
Abstract
Mental health is a significant public concern. Given that individuals spend extended periods indoors, understanding the psychophysiological health effects of indoor materials on well-being is crucial. This study compared the effects of wooden and resin plaster rooms on psychophysiological well-being. Well-being was assessed using heart rate variability measurements and an affective well-being questionnaire. Subjective perceptions were also evaluated using a semantic differential questionnaire. The results indicated higher heart rate variability in the wooden room compared to the reference room. Participants breathed about one breath per minute more slowly in the wooden room, with a negative correlation between heart rate variability and respiratory rate. Positive affect was elevated, and negative affect was reduced in the wooden room, which was also perceived more favorably in sensory evaluations. The findings suggest that wooden interiors are preferred over artificial materials, enhancing both physiological and psychological well-being.
Health Benefits of Natural Environments
Stress and psychological illnesses are substantial public health concerns at present. The famous biophilia hypothesis proposes that humans have an innate tendency to affiliate with the natural environment and that nature’s connection helps humans recover from psychophysiological stress (Richardson & Butler, 2022; Robinson & Breed, 2020; Wilson, 1984). The wellbeing benefits of nature have been extensively researched, with two theoretical frameworks linked to the biophilia hypothesis: the Attention Restoration Theory by Kaplan and Kaplan in 1989 and the Stress Recovery Theory by Ulrich in 1983. The former emphasizes cognitive benefits, while the latter focuses on stress reduction. Research supports links between nature exposure and enhanced physiological and psychological health (Berto, 2014; Bratman et al., 2022; Haluza et al., 2014; Mygind et al., 2019). Since long periods are spent indoors, it is essential to consider using elements of nature in the indoor environment to enhance well-being. Studies have shown beneficial well-being responses to indoor nature elements (Aristizabal et al., 2021; Mcsweeney et al., 2015; Perrins et al., 2021) and to solely viewing elements of nature as reviewed by Grinde and Patil (2009), Jo et al. (2019) and Lipovac and Burnard (2020). Unlike other biophilic elements, wood is often used as a building material, and it can cover large areas in a room to provide significant natural stimulation. The effects of wooden interiors have been investigated in several studies, but the physiological results are highly diverse.
Previous Wooden Interior Studies
The physiological effects of 90 s exposure to different amounts of wooden material have been examined by Sakuragawa et al. (2005) and Tsunetsugu et al. (2002, 2005, 2007). There are results for increased brain activity and decreased blood pressure in all rooms regardless of the interior wood ratio, which was 0% to 90% (Tsunetsugu et al., 2002, 2005, 2007). The heart rate was increased in the rooms with more wood (Tsunetsugu et al., 2002, 2005, 2007). Bamba and Azuma (2015) measured the effect of a 10 min stay in a wooden room compared to the control after completing an arithmetic task. They found no differences in heart rate variability (HRV) or salivary amylase concentrations. Psychological responses to short wooden exposures were found to be better or similar in wooden rooms compared to controls (Bamba & Azuma, 2015; Demattè et al., 2018; Sakuragawa et al., 2005; Tsunetsugu et al., 2002, 2005, 2007). Recently longer (60–75 min) exposures have been investigated where participants were working in wooden offices, and more differences in outcomes have been reported between the rooms. Shen et al. (2019) showed improved cognition in wooden rooms compared to a white control room. Burnard and Kutnar (2020) measured lower salivary cortisol in an oak room but not in a walnut room compared to controls. Zhang et al. (2016) and Zhang et al. (2017) found reduced heart rates, HRV, and blood pressure, as well as increased skin resistance, oxyhemoglobin saturation, and psychological well-being in wooden rooms compared to a white control room. The effects of wooden furniture have also been investigated. Douglas et al. (2022) found lower skin conductance and negative stress in a room with wooden furniture. Lipovac et al. (2022) found no change in HRV, skin conductance, or affective states in a room with a wooden table. The results are inconsistent, showing all positive, negative, or no health outcomes in wooden interiors. There are methodological limitations to the studies, as explained in more detail in reviews by Bower et al. (2019), Ikei et al. (2017), and Lipovac and Burnard (2020). There is still a lack of controlled research related to the psychophysiological health benefits of the wooden indoor environment.
HRV as an Indicator of Psychophysiological Well-Being
HRV is a non-invasive and well-established indicator of psychophysiological well-being. It has been widely used as an outcome measure and a specific target for treatment (Laborde et al., 2017; Shaffer & Ginsberg, 2017). HRV reflects the changes in parasympathetic and sympathetic control of the heart as a response to environmental and psychological influences. Parasympathetic activation is associated with normal bodily functioning under relaxed conditions and facilitates recovery. The sympathetic nervous system is responsible for stimulating activities in the body when facing a stressful situation. Higher HRV indicates higher parasympathetic activation, better health (Shaffer et al., 2014; Thayer et al., 2012), and self-regulation at the cognitive, affective, and social levels (McCraty & Shaffer, 2015). Lower HRV is related to higher morbidity, mortality, and psychological problems like depression, anxiety, and stress (Shaffer & Ginsberg, 2017). Given that the indoor environment affects humans physically and emotionally (Burnard & Kutnar, 2015; Ikei et al., 2017), HRV is an ideal measure for assessing the effects of wooden interior spaces on well-being.
