
Abstract
The demand for services and resources to support individuals with autism has increased in correspondence with the rising prevalence of autism around the globe. However, there is limited availability of resources and services to support autistic children and their families in low-to-middle-income countries. Caregiver training is an evidence-based practice that leads to positive outcomes for both caregivers and their autistic children, and is an appropriate way to deliver support for caregivers of autistic children in low-resourced settings. In this study, we used a convergent mixed-methods design to evaluate the effects and social validity of a culturally adapted caregiver training program with 17 caregivers of autistic children in Paraguay. Caregivers increased their knowledge about autism, their understanding of their children's strengths and needs, and their advocacy knowledge and skills, from pre-program to post-program. Additionally, caregivers deemed the program feasible, acceptable, and needed in the Paraguayan context. Implications for policy and practice, and directions for future research are discussed.
Autism is experienced by about 78 million individuals worldwide (Lord et al., 2021). Although formal documentation of the prevalence of autism in some countries is not available, or is limited or difficult to aggregate due to methodological differences (Lord et al., 2021), researchers have reported a median global prevalence of 1% (Zeidan et al., 2022). The demand for services and resources to support individuals with autism has increased in correspondence with the rising prevalence of autism in the last few decades. However, access to resources to support children with autism and their families is inequitable (Lee & Meadan, 2021; Magaña, Dababnah, et al., 2021). Children with autism and their families who live in rural areas, in low-resourced settings, and who are from historically minoritized and marginalized groups, are at greater risk for having unmet needs due to restricted accessibility to services (Lee & Meadan, 2021; Mazurek et al., 2017). One way to support caregivers of children with autism to overcome some of the challenges they face is through caregiver training (Bearss et al., 2015).
Caregiver training is an evidence-based practice through which caregivers may increase their knowledge, self-efficacy, and empowerment to support their children (Hume et al., 2021). Training caregivers and building their capacity may be a cost-effective and appropriate way to deliver support for caregivers of autistic children in low-resourced settings (Bearss et al., 2015; Lee & Meadan, 2021; World Health Organization, 2018). In such settings, where access to specialized services is limited, empowering caregivers through training is a strategic way to provide ongoing support for the diverse needs of autistic children and their families (Dawson-Squibb et al., 2020). Although caregiver training positively impacts caregivers, most caregiver training research has been conducted in high-income countries (DuBay et al., 2018; Magaña, Dababnah, et al., 2021). Importantly, researchers have highlighted a need to consider contextual local and cultural aspects when providing training to caregivers of children with autism around the globe (Dawson-Squibb et al., 2020). Specifically, cultural perceptions of disability and high stigma reported by caregivers of autistic children in Latin America may impact caregivers’ perceived needs, experiences supporting their child with autism, and response to training (Paula et al., 2020). Considering that it cannot be assumed that interventions developed and evaluated in high-income countries, predominantly with White participants, are appropriate for families in low-to-middle-income countries (LMICs; Bernal & Domenech Rodriguez, 2009; Buzhardt et al., 2016), research focused on culturally responsive caregiver training in such settings is needed (DuBay, 2022).
Available data indicate that caregivers of autistic children in Latin America would benefit from resources and support to meet the needs of their children and families (Paula et al., 2020). Specifically, families in Paraguay have reported several barriers to accessing services and support for their autistic children, such as financial burdens associated with services, scarcity of well-trained professionals and teachers, and stigma (Terol et al., 2023). To address these barriers, Terol, Meadan, et al. (2024) conducted a study to further explore the perspectives of community members on the needs of caregivers of children with autism in Paraguay and their suggestions to culturally adapt Parents Taking Action (PTA; Magaña et al., 2017), a caregiver training intervention developed for caregivers of Latin American descendents living in the United States.
PTA is a manualized intervention that was developed in collaboration with community members and incorporating cultural values such as familismo and personalismo. The program includes information on developmental milestones, autism, advocacy, service system navigation, self-care for caregivers, and evidence-based strategies to support the development of social communication, play, and social skills, as well as strategies to manage behavior. Following the positive outcomes of piloting PTA (Magaña et al., 2017), the program has been implemented across two sites with Latino families living in the United States, using a randomized control trial design with 96 participants (Lopez et al., 2019). Additionally, after identifying relevant community members from the target communities and collaboratively culturally adapting the intervention according to their needs, PTA has also been implemented with caregivers in Colombia (Magaña et al., 2019; Magaña, Tejero Hughes, et al., 2021), and has been extended to caregivers of children with autism from other cultural groups in the United States (i.e., Black caregivers; Dababnah et al., 2023, and Chinese caregivers; Xu, 2021; Xu et al., 2023).
PTA was identified as a training program that may be suitable to meet the needs of caregivers in Paraguay because of its acceptability, feasibility, and positive outcomes among caregivers of autistic children of Latin American descendents who live in the United States and in Colombia (Lopez et al., 2019; Magaña et al., 2017, 2019; Magaña, Tejero Hughes, et al., 2021). Recognizing the contextual and cultural differences among Latino groups (Borrell & Echeverria, 2022), Terol, Meadan, et al. (2024) conducted a study to culturally adapt PTA for its implementation in Paraguay. In Terol, Meadan and colleagues’ study, community members (N = 28) provided suggestions on adapting PTA to increase the intervention's contextual fit and thereby meet the needs of caregivers of autistic children in Paraguay.
Collaborating with community members is a key step in the cultural adaptation process (Kuhn et al., 2020; Lee et al., 2023). A detailed description of the previous steps we took for the cultural adaptation process is available in Terol, Meadan, et al. (2024). Piloting an intervention and asking for additional feedback is also part of the iterative process of cultural adaptation (Kuhn et al., 2020; Lee et al., 2023) and may aid in determining whether additional changes are needed and whether the adapted intervention yields the intended outcomes of the intervention. Thus, the purposes of this study were to assess whether the culturally adapted PTA leads to positive outcomes for caregivers of young autistic children in Paraguay and is socially valid. The following research questions guided the study: (1) Does the culturally adapted PTA increase the (a) knowledge of autism, (b) self-efficacy of parenting, and (c) understanding of their children's needs and strengths of caregivers of young children with autism (i.e., 2–8 years old) in Paraguay? and (2) Is the culturally adapted PTA socially valid?
Methods
The study was approved by the University's Institutional Review Board. We used a convergent mixed-methods design (Leko et al., 2023) and were guided by a pragmatism/pluralist paradigm (DeCuir-Guby & Schutz, 2016). We collected both quantitative and qualitative data for the purposes of triangulation and complementarity (Greene, 2007). We collected quantitative data through pre- and postintervention questionnaires, and attendance and attrition data and qualitative data through a set of open-ended questions in a social validity questionnaire and individual semi-structured interviews with caregivers.
