
Abstract
It is widely known that marginalized families of young children with disabilities have inequitable access to evidence-based practices within publicly funded systems of care, such as the Part C early intervention (EI) system. One factor contributing to this inequality is providers’ limited cultural self-efficacy, which can be defined as the confidence and competence to engage effectively with families from different cultural or linguistic backgrounds than their own. However, little is known about how to assess cultural self-efficacy specifically among EI providers. Therefore, this study aimed to adapt and validate the Cultural Self-Efficacy Scale in Early Intervention (CSES-EI), a scale to assess EI providers’ cultural self-efficacy when working with marginalized families. We used a modified Delphi method to adapt 32 items from an original scale into the CSES-EI. A total of 201 EI providers from diverse professional backgrounds completed the survey. Data analysis involved exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and multiple regression to assess the reliability, validity, and underlying structure of the scale. The CSES-EI demonstrated strong internal consistency (α = .91, ω = .94) and a three-factor structure accounting for 47.9% of the variance. Thematic analysis of open-ended responses revealed that EI providers emphasized family-centered coaching, cultural competence, and the need for flexibility when working with marginalized families. Findings underscore the importance of culturally responsive practices in EI and suggest that professional development targeting cultural efficacy is essential for improving service delivery with diverse populations. This validated tool provides a foundation for assessing and enhancing cultural self-efficacy among EI providers.
Early intervention (EI) is a publicly funded service in the United States that is federally mandated under Part C of the Individuals with Disabilities Education Act (IDEA, 2004). As a public service, it is a vital first step for many families entering the often lifelong journey of special education and disability services. In EI, evidence-based practices (EBPs) are used to ensure positive outcomes of young children with disabilities and their families, and most providers and agencies in EI are mandated by the IDEA to deliver EBPs that have empirical evidence behind them. EI providers work with infants and toddlers who have developmental delays, disabilities, or are likely to receive a diagnosis later in life. Under the auspices of IDEA Part C, these individuals provide various EBPs from disciplines including occupational therapy, speech language pathology, developmental therapy, physical therapy, and social work.
Many families who receive EI services are from historically marginalized backgrounds with limited cultural capital (Yosso, 2005). In the U.S. context, these include BIPOC (Black, Indigenous, and People of Color) families, immigrant or refugee families, as well as households that primarily speak languages other than English. Such families frequently encounter barriers related to language access, socioeconomic inequities, and systemic bias when navigating early intervention and special education systems that prioritize mainstream cultural norms (Yosso, 2005). Families living in rural or low-income urban areas may also face limited availability of culturally and linguistically matched providers. For these families, participating in EI is especially important as they are reported to naturally rely on the EI system of care and EI providers as the main gateway for services (Vohra et al., 2014). Unfortunately, access to EBPs is inequitable, and these disparities are especially highlighted among marginalized families. For example, caregiver coaching is an evidence-based delivery mechanism that many EI services are based on to efficiently deliver EBPs within time and resource constraints (Kemp & Turnbull, 2014). However, EI providers have reported language and cultural differences as major barriers to caregiver coaching in EI (Straiton et al., 2023; Tomczuk et al., 2022). Similarly, Asian immigrant caregivers of young children in EI have also reported that EI providers do not exhibit cultural responsiveness during their sessions, such as not speaking directly to the caregivers when there was an interpreter present or failing to teach caregivers what they could do outside the treatment sessions to promote skill and strategy generalization (Kang et al., 2023).
Cultural responsiveness extends beyond surface-level practices; it involves actively bridging the gap between the general clinical practice and the unique lived realities of diverse families (Gay, 2018). Gay's (2000, 2010, 2018) culturally responsive teaching framework emphasizes that educators’ knowledge of cultural diversity and commitment to using students’ cultural funds of knowledge make learning more relevant and effective. Similarly, Ladson-Billings (1995) highlights that along with academic success (developmental milestones in the context of EI), cultural competence and critical consciousness are key components to culturally relevant pedagogy. In a more recent work by Paris and Alim (2017), culturally sustaining approaches encourage educators to not only respect but sustain the diverse culture, language, and racial backgrounds rather than encouraging assimilation. Furthermore, Artiles (2023) also showed the importance of interventions that place families as active collaborators in order to address the issues of historical marginalization. These frameworks are critical to understanding and promoting cultural self-efficacy in EI providers as marginalized families often report mismatch and misalignment between traditional content and delivery of EBPs and their lived sociocultural realities and cultural values in parenting (Calzada et al., 2013; Castro et al., 2010). In addition, these families are more likely to receive a developmental disability diagnosis for their child later when compared to their White, English-speaking, or mainstream cultural group counterparts in the United States (Constantino et al., 2020; Weiss et al., 2024). This is problematic as such experience results in delayed access to intervention and support tailored to their needs.
These disparities and disproportionality are highly complex issues that are multifaceted with different contributing factors. One factor contributing to this is providers’ cultural self-efficacy in a field that has an increasingly diverse population. Despite the diversity of service recipients in Part C EI services, the workforce is predominantly White. In 2019–2020, less than 50% of the children receiving Part C EI services in the United States were White, with Latinx children making up 27.9%, followed by 12.4% of Black and 4.5% of multiracial children (IDEA Data Center, n.d.). On the contrary, a recent survey of professionals who provide EI special instruction revealed that 83% of the respondents (N = 1,008) identified as White (Childress et al., 2025). This mismatch of racial and ethnic composition, coupled with the limited access to culturally responsive training among EI providers, has contributed to the disparities in access to EBPs.
EI providers’ confidence and competence in working with these diverse populations is also crucial in addressing the disparities in access to EBPs. The theoretical construct of self-efficacy was developed by Bandura (1997) who defined self-efficacy as “beliefs in one's capabilities to organize and execute the courses of action required to produce given attainments” (p. 3). When this concept is applied to cultural self-efficacy, therefore, it refers to the providers’ self-perceived confidence and competence when working with families who have different backgrounds than their own (Kang et al., 2023; Zhang & Bennett, 2003). These constructs are also intertwined with the concept of agency, the ability and responsibility of providers to act as advocates and collaborators in challenging inequitable systems and sustaining families’ cultural strengths (Gay, 2018; Ladson-Billings, 1995; Yosso, 2005). There are field-specific definitions and applications of cultural self-efficacy in closely related fields. In fields such as mental health or nursing, cultural self-efficacy refers to professionals’ confidence in their ability to effectively communicate with individuals from diverse backgrounds and provide responsive care that is sensitive to these differences (Rice & Harris, 2021). Such responsive care practices include: (a) understanding and respecting cultural differences, (b) maintaining honest intercultural communication, and (c) adapting care to the needs of their patients (Chan & Sy, 2016).
In the context of EI, providers with a greater sense of cultural self-efficacy are more likely to engage in effective communication and build stronger relationships with families, which are essential in culturally responsive EI because of its strong focus on family-centered practices (Wray & Mortenson, 2011). EI providers have reported perceived barriers and needs across multiple levels related to accessing professional development (PD) focused on culturally responsive practices. Lee et al. (2024) conducted a qualitative study using individual interviews with 15 EI providers to examine determinants (e.g., barriers, facilitators) of providing culturally responsive EI. In this study, providers reported barriers that exist across individual, organization, and system levels. At the individual level, providers reported barriers like (a) cultural clash between the provider and families that they serve, and (b) limited cultural awareness of providers. At the organization level, the reported barriers included (a) limited opportunity for PD to increase their competency in working with families, (b) limited organizational climate or priority for cultural responsiveness, and (c) limited capacity to effectively collaborate with interpreters.