HRV in Previous Wooden Interior Studies
Many HRV parameters can be calculated either with time-domain methods such as the standard deviation of interbeat intervals (SDNN) and root mean square of successive differences (RMSSD) or frequency-domain analyses such as low frequency (LF; 0.04–0.15 Hz) and high frequency (HF; 0.15–0.40 Hz) bands. RMSSD reflects parasympathetic activity and is a widely used and recommended parameter for psychophysiological assessments (Laborde et al., 2017). In their review, Jo et al. (2019) show inter alia higher RMSSD and HF values when viewing nature compared to a reference scene. HRV has been measured in a few previous wooden room studies. Zhang et al. (2017) found lower HRV when working in a wooden office but did not report the HRV parameters. Kotradyova et al. (2019) measured no change in the LF/HF ratio after moving freely for 20 min in a wooden waiting room. Bamba and Azuma (2015) found no differences in HF values or the LF/HF ratio between the wooden and control rooms. HF also reflects parasympathetic activation, but there is no consensus on the physiological underpinning of the LF/HF parameter (Laborde et al., 2017; Shaffer & Ginsberg, 2017). One reason for the lack of HRV improvements in the wooden rooms might be the day-to-day variation of the HRV due to the different amounts of accumulated psychophysiological stress. Another challenge with previous research is between-subject designs for the reason that differences in physiological baseline values can be tenfold, and measurable changes are very small. Therefore, more studies, preferably with a one-session cross-over design, are needed to minimize the potential for results bias.
Purpose of the Present Study
The purpose of this study was to compare the HRV-derived psychophysiological well-being in wooden and reference rooms during the same session. Higher HRV within a wooden room compared to a reference room would suggest a positive effect on psychophysiological well-being, indicative of enhanced relaxation. Conversely, a lower HRV would suggest a negative impact, potentially reflecting increased stress or discomfort. Our findings, therefore, directly link changes in HRV to the psychophysiological impacts of the environments tested, supporting the specific contributions of different interior materials to health and well-being.
It was hypothesized that RMSSD, as the primary outcome, would be higher in the wooden room compared to the reference room. As explorative secondary outcomes, affective well-being was measured with Warr’s questionnaire (Warr, 1990) and the multidimensional perception of the rooms was examined with a semantic differential questionnaire (Osgood, 1952). Investigating the interplay between physiological, affective, and sensory responses should give a comprehensive idea of the environmental impact on a person.
Materials and Methods
In a randomized, cross-over study, 45 participants relaxed in both a wooden and a resin plaster room for 10 min each, with a 2-min washout period outside the rooms between exposures. While the room’s door remained closed for isolation, the researcher monitored the participants’ HRV externally. After each 10-min session participants completed questionnaires assessing affective well-being and semantic differential evaluations in the respective rooms.
Participants
The participants were 45 healthy Finnish individuals (32 females and 13 males) with a mean age of 43 years (SD = 13), a height of 169 cm (SD = 9), and a weight of 76 kg (SD = 15). They represent various primary occupations: employed (n = 36), unemployed (n = 1), retired (n = 4), studying (n = 3), and on maternity leave (n = 1). Recruitment was conducted through a variety of digital platforms, including Twitter, LinkedIn, Instagram, Facebook, and TikTok, to allow for wide and varied pool of participants. The study was presented as an “inner surface material study,” with no mention of wood or its potential well-being effects in either the announcements or during the measurements. Exclusion criteria included conditions that could potentially affect the behavior of HRV. Participants on cardioactive medications, such as antiarrhythmic drugs, β-blockers and sedatives, as well as those with cardiac-related illnesses, like myocardial dysfunction, were excluded from the study (Malik, 1996). The participants were asked to avoid exercise and alcohol for 24 hr, and food, caffeine, and other stimulants for 2 hr prior to measurements. Before testing, the participants were informed about the procedures and gave their written informed consent. The study was approved by the ethics board of the South-Eastern Finland University of Applied Sciences and was carried out in conformity with the Declaration of Helsinki.
Experimental Rooms
Two identical rooms were constructed for the experiment (Figure 1), with walls and floors made from solid wood (cross-laminated timber, CLT Plant Oy, Kauhajoki, Finland) and roofs of transparent polycarbonate material (Makrolife, Foiltek Oy, Vantaa, Finland) to facilitate natural lighting. The dimensions of the rooms (area = 6.08 m2; volume = 12.90 m3; maximum height = 2.90 m and maximum width = 3.67 m) were planned to ensure that the surface materials were in close proximity to participants, maximizing their effect, while also being spacious enough to accommodate comfortable use by individuals in wheelchairs (Futudesign Oy, Helsinki, Finland). The rooms taper upward, not maintaining the same area from floor to roof and lacking right angles, incorporating several corners, which adds unique architectural elements. Additionally, the design accommodates potential future uses, such as office space, ensuring practical utility beyond the experiment (Burnard & Kutnar, 2020).

Views and photos of the study rooms. (a) Window view of the wooden room. (b) Window view of the reference room. (c) Interior of the wooden room. (d) Interior of the reference room.