Researchers’ Identity
The research team was culturally, ethnically, and linguistically diverse. The team included two cisgender Paraguayan women graduate students, with experience working with young children with autism and their families in Paraguay, and two full professors, cisgender woman with vast experience conducting research with culturally diverse families. Additionally, two caregiver leaders collaborated in the delivery of the intervention. The team members’ shared cultural and linguistic background with participants informed key aspects of the study, including recruitment strategies, incorporation of feedback to inform the adaptation and implementation of the program, and the interpretation of findings. Ongoing collaboration with caregiver leaders also helped ensure that the intervention and study design remained grounded in community priorities and values. Our collaborative and reflective approach also helped reduce potential bias by promoting culturally situated interpretations and enhancing the validity of the findings.
Recruitment and Inclusion Criteria
For recruitment, we collaborated with a community-based organization of caregivers of individuals on the autism spectrum (i.e., TEA Paraguay) and shared digital flyers in Spanish through social media and researchers’ professional networks. To be eligible, participants needed to: (a) be a caregiver 1 of a 2–8-year-old child, either with an autism diagnosis based on a caregiver report, or referred for an autism evaluation and a score of 15 or higher on the social communication questionnaire (SCQ; Berument et al., 1999); (b) be 18 years old or older; and (c) live in Paraguay. Caregivers who reported that their children had an autism diagnoses but whose child's SCQ scores were below 15 were considered eligible to participate given that caregiver-reported autism diagnoses are generally accurate (Daniels et al., 2012). We focused on caregivers of children aged 2–8 to align with the developmental focus of the intervention, which targets early childhood and the transition into formal schooling.
A total of 138 people completed a screening questionnaire. We contacted caregivers who completed the screening questionnaire in the order in which we received their responses. Due to practical considerations, such as limiting the number of participants in each group to facilitate participation, we stopped recruitment once 26 caregivers enrolled in the study (i.e., provided informed consent and completed all preintervention measures). Similar sample sizes were used in previous pilot studies focusing on culturally tailored caregiver training (Pearson & Meadan, 2021; Rios et al., 2021), including the pilot study of the PTA (Magaña et al., 2017).
Participants
Of the 26 caregivers who enrolled in the study, 22 attended at least one PTA session. Of the 22 caregivers who started the program, all were female including 21 mothers and one aunt, three were caregivers of children who were being evaluated for autism, and 19 reported that their children had autism diagnoses. The majority identified as Hispanic or Latino (n = 18) and were married or living with a partner (n = 13). Half of the participants had college degrees (n = 11). The most reported caregiver age range was 31 to 35 years (n = 9). The participants’ children's mean age at the beginning of the study was 5.59 years old, and their mean age at the time they received autism diagnoses was 3.73 years old. Eighteen children were boys, and all were receiving at least one service with most receiving speech and language pathology and psychology services. See Table 1 for additional demographic information. Participants were considered to have attended the session if they logged in and stayed for at least 50% of the session (i.e., 60 min) for each session. Participants who attended 70% of the sessions (i.e., seven sessions) or more were considered to have completed the intervention. Overall, 17 participants completed the program. See additional information in the Results section.
Participants’ Demographic Information.
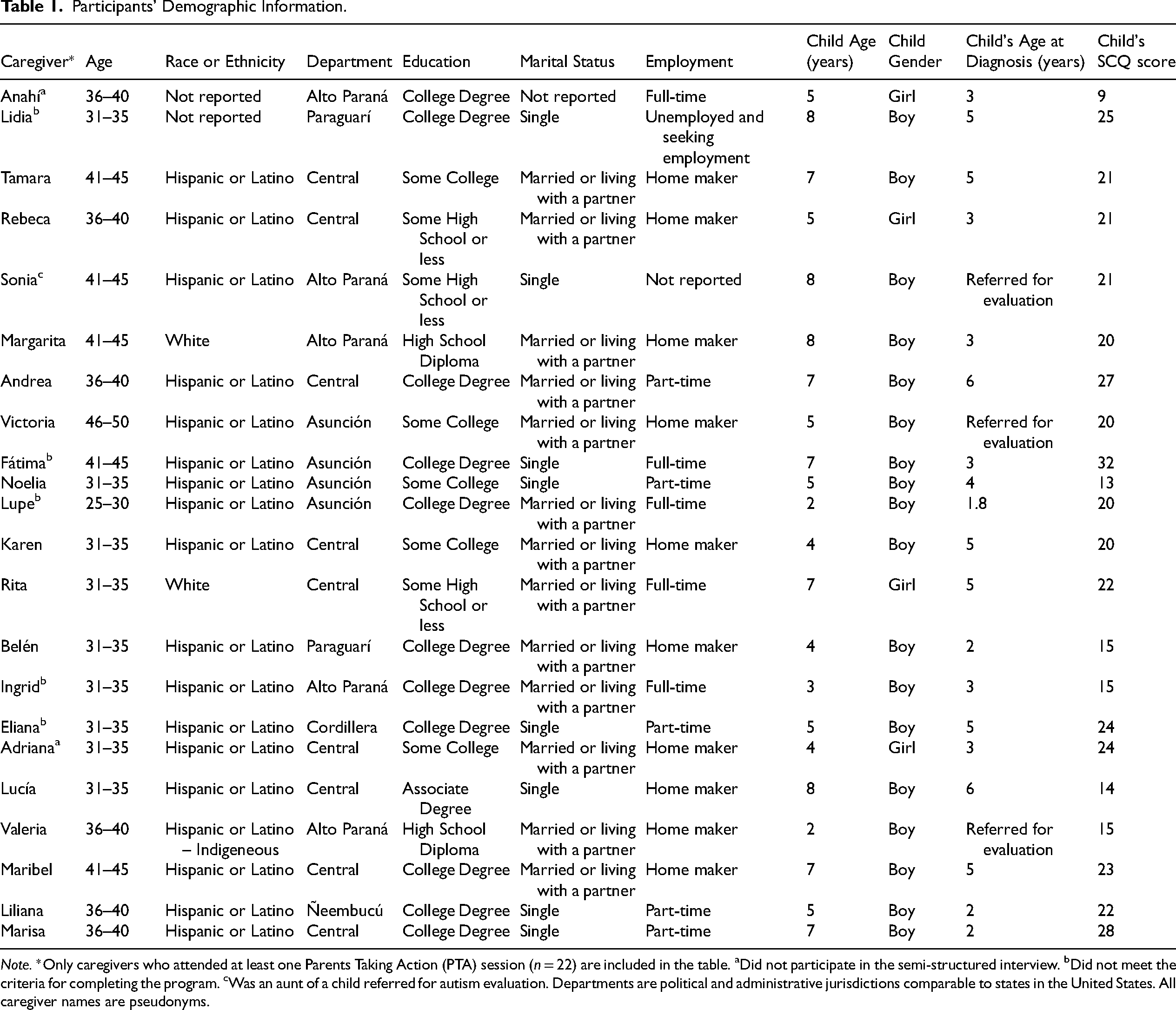
Note. *Only caregivers who attended at least one Parents Taking Action (PTA) session (n = 22) are included in the table. aDid not participate in the semi-structured interview. bDid not meet the criteria for completing the program. cWas an aunt of a child referred for autism evaluation. Departments are political and administrative jurisdictions comparable to states in the United States. All caregiver names are pseudonyms.