Despite the pressing need to create PD opportunities and implement policy-driven guidelines to increase cultural competence and self-efficacy, very little is known about measurements for cultural self-efficacy in EI and in the broader field of special education. There are some tools to measure self-reported cultural efficacy in closely related fields, such as in general education teacher training (Siwatu, 2007), and nursing (1993; Herrero-Hahn et al., 2017). However, it is necessary to examine a field-specific tool that will help us better understand how EI providers can enhance cultural responsiveness in their daily practices and EBP implementation with marginalized populations. Such a specialized instrument would also help us to reflect the complexities related to cultural, linguistic, or ethnic diversity, and provide more accurate assessments of providers’ attitudes, knowledge, and skills when they work with marginalized families. This also has critical implications for how we design and implement PD that plays a vital role in how effectively EI providers engage with marginalized families. Having a robust and psychometrically sound instrument will help professionals reflect on their own practices, and organizations to assess the cultural-self efficacy of their providers. The tool will also aid in identifying areas where professionals need additional support or training to achieve culturally responsive practices.
Therefore, the purpose of this study was to fill this notable gap in the field of special education by developing, adapting, and validating the Cultural Self-Efficacy Scale in Early Intervention (CSES-EI). The following research questions guided this study: (1) What are the psychometric properties of the CSES-EI in terms of reliability and validity? (2) What is the underlying factor structure of the CSES-EI? (3) What is the predictive value of demographic and professional practice variables on EI providers’ self-efficacy? and (4) What are providers’ experiences providing culturally responsive EI?
Method
Theoretical Frameworks
To answer these research questions, this study was guided by Dunst (2022) Adapted Family Social Systems Theory, which posits that child learning and development are influenced by both informal and formal social networks and resources, including professional supports such as EI providers, and the ways in which they collaborate with family members. This framework informed our research design by integrating a modified Delphi method for scale adaptation with professionals who collaborate with minoritized families in EI. Moreover, we were also informed by Romijn and colleagues' (2021) framework of PD in which practitioners’ knowledge, skills, attitudes, beliefs, and expectations interact with their own behaviors and practices through reflection, and how these factors are shaped by the context of the learners (e.g., culture, family background) as well as the PD in which providers participate. This framework informed our data analysis and interpretation of the adapted scale across providers’ awareness, knowledge, and skill domains. Finally, and most importantly, the culturally responsive (Gay, 2018), relevant (Ladson-Billings, 1995), and sustaining (Paris & Alim, 2017) frameworks along with Artiles's (2023) framework on culturally responsive interventions informed how we synthesize and incorporate suggestions from the panel experts to finalize the adaptation of the scale.
Scale Adaptation
We began our process by identifying the Cultural Competence Self-Assessment Checklist (CCSC; Central Vancouver Island Multicultural Society, 2012), which was created to help individuals assess their multicultural competence. We received permission from the organization to adapt this scale for the purpose of research. The original CCSC comprised 36 items across three constructs including: (a) awareness, (b) knowledge, and (c) skills. Each item was rated on a 4-point Likert scale, ranging from 1 (never) to 4 (always/very well), based on how much the respondents agreed with each item. The original CCSC was not psychometrically validated as it was not used for research purposes.
To adapt the CCSC for use in EI context, we utilized a modified Delphi method (Eubank et al., 2016) to adapt the items in an iterative process. We created an online questionnaire and sent it to a panel of 11 experts in the fields of EI, special education mental health, cultural adaptation, and culturally responsive practices with marginalized families. This panel represented a variety of disciplines, including faculty members in special education, speech-language pathology, family and human services, and psychology, and most experts self-identified as being bilingual and/or bicultural. The panel was provided with the context regarding the purpose of the CSES-EI, the constructs we aimed to measure, the intended target population, and the goal of incorporating their feedback to strengthen the scale's cultural validity and relevance. Given their respective expertise and lived experiences as bilingual individuals, BIPOC, and/or members of marginalized communities, panelists were invited to reflect on the relevance, clarity, and appropriateness of each item for EI providers working with diverse families. Panelists’ feedback was informed by their professional practice in early intervention and their understanding of cultural and linguistic diversity, rather than a formalized epistemological framework. These experts provided feedback related to each item as well as general feedback about how this scale may be used in the context of EI providers working with marginalized families. After receiving all responses, we synthesized their feedback on a spreadsheet and adapted the scale. In this adapted CSES-EI, a total of 32 items remained with each item on a 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). We changed from a 4-point Likert scale to a 5-point scale to allow participants a neutral option, enabling them to express uncertainty or neutrality rather than having to choose the degree of their agreement.
Data Collection and Recruitment
Then, with the approval from the University's institutional review board, we distributed the online survey hosted in REDCap through social media and emails to organizations or individuals who work with EI providers. A participant was eligible to participate in this study if they: (a) were 18 years and older; (b) had experience providing interventions to a child receiving EI services; (c) had experience working with children and families from marginalized backgrounds; and (d) were able to complete all survey instruments in English. Providers from any professional background were eligible to participate to reflect the diverse nature of EI service delivery. Each participant automatically entered a raffle for a $25 electronic gift-card with 10% chance. All participants were recruited online from April 2023 to April 2024, and a total of 201 participants completed the survey.
The survey included (a) demographic questionnaire, (b) CSES-EI, and (c) Cultural Competence Assessment (CCA; Schim et al., 2003). The demographic questionnaire included questions about participants’ race and ethnicity, use of language, country of origin, education level, type of organization, professional background, years of experience, prior training in cultural competence, as well as optional write-in responses on how they provide culturally responsive EI services to marginalized families. Given that cultural self-efficacy is conceptually linked to cultural competence where self-efficacy reflects confidence and perceived ability, we selected the CCA as a comparison measure. The CCA was developed to assess cultural competence among healthcare providers, and includes 25 items across the subscales of cultural awareness, sensitivity, and competence behaviors. Previously, several studies have evaluated psychometric properties of the CCA (Doorenbos et al., 2005; Suarez-Balcazar et al., 2011; Schim et al., 2003). For example, the CCA demonstrates strong construct validity, with confirmatory factor analysis in a sample of 477 practitioners supporting a three-factor model (awareness/knowledge, skills, and organizational support) that showed excellent model fit (CFI and NNFI > .95, RMSEA < .06) and high reliability (α > .90). In addition, based on a meta-analysis of 57 studies (Lin et al., 2017), the CCA was identified as one of the most psychometrically sound instruments for healthcare providers, showing acceptable construct validity and good internal consistency. The CCA's strong psychometric properties and its established use in assessing cultural competence made this measure ideally suited to assess the convergent validity of the CSES-EI. This alignment allows for a comprehensive evaluation of CSES-EI as both instruments assess cultural self-efficacy through similar constructs.