The only difference between the rooms was the surface materials, which can be seen in the mood board (Figure 2). The interior surfaces were treated so that the walls and floor were recognizably wooden in the wooden room; on the other hand, the reference space had no recognizable wooden surfaces. In the wooden room, the wall surface material was spruce (Picea abies, cross-laminated timber, CLT Plant Oy, Kauhajoki, Finland) with a translucent oil wax surface treatment (Osmo Clear Color Oil Wax, Sarbon Woodwise Oy, Lahti, Finland), and the floor was oil-waxed pine parquet (Pinus sylvestris, Country Collection Wooden Floors, Timberwise Oy, Loimaa, Finland). In the reference room, the walls were coated with gray resin plaster (Art Stuc Pava Fino, Pava Resine, San Martino di Lupari PD, Italy), which is a commonly used surface material. The floor surface was coated with gray resin plaster (nontransparent Art Stuc Grosso, Pava Resine, San Martino di Lupari PD, Italy) with preservative (Idropol 131, Pava Resine, San Martino di Lupari PD, Italy).
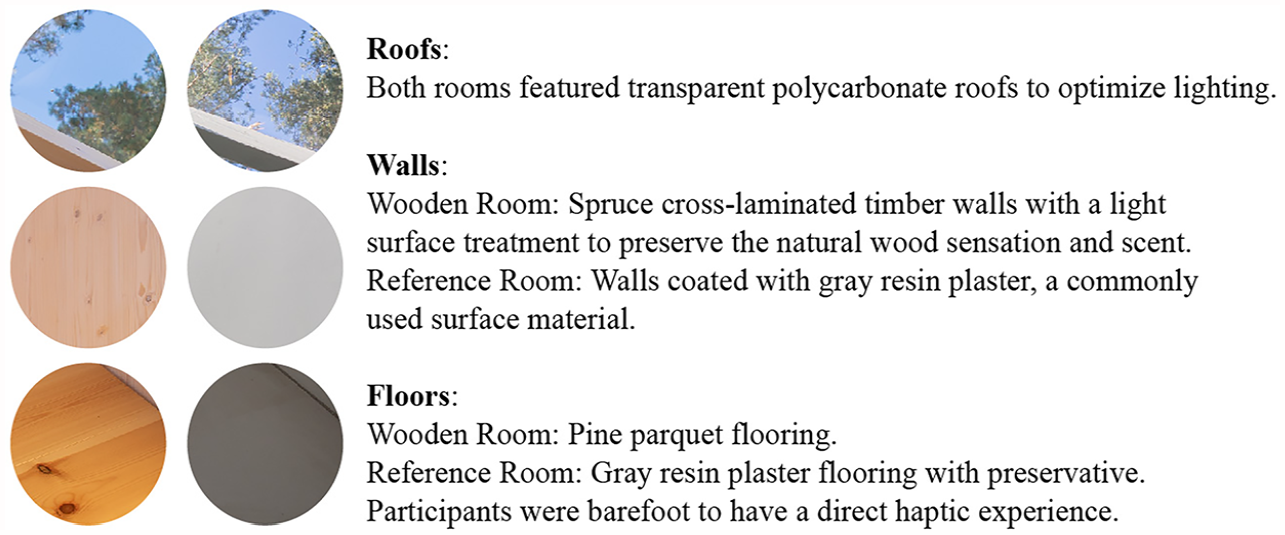
Mood board of the materials.
To ensure consistency, both rooms were furnished with only a single chair placed in the middle of the room and equipped with a thermometer (Wiiste WM1-WAN, Wiiste Oy, Tampere, Finland). The temperature was 25ºC, and the humidity was 43% during the measurement period.
Experimental Design
All measurements were done on one occasion, during which participants stayed in the wooden room and reference room in a randomized order (Urbaniak & Plous, 2013). The same procedures were repeated in both rooms. The participants were barefoot during the experiments to have a direct haptic experience of the surface material. First, the participants were asked to sit and relax for 10 min while the researcher (standing outside the room) measured the HRV. Following this an iPad was brought in for the participant to fill out affective well-being and semantic differential questionnaires. Thereafter the participant left the room. There was a 2 min washout period outside the rooms before entering the second room.
HRV Measurement
HRV data was recorded with a Polar H10 heart rate sensor (Polar Electro Oy, Kempele, Finland) with a sampling frequency of 1,000 Hz. The Polar H10 is an advanced model of the Polar H7, which has been shown to be a valid heart rate monitor when recording beat-to-beat (RR) intervals for HRV analyses (Giles et al., 2016). The heart rate sensor was mounted on a chest strap at the xiphoid process level and connected via Bluetooth to a validated Elite HRV application (Asheville, North Carolina, USA) on an iPad (Chhetri et al., 2022). The HRV was measured in a seated position for 10 min, of which the first 5 min were considered a heart rate stabilization period, and the last 5 min were analyzed (Laborde et al., 2017; Malik, 1996). The Elite HRV raw data was saved as RR interval data files, with an interval in ms. The data files were exported to a laptop and analyzed using Kubios HRV Scientific 4.0.1 software (Niskanen et al., 2004).
First, artifacts were removed and corrected following international Task Force guidelines (Malik, 1996) with an accurate and validated automatic correction method (Lipponen & Tarvainen, 2019). Following the correction, the RR interval data was considered normal and thus described as NN data. Subsequently, the primary outcome of RMSSD and the secondary outcomes of SDNN, LF, HF, and respiratory rate were analyzed for a broader description, as Laborde et al. (2017) recommended. A time domain analysis (RMSSD and SDNN) concerns the statistical representation of the variation in NN intervals within a sample (Malik, 1996). A frequency domain analysis provides basic information on how power distributes as a function of frequency using a fast Fourier transformation (nonparametric). A fast Fourier transformation allowed the analysis of the components of the power spectrum density to be quantified into different frequency bands, and following this, two spectral components of the recording were calculated: LF (0.04–0.15 Hz) and HF (0.15–0.40 Hz) as recommended (Malik, 1996). An estimate of the respiratory rate was computed from the RR data using Kubios (Tarvainen et al., 2014).