Intervention Description
The culturally adapted PTA included 10 sessions focusing on child development, autism characteristics, myths about autism, evidence-based strategies to support children with autism, advocacy, and managing caregiver stress. Each session lasted 2 hours. The first session started with an introduction of the instructors and participants. All other sessions started with a reflection and discussion related to an activity for the week, to be completed outside the sessions assigned in the previous session for all other sessions. Each session included the presentation of new content through case studies, mini-lectures, videos, and an individual or small group application activity in which participants were prompted to think about how the new content applied to their children. The sessions ended with another discussion and reflection on the content presented in the session, and an overview of the activity for the week designed to practice or discuss the content outside the sessions.
Procedures
Caregiver leaders training
Prior to the beginning of the study, we collaborated with TEA Paraguay, to identify two caregivers who were (a) active members of the organization, (b) caregivers of children with autism, and (c) had prior experience supporting other caregivers. These two caregivers received training and became co-instructors along with the first author to deliver the culturally adapted PTA. One caregiver was a woman, and the mother of a 10-year-old girl with autism. She had a college degree and was also a speech and language pathologist. The other caregiver was a man, and the father of an 11-year-old boy with autism. He had some college education. These caregivers will be referred to as “caregiver leaders” hereafter. Caregiver leaders received access to the culturally adapted PTA manual and all materials provided to participants, and participated in a 4-hour-long online training in Spanish via Zoom. During this training, caregiver leaders received an overview of each session and role-played delivering portions of the sessions. Additionally, during the intervention caregiver leaders met with the first author 10–15 minutes before the sessions to jointly prepare for the session of the day.
Preintervention
Participants completed the prestudy measures during a Zoom or WhatsApp meeting, or received a link to an online questionnaire to complete them on their own. Two groups were offered on Saturdays at a different time of the day, and participants were asked to select their group based on their availability. These will be referred to as morning sessions, and afternoon sessions, respectively, hereafter. Caregivers attended the same session (morning or afternoon) throughout the intervention. This was done to allow participants opportunity to build relationships within each group throughout the intervention sessions.
Intervention delivery
The culturally adapted PTA included 10 weekly 2-hour-long sessions. PTA sessions were conducted online, synchronously via Zoom, in Spanish, in a group format, with 13 enrolled caregivers in each group. Participants in both groups received the same intervention. To deliver the sessions, one caregiver leader codelivered the same five sessions for the morning and afternoon groups with the first author, whereas the other caregiver leader co-delivered the other five sessions for the morning and afternoon session groups with the first author. Each session was videorecorded for fidelity checks. Caregiver leaders led all discussion, reflection, and application activities. The first author led mini-lectures, case studies, and activities related to the presentation of new content.
Postintervention
Participants were allocated time to complete the postintervention questionnaire at the end of the last group session. If a participant did not attend the last session, they were sent the link to the online questionnaire. Participants were also invited to participate in a 30-minute individual semi-structured interview to assess the social validity of the intervention. Nineteen participants completed the semi-structured interview, which was conducted in Spanish through Zoom or WhatsApp by a research assistant who did not participate in the intervention delivery.
Measures
Demographic questionnaire
The demographic questionnaire included 19 questions inquiring about the demographic characteristics of caregivers (i.e., relationship with the child, age, education level, and employment status) and their children (i.e., date of birth, gender, date of formal autism diagnosis or an autism evaluation referral, and services they were receiving). Individual-level demographic data are included in Table 1 to allow for contextualization of participants’ reported experiences and opinions considering their demographic characteristics.
Autism spectrum knowledge scale—general population version (McClein et al., 2019)
This is a 31-item scale with false/true statements designed to measure knowledge of autism. Examples of items in the scale include “Autism is caused by a lack of motherly warmth” and “If a teacher believes a student has autism, they can make a diagnosis.” Benallie et al. (2020) reported Cronbach's alpha of α = 0.82 raw, α = 0.82 standardized, and Guttman's λ6 (0.86), indicating good internal consistency. The research team translated this measure into Spanish for this study using a forward–backward translation method (Brislin, 1970). Cronbach's alpha for this sample was .78 at pretest and .67 at posttest.
Autism-specific parenting self-efficacy scale (Kurzok et al., 2021)
This is a 17-item scale scored on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicate greater caregiver self-efficacy in their ability to meet their child's needs and manage challenges as caregivers of children with autism. Examples of items in the scale include “I feel confident that I can seek additional resources beyond what is provided to me” and “I feel confident that I can handle difficult moments with my child.” Kurzok et al. (2021) reported that the measure's Cronbach's alpha was α = 0.91, indicating good internal consistency. The research team translated this measure into Spanish for this study using a forward-backward translation method (Brislin, 1970). Cronbach's alpha for this sample was .92 at pretest and .83 at posttest.
Family outcomes survey (Bailey et al., 2008)
This is a 24-item scale rated on a 5-point Likert Scale (1 = not at all to 5 = completely) that measures various aspects of family outcomes including satisfaction, involvement, empowerment, and quality of life. Higher scores indicate better outcomes for each subscale. Examples of items in the scale include “We are able to tell when our child is making progress” and “We are able to help our child take care of his/her needs.” Olmsted et al. (2010) translated the measure into Spanish and reported Cronbach's alphas between .80 and .63 for the different subscales. Cronbach's alpha for the overall scale in this sample was .89 at pretest and .91 at posttest.
Social validity questionnaire
The social validity questionnaire was developed by the research team and comprises a total of 21 questions developed based on Wolf's (1978) social validity framework. The questionnaire includes 14 items that are scored with 5-point Likert-type questions (1 = strongly disagree to 5 = strongly agree) and seven open ended questions regarding caregivers’ satisfaction with the training, and its relevance to their daily lives. Examples of the questions include “What aspects of the intervention were the most relevant to you? Why?” and “What aspects of the intervention were difficult to complete? Why?”
Semi-structured interview
Upon completion of the intervention, participants were invited to participate in online individual semi-structured interviews. The interviews were conducted in Spanish via Zoom or WhatsApp by a research assistant. Questions in the interview (see the online supplemental materials) were designed to assess the social validity of the goals, procedures, and outcomes of the intervention (Wolf, 1978). Additionally, participants were asked if the intervention aligned with their cultural values. Nineteen participants completed the semi-structured interview. The interviews lasted an average of 17 minutes (range = 8–26 min).
Attendance and attrition
We collected data on the attendance of participants who logged into Zoom for each session and participants who arrived late or left before the session was completed. We used videorrecorded sessions to verify attendance data. The percentage of attendance was calculated by dividing the number of sessions the participant attended by the total number of sessions (i.e., 10). To measure attrition, we divided the number of participants who completed the program (i.e., participants who attended at least 50% of the time in at least 70% of the sessions) by the number of participants who attended at least one PTA session.
