good, you’re going to the gym and you don’t feel like doing it . . . you know, if you can just talk to someone and . . . they bully you up’. In this regard, peers can provide additional one-to-one emotional support to ERS clients using previously discussed personal attributes such as positivity and humour.
Thomas (client, 67 years) suggested that peers could help to create a more communicative and socially supportive ERS environment: If you’ve got somebody who was introducing people to each other . . . because some people can be quite shy, as you’re aware. I’m not, I’m quite open. But I’ve noticed . . . some people you can say, ‘good morning’, to and they’ll give you a nod, they’re very difficult to engage in conversation.
Here, Thomas draws from personal experience to highlight the difficulties some ERS clients face when attempting to socially engage their fellow scheme users. Peers who can build and maintain positive one-to-one relationships with ERS clients may be able to further enhance the ERS client experience by creating additional opportunities for social interaction among ERS clients themselves.
Sharon (provider, 41 years) explained how peers can promote feelings of resilience and persistence among ERS clients, qualities deemed especially valuable during the early stages of participation in an ERS: It’s proof to [clients] that . . . you can do it, basically. And, especially in weeks 1, 2, 3, when people are struggling because they’ve never been in a gym before . . . and you’ve got someone there who just looks like a normal, everyday person, to say, ‘well, I did it. If I can do it, you can do it’.
Peers can thus offer both direct and indirect motivational support to ERS clients by acting as relatable physical role models and providing positive verbal reinforcement.
The introduction of ERS peers also creates an additional outlet for clients to seek informational support. Participants, like Phillipa (client, 72 years), believed the introduction of peers would increase opportunities for clients to ask questions and seek reassurance on their exercise behaviour: I think it would be a good idea for older people to be able to go to someone and just say . . . ’ What do you think about this?’, ‘Do you think I’m doing this right?’, ‘Do you think I’m doing that right?’, instead of going to [exercise referral officer] all of the time.
As such, peers can act as information providers to simultaneously lessen the burden on EROs and reduce the number of ERS clients who may opt to ‘suffer in silence’ rather than reaching out to EROs for help.
Discussion
In this study, participants discussed preferences for demographic and personal ERS peer characteristics and described potential peer roles. Collectively, ERS clients and providers were amenable to recruiting peers who (1) had experience of managing a health condition and (2) had previously completed an ERS. Desirable ERS peers were those who exuded positivity and empathy and possessed sufficient interpersonal skills to initiate social interaction with a heterogenous ERS client base. ERS peers who met these criteria were seen as able to provide additional emotional, motivational and informational social support to ERS clients.
Overall, ERS clients did not indicate a preference for recruiting peers who were of a similar age, or the same gender, as themselves. ERS providers, on the contrary, recommended recruiting peers aged 50 years or older to align with the prevailing demographic characteristics of ERS clients, although also reported no preference for peer gender. Matching peers and the intended recipients of peer support based on age and/or gender similarity is common among successful peer-based PA interventions (Beauchamp et al., 2018). This practice reflects a preference for adults to exercise alongside individuals of a similar age to themselves (Beauchamp et al., 2007, 2018). In contrast, preferences for gender similarity are less pronounced in exercise settings (Beauchamp et al., 2018). It is interesting that ERS provider preferences for peer demographic characteristics mirror Beauchamp et al.’s (2018) findings. This may reflect ERS providers being able to draw from their prior experience to identify key features of previously successful schemes.
Fundamentally, shared demographic characteristics provide a basis for perceived similarity among PA group members. In heterogenous PA settings, such as ERSs where participants may vary by age, gender and health status, it is important to identify the characteristics which participants share. In this study, participants regarded prior scheme completion and the shared experience of ‘going through something’ as essential requirements for prospective peers. Here, shared experiences of poor health enable the development of trustworthiness and rapport between peers and clients (Englander et al., 2020). Moreover, ERS clients may experience additional benefits by interacting with peers with the same health condition as themselves. However, the heterogeneity of current ERSs may inhibit the specific recruitment of peers with matching health conditions.