Data Analysis
Quantitative Analyses
All analyses were performed using statistical software R with the implementation of psych (Revelle & Revelle, 2015) and lavaan packages (Rosseel, 2012). We used descriptive statistics to summarize the demographic information reported in the survey. Then, we conducted a series of analyses to evaluate the psychometric properties of the CSES-EI. First, we assessed the CSES-EI's internal consistency using Cronbach's alpha and McDonald's omega to determine reliability. Screeplots based on eigenvalues and parallel analysis were conducted to identify the number of underlying factors. Exploratory Factor Analysis (EFA) was then used to identify the factor structure, followed by Confirmatory Factor Analysis (CFA) to validate this structure. For EFA, we employed oblimin rotation and the ordinary least square (OLS) method to find the minimum residual (MR) solutions. In addition, we used a polychoric correlation matrix given that the responses were recoded as ordinal (i.e., 5-point Likert scale). For CFA, we estimated the model using the weighted least square mean and variance adjusted (WLSMV) method to take ordinal responses into account. To establish convergent validity of the CSES-EI, we computed correlations between the CSES-EI subscale scores and the CCA total scores. Finally, we employed multiple regression analyses to identify demographic and professional practice predictors influencing CSES-EI scores.
Qualitative Analysis
To analyze the optional write-in responses, we employed an inductive approach to thematic analysis (Braun & Clarke, 2006) in which we familiarized ourselves with the data, generated initial codes, identified and reviewed themes, and produced the final report. Two members of the research team engaged in this iterative process to analyze all write-in responses to ensure rigor and consistency in the analysis process.
Positionality of the Research Team
Our research team comprises individuals with diverse professional and personal experiences in EI and cultural competence. All authors identify as being bilingual and/or bicultural. Most authors have years of experience in working directly with children with disabilities and their families from minoritized backgrounds in different capacities, including board certified behavior analysts, early interventionists, speech and language pathologist, researchers, and faculty members. To mitigate potential biases, we engaged in reflexivity throughout the analysis process, including discussions about our implicit assumptions and biases and how they might shape the decision-making process in this study.
Results
Participants’ Demographics
Data were collected from 201 EI providers who represented 35 states and Washington D.C. with most participants from the states of Washington (n = 29; 14.4%), Utah (n = 21; 10.5%), Texas (n = 18, 9.0%), and California (n = 15; 7.5%). Most participants reported speaking English as a primary language (n = 164; 81.6%) and the United States as their country of origin (n = 187; 93%). In terms of race and ethnicity, the majority of participants identified as being White (n = 190, 77.5%). This was followed by Black participants (n = 27; 11.0%), Latinx participants (n = 18; 7.4%), and Asian (n = 6; 2.5%). Participants reported a broad range of educational attainment with 27.9% with bachelor's degree (n = 56), 58.7% with a master's degree (n = 118), and 7.5% with a doctoral degree (n = 15). See Table 1 for a description of providers’ demographic characteristics.
Participant Demographic Information.
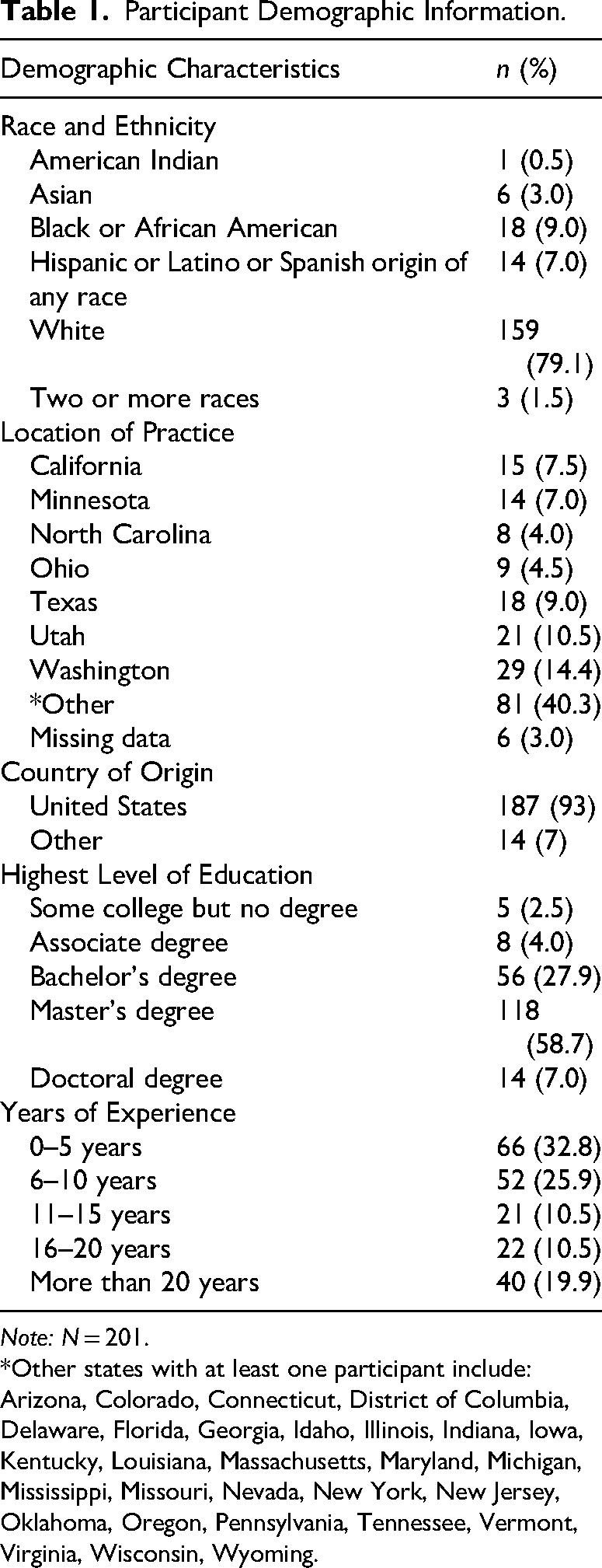
Note: N = 201.
*Other states with at least one participant include: Arizona, Colorado, Connecticut, District of Columbia, Delaware, Florida, Georgia, Idaho, Illinois, Indiana, Iowa, Kentucky, Louisiana, Massachusetts, Maryland, Michigan, Mississippi, Missouri, Nevada, New York, New Jersey, Oklahoma, Oregon, Pennsylvania, Tennessee, Vermont, Virginia, Wisconsin, Wyoming.