Treatment fidelity
Treatment fidelity was assessed through checklists for each group separately (Gersten et al., 2005; Toste et al., 2023). The fidelity checklist was individualized for each session following the manual guidelines. Fidelity was calculated by dividing the number of completed steps by the overall number of steps in the checklist and multiplying by 100. All sessions were conducted with 100% fidelity, except for one with the morning group (94%). A research assistant reviewed 30% of randomly selected sessions (i.e., six in total) and completed the same fidelity checklists to assess the reliability of the fidelity. The reliability of fidelity was evaluated by comparing the fidelity checklists completed by the primary and secondary observers and calculating a point-by-point agreement. The point-by-point agreement was calculated by dividing the number of agreements by the sum of agreements and disagreements, and multiplying the result by 100. Reliability was 100% for all checked sessions.
Data Analysis
For this convergent mixed-methods study, quantitative and qualitative data were analyzed separately and later integrated for interpretation through a joint display (Creswell & Plano-Clark, 2018; Love et al., 2023).
Quantitative data analysis
All quantitative data analyses were computed and evaluated using R (4.2.1.2022-06-23). Preliminary analysis was conducted, including interitem relations, missing data, and response distribution. Cronbach's alpha was calculated and we checked for the normality of responses using graphic displays and skewness and kurtosis (Harrell, 2001).
Pre-post measures
To examine pre-post changes in knowledge of autism, self-efficacy, and family outcomes in the total sample (i.e., both groups), we used paired-sample t tests. To determine the effect sizes for the paired-sample t tests, we used Cohen's d (i.e., .02 = small effect size, .05 = medium effect size, and .08 or larger = large effect size; Cohen, 1988).
Social validity questionnaire
Data from the Likert-type questions on the social validity questionnaire were analyzed using descriptive statistics.
Qualitative data analysis
Data from the interviews were transcribed verbatim in Spanish with the aid of the Zoom software. To analyze the data, the first author first listened to the recordings of the interviews and cleaned the transcripts generated by Zoom to ensure accuracy. Responses from the open-ended questions on the social validity questionnaire were added at the end of each participant's interview transcript. Second, we used Google translate to generate an English version of the transcript. Third, the first author revised each translated transcript for accurate translation. Fourth, three transcripts were randomly selected, and the first and second authors independently read the transcripts in English and independently coded the data using thematic analysis and deductive coding with codes selected a priori (Saldaña, 2021), based on Wolf's (1978) social validity theoretical framework. Through thematic analysis we assigned codes to identify patterns or recurrent ideas and experiences relevant to the research questions to subsequently group, organize, synthesize, and report these ideas and experiences (Saldaña, 2021). After coding these three transcripts, we developed a codebook to thematically analyze the 16 remaining transcripts. All codes were then reviewed, and the codebook was refined. Finally, the first author used the finalized codebook to conduct a second round of coding for all transcripts.
Data integration
The purposes of mixing methods included triangulation and complementarity. Triangulation increases the validity of the inferences. It is used to determine convergence or corroboration of results obtained through different methods (Greene, 2007). The purpose of complementarity is to create “broader, deeper, and more comprehensive social understandings by using methods that tap into different facets or dimensions of the same complex phenomenon” (Greene, 2007, p. 101). Through a merging approach, we brought together the qualitative and quantitative data (Gutterman et al., 2015) to draw conclusions about the overall effects and social validity of the culturally adapted PTA.
Results
Overall, 17 (77.27%) caregivers completed the program. These completers showed a significant improvement in autism knowledge, and modest, non-significant gains in caregiver self-efficacy and overall family outcomes. Subscales of assessing understanding of the child's needs and advocacy showed significant improvements. Participants rated the program as highly acceptable and provided suggestions for improving and expanding the program.
Quantitative Results
Attendance and attrition
Of the 26 caregivers who enrolled in the study, 22 attended at least one PTA session. Twelve started the program (i.e., attended at least one session) in the morning session group, and 10 started the program in the afternoon session group. Overall, 22.72% (n = 5) of the participants logged in to all PTA sessions, 54.54% (n = 12) logged in to at least nine PTA sessions, 63.63% (n = 14) logged in to at least eight PTA sessions, and 86.36% (n = 19) logged in to at least seven PTA sessions. Seventeen participants met the criteria for completing the intervention (77.27%). Data of participants who attended at least seven PTA sessions and stayed for at least 50% of the time in all seven sessions (i.e., completed the program) were included in the quantitative data analysis (n = 17). Out of the 17 participants who completed the program, eight were enrolled in the morning group, and nine in the afternoon group. Five participants constituted the attrition rate at 22.72%. Of the 22 participants who started the program, four participants (Ingrid, Lupe, Eliana, and Andrea) cited job responsibilities coinciding with the schedule as the reason for not attending the sessions. Other participants cited child caregiving responsibilities, extracurricular activities with their children with autism or their other children, health issues, child health issues, power outage, and internet problems as reasons for missing one or more PTA sessions.
Knowledge about autism
One participant (Sonia) was excluded from the analysis using listwise deletion due to extensive missing data (12 items unanswered at postintervention), making it difficult to interpret overall change scores reliably. There was a significant increase in caregivers’ knowledge about autism from pre- to postintervention—t(15) = -3.13, p = .005—with a large effect size (Cohen's d = - 0.99), indicating substantial improvement in understanding autism-related concepts and practices. See Table 2 for additional information.
Pre-Post Outcome Variables and Results.
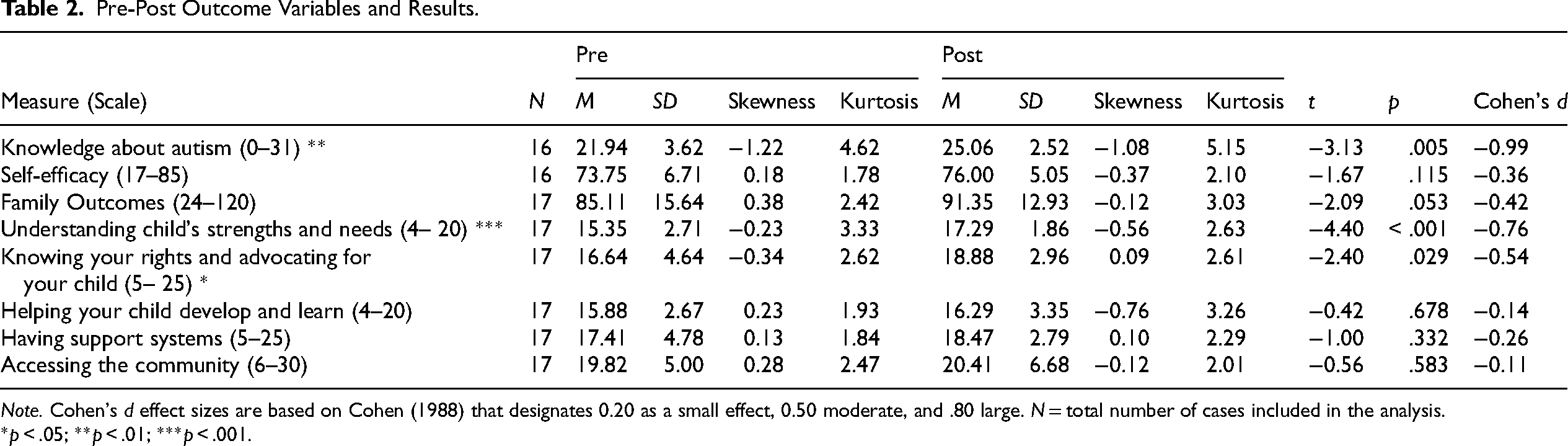
Note. Cohen's d effect sizes are based on Cohen (1988) that designates 0.20 as a small effect, 0.50 moderate, and .80 large. N = total number of cases included in the analysis.