We employed two resting state HRV measurements to compare differences between conditions, as outlined in the study which informed our sample calculation (Gladwell et al., 2012). According to HRV guidelines, short-term resting HRV recordings should last at least 5 min and be conducted following a stabilization period of no less than 5 min (Laborde et al., 2017; Malik 1996). Our study utilized an acute randomized crossover design, which allows for direct comparison between two conditions without the need for a separate third baseline condition. Instead, each environment—both the wooden and the resin plaster rooms—was treated as an individual condition with its own inherent baseline (Gladwell et al., 2012).
Affective Well-Being Questionnaire
The assessment of psychological affective well-being utilized Warr’s questionnaire (Warr, 1990), which is grounded in the circumplex model of affect proposed by (Russell, 1980). Dimensional models, chosen for their comprehensive range and balanced approach, are particularly suited for characterizing basic affective reactions. The measure of affective well-being has frequently been employed as a metric for internal recovery in previous research (Kim et al., 2017; Virtanen et al., 2021).
The instrument includes 12 adjectives derived from Warr’s work to measure affective well-being. In analyzing these responses, we adopted a two-dimensional configuration as recommended by Watson and Tellegen (1985), focusing on positive and negative affect. Positive affect refers to the extent of an individual’s pleasurable engagement with the environment, characterized by feelings such as calmness, contentment, relaxation, cheerfulness, enthusiasm, and optimism. Conversely, negative affect involves feelings that reflect distressing engagement with the environment, such as tension, unease, worry, depression, gloominess, and misery.
Participants were prompted to evaluate their current emotions, marking their responses on a 6-point scale, ranging from 1 (not at all) to 6 (extremely). The questionnaire items were analyzed using this two-dimensional configuration, yielding reliabilities of Cronbach’s α = .91 for positive affect and Cronbach’s α = .86 for negative affect.
Semantic Differential Questionnaire
The subjective perception of the rooms was assessed using a semantic differential questionnaire, a validated method for gauging individuals’ attitudes toward a given subject (Osgood, 1952). The instrument comprised 17 bipolar adjective pairs, and participants evaluated their immediate environment by selecting the most suitable option on a 7-point scale. A majority of the adjective choices stemmed from extant research on various materials (Bumgardner & Bowe, 2002; Demattè et al., 2018; Fleming et al., 2013; Lindberg et al., 2013). There was adjective pairs for five category: visual (dark to bright, beautiful to ugly, rich to bland, harmonious to chaotic), tactile (cold to warm, rough to smooth, hard to soft), olfactory (fetid to aromatic), auditory (reverberant to muffled, noisy to silent), and emotional (natural to artificial, stressful to relaxing, unknown to familiar, unpleasant to pleasant, interesting to boring, cheerful to sad, safe to unsafe). This method allowed us to evaluate how the specific characteristics of the environment influenced both physiological and affective responses, thereby linking wellbeing with physical space.
Statistical Analysis
Analyses were performed using IBM SPSS, version 28.0.1.1. Drawing from the RMSSD findings in a study by Gladwell et al. (2012) and assuming a minimum effect size of 0.40, a total of 45 participants was determined to achieve 80% power at a .05 significance level with a two-tailed test, assuming an r correlation of .90. For secondary outcomes, the minimum detectable differences with 80% power at a 5% significance level were established as follows: SDNN (3 ms), LF (600 ms2/Hz), HF (160 ms2/Hz), respiratory rate (0.5 breaths/min), affective well-being (1.9), and adjective pairs (0.6). Calculations for affective well-being derived from Virtanen et al. (2021) and for adjective pairs from Demattè et al. (2018).
The Shapiro–Wilk’s W-test assessed the normality of data distributions. Except for the respiratory rate, data were not normally distributed. Consequently, differences between the wooden and reference rooms were analyzed using the nonparametric, two-tailed Wilcoxon’s signed-rank test. The Spearman rank-order correlation examined the relationship between changes in LF values and respiratory rate shifts. The significance level was set at p < .05. Unless stated otherwise, all data are given as median and interquartile range for the nonparametric tests.
Results
HRV Parameters
The HRV results are presented in Figure 3. It was hypothesized that the RMSSD would be higher in the wooden room (Mdn = 23.6 ms, IQR = 38.1 ms) compared to the reference room (Mdn = 25.2 ms, IQR = 35.3 ms). However, there were no significant differences, Z = −0.58, p = .571. Additionally, the other time domain measure, SDNN, did not differ significantly between the rooms: wooden (Mdn = 30.9 ms, IQR = 34.5 ms) and reference (Mdn = 29.8 ms, IQR = 33.8 ms), Z = −1.73, p = .084.