Participants’ EI and Coaching Practices
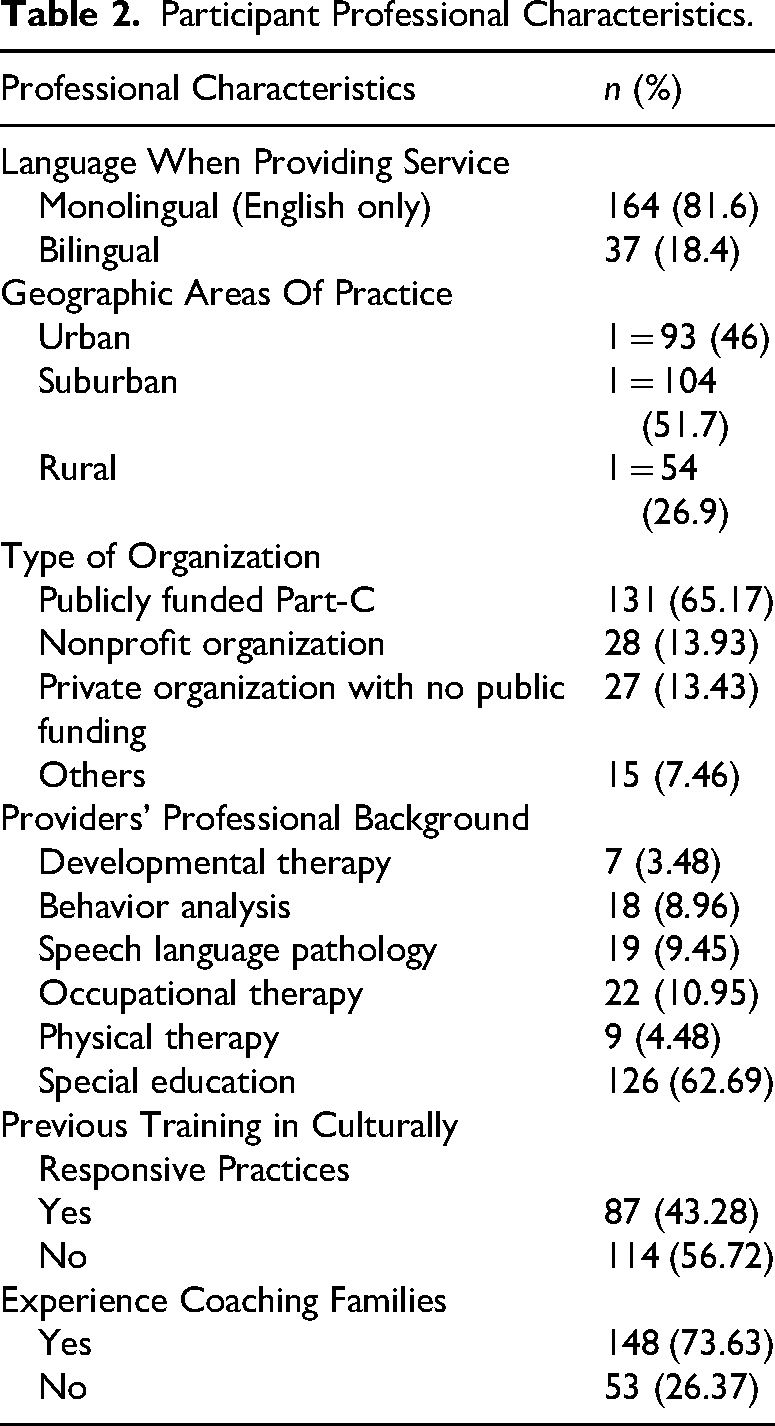
Most participants (n = 131; 65.2%) reported working in a state-funded, Part-C EI agency, 13.9% (n = 28) worked at a nonprofit organization, and a similar number of participants (n = 27; 13.4%) worked at a private organization that receives no public funding. In terms of their professional backgrounds, most participants reported having a special education or early intervention background (n = 126; 62.7%), followed by occupational therapy (n = 22; 11.0%), speech language pathology (n = 19, 9.5%), and behavior analysis (n = 18; 9.0%). There was also a broad range of years of experience in EI, with 66 participants (32.8%) with 0–5 years of experience, 52 participants (25.9%) with 6–10 years, 43 participants (21.5%) with 11–20 years, and 40 participants (19.9%) with more than 20 years of experience. See Table 2 for their professional characteristics. Additionally, we asked participants whether they have received any formal training in providing culturally responsive EI to which more than half (n = 114; 56.7%) responded “No.” We also asked whether they provided coaching to marginalized families to which most (n = 148; 73.6%) responded “Yes.” We asked participants who answered “Yes” to describe their coaching experience and strategies with marginalized families. We qualitatively coded these responses, which generated several themes, including: (a) use of interpreters or translation technology (e.g., Google Translate), (b) family empowerment, (c) cultural sensitivity and respect, (d) adaptation and flexibility to meet families’ unique needs, (e) empathy and building trusting relationships, and (f) reflective practice and continuous learning.
Participant Professional Characteristics.
Psychometric Properties of CSES-EI
Descriptive Statistics and Internal Consistency
The average score across all participants was 134.6 out of the maximum possible score of 160 possible score (SD = 13.3, range = 89–160), indicating generally high levels of self-reported cultural self-efficacy among participating EI providers. Overall, the CSES-EI exhibited excellent internal consistency with α = .92 and ω = .94, which indicated that the scale items were consistently measuring the construct of cultural self-efficacy. For each subscale, we also found acceptable internal consistency: awareness (α = .85, ω = .89), knowledge (α = .86, ω = .91), and skills (α = .86, ω = .90).
Exploratory Factor Analysis
A screeplot based on the eigenvalues is provided in Figure 1. Both screeplot and parallel analysis suggested a three-factor model (e.g., three eigenvalues were greater than 1; Kaiser, 1991). EFA was then conducted to explore the factor structure of this newly adapted scale, and the results showed that the three-factor model explained 47.9% of the cumulative variance. The factor loadings from the EFA also revealed a consistent pattern with items loading onto three distinct factors.
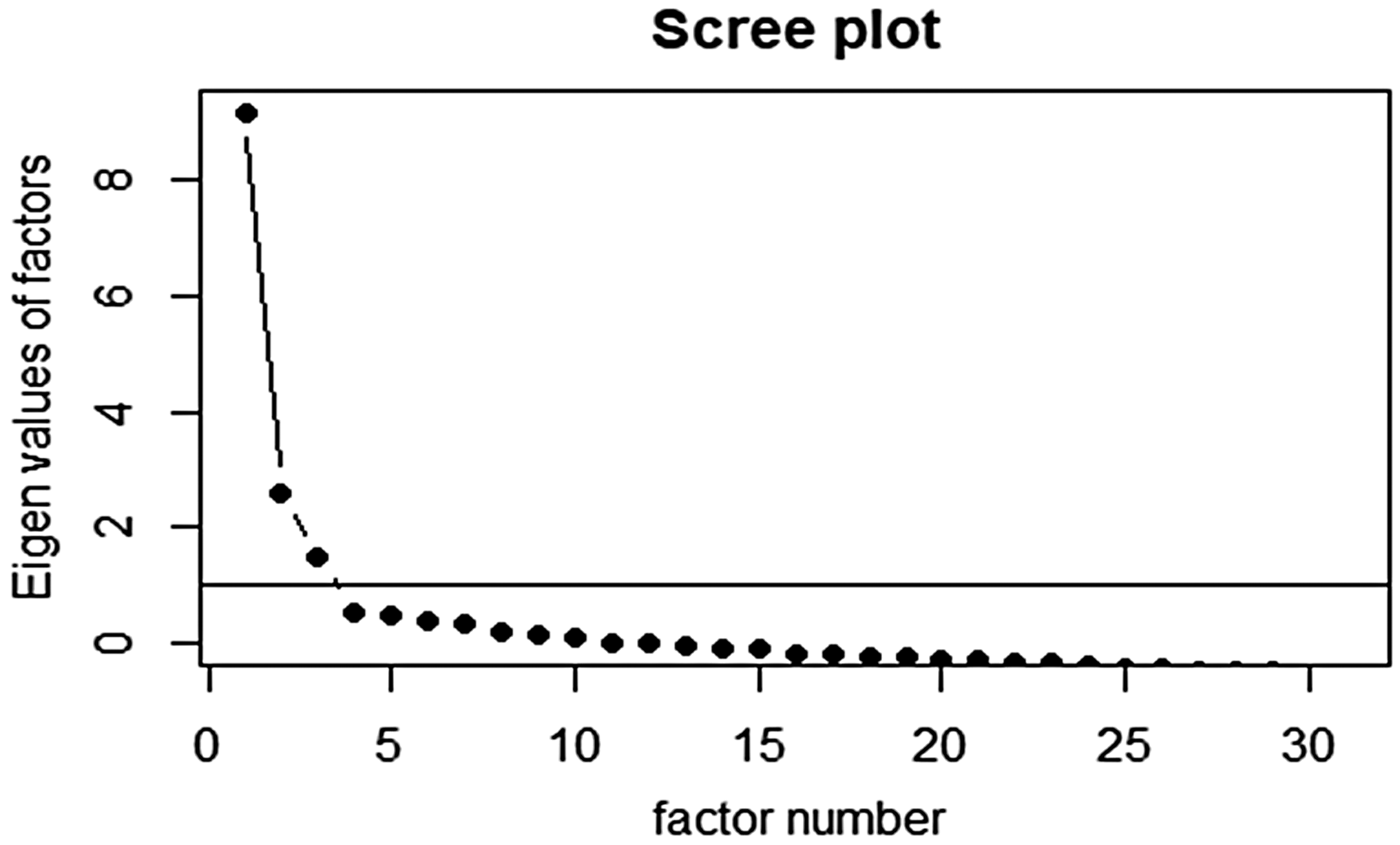
Screeplot.