*p < .05; **p < .01; ***p < .001.
Self-efficacy
Sonia's responses were excluded using listwise deletion due to inconsistencies in response patterns across items (e.g., alternating between the lowest and highest possible scores at postintervention without a clear rationale) and one missing item. These response patterns raised concerns about the validity of the data, and excluding them ensured a more accurate estimation of change over time. Data were normally distributed. While there was a slight increase in self-efficacy scores postintervention, the change was not statistically significant—t(15) = -1.67, p = .115, Cohen's d = - 0.36—suggesting that the program may have had a limited impact on caregivers’ confidence in their abilities to support their children. A post hoc power analysis was conducted using G*Power (Version 3.1.9.6) for a paired sample t test. With a sample size of 16 pairs, an effect size of d = -0.36, and an alpha = 0.05, the achieved power was 0.27 or 27%. Power was below the 80% recommended for behavioral sciences (Cohen, 1988).
Family outcomes
No data were missing for this measure. Data were normally distributed. There was an increase in the Family Outcomes from pre- to postintervention assessment. For the overall scale, the change was approaching significance—t(16) = -2.09, p = .053—with a small to medium effect size (Cohen's d = - 0.42). A post hoc power analysis was conducted using G*Power (Version 3.1.9.6) for a paired sample t test. With a sample size of 17 pairs, an effect size of d = -0.42, and an alpha = 0.05, the achieved power t was 0.37 or 37%. Power was below the 80% recommended for behavioral sciences (Cohen, 1988). The subscales Understanding child's strengths and needs—t(16) = -4.40, p < .001, Cohen's d = -0.76—and Knowing your rights and advocating for your child were significant—t(16) = -2.40, p = .029, Cohen's d = -0.54—had a medium to large effect size, and a small to medium effect size, respectively. Differences in all other subscales were not statistically significant.
Social validity
Responses were analyzed using descriptive statistics (see the online supplemental materials). All participants rated the goals, procedures, and outcomes of the program as highly acceptable. The highest-rated statements were “The information discussed in the training is important” (M = 5 out of 5) and “The objectives and goals of the training are important” (M = 5 out of 5). The lowest-rated statements were “Overall, the way I accessed the training was comfortable and allowed me to participate easily in the sessions” (M = 4.56 out of 5) and “The training had positive outcomes for my family” (M = 4.71 out of 5).
Qualitative Findings
Overall, caregivers expressed satisfaction with the goals, procedures, and outcomes of the program. They also provided some suggestions for changes and expressed the need for additional supports. The findings are organized based on Wolf's (1978) social validity framework.
Social validity of the goals
This theme comprises two main subthemes: (a) caregivers need support and training, and (b) the content is appropriate and necessary in the Paraguayan context.
Caregivers need support and training
Caregivers underscored the need for ongoing support and training for caregivers of autistic children in Paraguay. For example, Lucía stated, “It's very hard for us to understand what's happening to our children.” Rebeca emphasized the importance of equipping families with knowledge and strategies to support their children's development and learning, “In Paraguay there is no psychological help or anything for parents. So, all the information the [program] gives is really very enriching, because it helps us as a family to be able to help our children.” Caregivers also emphasized the need for increased autism awareness. As Lidia put it, “Here, for example, in rural areas this issue of awareness remains stagnant. There is a lot of discrimination, unfortunately even from teachers. There is a lack of awareness-raising policies.”
The content is appropriate and necessary in the Paraguayan context
Participants characterized the content of the culturally adapted PTA as “up-to-date” (Lupe and Rebeca), “comprehensive” (Marisa, Noelia and Karen), “important” (Lucía), “helpful” (Andrea), and “necessary” (Lupe). Caregivers also expressed that the program was appropriate for their cultural context and aligned with their everyday experiences and challenges. Fátima highlighted how the program's content and strategies resonated with her beliefs, values, and goals for her child: “For me, the content, the testimonies, the strategies they shared were very consistent and compatible with my beliefs, my values, and what I would like to achieve with my son.” Overall, participants perceived the content of the program as informative and practical as it provided them with the tools and knowledge necessary to better support their children.
Social validity of the procedures
Caregivers reported satisfaction with the procedures used in the program. They discussed five aspects including the program's (a) group format, (b) online delivery, (c) dosage, (d) instructors, and (e) accessibility (free program).
Group format
Caregivers reported high satisfaction with the group format, and reported that it gave them the opportunity to learn from each other's testimonies and the experiences of families with children at different ages and with varied characteristics and challenges. Adriana wrote that one of the most relevant aspects of the program for her was “sharing the experiences with other moms.” Victoria described how this exchange of experiences was beneficial: Meeting other families, other people who are going through the same thing as us and we all supported each other, we gave each other tips, we encouraged each other to continue because as they had, they had children of different ages, so, some could ‘see their child's future’ or tell other [moms with] younger ones, “well, you can do this.”
Caregivers also appreciated the opportunity to share their own experiences and support others. Rita said: We were able to contribute with our experience to the other moms who are new. Because my daughter is already— she's about to turn 8. And there were some moms who are—their son is 2 years old, they are just starting. … It gave us the opportunity to share experiences and listen to the concerns of the other moms.
Marisa shared how she appreciated the space so that caregivers could “express freely, without guilt.” Caregivers described the sessions as “harmonious” (Marisa) and a “meeting among friends” (Sonia). Overall, participants deemed the group format and the number of participants in each group appropriate for promoting learning, providing the opportunity to share and learn from each other's experiences, and creating a supportive community among caregivers.
Online delivery
The participants appreciated the accessibility and flexibility of the program. Many mentioned that attending in-person sessions would have been challenging due to their busy schedules, childcare responsibilities, or geographical constraints. For example, Marisa said, “I think that for many parents who have children with autism, the time factor to attend in-person talks is sometimes super complicated, because we have no one to leave our children with.” Eliana commented on how the online format helped overcome geographical constraints: “Sometimes, this kind of activities are done in Asunción, or in places that are hard for us to get to, because of distance, because of time, and for it [the format] to be virtual, it's great.” While the virtual format was highly praised for its accessibility, some participants acknowledged that it could be challenging, especially for those less familiar with technology or facing internet connectivity issues. Fátima acknowledged how the online format of the program can be a barrier for some families: I like it [the online format] because I am an open person. I have the resources. I have a laptop and good internet. I have a studio, an office where I can go in and study this, which is easy for me in my conditions, but I know that for many people it is not like that, right?