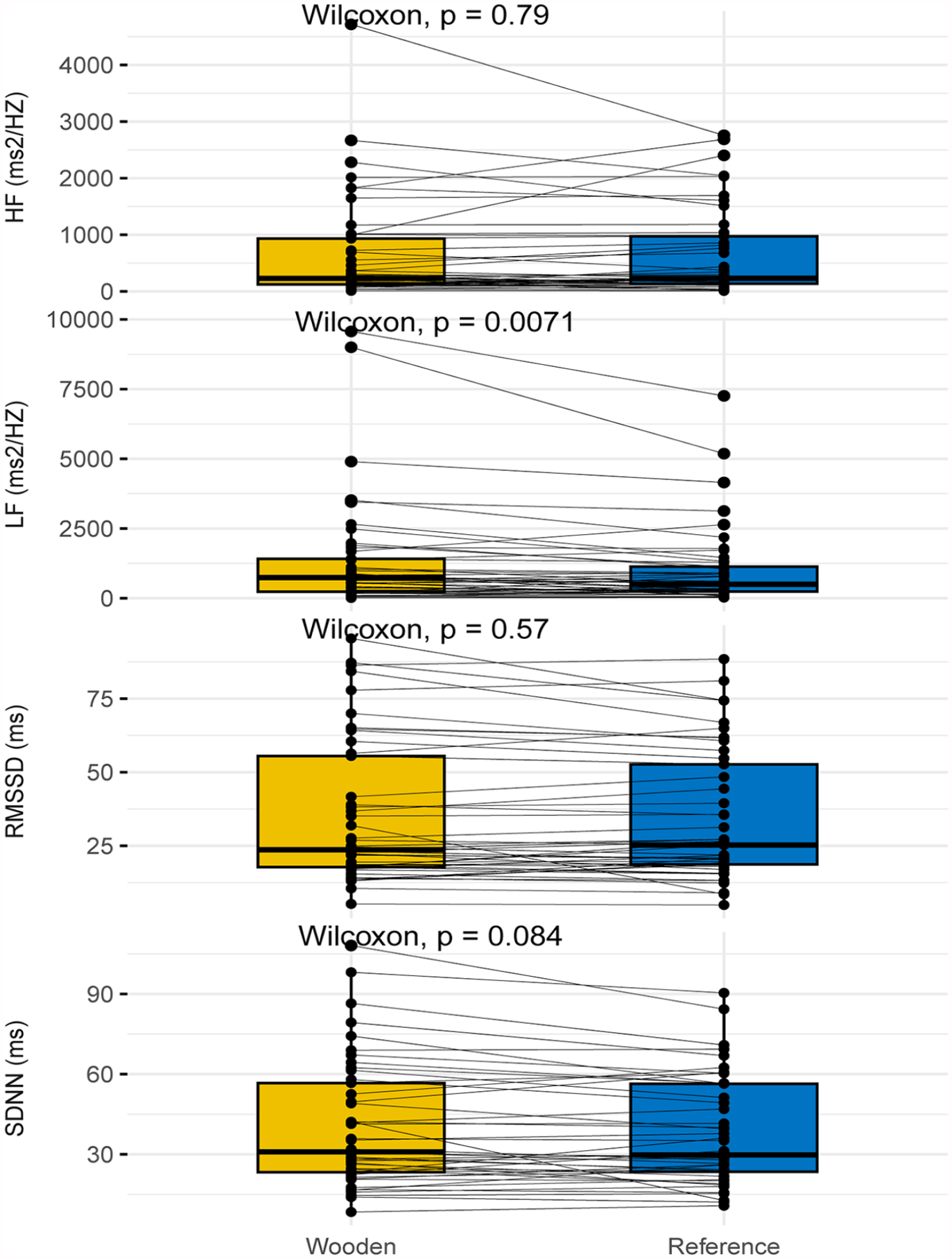
Heart rate variability results in the wooden and reference rooms.
For the frequency domain parameters, LF was significantly higher in the wooden room (Mdn = 743.8 ms2/Hz, IQR = 1,328.9 ms2/Hz) than in the reference room (Mdn = 593.3 ms2/Hz, IQR = 978.1 ms2/Hz), Z = −2.66, p = .007. Yet, there were no significant differences in the HF values between the wooden room (Mdn = 229.2 ms2/Hz, IQR = 841.3 ms2/Hz) and the reference room (Mdn = 231.5 ms2/Hz, IQR = 849.4 ms2/Hz), Z = −0.28, p = .790. Due to the high variability of the LF power, relative values were calculated as percentages of the total HRV power. The relative LF values were significantly different between the wooden room (Mdn = 70.3%, IQR = 17.6%) and the reference room (Mdn = 54.2%, IQR = 24.9%), Z = −2.13, p = .033. The difference in total power approached significance, with medians of 1,034.8 ms2/Hz (IQR = 2,686.9 ms2/Hz) and 942.9 ms2/Hz (IQR = 2,149.5 ms2/Hz) for the wooden and reference rooms, respectively, Z = −1.82, p = .068. These findings suggest that the wooden interior has a significant effect on LF, but not on other HRV parameters.
RR-Related Respiratory
The RR-related respiratory rate is presented in Figure 4. The respiratory rate was significantly lower in the wooden room (Mdn = 12.8 breaths/min, IQR = 5.3 breaths/min) compared to the reference room (Mdn = 13.8 breaths/min, IQR = 2.9 breaths/min), Z = −1.98, p = .048. The corresponding medians in hertz were 0.21 Hz (IQR = 0.09 Hz) for the wooden room and 0.23 Hz (IQR = 0.05 Hz) for the reference room. A decrease in respiratory rate often signifies a relaxation response. This observation, suggestive of increased parasympathetic activity, aligns with the HRV findings. There was a significant negative correlation between changes in the LF power and changes in respiratory rate, r(43) = −.43, p = .004, indicating that slowed breathing was associated with increased LF values.