Confirmatory Factor Analysis
Then, we conducted CFA to validate the three-factor model identified in EFA. Figure 2 presents the path diagram and standardized coefficients of the three-factor model. The CFA results indicated acceptable fit, with a Comparative Fit Index (CFI) of .939, a Tucker-Lewis Index (TLI) of .935, a Root Mean Square Error of Approximation (RMSEA) of .062, and a Standardized Root Mean Square Residual (SRMR) of .096. These indices indicate that this three-factor model provides an acceptable fit to the data based on Hu and Bentler (1999) criteria (e.g., RMSEA < .08, CFI > .90, TLI > .90, SRMR < .08). The standardized factor loadings matrix is provided in Table 3. The standardized factor loadings from CFA were statistically significant (p < .001), generally exceeding the threshold of .40, which further supports the validity of this model. Although the overall factor structure in this model was strong, there were three items that had factor loadings below .40, including Items 5, 20, and 23. These items belonged to one construct from each construct, with Item 5 in Awareness, Item 20 in Knowledge, and Item 23 in Skills. Given the low loadings and theoretical relevance of these items, we removed these items from the CSES-EI. Finally, latent factors were strongly correlated: awareness and knowledge (r = .76), awareness and skills (r = .51), and knowledge and skills (r = .77).

Path diagram and standardized coefficients of the three-factor model for the CSES-EI.
Standardized Factor Loadings from Confirmatory Factor Analysis (CFA).
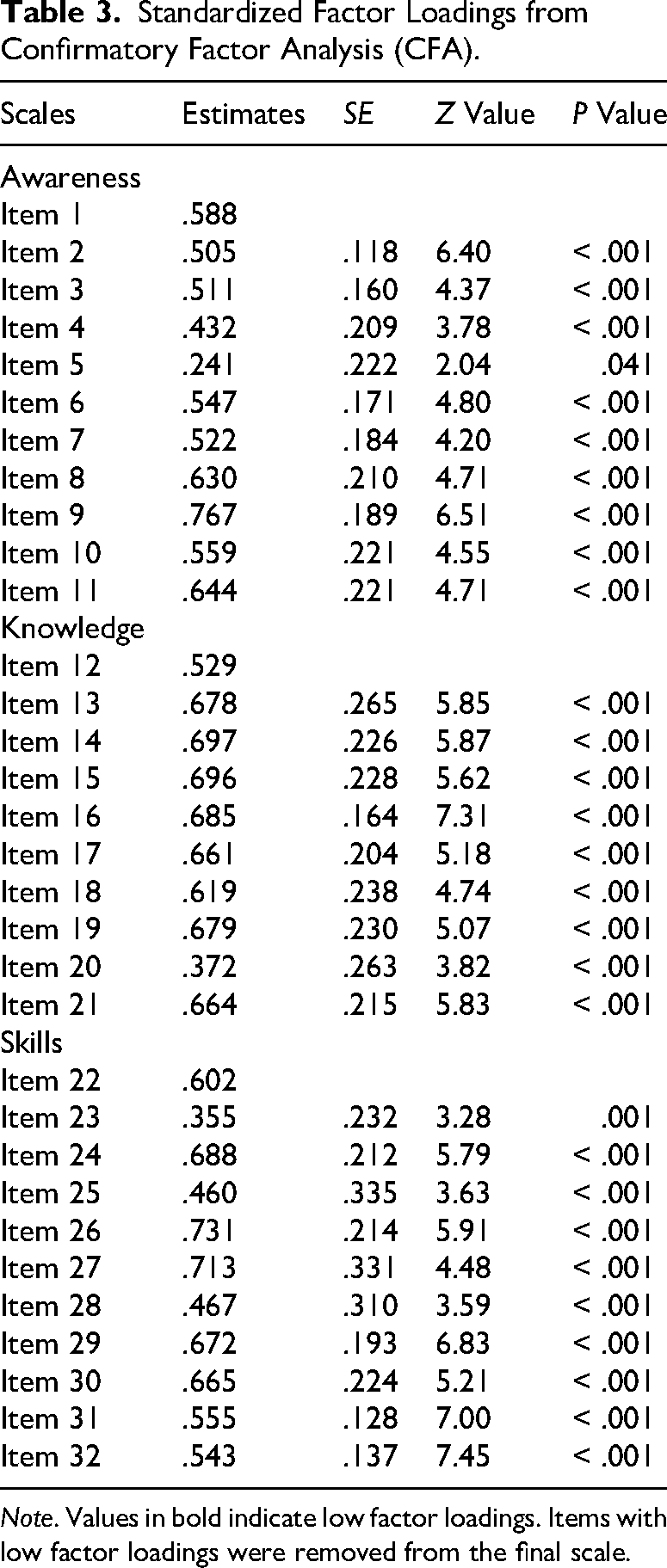
Note. Values in bold indicate low factor loadings. Items with low factor loadings were removed from the final scale.
Convergent Validity
As shown in Table 4, it was also revealed that each subscale of CSES-EI was significantly correlated with each other and the CCA (α = .90, ω = .93), which suggests a high level of convergent validity. All CSES-EI subscales correlations were statistically significant: (a) awareness and knowledge (r = .59, p < .001), (b) awareness and skills (r = .38, p < .001), (c) knowledge and skills (r = .70, p < .001). In addition, all CSES-EI constructs were significantly correlated with the composite score of the CCA: (a) awareness and CCA (r = .35, p < .001), (b) knowledge and CCA (r = .63, p < .001), and skills and CCA (r = .74, p < .001).
Correlation Between CSES-EI Subscales and CCA Sum Score.