However, despite these challenges, the consensus was that the virtual format was preferable due to its convenience, accessibility, and by reducing geographical limitations.
Dosage
Overall, most participants reported that the frequency of the sessions (i.e., once a week) was appropriate and manageable considering their busy schedules and other commitments. Only Tamara disagreed: “It would have been better if it was at least twice [a week].”
Regarding the total duration of the program (i.e., 10 sessions), opinions varied widely. Some felt that the 10 sessions were appropriate, covering essential topics without being too overwhelming. They found that the sessions flew by quickly, indicating that the duration felt suitable for the content covered. However, others, like Lupe, Liliana, and Lucía, expressed a desire for longer sessions or more sessions overall: “I would have liked it [the program] to be longer, actually” (Lupe). Lucía, Lidia, and Tamara felt that there was more to learn or explore beyond the 10 sessions provided: “For me it can be much more, much, but precisely covering several various topics” (Lucía).
Instructors
The instructors were praised for their kindness, empathy, and ability to explain complex concepts in accessible language. When talking about the instructors, Karen commented, “It was very easy because she always spoke in simple terms, or if there was something we didn't understand. She explained again with examples and all that.” Additionally, participants noted that the instructors’ knowledge, first-hand experience with autism, and use of relatable examples greatly enhanced the learning process. Maribel summarized it like this: The presentation of the instructor and the team [caregiver leaders] that accompanied her was always impeccable because they are also, as I told you, parents with children with autism. So there goes their knowledge and day-to-day experience, which also was very helpful to us.
Free training
Maribel, Noelia, Lidia, Lucía, Valeria, Liliana, and Andrea mentioned that they were grateful for the opportunity to receive the training without cost. They commented on how families of autistic children have many expenses associated with child therapies and how caregivers often encounter additional challenges to maintain employment. Lidia shared: I don't have income; I don't have work income. So, when I looked at Facebook, the advertisement said that registration was free, that everything was free—because there are, for example, some courses that you have to pay for. And it's fair to pay. [But] these are very important opportunities. We have to learn to take advantage of the opportunities to receive training.
Social validity of the outcomes
Caregivers shared their perspectives on how the program impacted them. Caregivers commented on four main outcomes: (a) increased knowledge and understanding autism and their children better, (b) sense of community, (c) empowerment, and (d) implementation of strategies.
Increased knowledge and understanding
Caregivers reported that the program helped them to increase their knowledge on various topics, such as communication strategies, myths about autism, and curricular adaptations. Additionally, participants appreciated learning about evidence-based practices and gaining practical tools to support their children. Noelia commented on how she changed her perspective as she learned the importance of using evidence-based practices to support her son instead of “trying everything”: Because it taught me to look at many things through different eyes and to be able not to have that desperation of doing something without having some concrete proof. Because it is like torture, for the children, when you, as a parent, try to do things without having some kind of knowledge.
Caregivers also mentioned gaining a deeper understanding of their children's needs, behaviors, and unique characteristics related to autism. Valeria commented, “It also helped me as a mother to understand my son better. Because before this course I didn't understand him. Not at all.”
Sense of community
Caregivers characterized the program as a “support group” where at the same time you are “learning new things” (Tamara) and a “therapeutic group” (Victoria). Belén reflected on how meeting other mothers and listening to their experiences impacted her: “So, when I listened to them [the other mothers], I said, well, if they were able to overcome this, it gives me the courage to continue fighting.” Similarly, Lupe reflected: It's nice to talk to people who go through the same thing as you. It helps you be more empathetic. And it also shows you that there are people who understand you, that you are not the only one who is going through this situation and that your son is not a very strange person either, but rather it is a process, a condition where he sees the world differently.
Empowerment
Caregivers reported renewed confidence, knowledge, and tools to advocate for their autistic children. Fátima reflected on how the program empowered her to support her child in his current developmental stage: The program was very positive for me. It empowered me again. During the pandemic, I also took an online course on autism, but my son was 3 years old at that time. So, I feel that those tools that I had learned were no longer working for me. So now that I learned again and refreshed myself, it empowered me again for the stage that my son is living right now.
Marisa commented on how the program gave her tools to advocate for her children: “They gave us tools so that we can advocate for our children, because before we were kind of in a nebula, everything was blank. We kind of knew, but with this training, now no one is going to silence us.” She then added, “It [the program] gave me more confidence in myself and it strengthened my knowledge to apply it with my children.”
Implementation of strategies
Caregivers shared that they implemented strategies they learned in the program which improved their ability to understand and support their children. Fátima, Victoria, Noelia, and Belén shared how learning strategies to manage behavior helped them remain calm when their children engaged in challenging behavior and to identify antecedents to behavior. Fátima described how she approached challenging behavior: Because that is exactly what we are experiencing now with my son, the tantrums. So, understand that there is an antecedent, something that generates it first, for that behavior to be shown, right? So now I know it's, like, “Ok, what happened?” I try to understand and then give him an alternative to regulate himself.
Karen, Belén, Fátima, and Lupe, shared that they learned about the importance of play and started investing more time in shared play, which helped them “teach [their children] things through play” (Belén) and “create spaces to connect” with their children (Fátima).
Another set of strategies that caregivers reported as helpful were the self-care strategies. Valeria shared the importance of self-care and how implementing the strategies impacted her: The part that talked about how we could take care of ourselves as caregivers. And it's something that really touched me because it was already affecting me. I'm not saying that I'm super, a 10 now, but I'm trying to take better care of myself.
Challenges and suggestions for improvement
Caregivers identified some challenges that hindered their participation in the sessions. Additionally, they provided suggestions for adding components to the program to address their needs for additional supports.
Challenges to participation
Participants reported challenges to participation including scheduling and childcare. Eliana mentioned that the Saturday afternoon schedule conflicted with some of her work responsibilities: “The only thing that was hard for me was the schedule; sadly, I couldn’t participate in some sessions because it conflicted with some job-related activities.” Lucía, Maribel, and Valeria reported challenges balancing participation in the training sessions while caring for their children, affecting their levels of engagement and focus during the sessions. Maribel said, My son, the one who has autism, was here with me because his father had other activities. So, it was me trying to be in the session, right? I didn't want to get lost and also had to look after [child's name] a little bit, right?
Need for additional supports
Caregivers expressed a need for ongoing guidance and support after completing the program, particularly to support the practical implementation of the strategies they learned. For example, Lidia said, “I understood. To put it into practice is what is a little … it is very difficult.” Valeria, Lupe, Andrea, and Fátima had specific suggestions on how the program could provide additional support to apply what they learned to their own situations. Valeria suggested, “It would have been nicer to have more videos.” Similarly, Lupe said it would be nice to have “additional demonstrations.” Andrea suggested increasing the number of sessions to provide case-by-case guidance on how to apply the strategies to specific situations: I would add two more Saturdays; they would simply be to be able to address better strategies or a greater number of strategies. Or see, for example … being able to share, “Look, hey, I'm having trouble implementing this, what strategies could we use?” For example, well, I'm going to commit to creating some play routines in my house with my son. Oh well, [you] call me on Wednesday [and ask], “What, what did you play? How was this session for you? What did you see differently?” That accompaniment to the parent, the mother or the person on something that is put into practice.