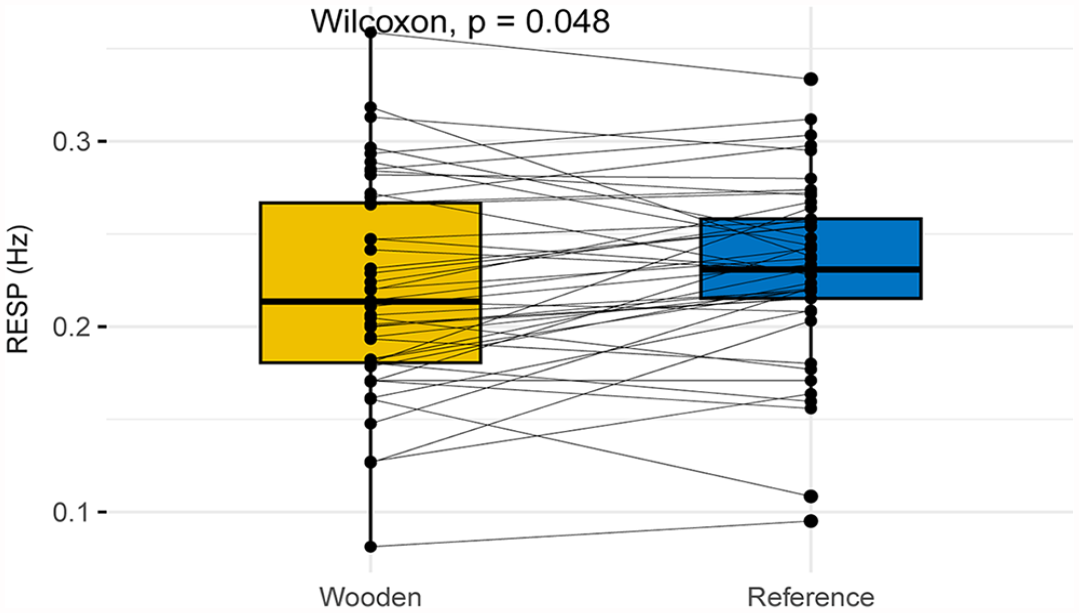
The respiratory rate (RESP) in the wooden and reference rooms.
Subjective Evaluation
Utilizing Warr’s questionnaire, the wooden room exhibited a significantly elevated positive affect (Mdn = 4.50, IQR = 1.33), Z = −2.99, p = .003, compared to the reference room (Mdn = 4.04, IQR = 1.33). Moreover, negative affect was notably diminished in the wooden room (Mdn = 1.40, IQR = 1.00), Z = −2.92, p = .004, relative to the reference room (Mdn = 1.80, IQR = 1.40). Table 1, detailing results from the semantic differential questionnaire, provides a thorough overview of subjective perceptions. It’s of note that, for enhanced readability, all adjective pairs initially presented in a positive-to-negative order in the questionnaire have been reversed in the table. Every adjective pair significantly favored the ambiance of the wooden room.
The Results of the Multidimensional Semantic Differential Questionnaire.
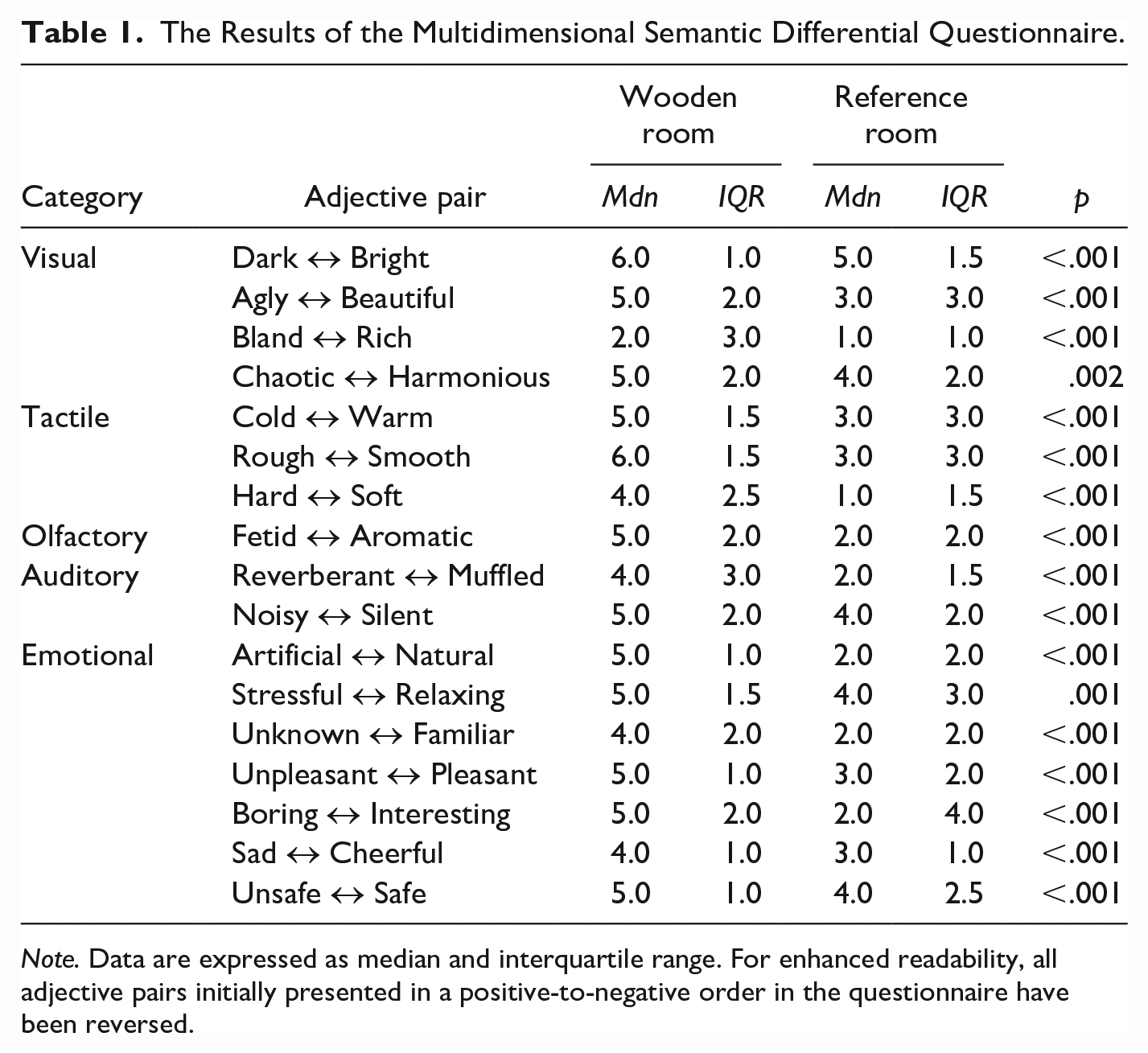
Note. Data are expressed as median and interquartile range. For enhanced readability, all adjective pairs initially presented in a positive-to-negative order in the questionnaire have been reversed.