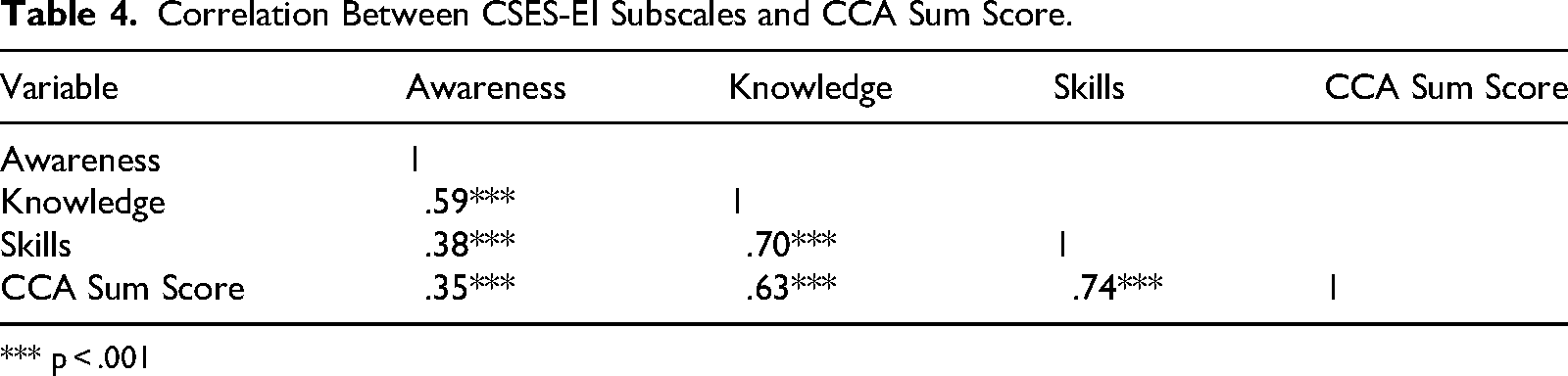
*** p < .001
Multiple Regression Analysis
A multiple regression analysis was performed to identify any significant predictors of CSES-EI scores based on participants’ demographic characteristics. This revealed that EI providers who (a) practice in urban settings (p < .05), (b) have higher levels of education (p < .01), and (c) have experience of coaching marginalized families in their sessions (p < .05) reported significantly higher CSES-EI scores. See Table 5 for more detailed information.
Multiple Regression Results.
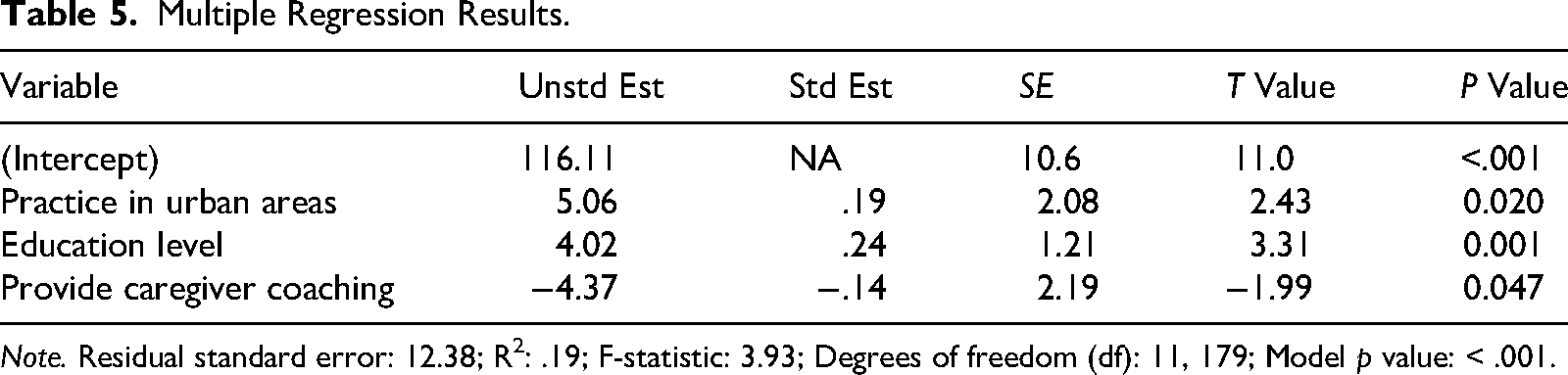
Note. Residual standard error: 12.38; R2: .19; F-statistic: 3.93; Degrees of freedom (df): 11, 179; Model p value: < .001.
Providers’ Experiences in Providing Culturally Responsive EI
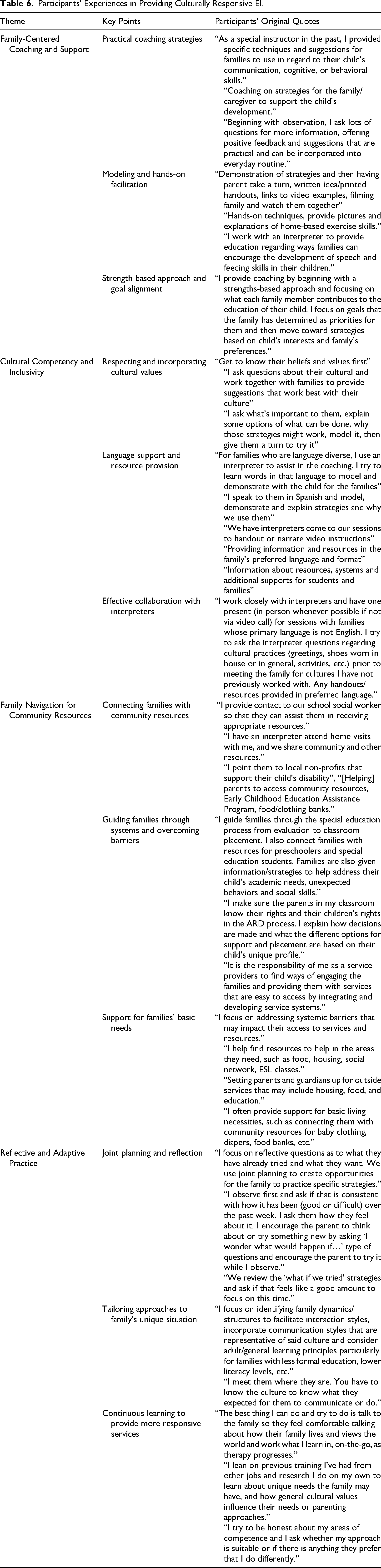
A total of 149 out of 201 participants (74.1%) shared their experiences of sustaining culturally responsive EI with marginalized families through write-in responses on the REDCap survey. A thematic analysis of these responses revealed four key themes: (a) family-centered coaching and support, (b) cultural competency and inclusivity, (c) family navigation for community resources, and (d) reflective and adaptive practice. Under the theme Family-Centered Coaching and Support, providers described how they observed families’ routines, asked questions without making assumptions, offered practical suggestions tailored to those routines, and provided hands-on demonstrations. In the theme Cultural Competency and Inclusivity, providers highlighted the need for cultural sensitivity, including efforts to engage marginalized families respectfully, deliver resources in the family's preferred languages, incorporate cultural parenting practices, and foster an inclusive, welcoming service environment. In the third theme, Family Navigation for Community Resources, providers reported assisting families in accessing community resources, navigating special education services, supporting basic needs, and connecting them with local nonprofit organizations to help further support them. Finally, in the final theme, Reflective and Adaptive Practice, participants highlighted the significance of reflective and adaptive practices in providing effective EI with marginalized families. This included engaging in joint planning and reflection to provide coaching, adapting and tailoring interventions to make these services more responsive to each family's unique needs, and continuing to learn about the family's cultural background to provide more responsive services. See Table 6 for more detailed quotes and categories.