Integration of Findings
A joint display was created for the purpose of integrating quantitative and qualitative findings and generating meta-inferences to answer the research questions (see Figure 1 for the Joint Display). The meta-inferences generated through the process of creating the joint display and examining the data include (a) Caregivers of autistic children in Paraguay need support and training, (b) The online group training program supported learning of new knowledge and provided a sense of community for caregivers of autistic children, (c) Caregivers gained knowledge and were able to better understand their autistic children's strengths and needs through the program, and (d) The program was feasible and acceptable in the Paraguayan context. Caregivers valued the goals, procedures, and outcomes of the program.
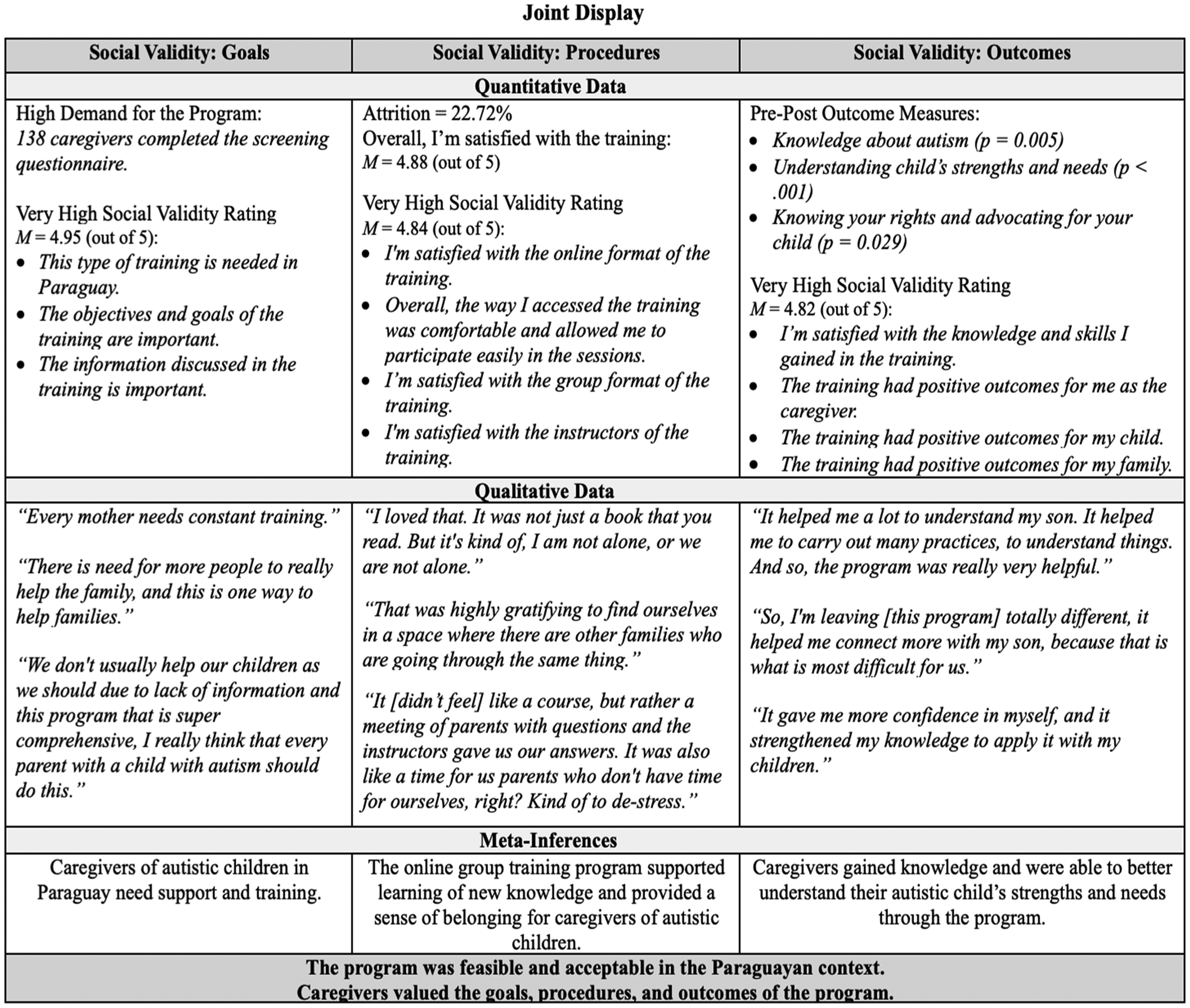
Joint Display.
Discussion
The purposes of this study were to evaluate the outcomes and assess the social validity of the culturally adapted PTA in the Paraguayan context. Through the integration of quantitative and qualitative findings, we generated four meta-inferences that we will further discuss next.
Caregivers of Autistic Children in Paraguay Need Additional Support and Training
In alignment with previous studies, findings from this study highlight need for additional training and support for caregivers in Paraguay (Terol et al., 2023; Terol, Meadan, et al., 2024) and the region. For example, in their study with Panamanian caregivers of children with disabilities, Bhana Lopez et al. (2023) identified caregivers’ need for reliable information and the creation of low-cost or free instructional materials on evidence-based strategies in Spanish as a pressing priority. In a review of parent education interventions, Dawson-Squibb et al. (2020) found studies published in peer-reviewed journals across all continents except South America. Similarly, DuBay's (2022) scoping review of parent-mediated autism interventions for Latin American families identified only one study conducted in South America, while the rest were conducted in the United States. Caregivers in Latin America have reported extensive needs associated with caring for their autistic children (Montenegro et al., 2022; Paula et al., 2020). The current study is among the first describing the implementation of a culturally adapted caregiver training program for caregivers of autistic children in the South American context with Spanish-speaking participants. The findings suggest that caregiver training can address some of the needs reported by caregivers in this context, such as limited information to access services and low caregiver knowledge of autism.
Learning Online in a Group Format is Acceptable
The present study was the first PTA implementation to be planned for online delivery as part of the cultural adaptation process (Terol, Meadan, et al., 2024). However, the PTA implementation studies reported by Dababnah et al. (2023) and Xu (2021) were delivered with some online components and completely online, respectively, due to restrictions associated with the COVID-19 pandemic. While participants in Xu's (2021) study mostly reported drawbacks of online delivery, Dababnah et al. (2023) reported that the unexpected shift to online delivery added some flexibility in scheduling and delivery of the program overall. In the current study, online delivery was deemed highly acceptable, and although two caregivers mentioned that childcaring responsibilities interfered with their participation in the sessions, most caregivers reported having the opportunity to participate in the training while also being able to take care of their children as an asset. This suggests that while in-person delivery may facilitate access for some, online delivery is a valuable alternative for many families as it helps to overcome common barriers associated with in-person delivery, such as limited availability of time and resources to commute, geographical distance, and childcare (Hao et al., 2021; Terol et al., 2023).