Discussion
This study employed a robust cross-over design to compare HRV-derived psychophysiological well-being, and questionnaire-measured affective wellbeing and perception between wooden and reference rooms within the same session. There were no differences in the RMSSD results between the wooden and reference rooms, or in the HF values, which are also commonly used to indicate parasympathetic activity. However, the LF was significantly higher in the wooden room. Existing mechanistic studies suggest that in resting conditions, LF also reflects parasympathetic activation (Brown et al., 1993; Kromenacker et al., 2018; Shaffer & Ginsberg, 2017). This result was supported by the lower breathing rate in the wooden room and the correlation between LF changes and breathing rate. The subjective results show that positive affect was higher and negative affect lower in the wooden room, which was also perceived more favorably with the sensory evaluation. Taken together, the findings of this study do not support the hypothesis that the wooden interior would increase the RMSSD. Nonetheless, the observed improvements in LF, breathing frequency, affective well-being, and sensory perception—although secondary outcomes—were sufficiently powered to detect changes. This supports the hypothesis that wooden interiors can produce acute beneficial psychophysiological effects.
The LF and Respiratory Rate Were Improved in the Wooden Room
The functional role of LF has not been clear, and 24-hr ambulatory observations have suggested that it displays influences of both sympathetic and parasympathetic branches (Pagani et al., 1984, 1986). Nonetheless, in a relaxed resting condition the LF seems to reflect baroreflex activity, which is primarily vagally mediated (Keyl et al., 2001) and thus indicates mainly parasympathetic activation (Goldstein et al., 2011; Reyes del Paso et al., 2013; Schwerdtfeger et al., 2020; Shaffer & Ginsberg, 2017; Shaffer et al., 2014). Especially during periods of slow respiration rates, respiratory-related vagally mediated influences are present in the LF band (Brown et al., 1993; Kromenacker et al., 2018; Shaffer & Ginsberg, 2017). This study also showed a significant negative relationship between the changes in LF values and the changes in the respiratory rates. Participants breathed about one breath per minute more slowly in the wooden room. Many HRV biofeedback studies have reported elevated LF values with SDNN and no change in HF when breathing more slowly (Lin et al., 2019; Schwerdtfeger et al., 2020; Steffen et al., 2021). In this study, the SDNN did not differ significantly, but there was an elevated trend in the wooden room compared to the reference room (p = .083). In short-term recordings, the SDNN seems to be linked with breathing (Shaffer & Ginsberg, 2017). HRV biofeedback aims to slow down breathing to obtain a higher HRV and various health benefits. Especially breathing at a resonance frequency of about 0.1 Hz, that is, six breaths per minute, plays a significant role in physical and mental health via optimizing energy supply (Laborde et al., 2022; Schwerdtfeger et al., 2020). In the current study, the participants breathed 12.8 times per minute in the wooden rooms and 13.8 times per minute in the reference rooms. Past research has not provided insights into respiratory rates within wooden interiors. As such, the differing respiratory impacts of the rooms had not been predicted, positioning the respiratory rate as an exploratory outcome for this study. Similarly, previous literature hadn’t reported on LF values within wooden environments. Without any specific breathing instructions, participants in this study instinctively adjusted their breathing in the rooms. Consequently, the wooden interior appeared to lead to slower breathing and a higher LF band power, indicative of enhanced relaxation.