Desirable ERS peers are positive and approachable individuals who can confidently engage in social interaction with ERS clients. Positivity was cited as a salient peer personal characteristic (Kritz et al., 2020), in part because it helps peers to allay participant concerns by normalising feelings of apprehension and providing reassurance for the future (Kohut et al., 2018; Kritz et al., 2020). Upon entering ERSs, clients typically experience social anxiety due to a common lack of previous exposure to a community-based gym setting (Moore et al., 2011). This anxiety stems from personal health-related concerns which may be compounded by upward social comparisons related to the physical appearance and functioning of fellow scheme users (Morgan et al., 2016). In this study, participants suggested early interactions with positive, gregarious ERS peers can lessen client’s experiences of social and health-related anxiety. Participants also highlighted the fundamental importance of peer empathy. Peer demonstrations of empathy promote reciprocal awareness of a shared journey towards enhanced health and facilitate the development of positive peer–recipient relationships (Moon et al., 2017). Desirable ERS peers were identified to be those who recognised and promoted the shared journey of ERS clients towards better health, irrespective of the client demographic heterogeneity.
In addition, ERS peers must possess adequate interpersonal and organisational skills. These skills are considered fundamental for peer implementation success in health- and PA-related contexts (Tobias et al., 2010) such as community-based peer-led PA programmes for older adults (Kritz et al., 2020). ERS providers highlighted the critical importance for peers to rigidly adhere to agreed roles and responsibilities prior to their implementation. Adherence to agreed role boundaries is essential to ensure client safety within health-related contexts (Englander et al., 2020). This is particularly relevant to ERSs, which involve a prescriptive PA component and are accessed by those with complex health needs. Providers proposed that peers act as supplementary sources of support under their supervision and should not offer advice relating to ERS client’s PA type, mode or intensity.
Consistent with Kritz et al. (2020), prospective peers were envisioned to provide additional one-to-one emotional support to ERS clients by regularly instigating social interaction with them and enquiring about their well-being. More frequent opportunities for ERS clients to socially interact with peers with comparable life experiences may facilitate decreased feelings of isolation and increased belonging (Moon et al., 2017). In this regard, peers can act as the catalyst for increasing ERS client’s social capital by expanding opportunities for social interaction. Edmunds and Clow (2016) found a peer-initiated support network facilitated the development of companionship, camaraderie and exercise group identity, features associated with enhanced PA in a workplace context. In turn, this study demonstrates that ERS clients are prospectively receptive to the introduction of peers, partly due to a similar belief that peers will create additional opportunities for the development of companionship and camaraderie within an ERS context. Moreover, this study provides further detail regarding who should be recruited to ERS peer roles and what roles peers should perform in order to facilitate increased social capital among ERS clients.
Limitations
This study is not without its limitations. For instance, the use of EROs as gatekeepers to recruit ERS clients for interview may have led to selection bias, with EROs potentially opting to approach those they considered likely to portray the ERS and/or themselves in a positive light. Notwithstanding, the likelihood of such bias influencing client’s responses is low given the prospective focus of the interviews. In addition, this study’s use of convenience sampling may have facilitated the recruitment of a somewhat atypical set of ERS participants aged 55 years and above. Those aged 55+ years are more likely to uptake and complete ERSs (Kelly et al., 2017), and thus, sample members may have been easier for EROs to recruit. Future study is needed to explore whether ERS peer preferences differ among younger ERS clients. Alternatively, participants aged < 55 years may benefit from recruiting younger peers who meet the desirable ERS peer personal characteristics identified here.
Conclusion
This study found participants and providers to be amenable to the integration of peers to increase social support opportunities within ERSs and identified desirable peer characteristics and roles to inform future recruitment. Desirable ERS peers were those with existing health conditions who have completed ERSs and have a positive and empathetic demeanour. Such peers could work alongside ERS providers to help clients access emotional, motivational and informational support. ERS providers meantime can focus more explicitly on the prescriptive exercise component of schemes.
Beyond its substantive findings, this study provides insight from key stakeholders on how best to integrate peer support within ERSs. Moreover, its exploratory approach can be utilised across a variety of health-related contexts seeking to assess the perceived need and incorporate structured peer support. Providers may find it helpful to follow the design of this study in order to inform bespoke peer recruitment and implementation practice within heterogeneous community-based PA settings.