Participants’ Experiences in Providing Culturally Responsive EI.
Discussion
This study aimed to adapt and validate the CSES-EI, a novel tool to assess EI providers’ cultural self-efficacy in working with marginalized families using both quantitative and qualitative methods. The results from 201 participants revealed high internal consistency of the scale (α = .91, ω = .94), which suggested that the scale reliably measured cultural self-efficacy among EI providers. The EFA revealed a clear three-factor model that explained a substantial portion of the variance. It was further supported by the acceptable fit indices in the CFA, which indicates a good fit between this model and the data. The convergent validity revealed the significant correlations among the CSES-EI constructs as well as with the CCA composite score, supporting the validity of CSES-EI. We also identified some demographic variables that significantly and strongly predicted the CSES-EI scores, which include (a) the setting of their practice, (b) higher education levels, and (c) their experience of coaching marginalized families. Lastly, the qualitative write-in responses revealed several themes related to the cultural self-efficacy of EI providers highlighting the importance of culturally responsive, adaptable, and supportive EI for all families.
Similar to how cultural self-efficacy is viewed in other disciplines such as nursing, social work, or psychology, this study reveals that EI providers’ cultural self-efficacy could be measured through their awareness, knowledge, and skills (Chu et al., 2022). Specifically, the validation of CSES-EI supports previous research by demonstrating the importance of not only knowledge and skills related to cultural self-efficacy but also the awareness and willingness to engage in culturally relevant practices (Lee et al., 2024b). The average sum score of CSES-EI across all participants was 134.6 out of 160 possible total score (89.7%), which reflects a high degree of self-reported cultural self-efficacy. However, this also raises important questions about whether such self-perceived confidence translates into culturally responsive practices as perceived by the families themselves. For example, Poulou et al. (2019) conducted a study to explore the relationship between general education teachers’ self-efficacy beliefs and their actual instructions and management in their classrooms. Although teachers in this study reported high levels of self-efficacy, there was a notable discrepancy between their self-efficacy beliefs and the observed use of behavior management strategies. Therefore, EI providers’ cultural self-efficacy may not accurately reflect their own practices or how the recipients of their services (e.g., marginalized families in EI) perceive their cultural responsiveness. This underscores the need for future research to examine the alignment, or lack thereof, between providers’ self-reported cultural self-efficacy and both observed practices and families’ lived experiences of cultural responsiveness in EI services. Beyond confidence and competence, culturally responsive frameworks also highlight agency as essential to equity-driven product (Gay, 2018; Ladson-Billings, 1995; Yosso, 2005). As such, future research should extend to capture how EI providers exercise agency as advocates and partners in promoting culturally sustaining practices.
In the family-centered model promoted in EI, being knowledgeable about and sensitive to differences in each family's beliefs and cultural backgrounds is crucial (Dunst, 2022; Dunst et al., 2013; Wray & Mortenson, 2011). EI practitioners should develop and integrate into their practices strategies that contribute to creating a positive climate and building authentic partnerships with families. Several CSES-EI items reflect this partnership orientation by asking providers to reflect on and consider how they seek and respect family input, individualize intervention approaches and goals with family priorities, and adapt strategies based on caregivers’ expertise on their child. The ability to effectively carry out culturally sensitive care through building trust, having honest, intercultural communication, and respecting and adapting to each family's cultural identities and experiences (Herrero-Hahn et al., 2019) is another component of cultural efficacy. As CSES-EI measures the key components of self-efficacy needed in providing culturally responsive EI, it can be utilized to provide opportunities to self-reflect and promote culturally relevant practices, ensuring the reduction of barriers that marginalized families may face as they engage in collaboration with the providers.
In addition to examining the psychometric properties of CSES-EI, we also collected qualitative data from EI providers on how they collaborate with families to co-construct and sustain culturally responsive practices with marginalized communities. The thematic analysis of these qualitative responses revealed rich insights into the strategies and approaches that EI providers employ to ensure their services are attuned to the families’ needs. Providers described various methods of engaging families, emphasized the importance of respect, empathy, and flexibility, and highlighted the significance of addressing multidimensional barriers that many marginalized families experience in the EI service pathway. For example, many providers reported adapting commonly used coaching principles and frameworks that focus on observations and providing tailored feedback (e.g., Rush & Shelden, 2020), and highlighted a need for flexibility in coaching. These findings underscore the importance of flexible, culturally responsive coaching approaches that honor family context and lived experience, especially when working with marginalized families navigating complex barriers within the EI system.
While these provider-level insights illustrate promising efforts to implement culturally responsive care, they also raise important questions about how such practices are supported or constrained by the broader systems in which EI services are delivered. Systematic reviews and meta-analyses have suggested that cultural adaptation of EBPs can be an effective and socially valid way to bridge the research-to-practice gaps for underserved populations (Cabassa & Baumann, 2013; Hall et al., 2016). More specific to special education, a recent meta-analysis has suggested that culturally adapted and tailored interventions are effective for young autistic children (Lee et al., 2025). Although these reviews suggest that culturally responsive interventions can have effective clinical utility among marginalized families, we must put an equal emphasis on the implementation within the systems of care in which most of these families rely on for service access. As implementation science reminds us, an intervention is only as effective as its delivery. Therefore, it is critical to examine how these culturally responsive interventions are implemented in EI. Examining the cultural self-efficacy of EI providers is one of the crucial first steps towards larger systemic changes, which can begin with identifying gaps in cultural responsiveness at both individual and organizational levels.
Implications for Practice, Research, Policy
Our findings on the three constructs of cultural efficacy suggest that in order to support the cultural responsiveness of EI, future training for providers may involve the evaluation of their awareness, knowledge, and skills through psychometrically sound measures and using this information to tailor contextual and relevant PD opportunities. For example, the scale can be used as a pre- and post-survey to examine the effects of an online module or PD training for pre- or in-service providers. Also, our findings on demographic predictors reveal the importance of more policies that support the resources for PD of EI providers on cultural efficacy, especially for providers who practice in rural or suburban areas, those with lower education levels, and providers with lower levels of experience coaching marginalized families. Moreover, our findings from the thematic analysis of providers’ description of collaboration with marginalized families highlight examples of culturally responsive practices such as collaboration with interpreters, empowering families, respecting one's culture, adapting to families’ needs, building trust, and continuous learning and reflection. Future research could use these components of culturally responsive collaboration practices as well as the three constructs in CSES-EI to examine the organizational climate for PD on cultural responsiveness as well as the impact of training programs for new providers entering the field and continuing education programs for more experienced providers. Furthermore, it is important to note that the ways EBPs are often presented may create tension with culturally responsive assessment and pedagogy, which emphasizes flexibility, contextual fit, and honoring families’ cultural and linguistic strengths (Lee et al., 2023; Pickard et al., 2023). This tension underscores the importance of positioning providers not merely as implementers of prescribed practices, but as reflective and collaborative decision-makers who can individualize EBPs to align with family values, community contexts, and systemic realities. In doing so, providers exercise professional and cultural agency to ensure that the implementation of EBPs with marginalized families is both effective and equitable.