Affective Well-Being Better in the Wooden Room
The positive affect was higher and negative affect lower in the wooden room compared to the reference room when measured with Warr’s affective well-being questionnaire. This suggests better psychological well-being in the wooden room. Our result is in line with a previous study by Demattè et al. (2018), who found more positive and fewer negative emotions during a 15 min stay in a wooden room compared to a plaster room. Demattè et al. (2018) used a Positive and Negative Affect Schedule of 20 adjectives. Additionally, Zhang et al. (2016) found that more positive and fewer negative emotions were experienced during a 60 min exposure to wooden environments. They used the Profile of Mood States (POMS) questionnaire, a 6-point scale consisting of 65 adjectives, summarized into six subscales: tension, depression, anger, fatigue, confusion, and vigor, to self-rate personal emotional states. Sakuragawa et al. (2005) measured a decrease in the POMS subscale of depression in a wooden room after a 90 s exposure, while Tsunetsugu et al. (2002, 2005, 2007) found no differences between rooms in the POMS total score or any of the subscales. Bamba and Azuma (2015) reported a faster rate of fatigue perception reduction in a wooden room after a 10 min exposure. It seems that several minutes of wooden exposure are required to induce positive psychological effects. Additionally, lengthy questionnaires might be problematic in short interventions, and POMS’ primary targets originally were depression and anxiety in clinical settings (Ekkekakis & Zenko, 2016). This study measured the core affect recommended for restoration research (Ekkekakis & Zenko, 2016; Lipovac & Burnard, 2020).
The Wooden Interior Was Perceived More Favorably
The positive physiological and psychological effects were accompanied by different subjective perceptions of the wooden room when measured with a multidimensional semantic differential questionnaire. All 17 adjective pairs relating to a sensory and emotional evaluation of the rooms were experienced differently. More favorable scores were obtained for the wooden room. The wooden environment was perceived as natural, familiar, pleasant, and safe, with appealing aesthetics, high contact comfort, and as having an enjoyable smell and convenient acoustics. The results are consistent with those of Demattè et al. (2018), who also used a semantic differential questionnaire and found differences in several adjective pairs across the four senses. Other studies have utilized a smaller number of questions related to perception and varied scales. Bamba and Azuma (2015) measured a more intense odor in the wooden room, which was experienced as more pleasant than in the control room. They also measured slightly higher volatile organic compound emissions in the wooden room and concluded that the positive psychological impact was probably due to the synergy of the sight and smell stimulation. Zhang et al. (2016) reported that the wooden room was warmer, lighter, and had a stronger odor, but they did not find differences in the comfort of these sensations. Additionally, a 90 s wooden exposure did not affect comfort (Sakuragawa et al., 2005; Tsunetsugu et al., 2002, 2005, 2007), but it was experienced as more natural than the control room (Sakuragawa et al., 2005; Tsunetsugu et al., 2007). The rooms and measurement setup in the present study were planned to stimulate the participants’ sensory systems as much as possible, as explained in the methods section. For example, the wooden surfaces had only a light surface treatment, and the participants were barefoot during the measurements. It seems that the holistic sensation of the wood led to a more comfortable and natural experience, as predicted by the biophilia hypothesis (Richardson & Butler, 2022).
Strengths and Limitations
Studies have shown that viewing nature and access to natural light are linked to positive well-being outcomes (Jo et al., 2019; Konstantzos et al., 2020). To maximize the wall surface area, a window was installed in the ceiling of the rooms for lighting in this study. In both rooms, there was a view of the sky and treetops in the participant’s field of sight, but there was no direct eye contact with the window. The only difference in the rooms was the material of the inner surfaces. If there were positive effects of viewing nature or lighting, they were the same in both rooms, and the achieved differences in the present study were due to the dissimilar inner surface material. Unlike previous studies, the one-session cross-over design effectively revealed minor differences in the parasympathetic outcomes between the inner surface materials. The psychophysiological outcomes are challenging to measure if the sessions are performed on different days due to the day-to-day variability in stress and HRV values. The HRV changes based on external and internal stress factors, such as physical activity levels, nutrition, sleeping patterns, illness, and alcohol use. For the same reason, the long-term effects of a wooden interior are challenging to investigate. Nonetheless, it can be presumed that the acute results seen in this study would accumulate after prolonged exposure to the wooden interior. Although there are statistically significant differences in the effects of the two rooms, inter-individual variability exists in the physiological responses. This might be due to the discontinuous ability to relax throughout the experiment or the variable nature relatedness of the participants. An additional limitation of the study is the overrepresentation of female participants (n = 37), which makes the results less representative for males (n = 13). Future research should also investigate gender-related effects. Furthermore, the study was limited to healthy adults. Future studies should investigate the effects of the wooden indoor environment on other age groups and clinical populations.
Conclusion
In conclusion, in the wooden room, there was higher HRV and a slower respiratory rate; both are related to better recovery and health benefits. In addition, the positive affect was higher in the wooden room, and the negative affect was lower when compared to the reference room. The positive physiological and psychological effects were accompanied by a more favorable sensory perception of the wooden room. Accordingly, wood was preferred over artificial materials and was found to have beneficial effects on psychophysiological well-being in this study. Our findings suggest that short-term exposure to wooden interior positively influences markers of relaxation and stress, with detectable effects observed after only 10 min. Although the effects noted in our study were modest, they serve as a promising indicator of the potential for wooden interior to contribute positively to health and recovery. This also hints at the possibility that longer exposure periods could yield more significant health benefits. Consequently, our results warrant further research into the long-term effects of wooden indoor environments on health, involving extended exposure periods and comprehensive evaluations of both physiological and psychological well-being. Additionally, future research should consider the impact of wooden interiors on diverse populations, including individuals with mental health conditions, to broaden our understanding of the therapeutic potential of wood in indoor environments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the European Regional Development Fund, Grant #308471. Preliminary results from some of the data were presented at the National Wood Seminar organized by Puuinfo, held in Helsinki, Finland on November 3, 2022.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article.