In alignment with previous studies, caregivers in the present study reported that meeting with other caregivers made them feel understood and less isolated, which helped them to develop a sense of belonging and community (Lee et al., 2024; Pearson & Meadan, 2021). Participants’ high satisfaction with the combination of caregiver leaders as co-instructors and the group delivery format extends previous research on the high acceptability of parent-to-parent support and its suitability among caregivers in LMICs where resources for autistic children and their families are limited (Lee et al., 2024).
Positive Outcomes for Caregivers
Quantitative and qualitative data indicate that caregivers gained knowledge and were able to better understand their autistic children's strengths and needs. The current study extends previous studies implementing PTA with similar results showing significant increases in knowledge about autism (Dababnah et al., 2023; Magaña et al., 2017), and in understanding of their children's strengths and needs (Lopez et al., 2019; Magaña et al., 2017; Magaña, Tejero Hughes, et al., 2021). Programs designed to increase caregivers’ knowledge about disability in general and autism specifically might be especially important in LMICs where stigma and lack of awareness about autism may further hinder families’ access to the already scarce available services and supports (He et al., 2024; Lee & Meadan, 2021).
Caregivers’ increase in advocacy knowledge and skills is particularly notable when considering the Paraguayan context. In LMICs, little information is available about existing policies and laws concerning childhood disability (Maulik & Darmstadt, 2007). Notably, families and individuals with disabilities in several LMICs, including Paraguay, have reported high stigma attached to disability (Montenegro et al., 2022; Terol et al., 2023). Therefore, equipping caregivers with knowledge about their rights and strategies for advocating for their children in this context is particularly crucial and may empower them to navigate complex systems and challenge societal attitudes toward autism.
Interestingly, there were no significant pre/postintervention changes in caregivers’ self-efficacy, or in three Family Outcomes Survey subscales: (a) helping their children develop and learn, (b) having support systems, and (c) accessing the community. This lack of statistically significant changes may be due to the study being underpowered, indicating that a larger sample size might be necessary to detect more subtle changes in these areas. However, there may be other reasons for these changes to be small, such as the relatively short duration of the program, the need for additional supports, including complementing training with coaching, and context-level issues related to the availability of resources in the community. Regarding caregivers’ self-efficacy, caregivers’ scores at preintervention were high, indicating a possible ceiling effect. Because the participants were performing at the upper limit of the scale at preintervention, the ability to detect further improvements or differences at postintervention was limited. Additionally, the self-efficacy measure was not previously culturally adapted or validated in Spanish, which may have affected how it captured the construct.
The Culturally Adapted PTA Program is Socially Valid
Overall, the program was found to be feasible and acceptable in the Paraguayan context. The findings of this study suggest that the initial steps in the process of culturally adapting the PTA were appropriate (Terol, Meadan, et al., 2024). Involving key community members such as professionals working with young autistic children in the country, caregivers of autistic children, and autistic adults and the guidance of the CAC framework (Lee et al., 2023), were key in the process of cultural adaptation. This pilot study was part of the iterative process of cultural adaptation and suggestions from the participants should be incorporated into future iterations.
Limitations
The present study has some limitations worth mentioning. First, the sample size was small, and the study was underpowered. Additional research implementing a more rigorous and experimental methodology, such as a randomized controlled trial, is needed to provide more robust evidence of the effects of the culturally adapted PTA. Another limitation is that all measures were self-reported, which poses a risk for social desirability. Additionally, some of the measures were not previously culturally adapted or validated in Spanish. In future research, observational measures may strengthen the results. Notably, although participants in this sample were diverse in terms of geographical location and employment, all were women, and all but one were mothers. Fathers and extended family members who often provide care to autistic children were underrepresented in this study. Additionally, it is likely that caregivers who participated in this study have higher education levels than the general population in Paraguay. Caregivers in this study had high scores at preintervention, particularly in self-efficacy. This may suggest a selection bias, as those who chose to participate in the study might already possess higher levels of confidence and skills in managing their caregiving roles, potentially skewing the results and limiting the generalizability of the findings. Furthermore, future studies should incorporate direct child outcome measures to provide a more comprehensive evaluation of the program's effectiveness.
Implications for Policy and Practice and Directions for Future Research
The findings from the present study underscore the need for policies and initiatives aimed at increasing autism awareness and expanding the availability and accessibility of support and training for caregivers of autistic children in Paraguay and other countries in the region. Despite growing recognition of the importance of early intervention and family support for children with autism, significant gaps remain in public awareness and service availability for this population in Paraguay (Terol, Xia, et al., 2024). There is a pressing need for increased funding and capacity building of researchers in LMICs to increase and improve contextualized research to better understand the potential for sustainability and the scale-up of culturally appropriate supports and interventions for autistic children and their families (Muttia et al., 2022).
In practice, it is important to increase availability and the sustainable implementation of culturally relevant caregiver training and coaching models within existing systems of care. While researcher-led initiatives are valuable for establishing an evidence base, there is a need to explore pathways for integrating and sustaining supports offered through community-based services. To this end, one strategy may be to build the capacity of local service providers, educators, and leaders in community-based organizations serving autistic children and their families. In this study, two caregiver leaders identified by a community-based organization for their leadership skills and their experience supporting families co-delivered the intervention, providing preliminary evidence of the feasibility and acceptability of this model in the Paraguayan context. Partnerships between community-based organizations and local service providers may facilitate the sustainability of support and training for caregivers of autistic children.
There are several important considerations for future research. First, as noted by Dawson-Squibb et al. (2020), there is a pressing need for studies with more rigorous methodology and larger sample sizes in LMICs to enhance the robustness of the findings and their generalizability. Second, caregivers in this study expressed a desire for additional, more individualized training beyond the scope of the culturally adapted PTA. Future research should explore integrating complementary components, such as individualized coaching, access to professional consultations, or booster sessions, to better support caregivers in applying the learned strategies and to address additional needs. Finally, future research could focus on evaluating the delivery of the program without direct support from the researcher, implementing a cascading model or train-the-trainer model (Biggs & Meadan, 2018), in order to strengthen the capacity of community members. This model has been effective in other LMICs and has been suggested as a viable alternative when the availability of specialized professionals is limited (Divan et al., 2015). While research employing more rigorous designs and with larger samples is warranted, these findings highlight the feasibility and acceptability of adapting programs to expand access to support and training for caregivers of autistic children in LMICs.
Supplemental Material
sj-docx-1-ecx-10.1177_00144029251375983 - Supplemental material for Pilot Implementation of a Culturally Adapted Training for Caregivers of Young Autistic Children: A Mixed Methods Study
Supplemental material, sj-docx-1-ecx-10.1177_00144029251375983 for Pilot Implementation of a Culturally Adapted Training for Caregivers of Young Autistic Children: A Mixed Methods Study by Adriana Kaori Terol, Hedda Meadan and Sandy Magaña in Exceptional Children
Footnotes
Authors’ Note
All authors are contributing writers and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of the University of Illinois Urbana Champaign. Informed consent was obtained from the participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.