Specifically, as previous studies show that parents from dominant sociocultural groups report higher satisfaction and greater perceived effectiveness of interventions compared to parents from marginalized groups (Bailey et al., 2004; Batz & Yadav, 2024; Hebbeler et al., 2007), CESE-EI scores can inform PD activities to allow providers to engage in asset-based behaviors that work towards learning, understanding, and respecting cultural norms and values of marginalized families, promoting positive family satisfaction and outcomes (Romijn et al., 2021). Throughout this process, it is crucial to consider not only provider-level beliefs and practices, but also how these factors may shape or challenge structural and systemic factors that may exist in EI, including racism, ableism, and dominant language ideologies or forces that prevent such marginalizations (Artiles, 2023; Paris & Alim, 2017). For example, providers’ knowledge, previous experiences, or beliefs may either intentionally or inadvertently influence how they perceive families’ caregiving practices and engagement (Romijn et al., 2021), which may impact the way they collaborate with and invite families to support and understand their child's development (Dunst, 2021). To this end, CSES-EI can be used to uncover and transform such deficit-based practices into strength-based practices that affirm families’ knowledge, value, and identities. It can also be used for self-evaluation and to elicit self-awareness for providers, and for the EI programs to evaluate providers’ perspectives and practices and identify areas of need for further professional development and training related to culturally responsive practices.
Notably, the qualitative responses in Table 6 indicate that providers do what they can to demonstrate their cultural self-efficacy and to promote cultural responsiveness in their own practices, such as collaborating with interpreters or tailoring intervention approaches. However, as Lee et al. (2024b) previously suggested, efforts at the individual provider level may not be sufficient in improving service access as a whole. Rather, it requires careful examination of multilevel determinants (e.g., organization and system levels) to bring systemic changes. Therefore, there are also important implications at the policy level. Given the significant predictors identified in this study (i.e., practice setting, education level, coaching experience), it is necessary to examine how current policies facilitate or hinder continuous access to PD among EI providers, especially among families who rely on public services like Part C EI. This could include providing PD with culturally responsive practices through online courses or webinars that could accommodate providers’ busy schedules, and CSES-EI can be used to assess the proximal effects of these PDs. Furthermore, it is necessary to examine how professionals in different disciplines cultivate a culturally responsive workforce. As many marginalized families receive services from these providers, the consideration of how they are trained and coached to effectively work with these families within their own professional society is crucial.
In a recent report to the Congress, the U.S. Government Accountability Office (GAO;, 2023) analyzed data on IDEA Part C EI programs, which included more than 770,000 children receiving services in EI. In their report, the GAO concluded that access to services still varies by child and family characteristics, such as race and income. This is despite the U.S. Congress expressing “an urgent and substantial need” to meet the needs of “all children, particularly minority, low-income, inner city, and rural children” (p. 26) in the latest amendment to the IDEA in 2004. The GAO further made recommendations to the Congress to authorize the U.S. Department of Education to collect demographic information on children and to use these data to better identify and rectify gaps in access to services. It is clear that disparities and inequities in accessing EI services still exist, even in light of Congressional efforts to address them. These findings show the critical need for more discussion around cultural self-efficacy for EI providers. On this note, CSES-EI can be used to assess the cultural self-efficacy of EI providers in working with these most marginalized and vulnerable populations in our society. By capturing how confident and competent providers feel in implementing services with children and families from different racial, ethnic, cultural, linguistic, and socioeconomic backgrounds, this scale can recommend policies and practices that could address potential barriers and facilitators to culturally sustaining and inclusive service delivery in EI.
Amidst the current sociopolitical uncertainties inequitably and unjustly threatening marginalized families utilizing public systems like Part C EI or Medicaid, there is an urgent need to focus not only on how culturally responsive practices are promoted at the provider level, but also on system-level advocacy to address structural inequities that shape access and quality. The CSES-EI can contribute to this process by helping programs assess provider readiness and identify areas for growth in cultural self-efficacy. When used across settings, the tool can also reveal patterns that inform targeted professional development efforts and highlight disparities that may warrant further organizational or policy attention.
Limitations
There are several noteworthy limitations. Despite our efforts to recruit a diverse sample, our sample was predominantly White, mirroring the current demographics in the field. Future research could explore the examination of cultural efficacy specifically among EI providers from marginalized backgrounds to examine the differences or similarities in how they practice cultural efficacy. Moreover, while the cultural self-efficacy of our sample was rated high, it is important to acknowledge that the sample may not represent the larger population of EI providers. Future research should consider the use of the measures to allow for a more holistic understanding of EI providers across various geographic regions, training backgrounds, and cultural contexts. Lastly, we used the Delphi method to obtain 11 experts’ evaluations of the survey; however, there may be a chance that their evaluations may have biases based on their personal beliefs, content and contextual expertise, and experiences. The main purpose of this process was to co-adapt an original, relevant scale to fit better within our field. As such, we acknowledge that we did not formally ask panelists to articulate or document specific epistemological frameworks or professional lenses, nor did we systematically document the influence of positionality or bilingualism on their judgments. Instead, our process relied on their professional expertise and lived experiences to identify items that were not adequately clear, or that were potentially biased, or not appropriate, for the purpose of this instrument. Relatedly, we were not able to recruit individuals with disabilities or family members as panel experts. Future research could finetune the scale by hearing from the families’ perspectives. This is an important limitation, as the absence of family voices may have constrained the scale's ability to fully capture dimensions of cultural self-efficacy related to authentic family–provider partnerships and shared decision-making. Incorporating families as co-designers or reviewers in future Delphi rounds or validation studies would strengthen both the cultural validity and ecological relevance of the CSES-EI.
Conclusion
In this study, we adapted and validated the CSES-EI to provide a tool for assessing cultural self-efficacy among EI providers who work with marginalized families. Overall, the findings indicate that the CSES-EI demonstrates adequate reliability and validity, supporting its use as a measure of cultural self-efficacy. The qualitative insights from participants also underscore the diverse strategies and their positive experiences of providing more culturally responsive EI with marginalized families. As the field of EI continues to evolve and the demographics in the United States continue to diversify, cultural responsiveness in a public system of care is not just a supplementary consideration; rather, it is a quality assurance issue that will fundamentally impact the overall quality and equity of the EI service system.
Supplemental Material
sj-docx-1-ecx-10.1177_00144029261433795 - Supplemental material for Adaptation and Multi-Methods Validation of the Cultural Self-Efficacy Scale in Early Intervention (CSES-EI)
Supplemental material, sj-docx-1-ecx-10.1177_00144029261433795 for Adaptation and Multi-Methods Validation of the Cultural Self-Efficacy Scale in Early Intervention (CSES-EI) by James D. Lee, Veronica Y. Kang, Sean Joo, Adriana Kaori Terol, Sehee Jung, Yuanchen Kuo and Hedda Meadan in Exceptional Children
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences, (Grant Number KL2TR002317).
Supplemental Material
Supplemental material for this article is available online.